
Abstract
Aim
Decisions made by social work professionals determine the scope and nature of the help clients receive. These decisions rest on professional judgement, making it essential to understand the foundations of such judgement to grasp social work practice. This qualitative study explores professional decision-making and practice among Danish addiction counsellors working in outpatient treatment for alcohol use disorders. The aim was to examine what the counsellors base their professional judgements on and the reasoning that informs their decisions.
Methods
Utilizing the vignette method, we conducted semi-structured interviews with 12 addiction counsellors. Interviews were analyzed using thematic analysis.
Results
Our findings show how the counsellors base their professional judgements and decisions on knowledge and values, respectively. We identified differences among counsellors in how values were understood and applied. Several values lacked clear definitions and appeared in varying or subtly distinct forms.
Conclusions
The study underscores the need to clarify the values guiding social workers’ judgements and decisions. Values shape how knowledge is used, making their clarification essential for evidence-based practice. Without such clarity, value-based practice becomes meaningless, and values cannot effectively guide professionals in their clinical work.
Keywords
Introduction
Decision-making is a fundamental element of social work (O'Sullivan, 2010). The decisions made by social work professionals are crucial in terms of the extent and type of help that clients are offered. This applies to all areas within social work, from public welfare and health care to aging, mental health, child welfare, substance use, etc.
Efforts to build an evidence-based practice have been increasing over the last 20 years (Bellamy et al., 2013; McNeece & Thyer, 2004; Trinder, 2000). This focus has come to play a significant role within the field of social work (Björk & Björk, 2019; Gray et al., 2009; Juul, 2018; Krogstrup, 2018), including the treatment for alcohol use disorders (AUD). Alcohol treatment increasingly relies on scientific knowledge about interventions and their effects. The underlying assumption is that producing and disseminating objective knowledge to practitioners will promote evidence-based practice and thereby improve treatment outcomes. This evidence-movement in social work is built on a belief in ensuring quality through scientific methods (Gray et al., 2009; Magill, 2006; Rosen et al., 2003). The same belief is seen within policy. In Denmark, an explicit objective for the national health authorities is to provide a uniform, evidence-based and quality assured treatment (Danish Health Authorities, 2018, 2019b). This objective is, among other things, pursued by formulating clinical guidelines for the treatment of AUD (Danish Health Authorities, 2018). Similar guidelines are now implemented in several countries globally (Haber & Riordan, 2021; National Institute for Health & Clinical Excellence [NICE], 2011; Socialstyrelsen, 2019). In Sweden, the promotion of evidence-based practice has been pursued from highest political level and implementation of a guideline model has been part of an explicit national strategy (Bergmark et al., 2012; Björk & Björk, 2019).
However, while guidelines provide knowledge about interventions and their effect, as well as recommendations for decisions to make and interventions to use, guidelines do not tell the social work professionals how to make the required decisions and judgements. When applying guidelines to social work practice, these are subject to interpretation by the practitioners. Wallander (2012) points out how “… several conditions of social work practice ‘facilitate’ or make room for the existence of such variation in judgements” (Wallander, 2012). Despite guidelines, a room for discretion still exists in the specific context (Evans & Harris, 2004).
As a consequence, the professional judgment and decision-making of social work professionals are central to the delivery of social work services. The findings from previous research underscore the importance of focusing on this aspect of practice across different social work disciplines.
A Danish study examined the use of decision-making tools and their influence on caseworkers’ room for discretion (Høybye-Mortensen, 2015). Despite the use of standardized assessment measures, a wide variation in the professional judgements was found to exist. Swedish studies of health care professionals’ and social workers’ judgements and decisions also found differences to exist among the professionals (Blomqvist & Wallander, 2004; Wallander & Blomqvist, 2009). Rather substantial disagreements and differences among the professionals were reported, both regarding the choice of intervention and the justification of the decision. Wallander & Blomqvist (2009) found, among others, that treatment recommendations for problem substance users varied depending on both the ideological convictions and the work position of the individual social worker, but they also note that “… a substantial amount of between-respondents variance was left unexplained” (Wallander & Blomqvist, 2009). In a study by Mosteiro et al. (2018), social workers, social educators and psychologists were presented to a case vignette from the child protection system, and their arguments and decisions regarding the case were investigated. The study showed significant differences among the professionals with regards to their conclusions and decisions to remove the child from the family or not. These differences in decisions were seen despite an overall agreement among the professionals as to which criteria to consider when making the decisions. Few Danish studies have also examined the opinions of social work professionals (Ejrnæs, 2006; Ejrnæs & Monrad, 2010, 2013). This research also revealed big differences in opinions and judgements among the professionals. Differences that showed to be hidden or “latent” because the professionals themselves were not aware of them (Ejrnæs, 2006; Ejrnæs & Monrad, 2010).
Overall, this points to a diversity in the professional judgement and decision-making, both within and across different social work disciplines, underscoring the importance of considering these aspects of social work practice. The opinions and judgements influence how clients and guidelines are acted upon. As such, with an aim of providing a uniform, evidence-based treatment in practice, the opinions of the addiction counsellors are central.
Previous studies have focused on the presence and degree of differences among social work professionals (Ejrnæs, 2006; Ejrnæs & Monrad, 2010). Focus has also been paid to welfare professionals as political decision-makers (May & Winter, 2009) and on the professionals’ ways of acting upon their judgements (Dreier & Østergaard, 2015). Other studies have focused on heuristics (i.e., how social workers use short cuts to reduce complexity when making judgements and decisions) (Kahneman & Klein, 2009; Taylor, 2016). Quantitative methods have also been used to identify the factors that influence the judgements and decisions of professionals. For example, factorial survey designs have been applied to investigate how social workers weigh specific information about clients and whether specific individual characteristics of the social worker influence the judgements and decisions made (Wallander & Blomqvist, 2009). However, this approach has the limitation of not providing an explanation for the assumptions or specific use of knowledge.
Addiction counsellors are key actors in the delivery of an evidence-based and quality assured alcohol treatment. Providing treatment inevitably involves making professional judgements and decisions. To understand the diversity of these, a focus on the specific judgements must be expanded to include a focus on the reasoning that informs the decisions and the arguments used to justify them. Qualitative research aimed at exploring what professional judgements and decisions are based on, and at understanding the differences that exist is lacking.
Study aim
The present qualitative vignette study explores professional judgement and decision-making among addiction counsellors working in outpatient treatment for alcohol use disorders in Denmark. The aim of the study was to examine what the counsellors base their professional judgements on and to explore the reasoning that informs their decisions. The findings will be discussed from a discourse theoretical perspective.
Terminology
In the research of judgement and decision-making, a variety of concepts are used. Here, we follow the terminology often used within social work (research). The term “professional judgement” is thus used to refer to an individual (counsellor) considering the evidence about a client or a situation and reaching a conclusion or recommendation. The term “decision-making” is used to refer to a conscious process of the individual (counsellor) leading the individual to select a course of action from among two or more alternatives (Taylor, 2023). As such, professionals form their judgements prior to or while engaging in decision processes (Killick & Taylor, 2024).
Methods
For the present study we made use of two methodological tools: the vignette method and the qualitative interview.
The vignette method
Vignettes are, like case stories, short fictional stories or descriptions of hypothetical contexts, actions, and individuals (Finch, 1987). Thus, a vignette can be seen as a “snapshot” of a given situation (Hughes, 1998). Vignettes are constructed according to the researcher's interests and study objectives and are therefore usually fictive. However, vignettes typically describe situations that are likely to occur in real-life because the vignettes are intended to constitute realistic descriptions of the situations concerned. When using the vignette method, respondents are presented to one or more vignettes and invited to respond to the situations, persons, events, etc., outlined in them. The vignette method is particularly suitable in exploring opinions, judgements, understandings, values and interpretations in relation to a specific phenomenon or a specific situation (Ejrnæs & Monrad, 2012).
Construction and content of the vignettes for the present study
Two vignettes were created by the researchers (KHV and ASN). When constructing the vignettes, the researchers drew upon their own professional experiences within the alcohol treatment field. Furthermore, available statistical data from the alcohol treatment field (e.g., gender, age, years of problematic/harmful alcohol use prior to applying for treatment, somatic and psychiatric conditions related to AUDs) were used to ensure that the clients in the vignettes resembled clients encountered by the counsellors in their daily practice. The vignettes were also read through by an experienced addiction counsellor who contributed with feedback on wording, inclusion and exclusion of information, and the realism and relevance of the vignettes, as well as the clarification of the practice context.
Both vignettes described a situation where a client sought treatment at the public alcohol treatment services and had shown up for the introductory interview with a counsellor in the outpatient treatment facility. The client's life situation and alcohol problem were described, primarily through information provided by the client himself. Selected information about family, employment, housing, mental health, etc., was also included in the vignette, albeit the information differed in the two vignettes. One of the vignettes was constructed to portray a typical client appearing at the outpatient treatment facilities. The other vignette was constructed to portray a client who was more strained and with more complex problems, including possible psychiatric comorbidity.
The vignettes are presented in Appendix 1 (in Danish). English translations of the vignettes are available upon request from the corresponding author.
Recruitment
A purposive sample of outpatient treatment facilities was invited to participate. The purposive sampling strategy was based on the size of the municipalities in which the treatment facilities were located, the capacity of the treatment facilities and on whether the treatment facilities offered treatment for AUD only or for all substance use disorders (alcohol as well as other substances). These criteria were considered to ensure that the sample of counsellors were representative of the diversity in the outpatient treatment facilities across Denmark. A sample of 29 treatment facilities, covering the spectrum on these variables, was selected.
The treatment facilities were contacted via email, which briefly presented the research objectives and advertised for addiction counsellors willing to participate in an interview. The only inclusion criterion was for the participants to provide psychosocial treatment for AUD as a substantial part of their daily job.
Sample
In total, 13 addiction counsellors volunteered to participate and all met the inclusion criterion. One counsellor dropped out due to illness, leaving completed interviews with a total of 12 counsellors from 10 treatment facilities. A detailed overview of the characteristics of the participating counsellors is presented in Appendix 2.
All participants received information about the study and gave their verbal consent to participate prior to conduction of the interviews.
Data collection
Individual interviews
The vignettes were used in the qualitative interviews. The vignettes provided a situated context for the counsellors to respond to, and the interviews offered a platform for exploring the counsellors’ opinions in relation to the vignettes (Hughes, 1998). The interviews gave access to the individual counsellor's reflections and arguments, thereby providing an insight into the reasoning informing the judgements and decisions.
The interviews were semi-structured. The questions to the vignettes were constructed beforehand and served as the interview guide. The questions revolved around five topics: (1) the counsellor's understanding of the situation and the client's problems; (2) the counsellor's assessment of the client's need for treatment; (3) the counsellor's judgement regarding the content of treatment; (4) the treatment goals; and (5) the counsellor's opinion on what the professional in the vignette should do. The counsellor's responses were consistently met with an inquisitive exploration, and the counsellor was encouraged to elaborate on the reasons behind the opinions and judgements expressed.
The interview guide is presented in Appendix 3 (in Danish). An English translation of the interview guide is available upon request from the corresponding author.
Setting and conduct of interviews
All interviews were conducted online via video to create a uniform context for all interviews, with counsellors residing in different parts of the country. The interviews had a duration of approximately 1 h. Only the interviewer and the counsellor were present during the interview. The vignette was read aloud by KHV, whereafter the counsellor was asked to answer the pre-constructed questions as a point of departure. The procedure was repeated with the second vignette.
All interviews were recorded and transcribed verbatim by KHV. NVivo (https://lumivero.com/products/nvivo) was used to systematize and code the data.
Data analysis
The transcribed interviews were analyzed using thematic analysis (Braun & Clarke, 2006). The coding of data was data-driven with no predefined codes or themes. Codes were developed concurrently with the thorough reading of the transcripts (Kvale & Brinkmann, 2015). Following the study objectives, particular attention was paid to passages where the counsellors clearly expressed their opinions or judgements regarding the topic in focus.
The analysis of the data consisted of the following steps: (a) thoroughly reading the transcripts of all 12 interviews; (b) making initial notes and explorative comments; (c) generating and applying initial codes; (d) developing emergent themes and collating the coded data extracts within these themes; (e) refining the themes; searching for patterns and connections across themes, thereupon forming superordinate themes and subthemes; (f) re-reading and elaborating on the most potent subthemes, resulting in a number of subcategories for each subtheme; and (g) searching for patterns and connections across superordinate themes, subthemes and subcategories.
When presented to an attitude object (a specific topic of matter), the counsellors expressed their opinions and argued for their judgements or decisions. As part of the analysis, themes were developed for both the specific judgements or decisions and for the arguments and reasons expressed by the counsellors. However, our analytical focus was on the latter because the study objective was to examine the basis of the professional judgements and decisions, and not the specific decisions and their content.
Theoretical approach
Laclau & Mouffe (Howarth, 2005) belong to a social constructionist tradition, in which knowledge is perceived not as a reflection of reality but rather as socially constructed. The discourse theory developed by Laclau & Mouffe (Howarth, 2005) emphasizes how nothing can have a meaning independent of the discourses it is placed within (Howarth, 2005). Social meaning is relational, contextual and contingent, and, in particular, social structures are conceived as incomplete and open meaning systems. Laclau & Mouffe (Howarth, 2005) focus on how social actors construct meanings within these social structures (Howarth, 2005).
Laclau & Mouffe (Phillips, 2020) relate to a distinct poststructuralist discourse-analytic approach (Phillips, 2020). This implies the view that there is no one general system of meaning, but rather a number of discourses where meanings change from discourse to discourse.
In the present study, specifically the concepts of “floating signifiers” and “subject positions” from Laclau & Mouffe's discourse theory (Howarth, 2005; Laclau & Mouffe, 2014; Phillips, 2020) will be used as analytical tools to discuss our findings. These concepts will thus constitute a lens through which the accounts of the counsellors (the social practices) can be understood by placing their meaning in a broader social and structural context (Howarth, 2005), thereby offering a perspective for understanding the results of the study.
Results
The basis of professional judgements and decisions
In examining the basis of the professional judgements and decisions made by the participating counsellors, one superordinate theme, “The reasoning” was developed. This theme encompassed counsellor statements that justified, supported, or explained the judgements and decisions that were made. Within this superordinate theme, two subthemes were developed, with these being “Knowledge” and “Values”. Across the multiple attitude objects, judgements and decisions, the counsellors’ arguments and reasons were consistently based on knowledge and/or values: knowledge and values functioned as the reasoning behind the judgements and decisions.
Knowledge and values are not mutually exclusive concepts. Often, they are entangled, and, in practice, the distinction between the two are not unambiguous. Knowledge may inform a value-based approach, just as values may shape the understanding of knowledge. Hence, a differentiation between knowledge and values will to some extent be an analytical distinction. However, for the analysis of the interviews from the present study, the development of “Knowledge” and “Values” as distinctive subthemes were analytically sound.
The use of knowledge and values to justify judgements and decisions were, among others, seen in relation to the topic of the client's treatment goal. For example, in this excerpt from an interview with a counsellor: Torben [the client] says himself that his goal is to reduce his alcohol consumption. He doesn't want to stop drinking completely. How should Henriette, the counsellor, deal with this? In the past, you would admonishingly have said that you can’t [emphasis added] do that and something is broken so that you will never be able to come back to that [drinking moderately]. Today, I think … with the new knowledge we have about addiction. That the brain is plastic and that you can always develop new paths and such things. I would recommend talking a bit about dependence and explaining why it is hard to control. And I might also recommend taking a break [from alcohol] … but not this restrictive approach.
The counsellor seemingly bases her professional judgement on knowledge about the brain and addiction and uses this knowledge as an explanation for accepting the client's goal.
Another counsellor, Ulla, on the other hand, responds to the questions about treatment goals from a value-based point of view: “We are not to be judges here. And we should not have a know-all attitude in many areas. It is people's lives, and it is their choice” (Ulla, counsellor). Here, the counsellor does not derive her arguments from factual knowledge. Instead, she justifies her judgement from a value-based standpoint, where the client's autonomy and humility as a professional are emphasized.
For each of the two subthemes, knowledge and values, we further identified several subcategories, presenting in more detail the reasoning that informed the counsellors’ judgements and decisions. Figure 1 provides an overview of the superordinate theme, the subthemes and the subcategories within.
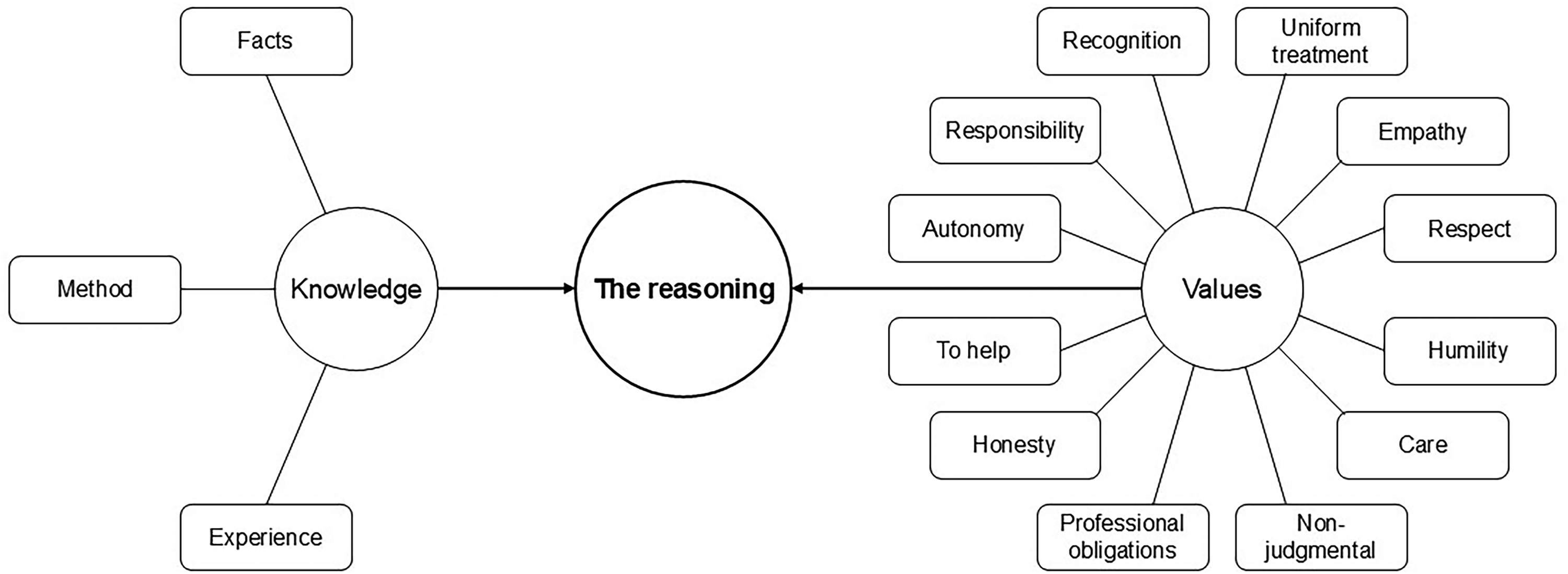
Overview of main theme, subthemes and subcategories identified through the analysis of interview data.
The two subthemes and the subcategories are elaborated below.
Knowledge
Overall, the factual and methodological knowledge articulated was very similar among the counsellors. This applied when explaining alcohol problems as well as choosing and describing needed interventions. We also found widespread similarities regarding the language used by the counsellors when discussing the vignettes and the related questions.
Three subcategories were developed, representing the different forms of knowledge referred to by the counsellors. The factual knowledge (“Facts”) primarily covered knowledge about addiction, biology and genetic/environmental predispositions to the development of alcohol problems. For example, one counsellor, Tove, mentioned the relevance of providing “… education on the biochemical. You know, why is it you are drinking? What it [alcohol] does in your brain, the dopamine-releasing and such things”. Several counsellors also referred to knowledge about the brain and addiction, e.g., the counsellor, Lone, who referred to “… the new knowledge that we have about addiction. That the brain is plastic and that you can always develop new paths and such things”, and the counsellor, Tanja, who described having experienced a shift in the approach to a treatment goal of moderate drinking: I remember, many years ago it was something like this when a client came in … that “if you drink like that, you will never [emphasis added] be able to drink again. You have to say no to alcohol for the rest of your life”. And I know that has scared many away [from treatment].
The factual knowledge also entailed known consequences related to harmful use of alcohol, such as cognitive impairments, sleep problems etc. Additionally, several counsellors referred to the National Health Authorities’ recommendations regarding alcohol consumption. The methodological knowledge (“Methods”) covered a number of different treatment methods. The methods most often referred to were cognitive behavioral therapy and motivational interviewing. However, other approaches and methods were also mentioned (e.g., family-oriented treatment, compassion focused therapy and meta-cognitive therapy). In addition to factual and methodological knowledge, experience-based knowledge (“Experience”) was applied by almost all of the counsellors. These were experiences gained through the counsellors’ clinical work. The experience-based knowledge related to experiences regarding similar cases as the two described in the vignettes and were typically mentioned in connection to the other two forms of knowledge. Counsellors often used their experiences to either substantiate or exemplify the factual knowledge, to justify their choice of method, or to support their judgements regarding the clients in the vignettes (problem severity, treatment goals, etc.).
The impact of the evidence movement
In Denmark, the treatment of AUD is publicly funded and free of charge for the clients. The public treatment is delivered by social- and health care professionals in municipal treatment facilities. Since 2005, educational courses for addiction counsellors in public outpatient treatment for AUD have also been partly funded by the Danish Health Authorities. These courses include the dissemination of knowledge about alcohol use, health consequences, addiction, biology, treatment methods, etc. In 2015, the Danish Health Authorities published the first National Clinical Guidelines for the treatment of alcohol use disorders (Danish Health Authorities, 2018). In 2024, 81% of the public alcohol treatment facilities reported that one or more of their employees had participated in the alcohol treatment courses and 93% of the public treatment facilities reported to have one or more employees with further training in cognitive behavioral therapy (Nordic Health Care Group, 2025).
Our finding of notable similarities among the counsellors regarding the factual and methodological knowledge used as a basis for judgement and decisions may be linked to the increasing political focus on evidence-based treatment and education of counsellors in the public treatment facilities in Denmark. Seven out of 12 counsellors in the present study had completed alcohol treatment courses funded by the Danish Health Authorities; the remaining five had training in cognitive behavioral therapy. All counsellors had participated in some form of addiction treatment training. Our finding that the counsellors refer to a rather uniform knowledge base and palette of treatment methods may reflect the national initiatives to strengthen professional qualifications in public treatment facilities and promote an evidence-based practice (Danish Health Authorities, 2019a). The treatment methods referred to by the counsellors align with the national clinical guidelines (cognitive behavioral therapy, family-oriented treatment, etc.), and the professional concepts applied by the counsellors reflect the terminology used in the guidelines and educational courses. For example, none of the counsellors used the term “alcoholic”. Instead, terms such as “people with addiction problems” and “symptoms of dependence” were used. The same applied when the counsellors described the suggested content of treatment. Here, similar terms, such as “motivation”, “a cognitive approach” and “permission-giving thoughts” recurred among the counsellors.
The similarities in language may also reflect the existence of “technical language” in the context of alcohol treatment. Sheppard & Ryan (2003) found that, in addition to references to laws, procedures and evidence-based knowledge, social workers’ clinical reasoning included “technical language”, comprising concepts and terms from social sciences characteristically used by the professionals in a specific occupation. In the present study, being an addiction counsellor constituted the specific occupation. However, we cannot exclude the possibility that the counsellors to some degree were influenced by language used by the interviewer and in the vignettes.
Values
From all data extracts collated under the subtheme “values”, we identified several values and ideals consistently recurring through the 12 interviews. These included: recognition, autonomy, responsibility, empathy, to help, honesty, humility, respect, professional obligations, non-judgmental, care and uniform treatment. The identified ideals were not merely words or expressions often used by the counsellors. Rather, they were a summary of several words and statements, whose meaning was interpreted and condensed in the values mentioned. An example of this was seen in a statement by the counsellor, Tanja: “Who likes to have others pointing their fingers at them? And being told that you are flawed or wrong? Then you won't come back. So, I think it's important to meet the client. And be inclusive and understanding”. This excerpt shows how values such as showing empathy and being non-judgmental were expressed.
In identifying the values underpinning the interviewees’ reasoning, we thus moved from the semantic level to an interpretive level (Braun & Clarke, 2006). A (not exhaustive) overview of data extracts (words and phrases) used in interpreting and condensing values is presented in Appendix 4 (in Danish). An English translation is available upon request from the corresponding author.
Differences among the counsellors regarding the use of values
While the knowledge used by the counsellors when justifying their judgements and decisions was rather uniform, there was a diversity regarding the specific values referred to by the counsellors. We identified a variation in how counsellors defined and applied particular values in their argumentation. Certain values showed not to have one clear definition but appeared in various versions or with subtle distinctions; for example, the values “recognition” and “responsibility”. Below, the value “recognition” will serve as an example to unfold this finding.
Recognition
Among the counsellors, the value “recognition” was brought up both explicitly and implicitly. However, the meaning of the value varied, and through the counsellors’ statements we saw how the concept of “recognition” was assigned with different content from counsellor to counsellor.
Recognition as a moral/ethical demand
Some counsellors articulated “recognition” as a moral/ethical demand; you should recognize the client, because that is the right thing to do. “Recognition” hereby implied an understanding of the client as the expert on his own life. These counsellors prioritized the client's understandings and wishes over their own judgement when making decisions, as they considered this to be morally right. The recognition thus expressed a desire from the counsellors to see, understand, and meet the client, as the client sees himself, understands himself, and wants to be met.
This understanding of “recognition” was seen in this excerpt from an interview with a counsellor: Based on your professional assessment of Torben's [the client's] situation and problems, what do you think should be the goal for Torben's treatment? Yes, it's a bit tricky, isn't it. Because my only goal would be that Torben felt that he benefited from coming here, so that he wanted to come again. I have no goal for Torben. It is Torben's goal, which is his goal. But my goal is that he feels recognized and understood and heard and wants to come again.
The counsellor directly used the word “recognized” and then connected it to the words “understood” and “heard”. Thus, feeling recognized was related to being heard and understood. Understanding the client presupposes a willingness to set aside one's own understandings and desires. This willingness was evident: through the articulation, the counsellor established a difference between “Torben's goal” and “my goal”. This distinction signaled that recognizing the client implied that only the client was to set the treatment goals, and that only the client's perception of treatment effect was important. The counsellor's goal related exclusively to her own way of meeting the client. Regarding the client as the expert on his own life and treatment substantiated the moral rightness in letting the client decide. Recognizing the client was framed as a moral and ethical imperative.
Recognition as (necessary) acceptance
Other counsellors framed “recognition” more like “acceptance”. These expressed that you must recognize the client's wishes, goals and choices, because no other real options exist. Given client autonomy, one must accept what the client is bringing. Emphasis was not on the moral/ethical aspect of recognition, but on acceptance as a condition. Recognition was also at times articulated with a tone of reservation.
This meaning of “recognition” was expressed in this excerpt from an interview with a counsellor: Torben [the client] says himself that his goal is to reduce his alcohol consumption. He doesn't want to stop drinking completely. (pretends to tear her hair) I just see so many of them at the moment! How should Henriette, the counsellor, deal with it? Well.. She will say: “Alright, fine. You should know that you meet at least three of the diagnostic criteria for dependence, so you will”. I am very honest – I am very [emphasis added] honest! The cards on the table: “So you should know that it will be very difficult for you. And you get these four months to try it out, and if you don’t succeed, then you have to do something else. Then I can’t teach you”. What is your professional opinion on Torben's goals? My professional opinion is … that it is utopia. Okay. And that's why you're tearing your hair out a little, thinking of all those similar cases you meet at the moment? Yes. I see so many at the moment who want to reduce [their drinking]. Who are [emphasis added] dependent. And I think: “Argh”. Because it's a bit of a waste of both their time and mine. That they must first come to realize that it is not possible. I can sit and say: “It is not possible”. But they must realize it themselves.
The recognition of the client's treatment goal was followed by a kind of “but”. The counsellor stated that she was “fine” with the client's goal but added a “very honest” and direct point that she herself did not believe that the client would succeed in his goal. Thus, the client's goal was recognized; it did set the direction for the treatment. The counsellor did not reject the goal – despite her “tearing the hair out” frustration. It was recognition borne by the fact that the counsellor had to recognize the client's decision, more than by a moral imperative. Thus, it was not recognition in the sense of happily setting aside one's own understandings and beliefs. Rather it was in the sense of (reluctant) acceptance.
Recognition as universally human recognizability
A third version of the concept “recognition” was articulated among still other counsellors in the study. Here, recognition was primarily related to something universally human in the client's situation with which the counsellor identified. It was recognition based on the counsellor's experience of understanding the client on a more human level. Thus, this recognition was not a result of the counsellor making a deliberate choice to meet the client with recognition or understanding. Rather, it was rooted in an immediate, spontaneous empathy based on recognizable circumstances in the client's situation.
Recognition in this version was expressed by one of the counsellors in this interview excerpt:
Lone, the counsellor, continues: It is my experience that people themselves do not understand what has happened. Firstly, this taboo about losing control over your “own shit”. Losing control over your problems and not being able to solve them yourself. And having made several attempts – because Henrik [the client] did that too. And that's because we all really just want to be able to handle our stuff on our own. Then there is the thing about explaining to them; why is it that you suddenly aren’t able to do that. And try to de-taboo it a little bit. Because people also get sick from other things in the world, in Denmark and around us, so why should this really be more shameful? Because you are just as involuntarily stricken by it [the addiction] as with other things. So, to try to de-taboo, to try to understand, so you don't have that feeling of being so fed up with yourself.
The counsellor recognized that making a change is difficult. Approaching the client by telling him to “just stop it” was thus considered not to make sense. The counsellor emphasized that “you” and “we” are already well aware that a change of behavior would be for the best. “We all” prefer to manage our problems ourselves, but it is difficult. By connecting the recognition to an understanding based on a generic “you” and a generic “we”, the recognition articulated was not only a result of the counsellor understanding this specific client but also a result of an identification with and humanization of the challenges faced by the client. The counsellor likened the client's problems to other, to her, common problems (smoking, overweight, illness). This became the basis for and reasoning behind meeting the client with recognition.
A discourse theoretical perspective on the identified differences in meaning
The results of our study showed that while similarities were found regarding the counsellors’ accounts of knowledge, diversity was found regarding the meaning of values used by the counsellors. Laclau & Mouffe's discourse theory (Howarth, 2005; Laclau & Mouffe, 2014) offers a framework for broadening our understanding of this finding. Specifically, the concepts of “floating signifiers” and “subject positions” will be applied in the following.
Laclau & Mouffe (Hein Jessen & Hansen, 2021; Phillips, 2020) describe how “floating signifiers” (i.e., signifiers referring to concepts within language that lack a fixed meaning) are contingent on the discursive context in which they are used. Thus, different discourses will compete to fix the meaning of the signifiers in different ways, and the same signifier may thus have several different meanings (Phillips, 2020). This corresponds to our finding that different counsellors may refer to the same value, but for different reasons, when arguing for their judgements and decisions regarding a specific topic. The value “recognition”, used in the present study as an example, showed not to have one fixed meaning. The meaning of the concept varied among the counsellors. Within the different discourses in which the value was used, “recognition” was assigned with content in different ways. From the perspective of Laclau & Mouffe (Phillips, 2020), this value/concept can be regarded a floating signifier; lacking a fixed, specific meaning. Each discourse competed to fix the meaning of “recognition” in its own specific way. This fight for “recognition” as, respectively, a moral/ethical demand, (necessary) acceptance or human recognizability showed how, in a discourse theoretical perspective, the value was a floating signifier. The same applied to other ideals and guiding principles that appeared through the analysis of the interviews. Thus, our analysis of these values as floating signifiers offers a perspective for understanding how one value can be used in different ways and for different purposes when counsellors argue for their judgements and decisions.
Subject positions refer to the positioning of subjects within a discursive structure. Different discourses constitute different subject positions with which the social actors – in this case the counsellors – can identify (Howarth, 2005). As the meaning of concepts (values) is contingent on the discursive context in which they are used, according to Laclau & Mouffe (2014), different discourses also open up to different subject positions. The subject positions influence which options for action or decision the counsellors experience having (Howarth, 2005). In a discourse theoretical perspective, the different versions of the value “recognition” can thus be linked to different competing discourses and subject positions. Recognition as a moral/ethical demand can be understood as linked to a subject position of “the humble social worker” for whom it comes naturally (as the available option for action) to see the client as the expert and to act based on joint responsibility. Recognition as necessary acceptance can be understood as linked to a subject position of “the practical facilitator”, constituted by a discourse within which the client's autonomy and responsibility are emphasized. For example, when the counsellor, Linda, explains that a moderate drinking goal will be challenging given the client's alcohol dependence, but accepts the client's wish to try anyway, because he must realize this himself. As a facilitator, the natural (available) action is to make treatment available, yet accepting and insisting on the client's responsibility. Recognition as human recognizability can be understood as linked to a subject position of “the authentic human being”, constituted by a discourse within which humanity and brotherliness are focal points, and the relation to the client is high priority. Thus, as an “authentic human being”, providing care and expressing empathy may be perceived by the counsellors as the obvious (available) option for action. A discourse within which emphasis is on factual, evidence-based knowledge and professional expertise, will likely open to a subject position of “the expert” for the counsellor to identify with. Accordingly, decisions and judgements within this discourse and from this subject position will likely be based on knowledge, and the communication of factual knowledge and expert guidance will be perceived as the proper action and a professional obligation (the available options for action within the discourse).
Consequently, different subject positions will result in different judgements and decisions and/or in different ways of arguing for and justifying the judgements and decisions. While similarities in the factual and methodological knowledge might be a result of training, dissemination of knowledge and implementation of clinical guidelines, the differences in meaning of values and in the use of values and/or knowledge can be understood as an expression of different subject positions made available through different competing discourses within the alcohol treatment context.
Discussion
In this qualitative study, we explored the professional judgement and decision-making among addiction counsellors working in outpatient treatment for AUD in Denmark. We showed how knowledge and values form the basis of the professional decision-making, as these function as the reasoning behind the opinions and judgements expressed by the counsellors. We identified both similarities and differences among the counsellors. Similarities were seen in the factual and methodological knowledge used by the counsellors, while differences were seen when values were used and referred to by the counsellors. Of particular interest, we identified certain differences in how values were understood and applied by the counsellors when referring to these as a basis for the professional judgements and decisions.
Diversity is a condition
The results of the present study are in line with previous research on professional judgement and decision-making in social work practice. Our finding of differences regarding counsellors’ understandings of specific values supports the findings of Blomqvist & Wallander (2004). Their study indicated a lack of professional consensus regarding the meaning of both different interventions and different concepts and terms. Blomqvist & Wallander (2004) also point out that there appear to be more fundamental differences in the social workers’ approach to clients. Their analyses indicated the existence of conflicting views or “styles” within the social work profession. This applied to, among other things, the importance of considering the individual client's point of view. Blomqvist & Wallander (2004) concludes that the differences identified were not to be explained by the variables included in their study. By applying the concept of “subject positions”, drawn from Laclau & Mouffe's discourse theory (Howarth, 2005; Laclau & Mouffe, 2014), our study offers a perspective for understanding this.
Our findings are also in line with the findings of Mosteiro et al. (2018). They found that the professionals used the same argument categories and criteria when making decisions, but that the weighting and interpretation of these criteria differed significantly when justifying the decisions. This corresponds with our finding that the interpretation and attribution of meaning play a substantial role when making professional judgements and decisions. In the present study, we showed how counsellors referred to the same values when justifying their decisions, but that these values were understood and applied in different ways. This adds to the understanding of differences derived by Mosteiro et al. (2018), who conclude that the argument variability primarily can be explained by different perceptions of the facts presented to the professionals, different decision thresholds and a diversity in the judgements of the situation described in the vignette. Our analysis suggests that differences among counsellors also reflect different interpretations and applications of values in decision-making, which in turn are connected to different discourses and subject positions.
Differences in the definition and meaning of values among counsellors are to be expected, especially from a constructionist perspective highlighting the incompleteness and openness of the social structures. However, this attribution of meaning was left implicit and unreflected upon in the interviews with counsellors. The identified differences seem to remain “latent” or hidden from the very professionals whose judgements and decisions are guided by the particular values.
Implications for practice
Focus on meaning as a prerequisite for uniform treatment
The present study demonstrates the importance of discussing and clarifying the meaning of values. Values reflect ethical and moral principles for action and practice, and social work as a (relational) profession is characterized by a focus on ethics and values (Banks, 1995). When counsellors base their judgements and decisions on values that are not unambiguously defined, this may result in alcohol treatment being not as uniform as counsellors and policymakers assume. In terms of knowledge, the treatment might be based on the same foundation of facts and methods, and counsellors might believe they provide good treatment anchored in classic social work values. However, the counsellors may remain unaware that their practice lacks uniformity because the ambiguous nature of these values is not apparent to them.
Blomqvist & Wallander (2004) call for a common language to describe and discuss the everyday practice of social workers in the addiction treatment. Although we found that counsellors to some extent used a common language, the findings of the present study still support a need to explicitly discuss and clarify the content and meaning of central concepts relevant to practice.
Concerning the factual and methodological knowledge that informs the treatment, uniformity may be both desirable and achievable. The results of the present study suggest that training and clinical guidelines have supported a shared knowledge base among addiction counsellors in the outpatient treatment for AUD in Denmark. However, treatment is provided by individual social actors. Consequently, differences regarding the judgements and decisions continuously made during treatment cannot be eliminated. Diversity is a condition in social work practice. Yet, in the efforts to strengthen professional quality and ensure a certain uniformity of treatment, values must be rendered visible and their content and meaning made a subject of professional discussion. Not with the purpose of eliminating differences, but with the purpose of facilitating reflection and a social work practice based on a shared understanding of values. Without this clarification of values, it is not possible to guide the clinical practice by anchoring treatment in social work values, such as recognition. If attention is not paid to the fact that the meaning of values varies from counsellor to counsellor (discourse to discourse), there is a risk that using values to guide a “best practice” will be ineffective or purposeless.
Focus on both knowledge and values
Ensuring a uniform, high-quality alcohol treatment can be pursued by implementation of clinical guidelines and formal in-service training of counsellors. That is, through means that focus on providing counsellors with knowledge. However, as can be concluded from our study, knowledge only forms part of the foundation on which counsellors base their professional judgements and decisions. Regarding several topics of matter, the arguments and justifications are also based on values.
The distinction between knowledge and values can be difficult to make. Adopting a practice based on particular values (e.g., autonomy) may reflect knowledge about how to efficiently approach clients in order to succeed, in addition to reflecting a moral or professional standpoint. Still, our finding that counsellors to a considerable extent use values as part of their reasoning and judgements underscores that dissemination of knowledge cannot stand alone in the training of counsellors. Focus must also include the values expressed and applied by the counsellors, as these ideals influence both whether and how the factual and methodological knowledge is used. To pursue the goal of a uniform and quality-assured treatment, it may be necessary to extend the focus beyond evidence-based knowledge. Attention must also be paid to the value base of the counsellors. Consideration might be given to incorporating this focus into the addiction counsellor curriculum.
Need for critical reflection and debate
The present study highlights the importance of critical reflection in the delivery of social work services, including the treatment for AUD. This is in line with conclusions from previous research that also emphasizes the necessity for facilitation and encouragement of social workers to both articulate and reflect on their judgement and decisions (Gambrill, 2006; Osmo & Landau, 2001; Wallander & Blomqvist, 2009). O'Sullivan (2010) argues that decision-making in social work requires reflexivity. This involves being critical about one's own practice as a social work professional and examining the beliefs, thinking, interpretations and reasoning that underlie the decisions made. O'Sullivan (2010) points at the need for both internal scrutiny (i.e., reflexivity) and external scrutiny, which includes “… explaining one's reasoning to others so that they can examine its validity” (O'Sullivan, 2010). Our finding of a diversity in the meaning and use of values supports this call for reflection.
In addition to highlighting the need for making judgements and decisions a subject of debate and reflection, the present study demonstrates how the vignette method can be a fruitful approach to facilitate this, as also suggested by Ejrnæs & Monrad (2012). O'Sullivan (2010) notes that, as part of supervision, “Case-based discussion can help to clarify and develop critical awareness of the practice context in which decisions are being taken” (O'Sullivan, 2010). The vignette method is well suited for this purpose and thus has the potential to constitute a model for professional development. This approach may also provide a counterweight to guidelines, manuals and documentation requirements that “tell” the counsellors what to do in their daily work and thereby supplement the evidence-based approach to treatment.
Methodological considerations, limitations and strengths
The vignettes developed and used for the present study have formed the context for our data and analysis. Our results must therefore be viewed in the light of these very vignettes. On that basis, we must be cautious about generalizing beyond the specific contexts described in the vignettes. However, the vignettes were used with the purpose of exploring what the counsellors more generally base their professional judgements on and how they more generally reason. The interviews and analysis did therefore focus on reasons for judgements and decisions rather than the specific judgements and decisions themselves. This makes it likely that the knowledge and values informing the counsellors’ professional judgement will also apply in relation to other situations or patients within the broader context of outpatient treatment for AUD.
A limitation also exists regarding the predictive validity of our results and analysis. By using the vignette method, we are not able to conclude on the actual actions of the counsellors; only their opinions and judgements regarding what should be done. Thus, the responses of the counsellors cannot be used to predict what these counsellors would actually do in a similar situation (Finch, 1987). The vignette method only conveys tendencies to act in certain ways. However, this aspect is more an empirical question of the correlation between two different phenomena (tendencies to act vis-à-vis actual actions) than of the validity of the method itself. In relation to our study objectives, we consider this aspect not to be of critical importance because our aim was to investigate differences in the reasons for a practice rather than differences in practice per se. Supplementing our data with observations from practice would, however, add an extra and interesting perspective to our findings.
The present study combines the vignette method with individual interviews to explore professional judgement and decision-making. Following this objective, we consider the two techniques to be complimentary and well suited for the study. The vignette method has several advantages. It allows the researcher to specify the context and certain features related to this in detail in a systematic way. Accordingly, the normative statements of the respondents are related to a specified context rather than more abstract ideas or generalized situations (Finch, 1987). This enabled us to compare the counsellors’ answers and judgements regarding the situations described and made it possible to highlight the nuances and the diversity that appeared.
The vignette method also has the advantage of distancing the respondent's judgement of the situations described from his/her personal circumstances. This is partly due to the hypothetical character of the situations outlined and partly due to the researcher's opportunity to ask the questions in third-person (Finch, 1987). This makes it less personal and therefore less threatening and vulnerable for the counsellors to share their opinions and judgements (Hughes, 1998). By using the vignette method, we thus supported honest reflection and reduced the risk of response bias.
Conclusions
The present study demonstrated how addiction counsellors working in outpatient treatment for AUD in Denmark base their professional judgements and decisions on knowledge and values. Of particular relevance, certain values showed to lack a clear definition when applied by the counsellors. Values influence whether and how knowledge is used, making their clarification essential for a practice built on evidence-based knowledge. Without such clarity, value-based practice becomes meaningless and values cannot effectively guide the professionals. At least not in the same direction.
Supplemental Material
sj-docx-1-nad-10.1177_14550725251407463 - Supplemental material for What shapes professional practice: Judgement and decision-making in Danish outpatient alcohol counselling
Supplemental material, sj-docx-1-nad-10.1177_14550725251407463 for What shapes professional practice: Judgement and decision-making in Danish outpatient alcohol counselling by Kristina Hasselbalch Volke and Anette Søgaard Nielsen in Nordic Studies on Alcohol and Drugs
Supplemental Material
sj-docx-2-nad-10.1177_14550725251407463 - Supplemental material for What shapes professional practice: Judgement and decision-making in Danish outpatient alcohol counselling
Supplemental material, sj-docx-2-nad-10.1177_14550725251407463 for What shapes professional practice: Judgement and decision-making in Danish outpatient alcohol counselling by Kristina Hasselbalch Volke and Anette Søgaard Nielsen in Nordic Studies on Alcohol and Drugs
Supplemental Material
sj-docx-3-nad-10.1177_14550725251407463 - Supplemental material for What shapes professional practice: Judgement and decision-making in Danish outpatient alcohol counselling
Supplemental material, sj-docx-3-nad-10.1177_14550725251407463 for What shapes professional practice: Judgement and decision-making in Danish outpatient alcohol counselling by Kristina Hasselbalch Volke and Anette Søgaard Nielsen in Nordic Studies on Alcohol and Drugs
Supplemental Material
sj-docx-4-nad-10.1177_14550725251407463 - Supplemental material for What shapes professional practice: Judgement and decision-making in Danish outpatient alcohol counselling
Supplemental material, sj-docx-4-nad-10.1177_14550725251407463 for What shapes professional practice: Judgement and decision-making in Danish outpatient alcohol counselling by Kristina Hasselbalch Volke and Anette Søgaard Nielsen in Nordic Studies on Alcohol and Drugs
Footnotes
Acknowledgements
We thank the counsellors who volunteered to participate in the interviews for this study and who openly shared their thoughts and opinions with us.
Ethical considerations
All individuals that were interviewed as part of this study, participated in their role as addiction counsellors. No personal data or information about the participants was collected, used or reported in the study. Therefore, application for ethical approval was deemed not required.
Consent to participate
Informed consent was obtained verbally from all individual participants included in the study prior to conduction of the interviews. The consent was video-recorded.
Consent for publication
All participants provided verbal consent to publish the study prior to conduction of the interviews.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.