
Abstract
Background:
At the time of diagnosis, almost one third of patients with renal cell carcinoma (RCC) have metastasis. We studied the prevalence, survival, and potential resectability of synchronous pulmonary metastases (SPMs) in a well-defined cohort of RCCpatients.
Material and Methods:
Aretrospective whole nation study including RCC patients with SPM diagnosed 1970–2005 in Iceland. Imaging studies and histology were reviewed, the TNM system used for staging the primary tumors, and disease-specific survival estimated. Eligibility for SPM removal was evaluated using different criteria from the literature on surgical management of SPM, including solitary SPM and SPMs confined to one lung.
Results:
Altogether, 154 patients (16.9%) had SPMs. In 55 of these patients (35.7%) the lungs were the only site, with detailed information available in 46 cases. Of these 46 patients with SPMs, 15 were unilateral, and of those 11 were solitary. All of these 11 patients were in good physical condition and were deemed eligible for surgical resection; however, only one of them was operated with metastasectomy. Disease-specific survival at five years for patients with solitary SPM was 27.2%, as compared to 12.7%, 7.1%, and 12.0% for patients with unilateral SPMs, all patients with SPMs, and patients with extrapulmonal metastases, respectively (p = 0.33).
Conclusion:
At the time of diagnosis, 16.9% of RCCpatients had SPM. In one in three of these SPM patients metastases were confined to the lungs, while one in five had solitary pulmonary metastases. Although the benefit of pulmonary metastasectomy in RCC is still debated and criteria for resection are not well defined, it appears that many RCC patients with SP Mare potentially eligible for pulmonary metastasectomy.
INTRODUCTION
In most European countries, including Iceland, RCC accounts for 2–3% of all cancers diagnosed (1). At the time of diagnosis, more than one third of RCC patients have metastases (2). These patients generally have a poor prognosis, with 5-year survival reported to be between 3% and 11% for unoperated patients (3). This was reflected in a population-based study from Iceland, in which 80% of patients with synchronous metastases died of RCC within two years of diagnosis (4).
The precise indications for surgical resection of pulmonary RCC metastases are still being debated. Most patients who develop pulmonary metastases cannot usually be cured, owing to multiple extrathoracic metastases and lack of effective systemic therapy (5,–7). However, numerous retrospective studies have suggested that there may be a survival benefit following pulmonary metastasectomy in selected patients, where survival rates at five years range from 21% to 60%, with many exceeding 40% (5, 7 –15). Favorable outcome has been related to complete resection, few and small lung metastases, long disease-free interval, and no mediastinal lymph node involvement as determined by preoperative radiological examinations (5,–7, 13, 15,16). Other factors that are used as general preconditions for meaningful surgical removal are loco-regional control of the primary RCC, absence of extrapulmonary metastases, and good general condition of the patient with sufficient respiratory function to tolerate pulmonary resection (5, 7, 17).
The introduction of novel agents as a first-line or second-line treatment in metastatic RCC, including tyrosine kinase inhibitors (TKIs) such as sorafenib and sunitinib, has not clarified the issues relating to the indications for surgical removal in these patients (18, 19). Thus, pulmonary metastasectomy still remains a mainstay in a multidisciplinary approach for selected patients with metastatic RCC (15, 20).
The aim of this study was to investigate the prevalence of SPM in a well-defined cohort of RCC patients and to compare their survival to that of other patients with metastases. Another aim was to try to evaluate potential resectability in patients with SPM, using different criteria regarding eligibility for surgical removal to those suggested in the literature.
MATERIAL AND METHODS
This was a retrospective whole population study involving all patients who were diagnosed with pulmonary metastases at the time of diagnosis of RCC in Iceland, between January 1, 1971 and December 31, 205. During this 35-year period, a total of 910 patients were diagnosed while alive with RCC in Iceland (autopsy cases were excluded). All of these patients have been registered in a database of RCC that contains detailed clinical and histological information on every case. Patients were identified through three different registries: (1) the Icelandic Cancer Registry, (2) a computerized diagnosis and operation registry covering all hospitals in Iceland, and (3) a centralized pathology registry at Landspitali University Hospital, Reykjavik. Through the Icelandic National Registry, patients were assigned a date and a cause of death or were identified as still living on December 31, 209. Mean follow-up time was 49 months (range 0–445 months).
Clinical data were collected retrospectively from the clinical records of the hospitals in Iceland using a standardized data sheet, and reviewed by two of the authors (S.J.O. and T.G.). Synchronous metastases were defined as metastases diagnosed within three months of the diagnosis of the primary RCC. Patients with metachronous RCC metastases and metastases from other cancers were excluded. The following information was collected when available: age, sex, and the dates when the primary RCC and the pulmonary metastases were diagnosed. The presence of other RCC metastases, clinical presentation and duration of symptoms, laboratory results, spirometry values, the preoperative American Society of Anesthesiologists (ASA) classification, and radiological workup were also registered. All available imaging studies were reviewed and the number, size, and location of pulmonary metastases defined. Finally, we registered pulmonary metastasectomies performed during the study period.
A chest X-ray was performed in all the patients preoperatively, together with computed tomography (CT) and/or ultrasound of the liver. A chest CT was performed selectively, usually if tumors were found on conventional chest radiographs or if clinically indicated. CT scans of the brain, bone scans, magnetic resonance imaging (MRI), or cavography were also performed selectively. PET scan is not available in Iceland. All histological specimens were evaluated at the Department of Pathology at Landspitali University Hospital and reviewed separately by two pathologists (S.H. and V.P.). Histological subtypes were classified according to the most recent guidelines from the World Health Organization (2004), and the Fuhrman four-grade scale was used for assessment of nuclear grade. All the primary tumors were staged according to the TNM classification system from 2002 and the AJCC stage grouping from 2002 (21).
Evaluation of potential resectability was based on three different criteria: A, B, and C, which were based on recently published literature. This included patients with solitary SPM without extrathoracic RCC metastases (criterion A), multiple but unilateral SPMs without extrathoracic RCC metastases (criterion B), and multiple bilateral SPMs but without extrathoracic RCC metastases (criterion C). In addition, to be deemed fit for surgery patients had to be in good physical condition (ASA score 1–3) and have sufficient respiratory function to be able to tolerate pulmonary resection.
Microsoft Excel (Microsoft Corp., Redmond, WA) was used for descriptive statistics but all other analysis was done using the R statistical package, version 2.5.1 (R Foundation for Statistical Computing, Vienna, Austria). Statistical analysis on categorical variables was performed using the Chi-square test or Fisher's exact test with 2 × 2 tables. Disease-specific (i.e. cancer-specific) survival rate was estimated using the Kaplan-Meier method. Survival of patients with SPM was compared with that of subgroups in the study population using the log-rank test. A probability value of less than 0.05 was considered statistically significant.
The study was approved by the Icelandic National Bioethics Commitee and the Icelandic Data Protection Commission.
RESULTS
Of the 910 RCC patients, 324 (35.6%) were diagnosed as having synchronous metastases at all sites, and these are listed in Table 1. Pulmonary metastases were most common; they were diagnosed in 154 patients (16.9%), followed by skeletal (11.2%) and liver metastases (7.1%).
Sites of distant metastases in 910 patients with RCC diagnosed in Iceland, 1971–205. Patients could have metastases in more than one organ. Lymph node metastases are not included.
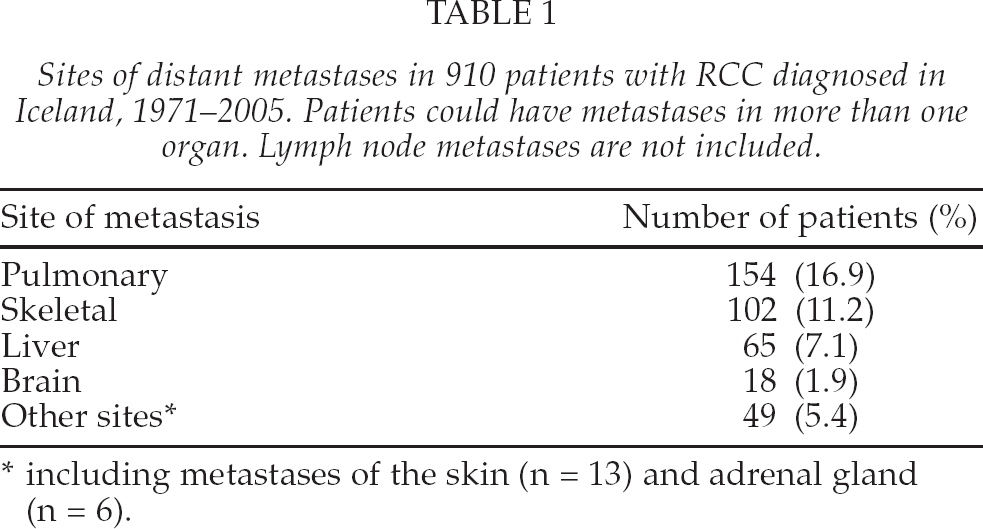
including metastases of the skin (n = 13) and adrenal gland (n = 6).
Patient demographics and clinico-pathological information for the 154 patients with SPM are given in Table 2 (subgrouped into patients with SPM and extrathoracic metastases, SPMs only, and solitary SPM). For comparison, 324 patients with synchronous metastasis in all sites are shown. No significant differences between groups were noted regarding age or gender. The same was true for laterality and T-stage of the primary RCC kidney tumor. The primary tumors, however, were significantly larger in patients with SPMs than in those with metastases in multiple sites (9.5 vs. 8.0 cm, p < 0.01).
Patient demographics for different subgroups of patients with RCC-related metastases diagnosed in Iceland, 1971–2005
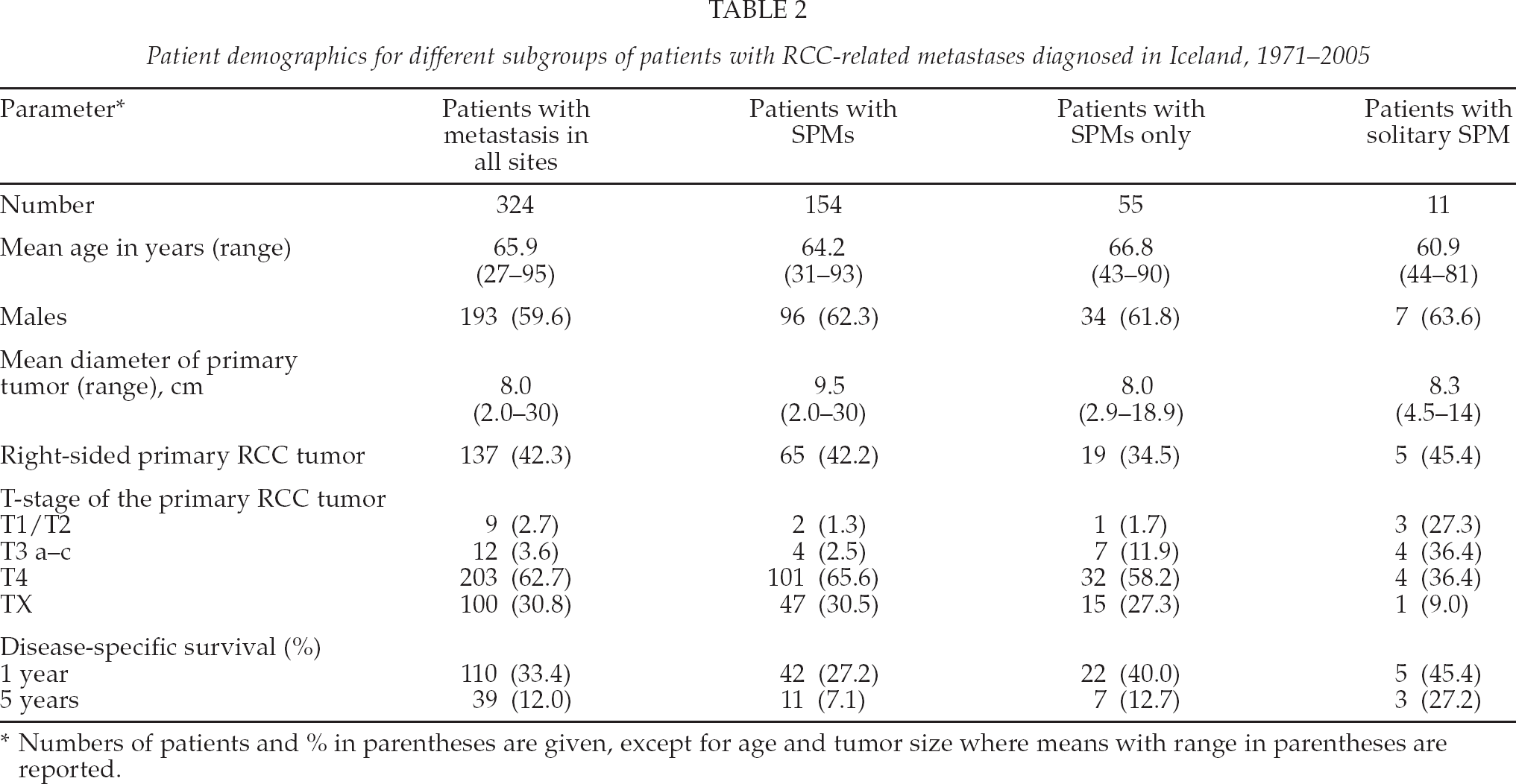
Numbers of patients and % in parentheses are given, except for age and tumor size where means with range in parentheses are reported.
In 99 of the 154 patients with SPM (64.3%), metastases also occurred in other organs, most often in bones (22.0%) or in the liver (17.5%), followed by the brain (5.8%) and the skin (4.5).
In patients with SPMs confined to the lungs (n=55), 21,7% had a solitary metastasis, 6,5% had two metastases, 15.2% had three metastases and 56.5% had four or more lesions. The average number of lesions was four (range 1–15); 31 patients (21.4%) had metastases in both lungs. In 9 cases, detailed information on the number of metastases was missing
The number of patients who fulfilled criteria A, B, or C, was 11 (7.6%), 15 (10.3%), and 55 (35.7%), respectively, which is depicted graphically in Fig. 1.
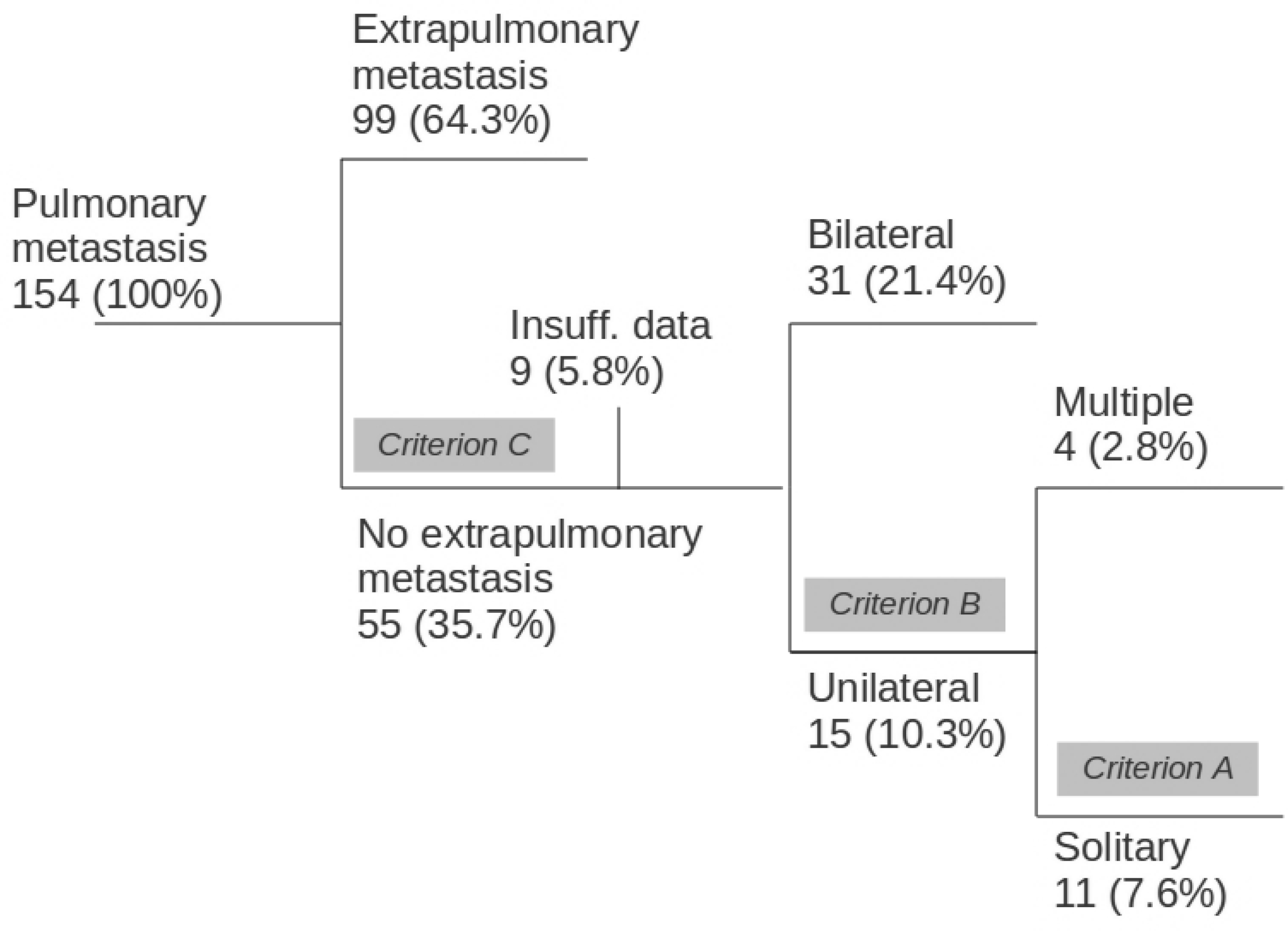
Schematic diagram showing the different numbers of patients with SPM that could be potential candidates for metastasectomy according to our eligibility criteria A–C, which were based on recent publications (see text for details). Potential resectability was 7.6% for patients with solitary SPM (criterion A), 10.3% for unilateral SPMs (criterion B), and 35% for patients with multiple bilateral SPMs but without any extrathoracic metastases (criterion C).
Eleven patients had solitary SPM (Table 3). Gender distribution and age were comparable to those in other SPM patients, and all patients were in good physical condition (ASA score 1–3) and had no major underlying diseases. Thus, all of them were deemed potentially eligible for surgical removal according to criterion A. The same was true for the 15 eligible patients according to criterion B. No extrapulmonary metastases were found in 55 patients, and these could theoretically have been operated on according to criterion C. (Fig. 1)
Clinicopathological information on RCC patients with solitary SPM in Iceland, 1971–205. All 11 patients were eligible for metastasectomy according to criterion A (see text for details)
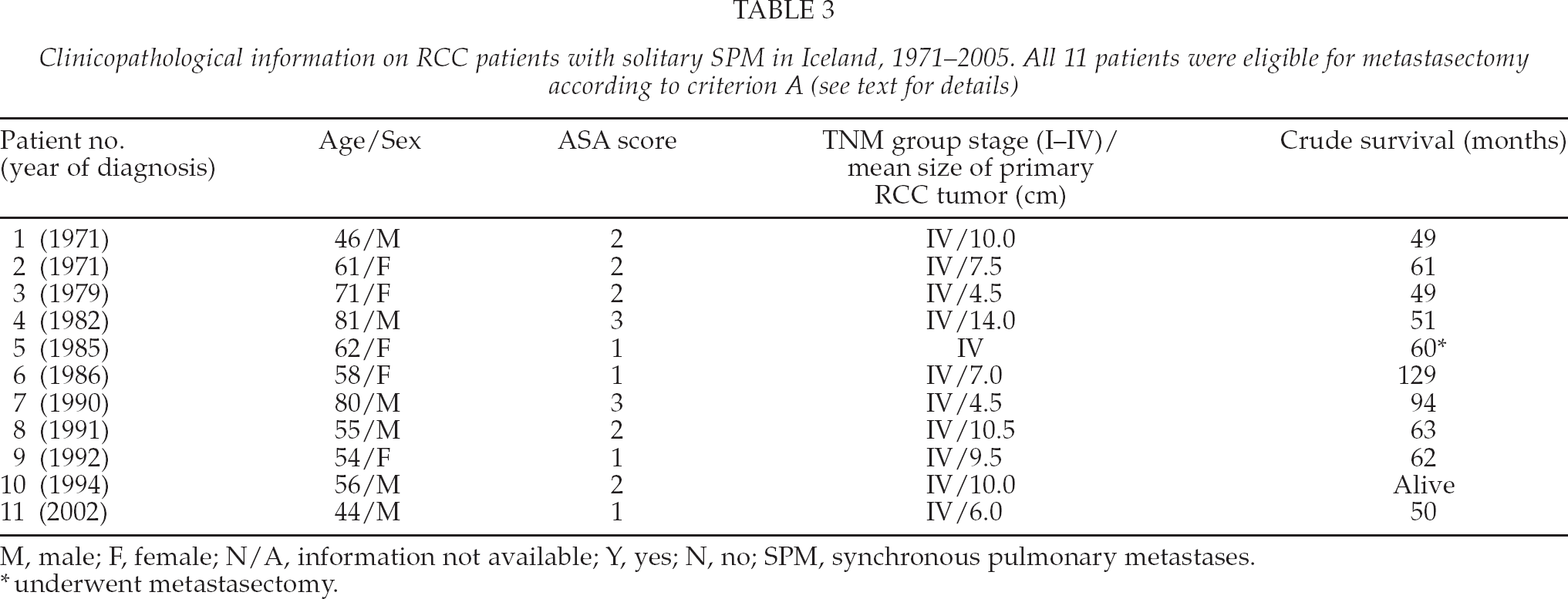
M, male; F, female; N/A, information not available; Y, yes; N, no; SPM, synchronous pulmonary metastases.
underwent metastasectomy.
Only one patient underwent pulmonary metastasectomy during the study period (in 1986). This patient had a solitary SPM and underwent resection one month after nephrectomy (Table 3). The other 10 patients with a solitary SPM were treated conservatively, and none of them received further treatment such as chemotherapy or radiotherapy.
Figure 2 shows a Kaplan-Meier analysis of estimated survival for the different subgroups of the patient cohort. Disease-specific survival at five years was 27.2% for patients with solitary SPM, 12.7% for patients with SPMs confined to the lungs, 7.1% for all patients with metastases including SPMs, and 12.0% for patients with extrathoracic metastases. The difference in survival between all four groups was not significant (log-rank test, p = 0.33).
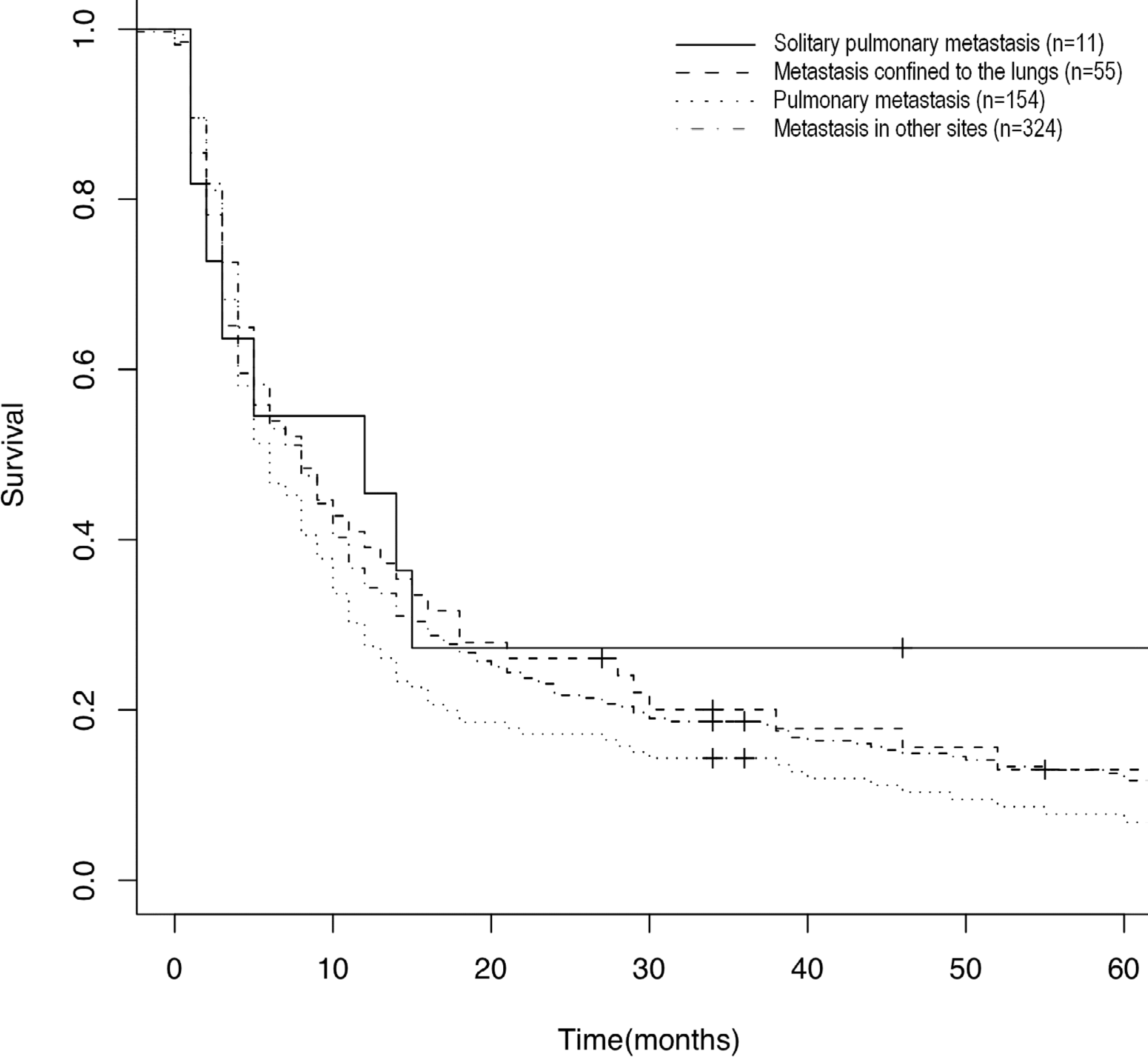
Five-year disease-specific survival for different groups of RCC patients with metastases. Survival was not significantly different between patients with solitary SPM (n = 11), those with SPMs confined to the lungs (n = 55), those with SPMs (n = 154), and those with metastasis at other sites (n = 324); log-rank test (p = 0.33).
DISCUSSION
In this nationwide study, SPMs were found in 16.9% of RCC patients at first diagnosis. Furthermore, our results show that one third of the SPMs were confined to the lungs and that one fifth of the patients had solitary SPMs.
Only one patient with SPM was operated on in the present study. Thus, it appears that a significant number of RCC patients in Iceland with SPM have not been offered pulmonary metastasectomy as a curative treatment option. This is important, since pulmonary resection for RCC metastases is a safe procedure (13, 15, 20). However, it must be remembered that the indications for metastasectomy were not well defined during the first half of the 35-year study period. Furthermore, the benefits of metastasectomy were poorly defined until the last decade of the study.
On the other hand, this cohort offers a unique and unselected group of patients that gives us valuable information on long-term survival without metastasectomy, and it may help us to estimate the impact of pulmonary metastasectomy in synchronous disease.
To evaluate potential resectability retrospectively, we defined criteria based on recent publications. This was necessary, as no formal guidelines on pulmonary metastasectomy for RCC have been published. Criterion A covered 7.6% of the RCC cohort, all of them with solitary SPM, that would theoretically have the greatest benefit of surgery (10, 12, 20). Criterion B covered four additional patients, or 10.3% of the RCC patients (3, 14). Finally, criterion C covered one third of the RCC patients with multiple SPMs but no extrathoracic metastases (9, 13, 15). In most studies, the latter category of patients are not believed to be candidates for metastasectomy, but in the recent study by Kanzaki et al. five-year disease-specific survival of up to 47% was achieved in this cohort of patients (20). It should be remembered that these criteria are solely based on retrospective studies and they are therefore subject to selection bias. Furthermore, when comparing studies, indications for metastasectomy can differ between institutions.
Our cohort only included patients with synchronous (and not metachronous) metastases. In Iceland, more than 20 patients have been operated on with pulmonary metastasectomy since 1984, all of them except one with metachronous metastases. In that study, survival for the single patient with SPM who underwent metastasectomy was 60 months, but for the other patients with metachronous metastasis, 29% were alive after five years (22).
Compared to unoperated patients with metastatic disease, selected patients treated with pulmonary metastasectomy have more favorable survival: several recent reports have given survival figures exceeding 50%, especially if disease-free interval is long (10, 13, 15,16). In a study by Pfannschmidt et al. (13) on 191 patients after pulmonary metastasectomy, median survival for synchronous disease (n = 50) was significantly less than for metachronous disease (n = 141) (median 20.0 months vs. 41.5 months). In our study, the overall group of patients with synchronous disease who were eligible for surgery showed a median survival of 10.0 months (± 2.0 months). This supports the necessity for critical patient selection for surgery in synchronous metastatic disease, preferably based on established prognostic parameters.
Even so, poor outcome for patients with untreated metastatic RCC disease has been documented in numerous studies, with survival at five years ranging from 0% to 11% (3, 4). Comparison of outcome between these groups of patients with RCC metastases is complex, however, since those who undergo surgery rarely have multiple organ metastases or diffuse pulmonary metastases. Thus, patient selection is a problem when interpreting surgical series on metastasectomy (23). Because younger and fitter patients are more likely to be referred for surgery, potential selection bias could favor the outcome of these treatments. The survival gain with resectable metastases could therefore be more related to the resectability and good performance status of the patient rather than to the resection itself. Randomized studies of pulmonary metastasectomy are certainly needed; however, such trials comparing surgical resection with no surgery or medical therapy have not been conducted.
Immunotherapy, such as the administration of recombinant human interleukin-2 or interferon-α in metastatic RCC has limited the overall response rate (11). Novel agents such as tyrosine kinase inhibitors (TKIs) have generated a certain amount of optimism. However, relatively few patients appear to achieve complete remission with TKIs and most of them eventually experience disease progression (18). During the last few years, there has been an increase in the availability and use of cryotherapy, radio-frequency therapy, and microwave therapy for metastatic RCCs. These procedures can be performed percutaneously without laparotomy, and although not as widely used as for liver metastases, there is continued interest in their use for pulmonary RCC metastases. In the study by Huo et al. (24), the use of ablations in these patients was regarded as an alternative tumor control, particularly in selected patients with multiple small lesions that were not suitable for pulmonary resection. In the present study, very few patients received interferon therapy following renal resection. Furthermore, TKIs and cryotherapy were first introduced in Iceland for the treatment of metastatic RCC after this study had ended. Future studies should clarify the indications for surgery in these patients and include the new treatment options. Until then, pulmonary metastasectomy appears to be the best curative treatment and should be offered to selected patients. The five-year survival was comparable for patients with solitary SPM, SPMs confined to the lungs, and patients with extrathoracic metastases. This was somewhat surprising, especially regarding patients with solitary SPM. One possible explanation could be our limited number of patients with solitary nodules, but it could also reflect the possible missed survival gain in these patients because metastasectomy was not performed.
This study had some limitations, including its retrospective design and the relatively small number of patients. The patients were treated over two decades, during which radiological modalities have changed. Thus, extrapulmonary metastases may have been underdiagnosed during the first years of the study. The strengths of the study, however, are is its nationwide design, minimizing selection bias, and the long and 100% complete follow-up with accurate survival data. Furthermore, the patients were identified independently using three different registries and operations performed in a single center, reducing the possibility that cases would missed.
In conclusion, our results show that at the time of diagnosis, 17% of RCC patients had SPMs and a significant number of these patients either had unilateral or solitary SPMs that are often resectable. Thus, it appears that although the value of pulmonary metastasectomy in RCC is still under debate, many RCC patients with suitable pulmonary nodules can be offered this treatment modality.
Footnotes
ACKNOWLEDGEMENTS
Thanks to Gunnhildur Johannsdottir for help with patient information. This study was supported by the Landspitali University Hospital Scientific Foundation and the Memorial Foundation of Bergthora Magnusdottir and Jakob Bjarnason, Reykjavik, Iceland.