
Abstract
Objectives:
This study was planned to evaluate the prognostic impact of end-stage renal disease (ESRD) in patients with critical leg ischemia (CLI) undergoing infrainguinal revascularization.
Materials and Methods:
1425 patients who underwent infrainguinal revascularization for CLI were the subjects of the present analysis. Ninety-five patients had ESRD (eGFR < 15 ml/min/m2), and of them 66 (70%) underwent percutaneous transluminal angioplasty and 29 (30%) underwent bypass surgery.
Results:
ESRD patients had significantly lower overall survival (at 3-year, 27.1% vs. 59.7%, p < 0.0001), leg salvage (at 3-year, 57.7% vs. 83.0%, p<0.0001), and amputation free survival (at 3-year, 16.2% vs. 52.9%, p < 0.0001) than patients with no or less severe renal failure. The difference in survival was even greater between 86 one-to-one propensity matched pairs (at 3-year, 23.1% vs. 67.3%, p < 0.0001). ESRD was an independent predictor of all-cause mortality (RR 2.46, 95%CI 1.85–3.26).
Logistic regression showed that age ≥ 75 years was the only independent predictor of 1-year all-cause mortality (OR 4.92, 95%CI 1.32–18.36). Classification and regression tree analysis showed that age ≥ 75 years and, among younger patients, bypass surgery for leg ulcer and gangrene were associated with significantly higher 1-year mortality.
Conclusions:
Lower limb revascularization in patients with CLI and end-stage renal failure is associated with favourable leg salvage. However, these patients have a very poor survival and this may jeopardize any attempt of revascularization. Further studies are needed to identify ESRD patients with acceptable life expectancy and who may benefit from lower limb revascularization.
Keywords
INTRODUCTION
In the nineties, a number of small series provided evidence on poor survival after lower limb revascularization in patients with both critical leg ischemia and end-stage renal failure (ESRD) (1 –3). This issue has been investigated in an increasing number of studies confirming the poor life expectancy of these patients. Indeed, a recent meta-analysis on infrainguinal bypass surgery in ESRD patients showed a 5-year pooled primary patency of 50%, secondary patency of 51%, limb salvage of 67% and survival of 23% (4). Similar results have been reported after endovascular revascularization (5).
These findings suggest that a strict preoperative selection is indicated as successful attempts to leg salvage may be contradicted by poor survival. Herein we evaluated the results of our recent experience in infrainguinal revascularization for CLI in ESRD patients in order to assess the benefits and limits of an aggressive revascularization policy in these very high risk patients.
MATERIAL AND METHODS
A total of 2054 revascularizations were done due to CLI at the Department of Vascular Surgery, Helsinki University Central Hospital, Helsinki, Finland, between 2000 and 2007. Complete data were available in 1425 cases in whom single and unilateral revascularization procedure was done. These procedures were the subjects of the present analysis. All cases and angiographies were reviewed and discussed for decision making at the daily integrated vascular meetings of vascular surgeons and interventional radiologists. Clinical characteristics, operative data and immediate postoperative outcome data of these patients were prospectively collected in our institutional database and scrutinized retrospectively (Table 1). Dates and causes of death were retrieved from Finnish national registry (Statistics Finland). Data on late major lower amputation and re-interventions have been completed retrospectively from files of National Research and Development Centre for Health and Welfare. The study protocol was approved by the Institutional Review Board of Helsinki University Central Hospital, Finland (Department of Surgery).
Baseline characteristics and operative data on patients who underwent infrainguinal revascularization for critical limb ischemia. Relative risks and p-values refer to any early or late all-cause mortality.
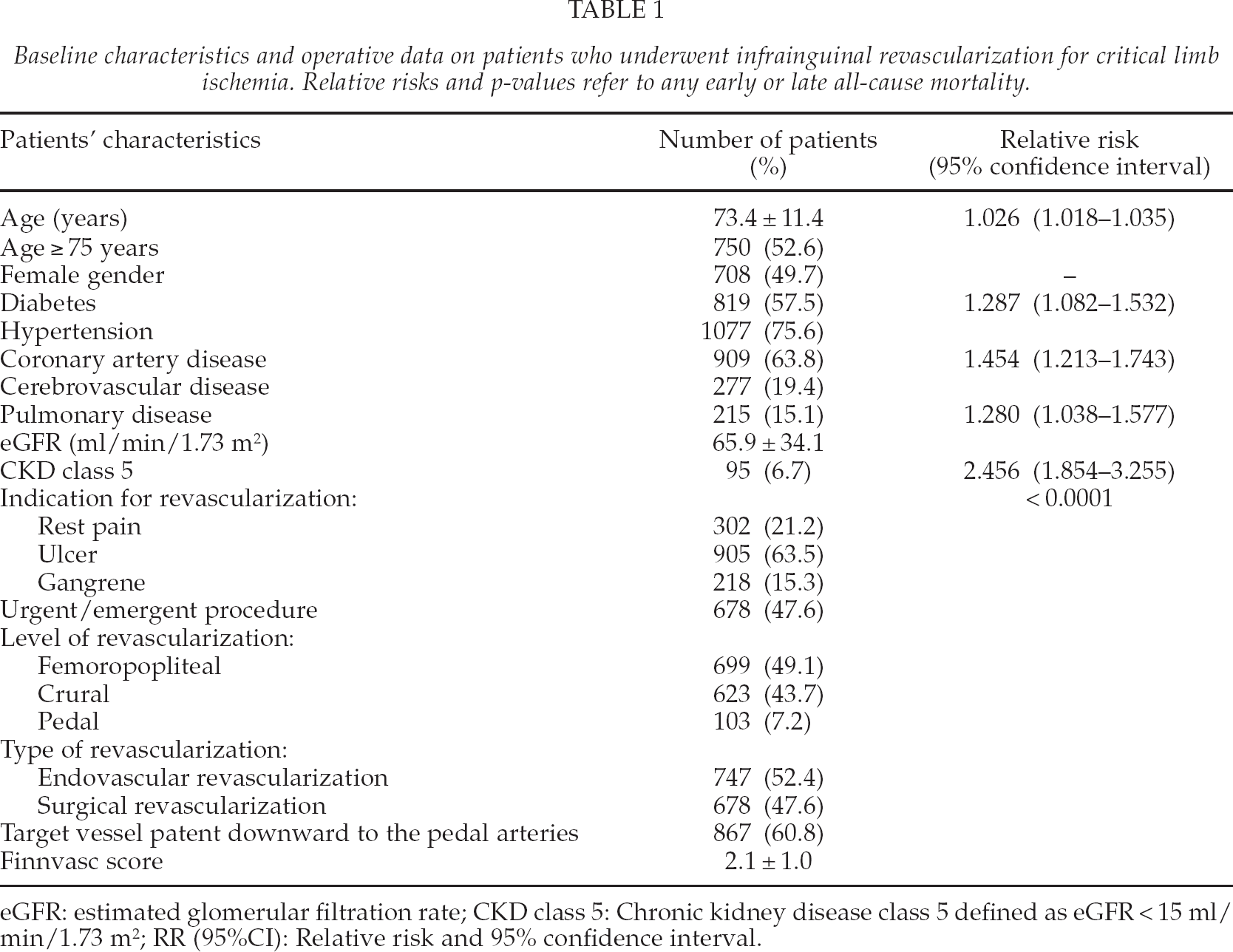
eGFR: estimated glomerular filtration rate; CKD class 5: Chronic kidney disease class 5 defined as eGFR < 15 ml/min/1.73 m2; RR (95%CI): Relative risk and 95% confidence interval.
Preoperative estimated glomerular filtration rate (eGFR) was calculated according to the Modification of Diet in Renal Disease study equation (Levey). Severity of renal failure was classified according to the chronic kidney disease (CKD) classification (6). For the purpose of this study we evaluated patients with eGFR < 15 ml/min/m2 with patients with no or less severe renal failure, i.e. CKD classes 1–4. Operative risk was estimated by the Finnvasc score (7).
ENDOVASCULAR REVASCULARIZATION
Endovascular intervention was performed in 747 cases. Balloon angioplasty was the method of choice for endovascular approach. The use of stents was reserved for cases in which there was a flow-limiting dissection or a significant residual stenosis after balloon angioplasty. A stent was placed in 3% of the primary interventions. Intra-arterial heparin (5000 I.U.) was routinely administered just before the endovascular procedure.
After successful endovascular intervention, patients received 300 mg of clopidogrel orally and were maintained on 75 mg/day for at least 1 month, except for those on continued anticoagulation already before revascularization. In addition, patients were treated with 100 mg aspirin once a day indefinitely. This medication strategy became routine in 2001 as previously patients received postoperatively only aspirin. Routine follow-up included one clinical examination at one month after the procedure. Duplex-Doppler ultrasound (DD) scan was done when needed.
SURGICAL REVASCULARIZATION
Surgical revascularization was performed in 678 cases. Saphenous vein graft was used in 606 cases and, among these, reversed vein grafts were used in 165 cases (27.2%). A prosthetic graft had to be utilized in 72 cases (10.6%) because of the lack of suitable veins. Patients received low molecular weight heparin during their post-operative hospital stay in addition to 100 mg of aspirin orally which was continued indefinitely. Routine surveillance included a clinical examination, ankle-brachial-index measurement and DD scan at 1, 6 and 12 months.
ANGIOGRAPHIC STATUS OF RUNOFF ARTERIES
Periprocedural angiographies were retrospectively reviewed by three authors (MV, KH, MK) and the angiographic status of the runoff vessels was quantified at the site of angioplasty/distal anastomosis downward according to the SVS/ISCVS criteria (8).
OUTCOME MEASURES
Overall survival, amputation and amputation-free survival were the outcome measures of this study. Since all-cause mortality risk in patients with end-stage renal failure was extremely high and affected amputation free survival, all-cause mortality was considered the main outcome measure in the present analysis.
STATISTICAL ANALYSIS
Statistical analysis was performed using a SPSS statistical software (SPSS v. 16.0.1, SPSS Inc., Chicago, Ill., USA). Continuous variables are reported as the mean ± standard deviation. Pearson's chi square test, Fisher exact test, and Mann-Whitney test were used for univariate analysis. Long-term outcome was assessed by the Kaplan-Meier's method with the log-rank test and the Cox regression method. Only variables with a p < 0.050 in univariate analysis were included in the Cox regression model.
Patients with ESRD were found to significantly differ from those without or with less severe renal failure in terms of baseline and operative characteristics. Therefore, logistic regression with backward selection was used to estimate the risk of being in the CKD class 5 group or in the CKD classes 1–4 group. Hosmer-Lemeshow's test was used to assess the regression model fit. Variables listed in Table 1 and having a p < 0.20 in univariate analysis were included in the regression model. Receiver operating characteristic (ROC) curve analysis was used to estimate the area under the curve of the model predicting the probability of being included in one of these study groups. The calculated propensity score was employed for one-to-one matching as well as to adjust for other variables in estimating their impact on the postoperative outcome. We did not perform analysis in propensity score percentiles because of the relatively small number of patients. One-to-one propensity score matching between study groups was performed according to a difference in the logit of propensity score of less than 0.018 between each patient pairs in the study groups. Such a calibre width was equal to 0.2 of the standard deviation of the logit of the herein calculated propensity score (0.09) (9). Outcome in the propensity matched pairs was evaluated by Kaplan-Meier's methods as well as Cox regression method. Beside logistic regression, classification and regression tree (CART) analysis has been performed to identify independent risk factors for 1-year all-cause mortality. Validation of the classification tree procedure was assessed by cross validation through 25 folds. The minimum number of patients for parent node was set to 15 and the minimum for child node was 5. Receiver operating characteristic (ROC) curve analysis was used to estimate the area under the curve of probabilities values estimated by logistic regression and CART analysis models in predicting 1-year all-cause mortality. A p < 0.050 was considered statistically significant.
RESULTS
The mean length of the follow-up was 2.4 ± 2.2 years. Overall survival rates were significantly lower in the CKD class 5 group (Table 2, Fig. 1).
Baseline characteristics and operative data on patients with and without end-stage renal failure who underwent infrainguinal revascularization for critical limb ischemia in the overall population and in propensity matched pairs.
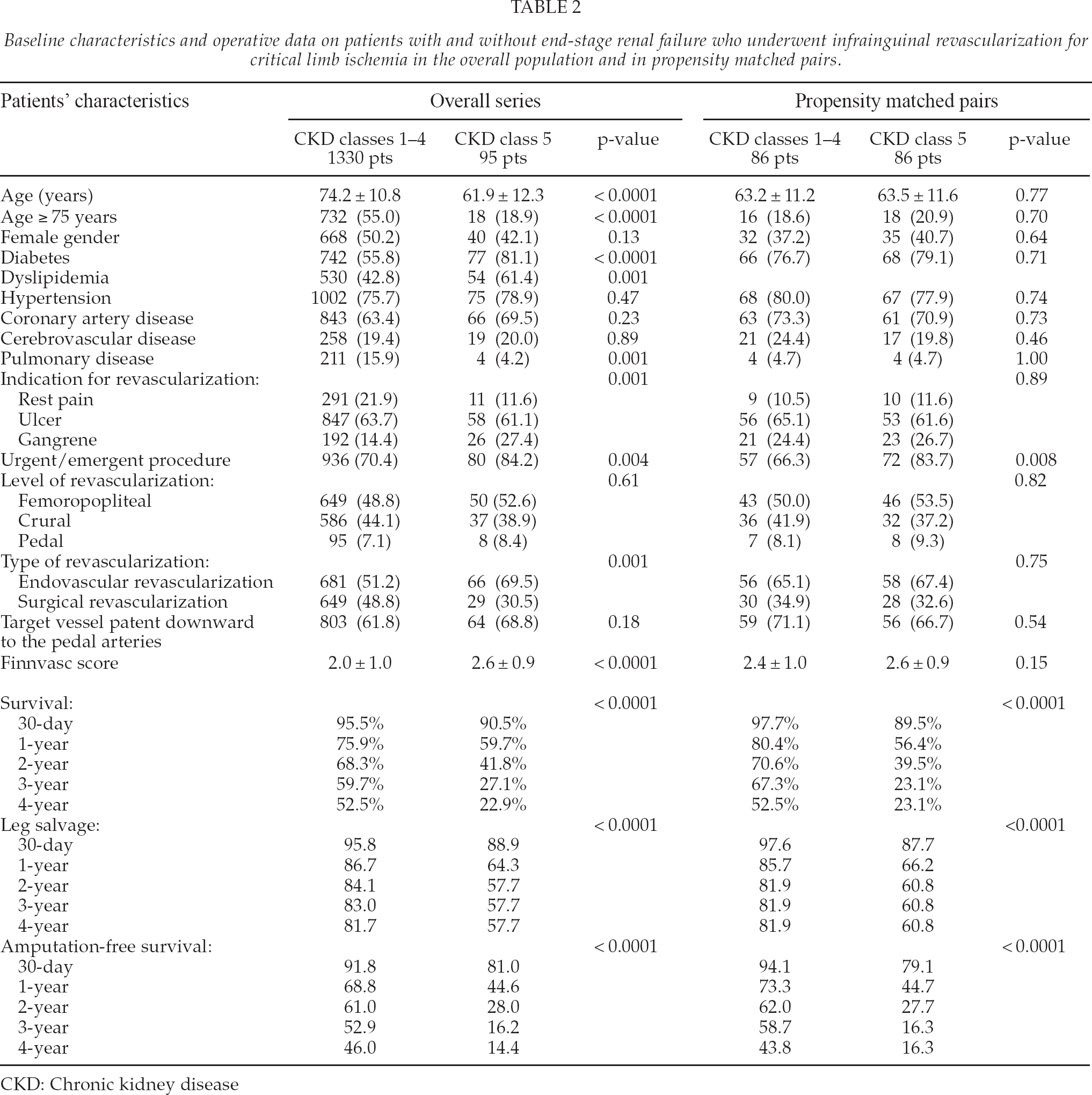
CKD: Chronic kidney disease
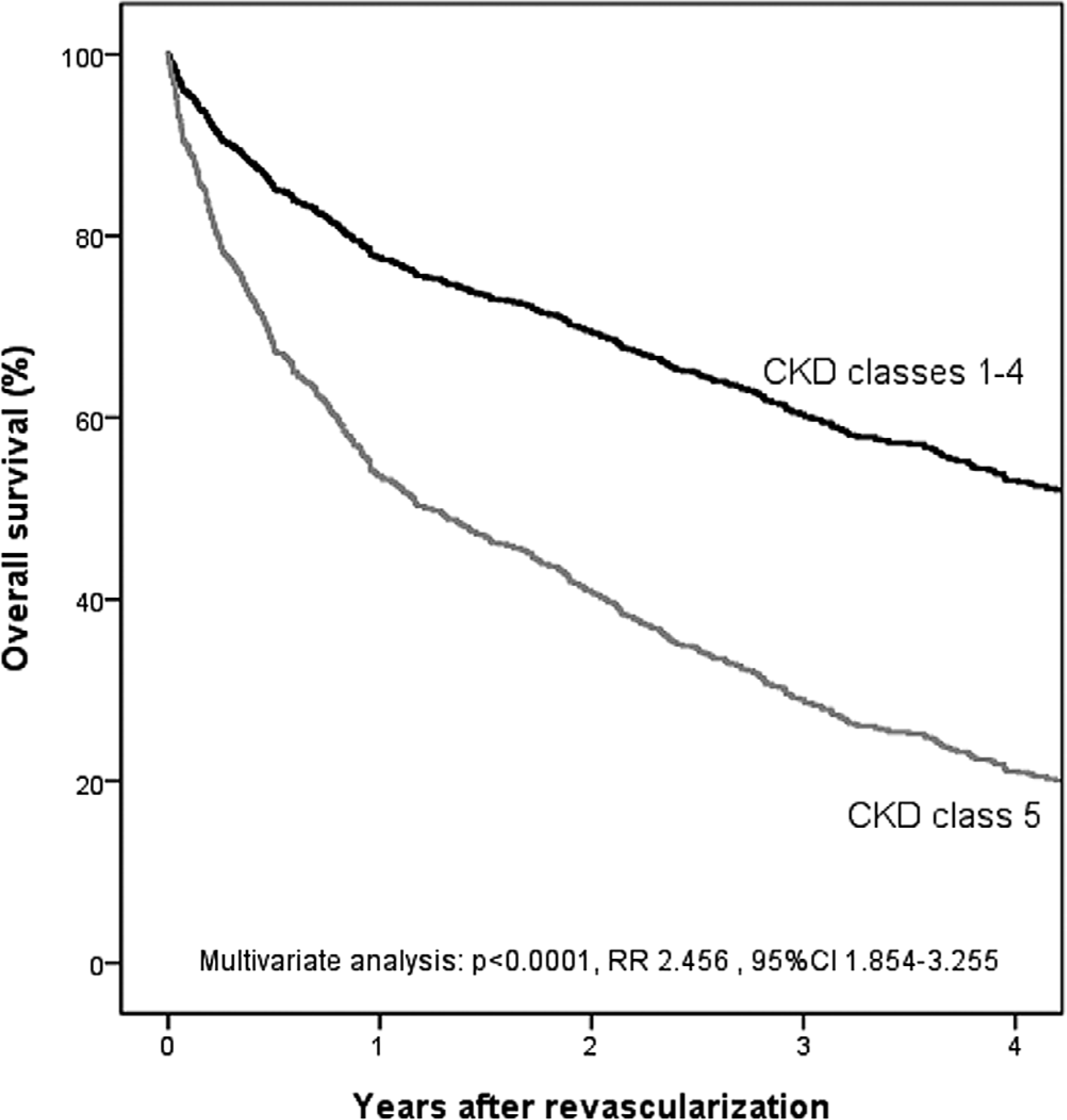
Overall survival according to Cox regression analysis in patients with end-stage renal disease (CKD class 5) and patients with no or less severe renal failure (CKD class 1–4).
Independent predictors of early and late all-cause mortality are summarized in Table 1. Cox regression analysis failed to identify any predictor of early and late mortality in patients with CKD class 5 disease. Since survival rate in these patients was rather low at 1-year follow-up, we decided to further analyze all-cause mortality at this interval. Logistic regression evaluating 81 patients with a possible follow-up of at least one year and including age ≥ 75 year, cerebrovascular disease, leg ulcer or gangrene vs. rest pain and treatment modality (PTA vs. bypass surgery), showed that age ≥ 75 years was the only independent predictor of 1-year all-cause mortality (p = 0.018, OR 4.919, 95%CI 1.318–18.358). When the same variables were considered for CART analysis, age ≥ 75 years, leg ulcer and gangrene as well as bypass surgery were associated with higher 1-year all-cause mortality (Fig. 2). Area under the ROC curve was 0.678, 95% CI 0.553–804.
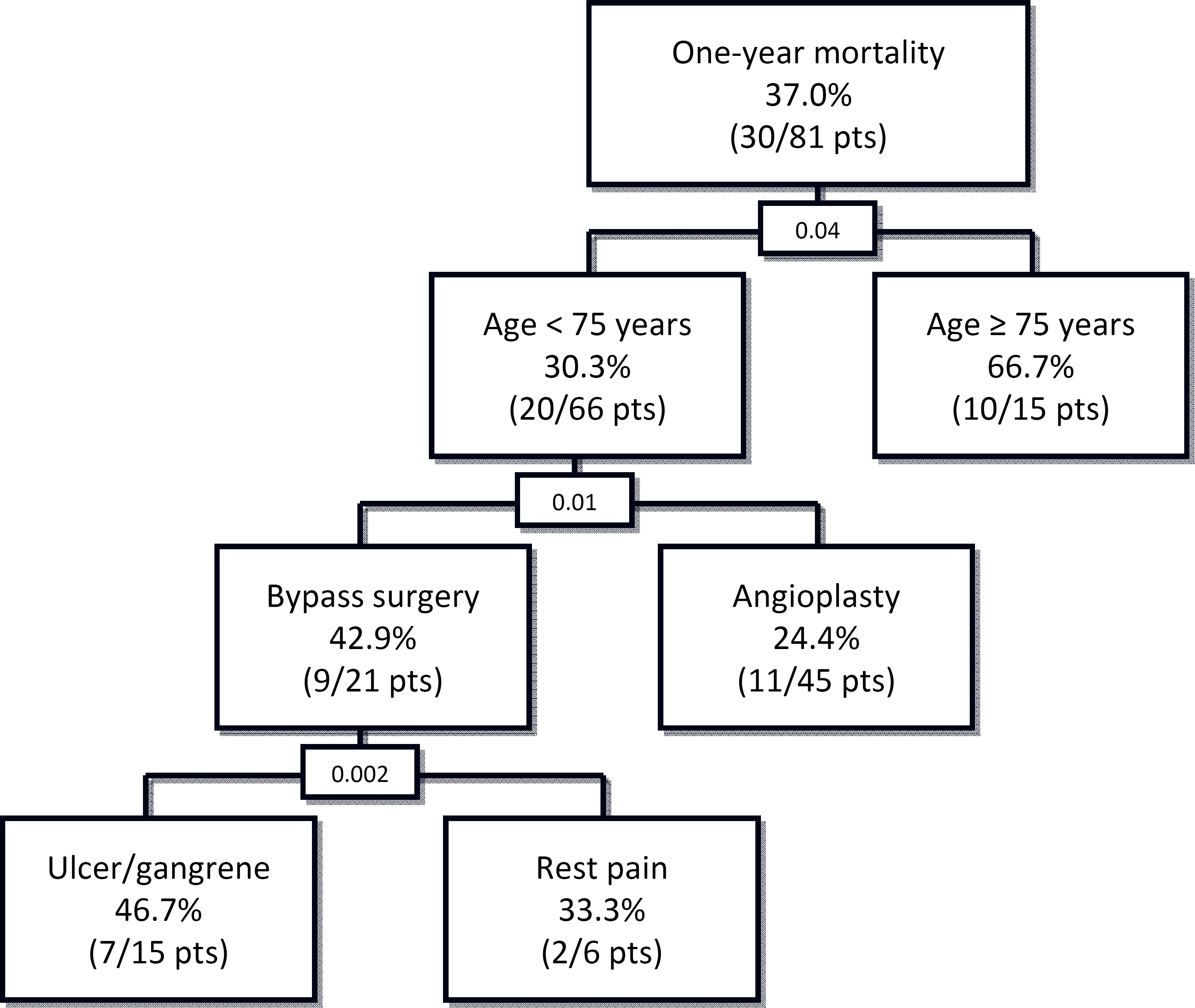
Classification and regression tree for identification of predictors of 1-year mortality among 81 patients with end-stage renal disease who underwent infrainguinal revascularization for critical leg ischemia.
PROPENSITY SCORE ANALYSIS
Age (β-coefficient −0.087), diabetes (β-coefficient 0.500), pulmonary disease (β-coefficient −1.398), treatment method (PTA vs. bypass surgery, β-coefficient −0.817), coronary artery disease (β-coefficient 0.829) and foot gangrene (β-coefficient 0.699) significantly differed at logistic regression between CKD class 5 group and CKD classes 1–4 group (constant β-coefficient 2.699, Hosmer-Lemeshow's test. p = 0.686). The obtained propensity score had an area under the ROC curve of 0.818 (95% C.I. 0.773–0.862, S.E. 0.023, p < 0.0001).
When adjusted for this propensity score, CKD class 5 was associated with significantly higher risk of all-cause mortality (p < 0.0001, RR 2.468, 95% 1.853– 3.287), major amputation (p < 0.0001, RR 2.853, 95% 1.841–4.422), and combined all-cause mortality or major amputation (p < 0.0001, RR 2.578, 95% 1.970–3.373).
One-to-one propensity score matching resulted in 86 pairs of patients with similar baseline and operative characteristics (Table 2). In these propensity matched pairs 4-year overall survival of patients with CKD class 5 was 23.1% whereas it was 52.5% in patients with no or less severe renal failure Log-rank: p < 0.0001. Similarly, also leg salvage and amputation free survival rates were significantly lower in patients with ESRD.
DISCUSSION
Lower limb revascularization for CLI in ESRD patients is associated with rather favourable limb salvage rates (4). In fact, despite the well recognized significant risk of major amputation despite patent graft in these patients (10, 11), pooled limb salvage rates at 5 year was 66% (4). Furthermore, a recent systematic review reported a 1-year limb salvage of 70% in survivors with ischemic diabetic ulcers (12). The herein observed limb salvage rate of 61% at 4 years confirms that, when feasible, endovascular and surgical revascularization can be highly successful in achieving limb salvage in these patients. However, success of revascularization is contradicted by high mortality rates.
A recent meta-analysis (13) evaluating the impact of kidney function on the outcome after surgery indicated that the relative risk of 30-day mortality per 10 ml/min/m2 lower eGFR at baseline was 1.27 (95%CI 1.23–1.31). Such a risk increased dramatically along with CKD classes (CKD class 3: RR 1.62; CKD class 4: RR 2.85; CKD class 5: RR 3.75). Indeed, such a mortality risk is particularly high after lower limb revascularization as pooled analysis of surgical series showed a 30-day mortality rate of 5% (4), and some more recent studies including endovascular treatment reported immediate mortality rates of about 10% (14, 15). Even more dramatic is the increased risk of late mortality in these patients, which suggests that CLI is a malignant condition in ESRD patients. Interestingly, the pooled analysis by Albers and colleagues (4) indicates that 3-year survival of ESRD patients undergoing bypass surgery for CLI (41%) was similar to that of 13 085 ESRD patients who underwent coronary artery bypass surgery (42%) (16). These findings indicate that clinically severe atherosclerosis is a major determinant of very poor survival in ESRD patients.
The present results may be partly due to other severe comorbidities usually observed in ESRD. Indeed, Table 2 shows that ESRD patients had higher prevalence of important risk factors as also suggested by higher Finnvasc score. Because of this, we have adjusted ESRD with other covariates at logistic regression and Cox regression analysis (Fig. 1). Furthermore, with the help of a propensity score, we obtained two groups of patients with and without ESRD with similar characteristics (other than the severity of renal failure). Comparative analysis of these propensity matched pairs suggested that survival of ESRD patients with CLI could be somewhat worse than that estimated by usual statistical methods.
Early referral, adequate treatment of tissue loss and complete revascularization are essentials in the management of these patients (17). However, current evidence suggests that life expectancy of ESRD patients with CLI should be scrutinized before any decision to revascularize. In this sense, clinicians do not have enough data yet to support the decision whether to revascularize or not. The small size of reported series and the significant number of deaths may prevent the identification of risk factors associated with poor survival. Herein, CART analysis identified patient's age ≥ 75 years and, among younger patients, bypass surgery for leg ulcer and gangrene as significant determinants of increased 1-year mortality. Advanced age can intuitively contraindicate lower limb revascularization in presence of ESRD. Poor survival of patients requiring bypass surgery for CLI and tissue loss may indicate the severity of peripheral vascular disease and poor control of systemic diseases. However, these findings might be biased by the relatively small number of patients in this study evaluated. Therefore, further studies are certainly needed to better identify prognostic indicators in this fragile patient population.
The retrospective nature is a limitation of this study. However, most of the data herein evaluated were prospectively collected. Furthermore, a number of patients were excluded from this analysis because of lack of data, particularly on preoperative creatinine levels. Even if this might introduce a significant bias, we believe that using propensity score analysis might have reduced this potential flaw and provided reliable results because it resulted in two rather large study groups with similar baseline characteristics.
In conclusion, lower limb revascularization in patients with CLI and end-stage renal failure is associated with favourable leg salvage. However, these patients have a very poor survival, which may threaten any attempt of revascularization. Further studies are needed to identify subgroups of patients with reasonably good life expectancy and who may benefit from lower limb revascularization.