
Abstract
Background:
Giant pulmonary bullae (GPB) are rare and there is little information on incidence, long-term prognosis, and outcome of treatment.
Objectives:
To assess the incidence of GPB in the Icelandic population and to evaluate the outcome of surgical treatment.
Methods:
Twelve consecutive patients (11 males; mean age 60 ± 15.7 years) underwent resection for GPBin Iceland between 1992 and 2009. All were heavy smokers and had bullae occupying > 30% of the involved lung. There were 8 bilateral and 3 unilateral bullectomies and one lobectomy. Pulmonary function tests were performed preoperatively, and at one month and 5.4 years postoperatively. Age-standardized incidence rate (ASR) was calculated, complications and operative mortality were registered, and overall survival was estimated. Mean follow-up time was 8.2 years.
Results:
The ASR for GPB was 0.40 and 0.03 per 100,000 per year for men and women, respectively. There was no operative mortality, but prolonged air leakage (75%) and pneumonia (17%) were the most common postoperative complications. One month postoperatively, mean FEV1 increased from 1.0 ± 0.48 L (33% predicted) to 1.75 ± 0.75 L (57.5% predicted) (p < 0.01), but FVC remained unchanged. RV decreased from 3.9 ± 0.8 L (177% predicted) to 3.0 ± 1.0 L (128% predicted) (p < 0.05), but TLC and DLCO did not change after operation. At long-term follow-up the FEV1 and FVC had declined to near-baseline values. Five-year and 10-year survival were 100% and 60%, respectively.
Conclusions:
The ASR of GPB in Iceland was 0.21 per 100,000 per year. In this small series, bullectomy was found to be a safe procedure that significantly improved pulmonary function. The functional improvement then declined over time. Prolonged air leakage was a common postoperative complication that prolonged hospital stay.
INTRODUCTION
Giant pulmonary bullae (GPB) are defined as large bullae occupying at least one third of the hemithorax (1). Although no large studies have been published, bullectomy has been regarded as the treatment of choice and is recommended in cases with significanct dyspnea related to GPB or complications such as recurrent infections or pneumothorax (2). Early improvements in pulmonary function have been well documented, but information on long-term outcome and survival are scarce. Furthermore, to our knowledge, the incidence of GPB has not been published before (3 –8).
In this population-based study, we used centralized registries to establish the nationwide incidence rate of the disease. At the same time, we evaluated the early and late effects of bullectomy for GPB in Iceland regarding lung function.
MATERIAL AND METHODS
PATIENT SELECTION AND INDICATIONS FOR SURGERY
This was a retrospective study that included all patients who underwent bullectomy for GPB in Iceland between January 1, 1992 and December 31, 2009. GBP was defined as a dilated air space that occupied at least one third of the hemithorax on a chest X-ray or computed tomography (CT) on the chest.
During the study period, a total of 12 patients were diagnosed with GPB and registered in a database containing detailed clinical information on every case. The patients were identified through two different registries: a computerized diagnosis and operation registry and a centralized pathology registry at Landspitali University Hospital, Reykjavik (the only hospital performing thoracic surgery in Iceland).
All the patients had pulmonary emphysema secondary to smoking (mean pack-years: 33.8 ± 14.7) with severe dyspnea and/or complications related to the GPB, such as pulmonary infections or pneumothorax.
All the patients had quit smoking for at least 6 months before the operation and were required to participate in a multidisciplinary pulmonary rehabilitation for at least 6 weeks before the operation. The pulmonary rehabilitation consisted of education, physical and respiratory care instruction, supervised exercise training and psychosocial support.
During the study-period, there was no formal criteria for surgical resection of GPBs. However, cases from the whole country were reviewed by a multidisciplinary pulmonary board at Landspitali Hospital and all GPB cases that met the above criteria and were felt to be suitable for surgery were operated on.
DATA REGISTRATION AND PULMONARY FUNCTION MEASUREMENTS
Data were collected from the clinical records of Landspitali using a standard data sheet. The following information was collected: age, sex, presenting symptoms that led to diagnosis, and duration of symptoms. Radiological findings were also registered from chest X-ray and CT-scan in all cases.
Spirometry was performed before and after surgery (Gould Instruments, Cleveland, OH or Vmax Encore; Sensormedics, Yorba Linda, CA) and long-term spirometry measurements were collected from hospital records and out-patient clinics. Lung volumes were measured using either the helium dilution method or the nitrogen washout method. Diffusion capacity for carbon monoxide (DLCO) was measured with the “single-breath CO” method.
SURGICAL TECHNIQUE
The operations were performed through a sternotomy or anterolateral thoracotomy, and reinforced stapling lines were used for wedge resections. All patients were extubated directly after the operation and chest tubes were removed when the lungs were fully expanded, with no air leakage. Postoperative course was assessed and the number of postoperative complications and the length of hospital stay were recorded. Persistent air leakage was defined as continuous leakage for more than 7 days postoperatively. Operative mortality was defined as death within 30 days of surgery.
STATISTICAL ANALYSIS
Results are presented as mean ± standard deviation or median (range). Paired t-test was used to compare normally distributed data. A p-value of 0.05 or less was considered significant for all tests. For calculations of age-standardized incidence rate, a world standard population was used. During the study period, the average number of individuals living in Iceland was 283.560 (a minimum of 259.727 in 1992 and a maximum of 319.368 in 2009; Icelandic National Registry). Overall survival rate was estimated using the Kaplan-Meier method. Survival data were obtained through the Icelandic National Registry, where dates and causes of death were identified or patients were identified as still being alive on December 31, 2009. Mean follow-up time was 8.2 ± 3.0 years.
The study was approved by the Icelandic National Bioethics Committee and the Icelandic Data Protection Commission.
RESULTS
During the 18-year study period, 12 patients were diagnosed as having GPB. Eleven of them were males, and mean age was 60.0 ± 15.7 years (range: 22 to 77 years). The age-standardized incidence (ASR, world standard) for both genders was 0.21 per 100.000 per year for the whole nation (95% confidence interval: 0.11–0.38); 0.40 (95% CI: 0.20–0.73) per 100.000 for men and 0.034 (95% CI: 0.00085–0.22) per 100.000 for women.
The average operation time (skin to skin) was 90 min (range: 58–150) and all patients were extubated in the operating room. The most common complications were prolonged air leakage (75%, n = 9) and pneumonia (17%, n = 2). One patient was successfully reoperated on for sternal dehiscience. All patients survived surgery and were discharged for further pulmonary rehabilitation.
The median length of hospital stay was 24 days (range: 10–74 days). Overall survival at 5 years was 100% and overall survival at 10 years was 60%. By the end of the study period, 6 of the 12 patients had died, with four deaths occurring at 5.8, 6.8, 7.2, and 8.7 years postoperatively and two deaths occurring more than 11 years after surgery. The causes of death were respiratory failure (n = 4) and pneumonia (n = 2).
Postoperatively, FEV1 improved significantly from 1.0 ± 0.48 L (33.3% ± 11.3 predicted) to 1.75 ± 0.75 L (57.5% ± 20.4 predicted) (p = 0.003) (Table 1). The FEV1/FVC ratio also increased significantly from 34.8% to 48.7% (p = 0.007). The mean increase in FEV1, FEV1 percent predicted, and FEV1/FVC ratio was 0.58 ± 0.4 L, 20 ± 16%, and 13 ± 8%, respectively. Residual volume (RV) decreased from 3.9 ± 0.8 L (177% predicted) to 3.0 ± 1.0 L (128% predicted) (p = 0.02). All the patients remained smoke-free postoperatively.
Pulmonary functional values and diffusion capacity of the lung for carbon monoxide (DLCO) obtained before and 1 month after surgery. Long-term spirometry values are also shown. Values are mean ± SD.
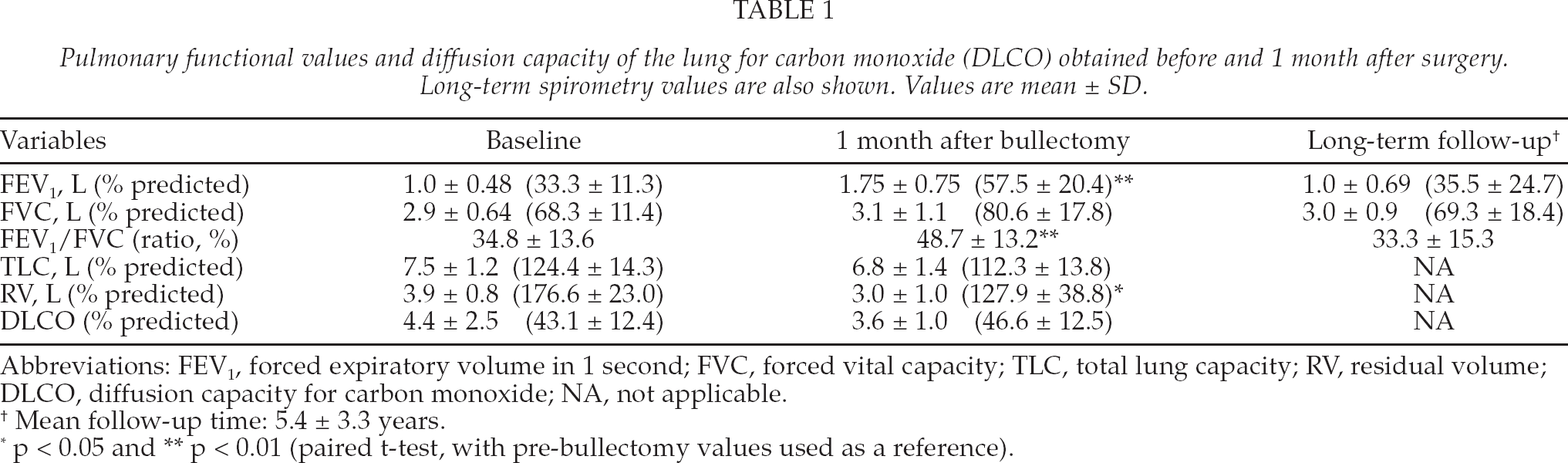
Abbreviations: FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; TLC, total lung capacity; RV, residual volume; DLCO, diffusion capacity for carbon monoxide; NA, not applicable.
Mean follow-up time: 5.4 ± 3.3 years.
p < 0.05 and
p < 0.01 (paired t-test, with pre-bullectomy values used as reference).
Five years postoperatively, the pulmonary function tests had declined to near-baseline levels; FEV1 and FEV1/FVC ratio were 1.0 ± 0.69 L and 33.3 ± 15.3%, respectively. There was no significant difference between the subjects who died and those who survived until the end of the study period regarding mean age, FEV1, or FEV1/FVC ratio (data not shown).
DISCUSSION
In this small population-based series, we found that the ASR of GPB in Iceland was 0.21 per 100.000 per year for the entire nation. To our knowledge, the incidence of GPB has not been reported previously. Despite the limited number of patients, we found a statistically significant improvement in FEV1 and FEV1/FVC ratio after surgery. However, at long-term follow-up (mean 5.4 years postoperatively) the pulmonary function values had declined to near-baseline levels. In other studies, similar findings have been reported, with only one third of the patients maintaining improvements at the five-year follow-up (3, 5, 9,10).
As many GPB patients have no symptoms of their disease, incidence rates largely depend on the likelihood of incidental discovery/diagnosis. Thus, the frequency of medical imaging of the chest, including that performed because of smoking-related conditions, is likely to affect incidence rates. Considering the good availability of medical imaging in Iceland, the ASR of GBP in Iceland could be expected to be in the higher range. There have been few other studies on which to base comparisons, but in a literature review by Snider et al. 476 patients with GPB were reported from 1951 to 1992 (1).
In this series, the bullae were removed surgically, either via thoracotomy or sternotomy. These procedures have gradually been replaced by video-assisted thoracoscopic surgery (VATS), where recovery is quicker and post-operative pain less of a problem (11,–13). Furthermore, for high-risk patients who cannot tolarate open surgery, the modified Monaldi-type drainage procedure (14, 15) or an endobronchial placement of one-way valves have shown to be effective treatment alternatives (16).
The results of this study, although limited, are good in terms of operative mortality and rate of complications. There was no early mortality and 5-year survival was 100%. In other studies, operative mortality has been reported to be between 0% and 22.5% and five-year survival to be in the 76–88% range (3, 17, 18). At follow-up 10 years after surgery, four patients had died, two from pulmonary infections and the other two from respiratory failure related to pulmonary emphysema. Prolonged air leakage was the most common postoperative complication, occurring in three quarters of the patients. This is a relatively benign complication, but it often prolongs the hospital stay. Similar findings have been reported by others (8).
This study is limited by the small number of patients and its retrospective design. Patients were seen over two decades, during which significant improvements in imaging occurred, and this may have affected the number of cases diagnosed during the first years of the study. No standard guidelines for referral of patients for bullectomy were in use during the study period. The strengths of the study were its nationwide design and the complete and relatively long follow-up period. Patients were identified through two different registries separately, and all were operated on at a single cardiothoracic surgical center.
In conclusion, GPS is a rare disease with an ASR of 0.21 per 100.000 population per year in Iceland. Bullectomy is a safe procedure with excellent short-term outcome. Pulmonary function does, however, decline over time and reaches preoperative values by five years postoperatively.