
Abstract
Background and Aims:
Loosening of a hip prosthesis after total arthroplasty is related to periprosthetic bone loss. Calcitonin has been used in the treatment of bone loss in osteoporosis and prevention of fractures. The main purposes of the study were firstly to evaluate the effect of calcitonin on periprosthetic bone after total hip arthroplasty, secondly investigate possible loosening of the prosthesis and thirdly examine further clinical outcome.
Patients and Methods:
60 patients who underwent total hip arthroplasty using cemented Exeter prosthesis were randomized in the treatment group (salmon calcitonin 200 IU nasal spray daily + calcium 500 mg) and the placebo group (inactive nasal spray + calcium 500 mg) for six months. Bone mineral density (BMD) was measured from different locations at the time of discharge and after six and 12 months. Dynamic histomorphometry on bone biopsies taken from femoral collum was performed. Serum bone-specific alkaline phosphatase (BAP), serum osteocalcine (OC) and cross-linked N-telopeptides (NTX) were measured after one week, one month, three months and 12 months. Clinical manifestations and the incidence of fractures and loosening of the prosthesis were followed up to eight years.
Results:
Statistically there was not significant difference in bone histomorphometry between the groups. In both groups there was a significant BMD decrease in periprosthetic bone. However, the difference between the groups was not statistically significant. In the biochemical analysis NTX increased more in the Miacalcic group than in the placebo group (p = 0.013). There were no significant differences between the groups in serum BAP or OC even though the changes within the groups were statistically significant. No loosening of the prosthesis was seen during the follow-up and there was no need for revision of any reason. Four fractures were recorded in three patients. One patient sustained a periprosthetic fracture. All the patients with fractures were allocated in the placebo group.
Conclusions:
Nasal salmon calcitonin 200 IU on a daily basis does not promote any additional value on calcium substitution to prevent bone loss after hip replacement. The durability of the Exeter prosthesis was good.
Keywords
INTRODUCTION
Hip replacement is the best treatment modality in hip arthrosis. Aseptic loosening of the prosthesis is the most frequent complication requiring in most cases revision surgery of the failed prosthesis. Often aseptic loosening is complicated by periprosthetic bone loss. Osteolysis is caused by wear of polyethylene and as a result of relative motion between the opposing surfaces under load (1, 2, 3). The wear particles in a biological environment cause a tissue reaction where macrophages are in central role. The end result is aseptic loosening of the prosthesis and destruction of bone.
Less attention has been paid to the bone as a biological living organ in which the prosthesis is applied. There are only a few histomorphometric studies on periprosthetic bone (4). Although the best prosthesis and bone cements are used, the arthroplasty may fail if the bone is not well adhered to the cement or prosthesis. Immediately after cementing, the bone-cement interface is tight. Bone remodelling may not be sufficient to keep the bone firmly adhered to the cement, as the resorption of bone without compensatory new bone formation will result in loosening of the mantle from the bone and widening of the effective joint space. This phenomenon may begin immediately after the hip replacement. Heat is produced during polymerization of the bone cement and this may cause injury to the adjacent bone. Injured bone is resorbed, and new bone should be produced to replace the damaged one. If the repairing process is not sufficient, it will result in incomplete bonding between the cement and bone.
Osteoporosis is a disorder where this imbalance between bone formation and resorption exists (5). Immobilization is known to lead in local bone loss (6) and periarticular loss of bone is well known for example in patients with rheumatoid arthritis (7). The basic mechanism of loosening of cemented hip prosthesis is suggested to be based on the same type of imbalance between osteoblastic and osteoclastic activity where bone resorption dominates bone formation.
Calcitonin has been widely used in the treatment of osteoporosis (8). It is a 32-amino acid polypeptide hormone produced predominantly in C-cells of the thyroid gland. Calcitonin mainly acts in inhibiting osteoclast function. It has been shown that nasally administered salmon calcitonin decreases osteoporotic fractures (9). Studies have shown that 200 IU salmon calcitonin is the most effective dose to treat osteoporosis.
The main aim of the study was to show that salmon calcitonin 200 IU on a daily basis can improve periprosthetic bone metabolism and prevent from loss of bone mineral density (BMD) after hip replacement, and make implants less vulnerable to loosening. The second purpose of the study was to examine whether the preoperative status of bone turnover has any predictive value in the loosening of hip prosthesis. The third objective of the study was to evaluate the outcome of the implant and the incidence of fractures after the hip replacement.
PATIENTS AND METHODS
A total of 60 patients were enrolled in the study between May 2002 and June 2003. They all underwent total hip arthroplasty in the Kanta-Häme Central Hospital, Hämeenlinna, Finland. Arthroplasties were performed using cemented Exeter prosthesis. Female and male patients with unilateral hip arthrosis were included in the study. Patients with secondary arthrosis, diseases or previous treatments that could have had effect on bone metabolism were excluded. The patients were randomly enrolled into two groups (30 patients in each group) and Informed consent was obtained. The study protocol was reviewed and accepted by the local ethics committee.
The investigational therapy was synthetic salmon calcitonin (Miacalcic) 200 IU nasal spray, which was given as a single spray daily in alternating nostrils for six months. The reference therapy was placebo nasal spray matching Miacalcic 200 IU nasal spray without the active component. The treatment modalities were introduced on the first postoperative day. All patients were given 500 mg calcium daily.
BONE MINERAL DENSITY
BMD was measured using dual-energy X-ray absorptiometry (DXA; Lunar DPX, Madison, WI) at intact proximal femoral neck, trochanter, Ward's triangle and lumbar spine. BMD was also measured above the acetabular component at standardized region of interest (ROI, modified zone 1) and from periprosthetic bone of the femoral component (Fig. 1), so called Gruen's zones (10), using a special software. The measurements were performed by trained personnel and quality standards were tested daily. BMD was measured after the hip replacement at the time of discharge and after six and 12 months.
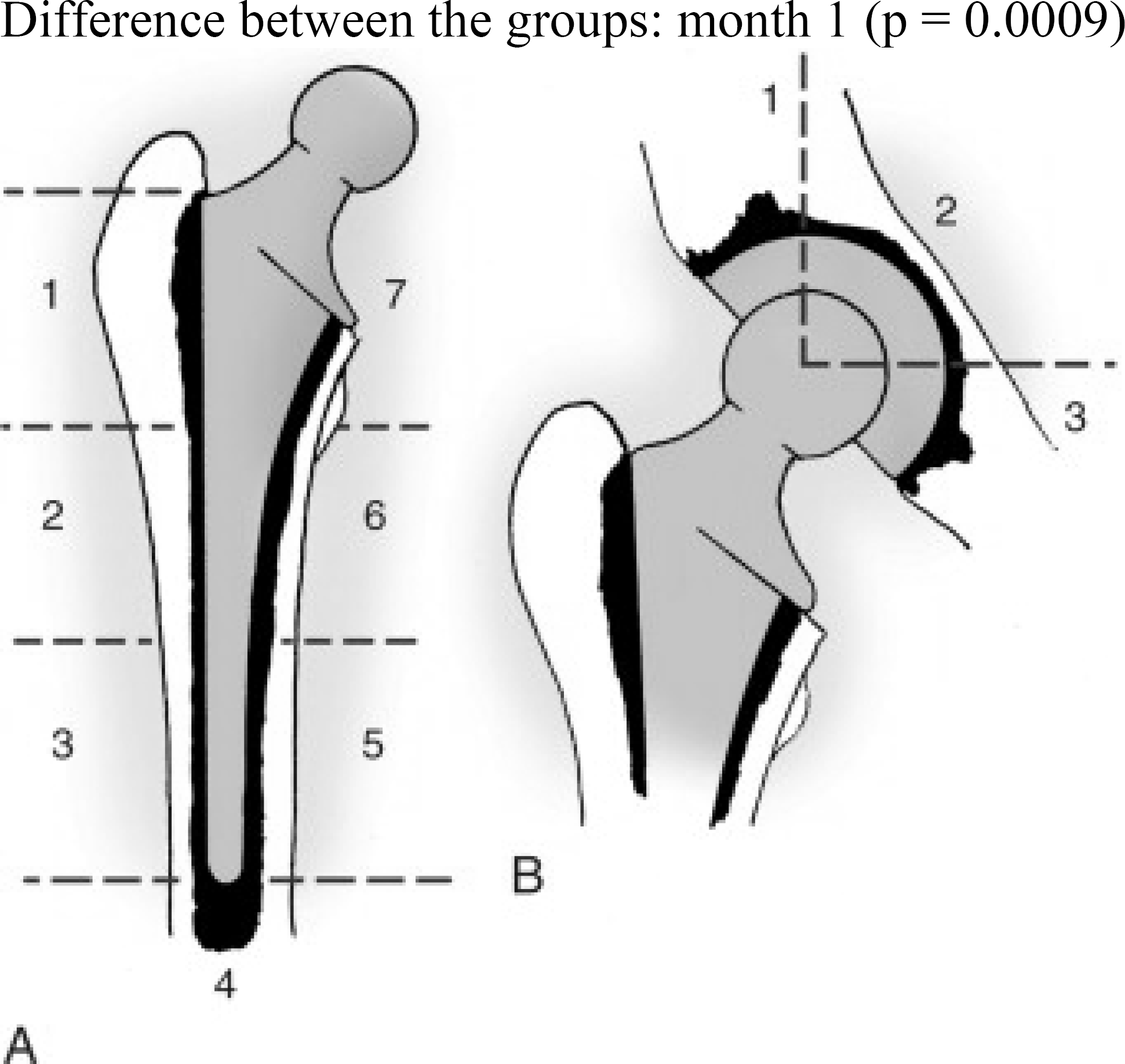
Zones around cement mass in femur (A) and in pelvis (B). (Redrawn from Amstutz HC, Smith RK: Total hip replacement following failed femoral arthroplasty, J Bone Joint Surg 61A: 1161, 1971) Published in Campbell's operative orthopaedics, 11th ed., 2007, p. 421. Published with permission.
BONE HISTOMORPHOMETRY
A bone biopsy was performed at the time of surgery. A bone sample, 25–30 mm in length, was taken from trabecular bone of femoral collum at the resection line using a trephine. Double labelling of bone was performed using tetracycline hydrochloride 500 mg t.i.d. with a regimen of 2 – 10 – 4. All bone samples were processed without removal of the mineral (11). They were fixed in ethanol, and embedded in methylmethacrylate. Serial undecalcified sections of 3 and 7 micrometers were cut using a microtome. Three micrometer sections were stained with the modified Masson-Goldner trichrome stain (12). Ten micrometer sections were prepared for fluorescent light microscopy. Static and dynamic parameters of bone structure, formation and resorption were measured using an Osteoplan system (13).
BIOCHEMISTRY AND RADIOLOGY
Blood samples were taken preoperatively, after one week, one month, three months and 12 months. BAP was measured using routine clinical laboratory methods. BAP is a bone turnover marker measured in serum. BAP reflects the increased turnover of bone in various conditions. OC is produced by osteoblasts and it is used as a marker of bone formation. OC was measured with RIA method. A specific immunoassay was used to study bone resorption with NTX, which is generated from bone by osteoclasts as a degradation product of type I collagen.
Routine X-ray examinations were performed at the first postoperative day, three months and 12 months. Especially signs of loosening were evaluated based also on Gruen's zones (Fig. 1). After 12 months of study X-rays were taken every three years during routine check-up visits.
CLINICAL EXAMINATION AND LONG-TERM FINDINGS
After screening and randomization the patients were examined three, six and 12 months after study began. Clinical evaluation and functional analysis were based on a follow-up protocol approved by a Finnish Arthroplasty Society. Visual analogue scale (VAS) was used to evaluate pain on day 0, 1, 2, 3, 5, 7 and one month and three months after the operation. VAS analyses were performed under the guidance of a study nurse. Further clinical evaluation was based on our routine protocol.
The patients enrolled in the study were followed up to eight years to study possible further Clinical outcome. Periprosthetic or any other fractures were recorded. Also the rate of and reasons for revisions were examined.
STATISTICS
Comparison within and between the groups were performed using the SPSS statistical program (SPSS Inc., Chicago, Illinois). Non-parametric test (Mann-Whitney U-test) was used for comparison of the histomorphometric parameters. For BMD and biochemical data an analysis of covariance (ANCOVA) was used to evaluate the significancies for repeated measures. Unpaired T-test was used for analysis between the groups.
RESULTS
BONE MINERAL DENSITY
In the femoral neck, there was a 0.9% average decrease in BMD from baseline to six months and a 0.2% mean increase from baseline to 12 months in the Miacalcic group. In the placebo group, there was a 0.2% mean increase from baseline to six months and a 0.2% mean decrease from baseline at 12 months. These changes were not statistically significant.
In trochanter and Ward's triangle, there was a 0.3% mean decrease in BMD both from baseline to six months and from baseline to 12 months in the Miacalcic group. In the placebo group, there was an increase from baseline to six months and a 1.1% mean decrease from baseline to 12 months. These changes were not statistically significant.
In lumbar spine there was a similar percentage increase in BMD from baseline to 6 and 12 months in both groups. In the Miacalcic group, BMD increased 1.6% from baseline to 6 months and 1.4% from baseline to 12 months. The increase to 6 months was statistically significant (p = 0.033), but the increase to 12 months was not (p = 0.059). In the placebo group, the increase was 1.2% to 6 months and 0.6% to 12 months. No statistical significance was detected.
In acetabulum BMD increased 0.2% from baseline to six months and 1.0% from baseline to 12 months in the Miacalcic group. In the placebo group, there was a 0.6% decrease to six months and a 0.3% increase to 12 months. These changes were not statistically significant.
In Gruen zones (Fig. 1) the interaction between the visit and the zone, testing whether the changes from baseline to six months were different compared to the changes from baseline to 12 months between the different zones, was statistically significant (p = 0.012). The changes from baseline to six and 12 months were not statistically significantly different between the two groups and the zones (p = 0.053). In the Miacalcic group, there was a statistically significant decrease from baseline to 6 months in zones 5, 6 and 7 and to 12 months in zones 3, 4, 5, 6 and 7. The largest decrease of 12% was seen in the change to 12 months in zone 7. In the placebo group, there was a statistically significant decrease from baseline to six months in zones 5, 6 and 7 and to 12 months in zones 3, 5, 6 and 7. The largest decrease of 9.0% was seen in the change to 6 and 12 months in zone 7 (Table 1.).
BMD at Gruen zone 7 (g/cm2)
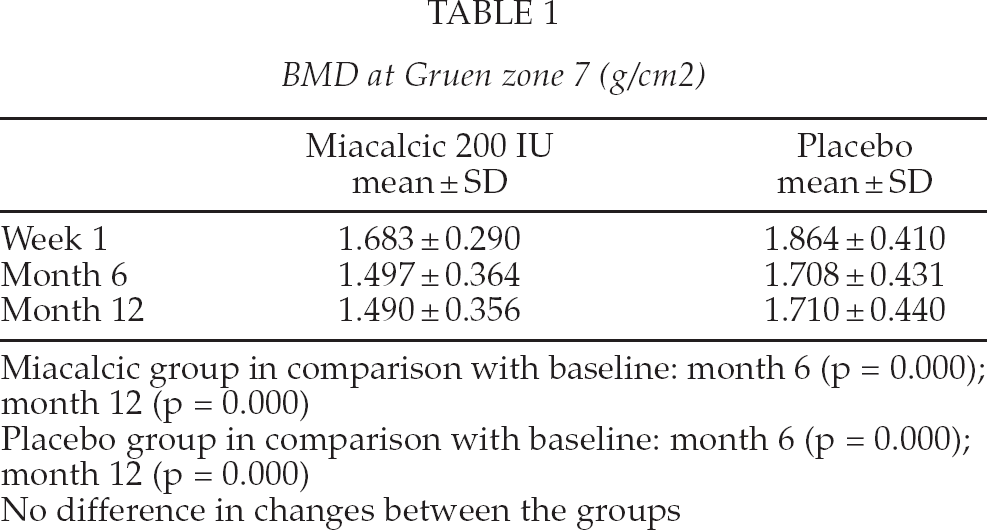
Miacalcic group in comparison with baseline: month 6 (p = 0.000); month 12 (p = 0.000)
Placebo group in comparison with baseline: month 6 (p = 0.000); month 12 (p = 0.000)
No difference in changes between the groups
BONE HISTOMORPHOMETRY
There was not a statistically significant difference between the Miacalcic and placebo group in the variables of bone histomorphometry except in the erosion surface (ESBS). The mean ESBS was higher in the placebo group compared to the Miacalcic group (p = 0.026). The bone histomorhpmetry parameters did not have a statistical impact on any of BMD response variables, when the BMD baseline value was used as a covariate in the statistical model, ie. the baseline BMD measurement explained the changes in the BMD values better than the histomorphometry parameters.
BIOCHEMISTRY
Mean BAP decreased from the preoperative level to one week and increased from one week to three months and decreased slightly after that and reached the same level at 12 months as at one month after surgery (Table 2.). The trend was similar in both groups, and the difference between the groups was not statistically significant (p = 0.94). The decrease in mean BAP from baseline to one week was statistically significant in both groups (p < 0.001). The decrease from preoperative level to 12 months was statistically significant in both groups (Miacalcic 0.0496; placebo 0.030). The preoperative value of BAP had a statistically significant impact (p < 0.001) on the change from baseline.
Serum bone specific alkaline phosphatase (μg/l)
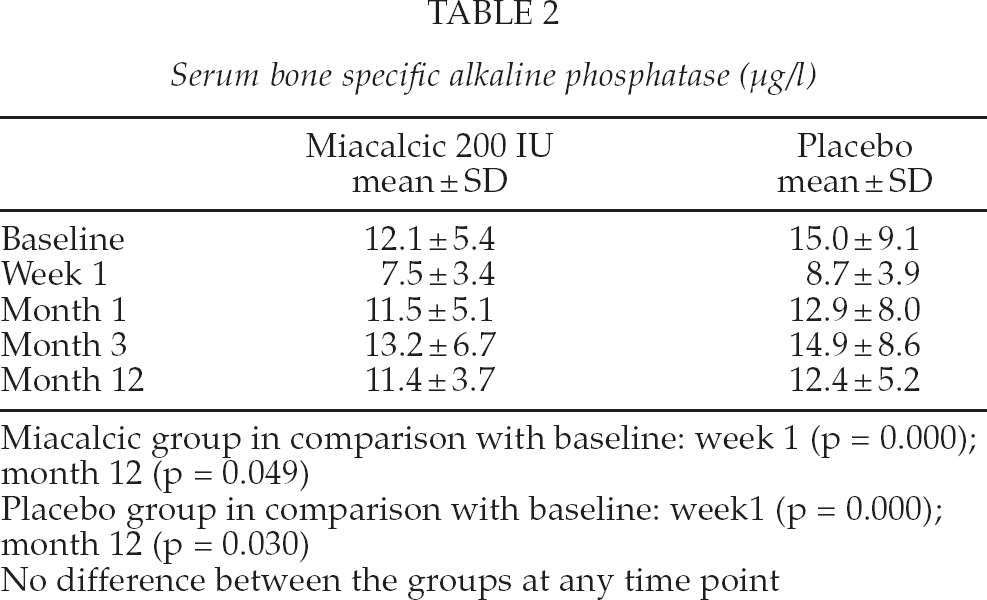
Miacalcic group in comparison with baseline: week 1 (p = 0.000); month 12 (p = 0.049)
Placebo group in comparison with baseline: week1 (p = 0.000); month 12 (p = 0.030)
No difference between the groups at any time point
After a short postoperative decrease OC reached the preoperative level at one month (Table 3). The trend was similar in both groups. The decrease in mean OC from the baseline to one week was statistically significant in both groups (p < 0.001). The changes in later visits were not statistically significant in neither group. Preoperative OC value had a statistically significant impact (p = 0.013) on the change from baseline.
Serum osteocalcine (μg/l)
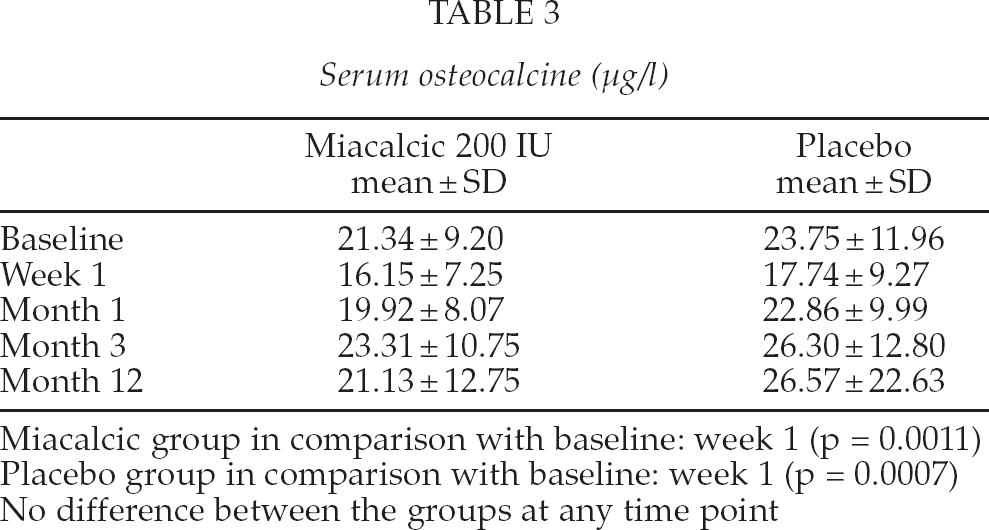
Miacalcic group in comparison with baseline: week 1 (p = 0.0011)
Placebo group in comparison with baseline: week 1 (p = 0.0007)
No difference between the groups at any time point
The values in the NTX increased more in the Miacalcic group compared to the placebo group and the overall difference between the groups was statistically significant (p = 0.013). In addition, the interaction between the treatment and the visit was almost significant (p = 0.059), indicating that the differences between the groups were not consistent at the different time points
The largest difference between the groups was seen at one month, the increase in the Miacalcic group being 31.5 points higher than in the placebo group (p < 0.001). The increase in the Miacalcic group was also somewhat higher compared to the placebo at month three, the difference being 17.1 units (p = 0.07). The differences at week one and 12 months were clearly smaller, p-values for the treatment difference being 0.29 and 0.89 respectively.
In the Miacalcic group mean NTX increased from baseline to 3 months and reached its highest value at one month (Table 4). Thereafter there was a decrease and the mean N-telopeptides at 12 months was slightly below the baseline value. The increases to one month and three months were statistically significant (p < 0.001 and p = 0.004 respectively).
Serum cross-linked N-telopeptides (nmol/mmol)
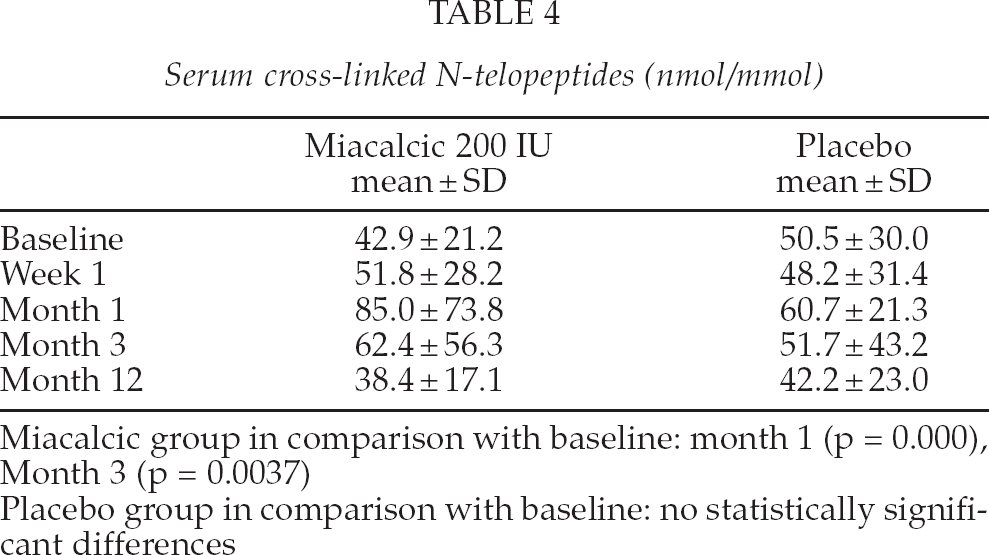
Miacalcic group in comparison with baseline: month 1 (p = 0.000), Month 3 (p = 0.0037)
Placebo group in comparison with baseline: no statistically significant differences
In the placebo group mean NTX decreased from preoperative level to one week and increased after that up to 1 month. Thereafter there was a decrease and the mean NTX at 12 months was slightly below the baseline value. None of the changes were statistically significant.
RADIOLOGY
Postoperative X-rays from all of the patients revealed good radiological results without any immediate postoperative complications. During 12 months follow-up no radiolucent lines were seen in either of the treatmnet groups.
CLINICAL EXAMINATION AND FOLLOW-UP
The intensity of pain decreased during the study significantly in both Miacalcic (p < 0.001) and placebo group (p = 0.003). At any time point there was not a statistically significant difference in pain between the groups. No serious side effects or complications with the implants were reported during the extended clinical follow-up. Seven of the patients have died. Four of them were enrolled in the placebo group and three in the Miacalcic group. The follow-up time of these deceased patients was from seven months to six years. The causes of death were not prosthesis or fracture related.
Four fractures in three patients were recorded during the follow-up period. All patients with fractures were women and they were allocated in the placebo group. One patient sustained a supracondylar fracture of the right humerus after four years of intervention. After falling down one patient had a distal radial fracture of her left radius and just after one week she sustained a periprosthetic fracture of her left hip. These fractures occurred six years after the beginning of the study. One patient sustained a fracture of the lateral malleoli of her right ankle after a minor accident. In the Miacalcic group there were no fractures during the follow-up period. There were no clinical or radiological signs of loosening of the prosthesis components, dislocations or need for revisions
DISCUSSION
Previously it has been shown that biological reactions in the periprosthetic tissue may lead to loosening of the prosthesis (14, 15). Also, it has been shown that alumina and ultra-high molecular weight polyethylene may affect on osteoclastogenesis predisposing to osteolysis (16). In addition to studies at molecular level, there are some publications showing that calcitonin might have a positive effect on the inhibition of periprosthetic bone loss after hip replacement. In a study, where hip fracture patients were treated with cementless total hip arthroplasty, calcitonin 200 IU intranasally was given postoperatively (17). They found that calcitonin reduced bone turnover, loss of bone density and also pain. The functional status of the patients was improved, too. There are no previous publications of the effect of calcitonin on periprosthetic bone after elective hip arthroplasty. Therefore, calcitonin was selected as an antiresorptive agent in this study.
Also, other antiresorptive drugs have been used to prevent bone loss after the joint replacement. In a meta-analysis (18) it was concluded that bisphosphonates appeared to have a larger effect on bone loss following arthroplasties with cement than on bone loss following arthroplaties without cement especially in knee replacements. In a recent meta-analysis of 14 randomized controlled trials (19) RCTs confirmed a significant short-term and middle-term efficacy of bisphosphonate on periprosthetic bone loss after joint arthroplasty.
In this study there were no statistically significant differences in BMD between the groups in the periprosthetic bone. However, in the lumbar spine BMD was increased (p = 0.0033) from the baseline to six months in the Miacalcic group. In studies on treatment of osteoporosis it has been shown that calcitonin can decrease fracture rate even though changes in bone mineral density are minor (20).
Evaluation of periprosthetic bone using dual-energy X-ray absorptiometry has been conducted during many years. Significant postoperative bone loss has been shown to develop in the calcar region both using uncemented and cemented prosthesis models (21, 22, 23, 24). In addition, it has been shown that the most remarkable bone loss is evident during the first six months. In all studies the greatest bone loss has been seen in the calcar region. These results are in accordance with the present study. Thus there are only minor changes in periprosthetic bone after one year.
A bone biopsy taken from the iliac crest has previously been used to predict loosening of the hip prosthesis (4). In this study a biopsy taken from the cancellous part of the femoral collum was used to study bone histomorphometry. There are no reference values for histomorphometry in this region. The baseline bone mineral density explained the changes in postoperative BMD better than histomorphometry. It seems that histomorphometry on bone biopsies taken from the femoral collum is too arduous and does not give any added value in comparison with BMD measurement and biochemistry.
Bisphosphonates has been shown to be associated in the supression of biochemical markers in studies after hip replacement (25, 26) In the present study BAP and OC decreased immediately after surgery in both groups. Later there was an increment in both parameters. There was no statistically significant difference between the groups. NTX increased postoperatively in both groups and there was a statistically significant difference between the groups at one month. This increment was higher in the Miacalcic group. This outcome may reflect suppression of cellular activity in the periprosthetic bone immediately after hip replacement using cemented components. Later there is recovery of bone metabolism even though the balance between resorption and formation may be slightly negative.
The patients tolerated treatment modalities well and no serious side effects or discontinuation of the medication were reported. Calcitonin did not promote any pain relief in comparison with the placebo group. Calcitonin has also been used after hip replacement to prevent heterotopic bone formation after total hip replacement (27). In this study, no heterotopic ossification was seen in either group during the 12 month study period.
The changes in the bone mineral density after hip replacement in the intact proximal femur, lumbar spine and in the priprosthetic bone were small. The greatest decrement of BMD was seen in the calcar region after the operation as has been shown in previous publications. There were no statistically significant changes between the groups. The lack of difference may be explained by calcium substitution given to all the patients. Also, after the immediate recovery period physical activity level of the patients increased in both groups. It seems that nasal salmon calcitonin 200 IU daily does not promote any added value on calcium substitution to prevent bone loss after hip replacement. This is also supported by clinical and radiological follow-up of the patients up to eight years. There were no loosening or need for revision in any of the patients. All the fractures in the follow-up period occurred in the placebo group. No patient had bone specific treatment after the study period except calcium substitution of 500 mg. The possible role of calcitonin in the prevention of further fractures during the follow-up period can not be confirmed based on the results of this study. The main goal of the study was to examine short term effects of calcitonin in the periprosthetic bone.
Footnotes
ACKNOWLEDGEMENTS
The work was financially supported by Novartis.