
Abstract
Background and Aims:
Revision arthroplasty of metacarpophalangeal (MCP) joints in chronic inflammatory arthritis patients after silicone implants is challenging due of severe bone loss and soft tissue deficiencies. The aim of this study was to evaluate the outcome of revision MC Parthroplasty using poly-L/D-lactic acid 96:4 (PLDLA) interposition implant and morcelised allograft or autograft bone packing in patients with failed MCP arthroplasties and severe osteolysis.
Material and Methods:
The study group consisted of 15 patients (15 hands and 36 joints) at a mean follow-up of seven years (range 5–10 years). The radiographs were reviewed for osteolysis and incorporation of the grafted bone. The clinical assessments included active range of motion, evaluation of pain, subjective outcome and assessment of grip power.
Results:
PLDLA interposition arthroplasty combined with bone packing provided satisfactory pain relief, but function was limited. Radiographic analysis showed complete incorporation of the grafted bone to the diaphyseal portion of the host metacarpal and phalangeal bones in 30 of the 36 joints. All the patients had very limited grip strength, both on the operated and non-operated side.
Conclusions:
Due to soft tissue deficiencies long-term function and alignment problems can not be resolved with PLDLA interposition implant.
Keywords
INTRODUCTION
Several studies have shown that metacarpophalangeal (MCP) joint arthroplasties using a silicone implant provide good pain relief, improve the arc of motion and correct the deformity (1, 2) though the results deteriorate over time (3, 4). In long-term follow-up studies after silicone arthroplasty of the MCP joints, osteolysis, subsidence and fracture of the implants frequently occur (3, 5, 6). One radiological study showed osteolysis around 89% of the implants (1). Revision MCP arthroplasty after silicone implants is challenging because of severe bone loss and soft tissue deficiencies. The use of a silicone implant in revision MCP arthroplasty is limited by poor survival (7).
A porous, bioabsorbable poly-L/D-lactic acid 96:4 (PLDLA) interposition implant is designed to retain its shape long enough to allow the ingrowth of host tissue and then gradually be replaced with fibrous tissue in approximately 2–3 years (8–10). This implant has yielded promising results in both primary and revision MCP arthroplasties (11–14).
In this study, we report the mean seven years follow-up results of revision MCP arthroplasty using PLDLA interposition implants and morcelised allograft or autograft bone packing in patients with failed MCP arthroplasties and severe osteolysis. The one-year results were published earlier (14).
MATERIAL AND METHODS
This study was approved by the Päijät-Häme Central Hospital district ethical committee, Lahti, Finland. Initially, 18 patients (21 hands; 52 joints) with chronic inflammatory arthritis (all women, all right-handed), previous MCP arthroplasty and severe osteolysis at one or several MCP joints, were recruited to this prospective, non-randomized study. There were three dropout patients (6 hands, 16 joints). One patient of the dropouts had both hands operated (all together eight MCP joints) and two patients had one hand (all together five MCP joints). In two of all analyzed patients both hands were operated, but only one was controlled and thus two hands were dropped out (all together three MCP joints), leaving 15 patients (15 hands; 36 joints) to be assessed. All patients signed a written informed consent and were operated on using morcelised allograft or autograft bone packing and PLDLA interposition implants (Bionx Implants Inc., Tampere, Finland; currently Scaffdex, Tampere, Finland) during the 2001 to 2003 time period at the Rheumatism Foundation Hospital (Heinola, Finland). The mean follow-up time was seven years (range 5–10 years). In addition, one patient had recently suffered a forearm fracture and due to an over-elbow plaster cast she was unable to perform some of the functional tests.
The indication for all of the MCP joint revision arthroplasties was a combination of pain, dysfunction and bone loss. 10 patients had rheumatoid factor positive rheumatoid arthritis (RA), three had juvenile idiopathic arthritis, one had psoriatic arthropathy and one had rheumatoid factor negative chronic polyarthritis.
The procedure was done under tourniquet, and the patient was given routinely single dose antibiotic prophylaxis of cefuroxime 3000 mg. Joint was approached by longitudinal incision adjacent to extensor tendon. Old prostheses were removed. Scar and granulation tissue was removed from inside the metacarpal and phalangeal bones. Volar plate was released, when necessary. Ulnar intrinsic tendons and abductor digiti minimi tendon were always checked and released if not performed previously or if there was found tight scar tissue. Significant cortical bone perforations and periarticular cortical defects were recorded. Allograft bone (fresh frozen femoral heads or tibial/femoral cuts of non-rheumatoid patients) was morcelised to 2–3 mm chips which then were packed inside the bones leaving the juxta-articular portion empty at this stage. Two to three microburr holes were drilled to the distal dorsal aspect of the metacarpal bones. Collateral ligaments were tied with absorbable multi-filament 2–0 or 3–0 hold sutures for later tightening or reconstruction and the threads were passed through the burr holes. A PLDLA scaffold (thickness 4 mm, diameter 12 or 14 mm, provided by Tampere University of Technology (Tampere, Finland) was inserted in the joint space and fixed with a 1–0 absorbable suture passing through the burr holes and grabbing the volar plate adjacent to the base of the phalanx. At this stage the bone packing was completed up to the level of bone ends. After bone packing the implant fixation suture was tightened and thereafter the collateral ligaments were tightened while balancing the finger alignment simultaneously. Suction drain was applied in revisions of all metacarpophalangeal joints, except not in cases with one or two revised metacarpophalangeal joints. Capsule closure was performed with 3–0 absorbable sutures and extensor tendon was centralized. Duplication or small resection of capsule was performed when necessary. Subcuticular closure with 4–0 absorbable sutures and skin closure with 4–0 non-absorbable sutures. Padded dressing supporting fingers towards the radial direction was used.
On second or third day after operation the fingers were supported with a rest splint. Patients were discharged and they returned to the ward at 10–14 days postoperatively in order to begin the range of motion exercises and dynamic splint. Splints were used for 3 months and the range of motion exercises were supervised by an occupational therapist in the ward and in outpatient follow-ups. Outpatient control visits were programmed at 6 weeks, 3 and 12 months postoperatively with radiographs taken before and after the operation and at 3, 12 and 24 months. The final control was done in this study at 5 to 10 years after revision operation.
The clinical assessments included active ROM measurement of the MCP joints, evaluation of pain and measurement of deformity of the MCP joints and assessment of grip power and functional tip pinch, precision and power grips. Active extension and flexion were measured from the dorsal surface using a goniometer. A visual analogue scale (VAS, 0–100) was used to evaluate pain. Palmar subluxation of the MP joints was measured from standardized supine oblique radiographs with fingers in maximal active extension, and it was graded as 0 = no subluxation, 1 = subluxation less than 50% of metacarpus thickness, 2 = subluxation more than 50% of metacarpus thickness, 3 = complete dislocation. Radiographs were assessed visually the incorporation of the bone grafts. The radiographic osteolysis changes were assigned of the metacarpal and the proximal phalangeal bones to four grades depending on the radiological cortical bone changes (15): Grade I: Osteolysis varying from a single clear line adjacent to the stem of the prosthesis to a larger, clear area which did not involve the bone cortex. Grade II: Osteolysis affecting the bone cortex to a maximum of one half of its thickness. Grade III: Osteolysis affecting the cortex to more than one half of its thickness but not perforating it. Grade IV: Osteolysis perforating the cortex.
Ulnar deviation was measured dorsally using a goniometer with the fingers in maximal active extension. Grip strength in both hands was measured using a Jamar dynamometer (Preston, Jackson, MI, USA) with the handle in position two. The best value of three consecutive measurements was recorded. Function of the hand was evaluated by an occupational therapist. Tip pinch grip was assessed for each finger with a wooden bead of diameter 10 mm: the patient was asked to pick up the bead from the table using tip pinch in each finger by turn. A therapist performed simulated ADL tests, such as ability to handle a knife and fork (precision grip) and a jug with capacity of 0.5 litres (cylinder and transverse volar grip). In the precision grip assessment the patient used a knife and fork to cut a piece of resistive exercise putty (Rolyan A497-280, diameter 7.5 cm). In the cylinder grip test the patient was asked to decant 1 dl water from a jug to a glass (diameter 6–7 cm), and decanting the water back to the jug was assessed as a transverse palmar grip. These functional grips were graded as normal, adapted or not able, the adapted meaning to be able to perform the task but not in the requested way. A timed Box and Block test was used to evaluate the dexterity of the hand (16). The Box and Block test result indicates the number of cubes transposed per 60 seconds. Patient satisfaction was assessed using a scale indicating excellent, good, satisfactory or poor outcome. Measurements were recorded by an occupational therapist and radiographs were analyzed by an orthopaedic surgeon.
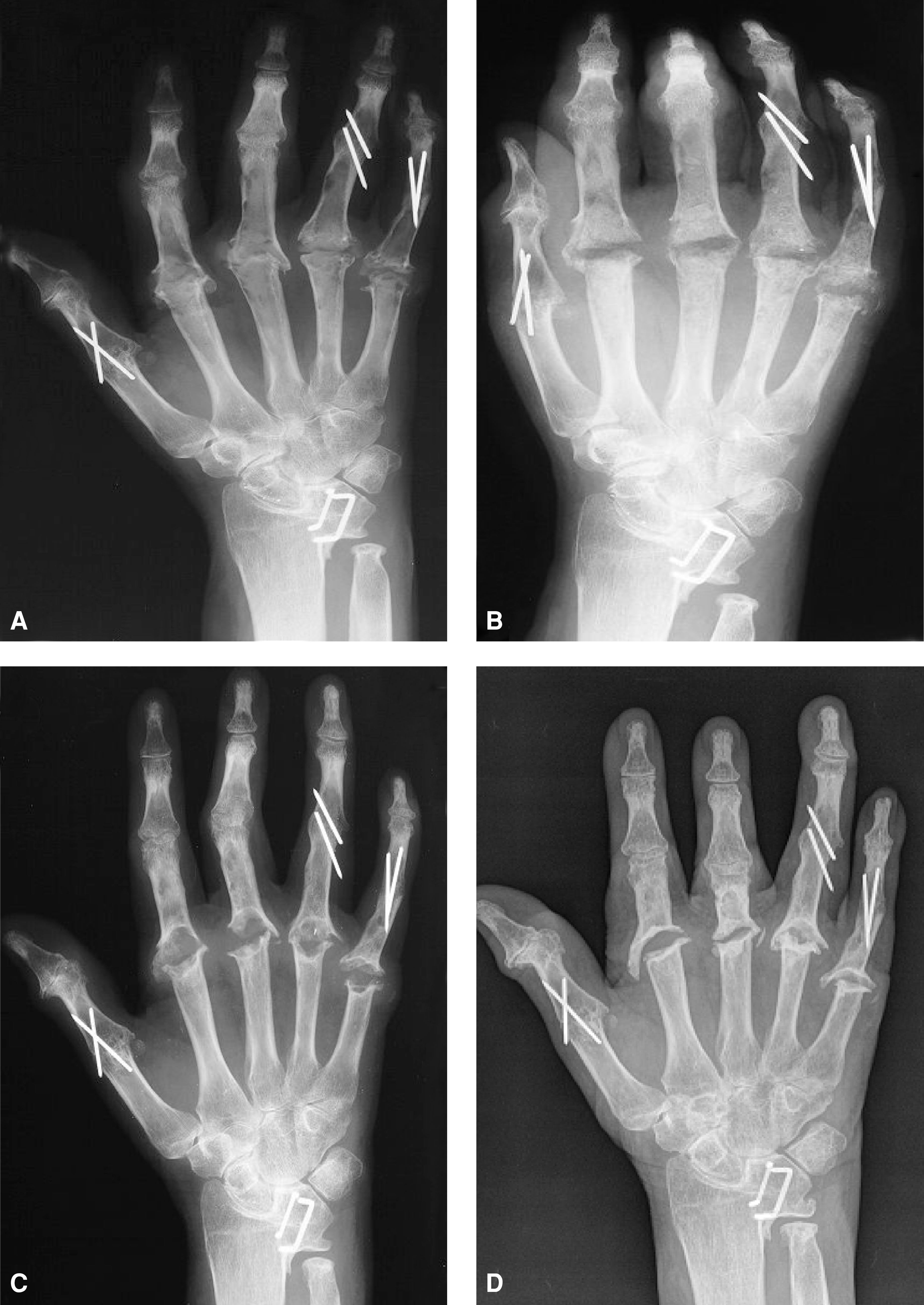
(A) Preoperative radiograph rheumatoid arthritis patients with severe osteolysis and broken silicone implants in all four MCP joints. In the metacarpal bones II–V osteolysis is assigned grade III. In the 2nd and 5th proximal phalanges osteolysis is staged grade III, 3rd and 4th proximal phalanges grade IV. (B) Postoperative radiograph after bone packing and PLDLA implant interposition arthroplasty. (C) After one-year postoperatively bone graft incorporation was good to the diaphyseal portion of the metacarpal and phalangeal bones, but typical periarticular bone absorbtion was noticed. (D) After seven years postoperatively.
The most descriptive data are presented as mean and (SD) or range. Statistical comparisons were performed using oneway-ANOVA. We used SPSS 17.0 statistical software (SPSS Inc, Chicago, Illinois, U.S.A.) for the statistical analyses.
RESULTS
Radiographic analysis showed complete incorporation of the grafted bone to the diaphyseal portion of the host metacarpal and phalangeal bones in 30 of the 36 joints. At one-year follow-up complete incorporation in the metacarpal and phalangeal bones was 48/52. Grade III or IV osteolysis recorded in 32 (89%) of the metacarpals and 34 (94%) of the proximal phalanges (Table 1). Grade I osteolytic changes were only one patient. This patient with single MCP joint silicone implant arthroplasty developed aggressive foreign body reaction against silicone implant, and PLDLA implant and bone packing was chosen to avoid recurrence even in the absence of severe bone loss.
The osteolytic grades in metacarpals (n = 36) and proximal phalanges before MCP revision arthroplasty using bone grafting and PLDLA interposition implant.
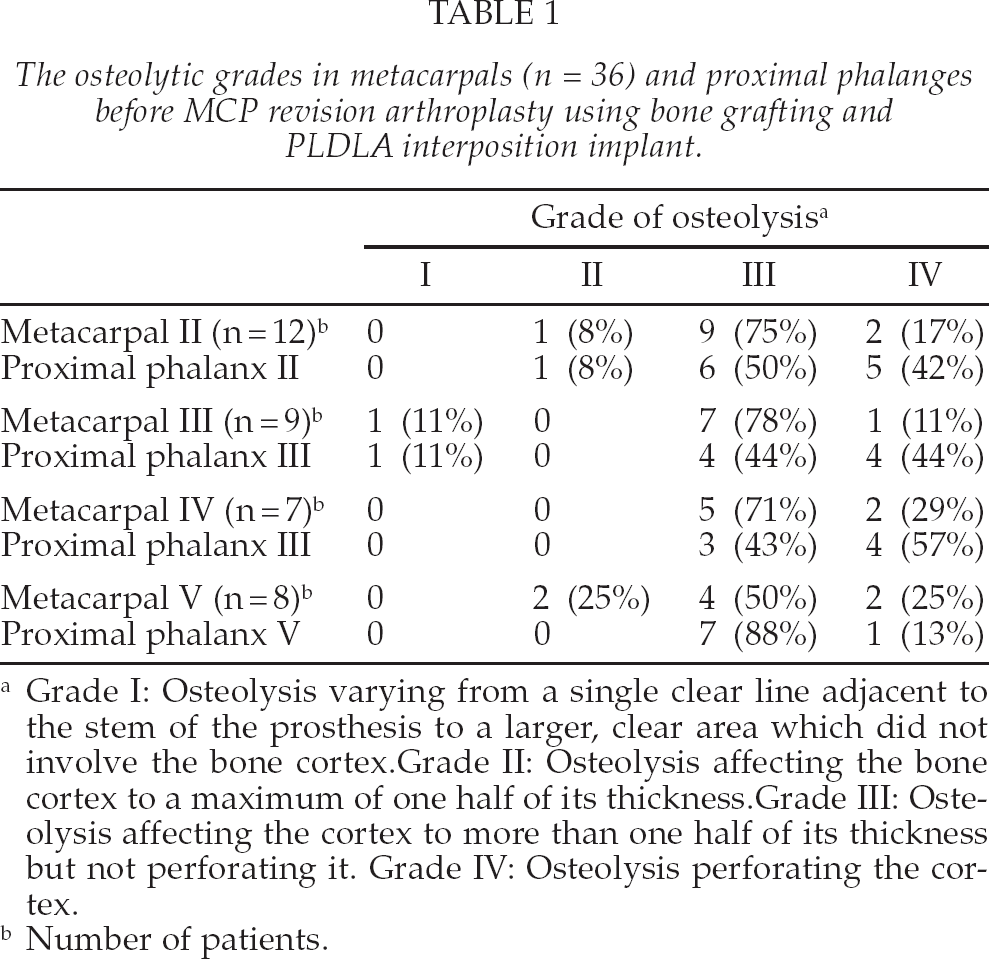
Grade I: Osteolysis varying from a single clear line adjacent to the stem of the prosthesis to a larger, clear area which did not involve the bone cortex. Grade II: Osteolysis affecting the bone cortex to a maximum of one half of its thickness. Grade III: Osteolysis affecting the cortex to more than one half of its thickness but not perforating it. Grade IV: Osteolysis perforating the cortex.
Number of patients.
The presence of self-reported pain was favourable and the pain was usually rated mild with mean pain being VAS 12.3 (range: 0–53). At the time of the interview, 13/15 (87%) of the patients had no (n = 5) or minimal pain (VAS less than 27). The patients with a 4-MCP revision had a tendency to have less pain compared to those with a single or 2-MCP revision but there was no statistical difference.
Limited flexion at average seven years after MCP revision arthroplasty was the most common clinical finding in active range of motion examination; detailed results are presented in Table 2. In the measurements made before the operation and at the clinical follow-up, both the active extension and flexion range of motion had a tendency to diminish. The worsening was statistically significant in MCP II active flexion, and almost reached significance in MCP III and IV flexion, despite the small number of patients.
Operated MCP joint active range of motion (ROM) before and after MCP revision arthroplasty using bone grafting and PLDLA interposition implant.
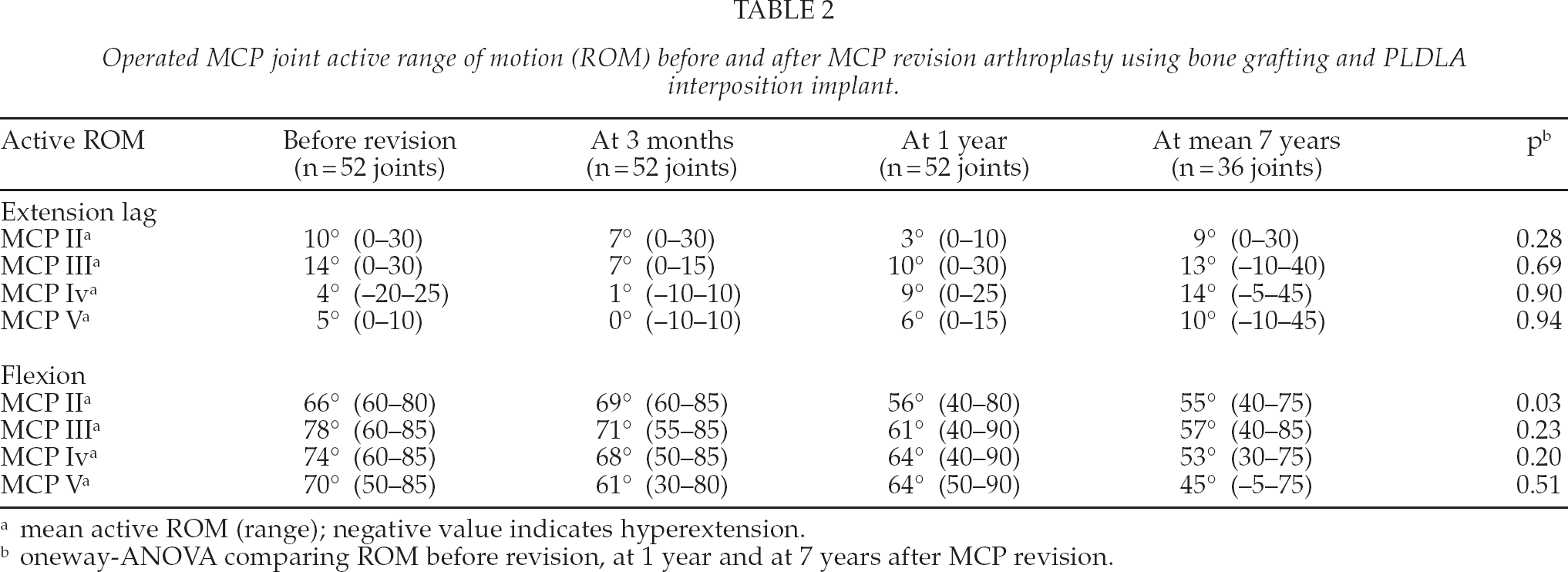
mean active ROM (range); negative value indicates hyperextension.
oneway-ANOVA comparing ROM before revision, at 1 year and at 7 years after MCP revision.
All the patients had very limited grip strength at average seven years follow-up, both on the operated and non-operated side. The mean grip strength was 4.3 kg (range: 0–14) on the operated side (13 right and 2 left hands) and 5.9 kg (range: 0–26) on the non-operated side. Furthermore, only three (20%), five (33%) and two (13%) of patients could perform the power grip jug test, the power grip glass test or the precision grip test, with a normal grip. Results of other function tests are presented in Table 3.
Operated hand (n = 15) power, precision, pinch grip and Block and Box tests at mean 7 years after MCP revision arthroplasty using bone grafting and PLDLA interposition implant.
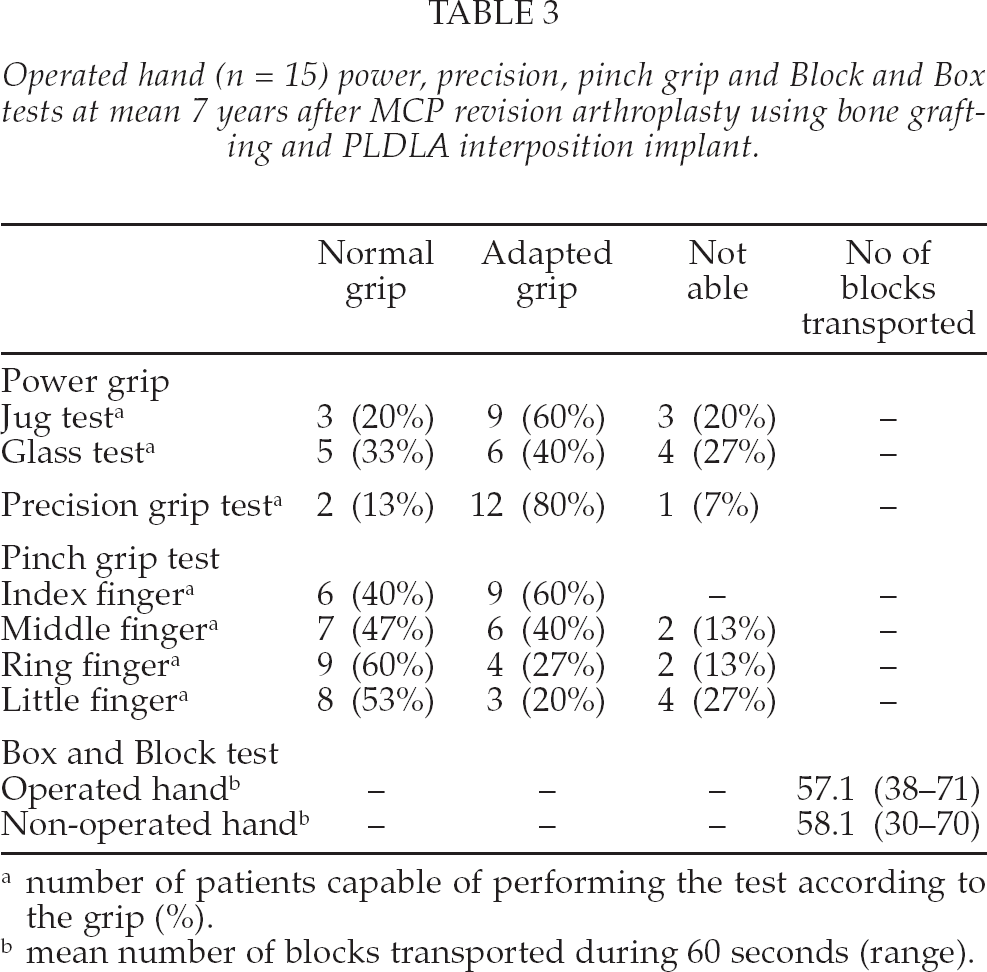
number of patients capable of performing the test according to the grip (%).
mean number of blocks transported during 60 seconds (range).
Initially the overall patient satisfaction was good with 93% and 90% good or satisfactory results at three months and one-year, respectively. At the final follow-up, subjective outcome was excellent in one patient with a single-MCP revision. Three patients considered the result to be good, all having undergone a single or 2-MCP revision. Six patients considered the outcome satisfactory and five patients the outcome poor.
Number of operated joints (36 joints) presenting volar dislocation at mean 7 years after MCP revision arthroplasty using bone grafting and PLDLA interposition implant.
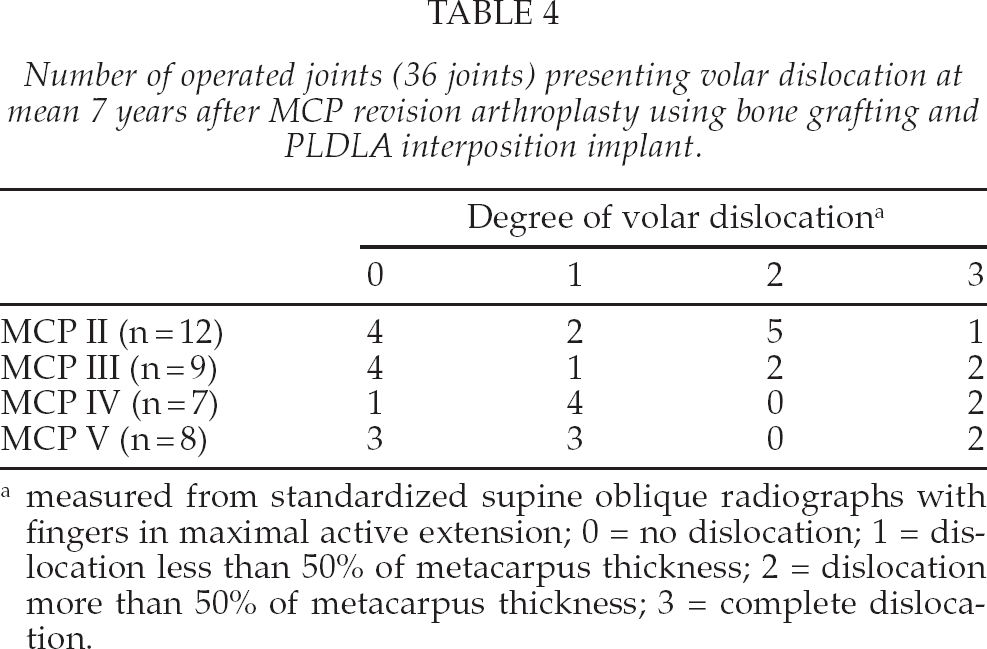
measured from standardized supine oblique radiographs with fingers in maximal active extension; 0 = no dislocation; 1 = dislocation less than 50% of metacarpus thickness; 2 = dislocation more than 50% of metacarpus thickness; 3 = complete dislocation.
Volar displacement of the proximal phalanges occurred in 24 of the 36 joints (67%). Complete dislocation was in 7 joints (table 4). In one juvenile rheumatoid arthritis patient, all four revised MCP joints were completely dislocated at mean seven years follow-up. Recurrent volar displacement occurred already in 33 of the 52 joints (63%) at one-year follow-up. The average ulnar deviation was in 2-MCP 4° (range: −35–25), 3-MCP 10° (0–20), 4-MCP 14° (5–20) and 5-MCP 13° (0–30) at final follow-up. At one-year follow-up ulnar deviation was 5–13° degrees with tendency to be larger towards the ulnar fingers.
No wound healing problems were encountered. Some patients suffered transitional loss of tactile sensation. Three patients required manipulation under regional anaesthesia at five, six and seven weeks after surgery, respectively, because of limited flexion movement in at least one of the fingers which had undergone surgery. In all three patients, the ranges of motion improved notably and were satisfactory at one year follow-up but deteriorated again corresponding to the common tendency.
One patient with severe dorsal defects in the second metacarpal bone underwent additional surgery to excise sharp residual volar osteophytes that were interfering with flexor tendon function in the tenosynovial sheath at eight months after the revision arthroplasty.
DISCUSSION
Revision MCP arthroplasty using PLDLA interposition implant and bone packing in patients with failed MCP arthroplasty and severe osteolysis can prevent or reduce the rate of bone loss. Pain relief continues to be good at average seven years after revision but the initially acceptable functional results have a tendency to deteriorate.
Silicone arthroplasty is still the golden standard for MCP primary joint replacement. In a large study, 17 years' survivorship of silastic MCP implant arthroplasty has been 63% using revision or radiographic implant fracture as the end-point (6). In that study revision rate was low: 76 of 1336 implants; 39 implants (2.9%) were reoperated due to fractured stems. Study group concluded that radiographic implant fracture doesn't necessitate revision arthroplasty. There are only a few series concerning revision MCP arthroplasties (4, 17–20). Re-revision rates have varied from 2.1% to 26.5%. In these studies, reported implant fracture rates varied from 2.9% to 10.4%. Broken implants were only one reason to revision surgery, other causes included deformity, stiffness, malalignment and silicone synovitis. Parkkila et al have reported that fractured silicone implants are associated with osteolysis (5). Due to severe osteolysis, bone perforations and diverse soft tissue problems were encountered during revision surgery in our patients, a new silicone implant is not an ideal option in revision MCP arthroplasty. The PLDLA interposition arthroplasty aims to avoid the foreign body reaction, prosthesis wear or fracture complications associated with the use of silicone implant (10, 12, 13).
Revision MCP arthroplasty using a PLDLA implant interposition, provides a good pain relief. Initially good patient satisfaction declined during the follow-up; ultimately 75% of the patients considered the outcome satisfactory or poor. All the patients had very limited grip strength measurements at average seven years' follow-up, both on the operated and non-operated side. These patients had very severe rheumatoid disease and also the other hand was destroyed. Limited flexion was the most common clinical finding of active range of motion.
Volar displacement of the proximal phalanges occurred in 24 of the 36 joints (67%) and complete dislocation in seven joints. One patient had a complete dislocation of all four MCP joints and three patients had a complete volar displacement in one MCP joint. In the one-year results, volar displacement occurred in 63% (33/52 joints). Ulnar deviation remained the same during follow-up. This study shows that majority of recurring of volar displacement and ulnar deviation occur during first year after revision operation. This trend is also evident in revision arthroplasties using silicone implants: pain relief is excellent but there is only minimal improvement in ulnar drift, a high rate of implant fracture (34%), and no change in arc of motion (7).
The main problem in revision MCP arthroplasty seems to be soft tissue reconstruction. If collateral ligaments and other soft tissue support are lost, none of the available implants or scaffolds can stabilize the MCP joint. All patients of our series presented severe soft tissue deficiencies, including missing or only rudimentary collateral ligaments. Also, the joint capsules and extensor mechanism were stretched and elongated. In revision operation the collateral ligaments were reconstructed through the bone holes with absorbable, multi-filament sutures. When sutures absorb there is no collateral support and volar displacement can occur. After this study, we have started to use non-absorbable instead of absorbable sutures to reconstruct collaterals. Surgical technique has also been altered to include resection of the prominent volar lip of the proximal phalanx, and the attachments of the ligaments are sacrificed. Non-absorbable sutures are passed through drill holes in both phalangeal and metacarpal bones. These sutures are tightened while balancing the finger alignment. We expect these amendments to provide a longer lasting primary support and in the long term diminish recurrence of ulnar deviation.
Incorporation of grafted bone was radiographically complete to the diaphyseal portion of the host metacarpal and phalangeal bones in 30 of the 36 joints. Periarticularly bone absorbtion was noticed already at one-year after operation. This may have occurred as a result of insufficient blood supply or foreign body reaction caused by the PLDLA interposition implant (14).
In conclusion, revision MCP arthroplasty using PLDLA interposition implants and bone packing provided good pain relief, but functional results were generally poor. This study showed that soft tissues are very critical to the function and alignment. Thus far, none of the available implants or PLDLA interposition arthroplasty can not stabilize the MCP joint in severe cases and malalignment will return soon.
Footnotes
ACKNOWLEDGEMENTS
This work was supported by Päijät-Häme Hospital special state subsidy (EVO) for health science research.