
Abstract
Introduction
Social support that facilitates healthy community belonging is essential to obtaining and maintaining recovery from substance use disorder (SUD) (Vigdal et al., 2022). Recovery from SUD is considered a protracted, multidimensional, heterogeneous process (Witkiewitz et al., 2020). The clinical recovery framework depicts SUD as a mental disorder containing specific core symptoms (Liberman et al., 2002). The symptom criteria are based on researcher-derived thresholds and predefined objectives, and recovery is achieved when symptoms subside below a diagnostic threshold. Within a personal recovery tradition, recovery is viewed as going beyond a reduction in core symptoms, and the focus is rather on contributory citizenship, identity change, connectedness, hope, optimism, meaning in life and the ability to build a new life despite the presence of symptoms (Davidson et al., 2007; Leamy et al., 2011).
Both the clinical and personal recovery frameworks have been criticised for overemphasising intrapersonal experiences and underestimating the interpersonal context of recovery (Price-Robertson et al., 2017). It is, however, currently common across traditions to consider symptom reduction as expedient to obtaining and maintaining recovery. Further, the focus on interpersonal aspects has gradually received more general support (Fowler et al., 2019; Pettersen et al., 2019).
Polysubstance disorder is common in clinical samples, although it is not a specified diagnosis in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) (Bhalla et al., 2017; Hasin et al., 2013). Among patients seeking treatment for mono-substance use disorder polysubstance use is frequent (Hetland et al., 2021; Onyeka et al., 2012). It is important to address polysubstance use since it seems to reflect the reality in treatment situations. The current study is part of the Norwegian Stavanger Study of Trajectories in Addiction (STAYER), a prospective naturalistic follow-up study of change trajectories among people diagnosed with SUD, investigating the course and timing of neurocognitive and psychosocial factors, including recovery (Hagen et al., 2016; Svendsen et al., 2017). In agreement with previous research on the STAYER sample (Erga et al., 2020), “polysubstance use disorder” (PSUD) refers to the use of multiple substances as part of a pattern of problematic substance use, in which the participants meet the criteria for SUD for some, but not necessarily all substances used. Nonetheless, polysubstance use is complex phenomenon and that research has defined it differently according to simultaneous or sequential use and short and long time frames (Ellis et al., 2023; Fitzgerald et al., 2022; Liu et al., 2018; Mefodeva et al., 2022). However, most researchers would agree on a consensus definition of it involving consumption of multiple substances within a specified time frame.
Previous research and reviews have found that supportive friendships in recovery networks, such as Alcoholics Anonymous or non-drug-using social networks, are related to sustained abstinence (Best et al., 2016; Drake et al., 2008; Nesvåg & McKay, 2018; Weisner et al., 2003) and reduced relapse risk (Ness et al., 2014; Nordfjaern, 2011), but the role of supportive friendships in recovery is complicated and broad. Research indicates that supportive friendships may have a positive impact on recovery, but it varies and depends on several factors such as the specificity of the measure (general or specific support to substance use), and other factors, e.g., readiness to change and age (Groh et al., 2007; McKay et al., 2011; McKay et al., 2013a). Friendships or networks that support abstinence are favorable to sustained abstinence (Litt et al., 2009). However, the support might be indirect through environmental factors (i.e., others in one's network misuse substances), rather than supporting substance use (Groh et al., 2007). Overall, previous research finds that social factors may be positive, negative or mixed in promoting recovery (McCrady, 2004).
Weisner et al. (2003) investigated to what extent individual, treatment, or extra-treatment characteristics were predictive of abstinence at the 5-year follow-up based on participants’ interviews at baseline, at 6 months and at the 5-year follow-up. They found that abstinence at 6 months predicted abstinence at 5 years, and predictors of abstinence were, among others, being female and involvement in recovery-oriented social networks. However, they might have missed other association since they did not conduct annual interviews. A systematic review found that having supportive friendships was indispensable to recovery (Vigdal et al., 2022), while a literature review found that having unsupportive drug-free friendships negatively affected recovery (Groh et al., 2008). Dennis et al. (2007) interviewed patients in treatment for alcohol or drug use about their perceived social support and number of drug-free friends at 6-month follow-up and annually for 8 years. They found a positive association between the duration of abstinence, experiencing social support and having drug-free friends, and that females were significantly more likely to maintain abstinence than men. However, the assessment of drug and alcohol use was conducted retrospectively. Thus, previous research has long intervals between participant assessments and retrospective calculations of drug and alcohol use, which include methodological uncertainties that our research aims to mitigate.
There are few Scandinavian studies of patients with SUD with comparable follow-up design to the current study. Several of the longitudinal studies are of high-risk groups, such as the Norwegian Offender Mental Health and Addiction study (NorMA) (Bukten et al., 2015), adolescents (12–16 years of age) with SUD (The Monitoring Young Lifestyles (MyLife)) (Brunborg et al., 2019) or general population based longitudinal studies such as the Norwegian Tracking Opportunities and Problems Study (Nilsen et al., 2017), resulting in issues with generalisation to patients with SUD. This is also the case for research from Finland and Sweden focusing on the general population (Nilsson et al., 2014; Savage et al., 2018), a collaboration between Norway, Denmark, Finland, Iceland and Sweden focusing on adolescents (Raitasalo et al., 2024), and The Danish longitudinal study of alcoholism 1978–2008 (Knop, 2011). In one Norwegian study with 10-year follow-up of patients with SUDs, the role of friendships for recovery trajectories where not explored (Melberg et al., 2003).
The ability to recover may also depend on substance use debut age, biological sex and gender. Research shows that obtaining recovery and reduction in substance use are associated with onset age (Dennis et al., 2005; Grella et al., 2003; Hser et al., 2007; Scott et al., 2005; Simpson et al., 1997). Females tend to have a lower risk of relapse after recovery than males (Grella et al., 2008), but gender-associated relapse risk depends on the substance used (Riley et al., 2018; Zakiniaeiz & Potenza, 2018). Although recent research suggests that females and males do not differ considerably in terms of SUD treatment outcome, the findings on biological sex and gender differences in SUDs are complicated due to the complex interaction between biological and environmental aspects (McHugh et al., 2018).
However, previous and recent reviews suggest that most SUD research is short-term and focuses on substance use reduction rather than functioning (Moe et al., 2021; Tiffany et al., 2012). Systematic reviews suggest there are few longitudinal SUD studies on drug-free relationships, debut age and gender with a duration extending 2 years (Bjornestad et al., 2020; Vanderplasschen & Best, 2021). It seems that the field needs longitudinal SUD research extending two years focusing on functional aspects and drug-free relationships of addiction recovery, and how they relate to gender, as well as substance use debut age. The present study aims to mitigate this knowledge gap by analysing changes in trajectories of drug-free friendships and alcohol and substance use, and debut age and gender (differences between female and male) annually across 4 years.
Methods
Sample
We recruited the study sample (n = 208) from the ongoing Norwegian Stavanger Study of Trajectories in Addiction (STAYER), comprising a prospective naturalistic follow-up study of change trajectories among people diagnosed with SUD investigating the course and timing of neurocognitive and psychosocial factors, including recovery (Hagen et al., 2016; Svendsen et al., 2017). Participants were included between March 2012 and December 2015, and they were recruited at the start of treatment in outpatient or residential treatment facilities in the Stavanger region of Norway. The sample consisted of patients with SUD, alcohol dependence and behavioural addictions. The STAYER study has been approved by the Regional Ethical Committee (REK 2011/1877). All participants provided written informed consent.
We included participants (1) starting a new treatment sequence within addiction treatment services; (2) aged ≥ 16 years; (3) enrolled in a treatment programme to which they were admitted for at least 2 weeks; and (4) reporting polysubstance use (i.e., patients with SUD who informed the use of multiple substances within the last year before inclusion). In Norway, patients need to have a SUD diagnosis to access specialised addiction treatment. The diagnostic assessment is carried out either by a clinical psychologist or physician and based on the criteria in the International Classification of Diseases, 10th edition (ICD-10). Of the 208 participants in the STAYER study, 164 met these criteria and were included. Due to missing data, only 155 were included in most analyses (detailed below). Details on the STAYER study methodology and retention are published elsewhere (Svendsen et al., 2017).
Measures
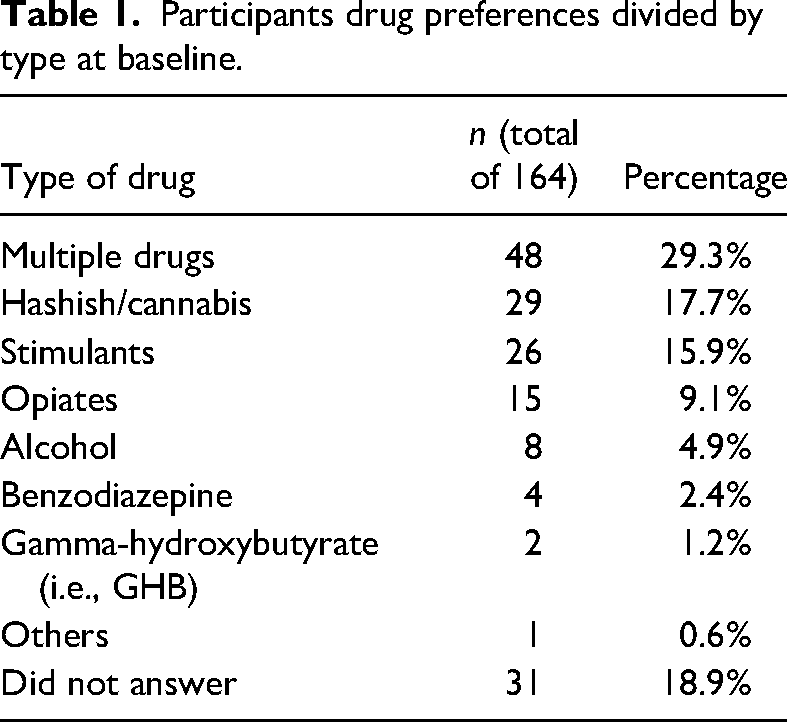
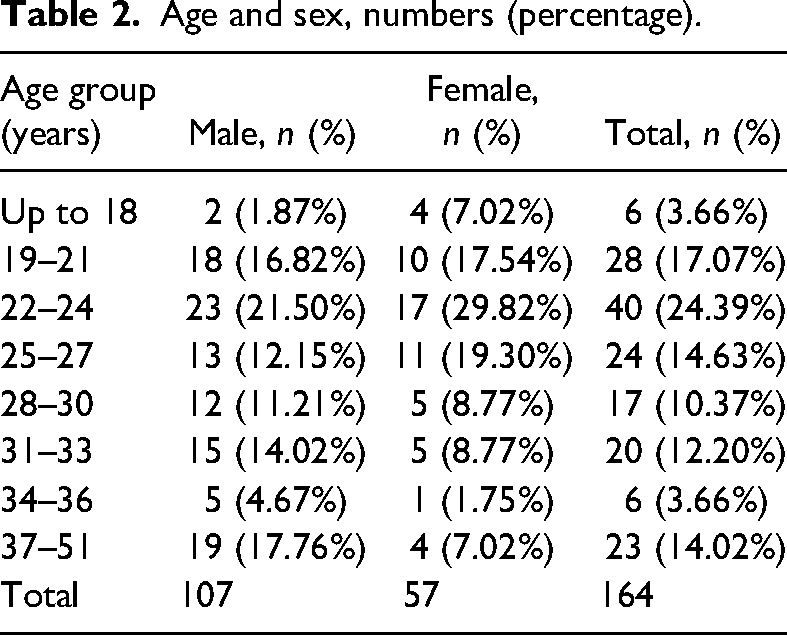
Age was calculated by subtracting birth year from inclusion year at baseline. Gender was reported at baseline. Age and gender were reported in descriptive statistics but were not used in the latent growth curve analyses. Debut age refers to age of initiation of substance use. Because there is no defined cut-off age to indicate early versus late debut age, we chose to analyse drug debut before the age of 13 years versus debut at 13 years and older. We assessed it as favourable to divide between children and adolescents and the transition from elementary school to secondary school often follows the age of 13 years in Norway. More details on distribution of age, gender and substance use disorder are provided in Tables 1 and 2.
Participants drug preferences divided by type at baseline.
Age and sex, numbers (percentage).
Drug and alcohol use
Drug and alcohol use was assessed using adjusted versions of the Drug Use Disorders Identification Test (DUDIT) (Voluse et al., 2012) and the Alcohol Identification Disorder Test (AUDIT) (Babor et al., 1992; Berman et al., 2005). Both DUDIT and AUDIT have been found to have good reliability and validity (Bohn et al., 1995; Hildebrand, 2015; Meneses-Gaya et al., 2009; Voluse et al., 2012). We used DUDIT-C, which consists of the four consumption items measuring drug consumption, to measure drug use (Basedow et al., 2021; Berman et al., 2005). We used AUDIT-C, which consists of the three consumption items of AUDIT, to measure alcohol use (Campbell & Maisto, 2018).
We used DUDIT-C and AUDIT-C scales (ranging from 0 to 8 and from 0 to 12), merging AUDIT-C and DUDIT-C by adding them together after dividing DUDIT-C scores by 8 and AUDIT-C scores by 12. Further, we multiplied the result by four and rounded the result to whole numbers, making a scale from zero (no drug and no alcohol) to eight (maximum on both DUDIT-C and AUDIT-C scales). This new composite variable was termed “alcohol and drug use”. For participants missing AUDIT-C, we used only DUDIT-C, and vice versa. Participants with missing scores on both AUDIT-C and DUDIT-C were coded as missing at that timepoint. We calculated “alcohol and drug use” for 5-yearly follow-ups. Previous research suggests that early treatment response measured at first follow-up is a good predictor of long-term treatment response (McKay et al., 2005; McKay et al., 2013b). Therefore, we excluded baseline measures from the latent growth models.
Drug-free friendships
“Drug-free friendships” was assessed using a self-report questionnaire (KVARUS) to measure social support. “Drug-free friendships” has previously been used to measure social resources (Carlsen et al., 2020). Having drug-free friendships was measured using a dichotomous question (YES/NO) at baseline and follow-ups: “Do you have friendships without a history of substance use?”
Data analysis
Descriptive statistics, data preparation and export were computed using Stata/IC 15.1 (https://www.stata.com). Mplus, version 8 (https://www.statmodel.com) was used for the latent growth curve models (LGM). We defined the “alcohol and drug use” scale as continuous variables and used the standard ML estimator in Mplus. Because the “drug-free friendships” measures were categorical, we used the Mplus standard for categorical dependent variables: the WLSMV-estimator (Brown, 2015). To evaluate the goodness of fit for the tested models, we used the root mean square error of approximation (RMSEA) and comparative fit index (CFI). Both measures indicate the degree to which a model fits data. CFI scores closer to 1 and RMSEA scores closer to 0 indicate better model fit (Bollen & Curran, 2006). More specifically, CFI scores ≥0.95 and RMSEA scores ≤0.05 indicate good model fit (Barbara, 2012), whereas RMSEA scores between .05 and .08 have been deemed acceptable (Kim et al., 2016).
First, we examined the association between “alcohol and drug use” and “drug-free friendships” across the last five follow-ups (Table 3). We tested if these associations were significant using chi-squared tests. Second, we ran multiple longitudinal models to examine possible models for understanding the association between “alcohol and drug use” and “drug-free friendships”. We developed three LGMs. Model 1 (M1) investigated to which degree the LGM on longitudinal development in alcohol and drug use fits the data. Model fit indicators for all models were summarised in Table 4.
“Alcohol and drug use” (0–8) across drug-free friendships, five waves.
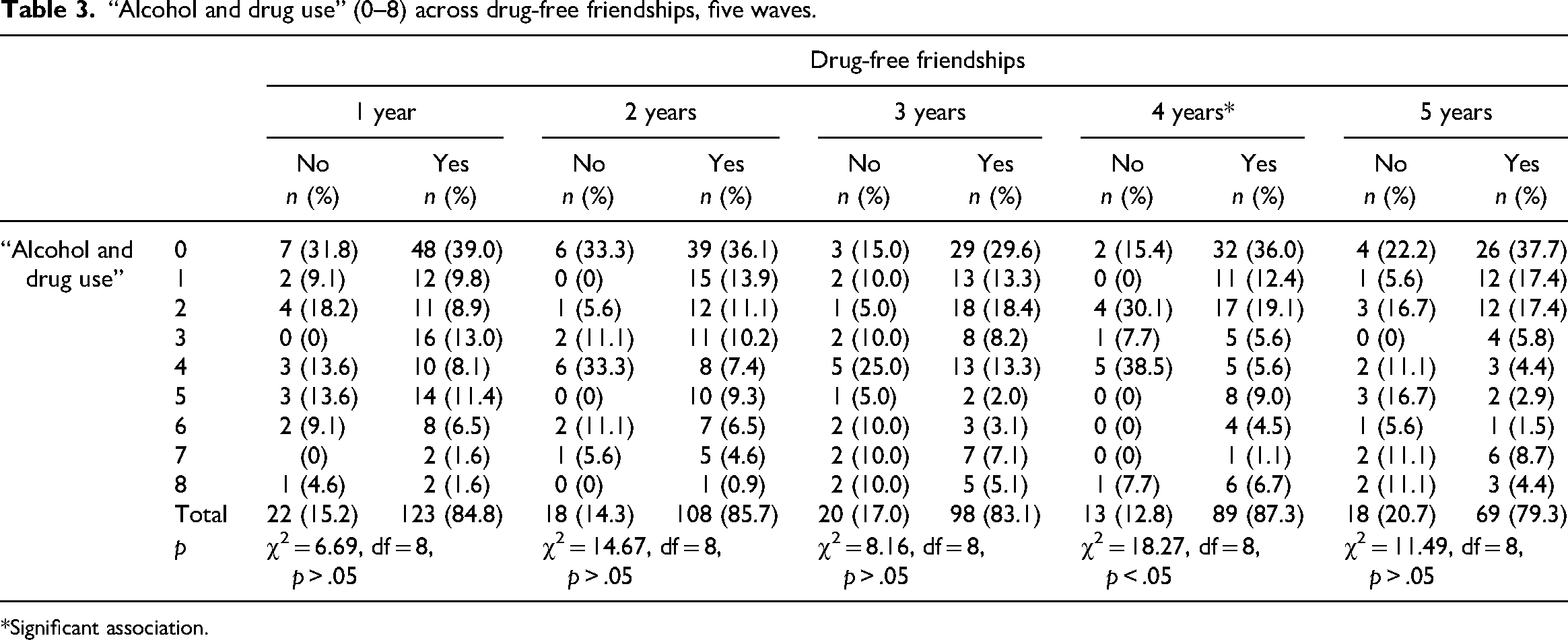
*Significant association.
Fit indices for the tested models.
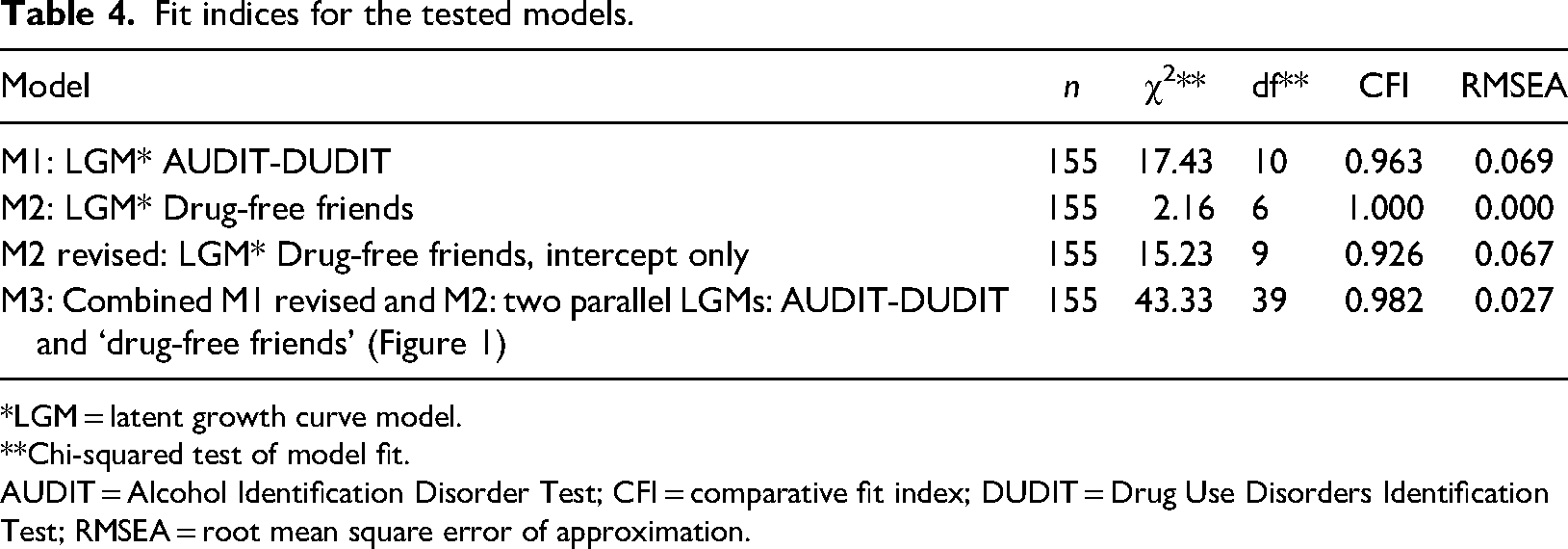
*LGM = latent growth curve model.
**Chi-squared test of model fit.
AUDIT = Alcohol Identification Disorder Test; CFI = comparative fit index; DUDIT = Drug Use Disorders Identification Test; RMSEA = root mean square error of approximation.
We divided M1 into two groups based on gender. As the unconstrained model was not significantly better than the constrained model (χ2 difference = 11.32, df difference = 8, p = .18), we rejected gender groups in M1. Furthermore, we divided M1 into two groups based on drug debut before the age of 13 years versus debut at 13 years and older. The unconstrained model was not significantly better than the constrained model (χ2 difference = 8.31, df difference = 8, p = .40). Hence, we kept M1 without groups (M1). However, because participants were selected based on alcohol and drug use at baseline, we removed baseline from the LGM and used this LGM as a predictor (M1 revised).
Model 2 (M2) investigated the degree to which an LGM fits the development of “drug-free friendships”. The model was an LGM with two latent variables (intercept and slope) reflecting “drug-free friendships” development based on five dichotomous variables. Hence, the model “drug-free friendships” had too few degrees of freedom to estimate model fit. Furthermore, the variance on the slope was not significant. We therefore made a new model with intercept only (M2 revised). We chose to use the initial model (M2) because M2 fits conceptually better with “M1 revised” when making model 3 (M3).
M3 was constructed by combining M1 revised and M2. Thus, M3 was a growth model for two parallel processes with categorical outcomes, “alcohol and drug use” and “drug-free friendships”. We allowed association between the two intercepts. Furthermore, we added a regression from the “alcohol and drug use” intercept to the slope on “drug-free friendships”. We also added a regression from the “drug-free friendships” intercept to the slope on “alcohol and drug use”. Finally, we made a figure for the final model, M3, reporting only significant and standardised weights (Figure 1).
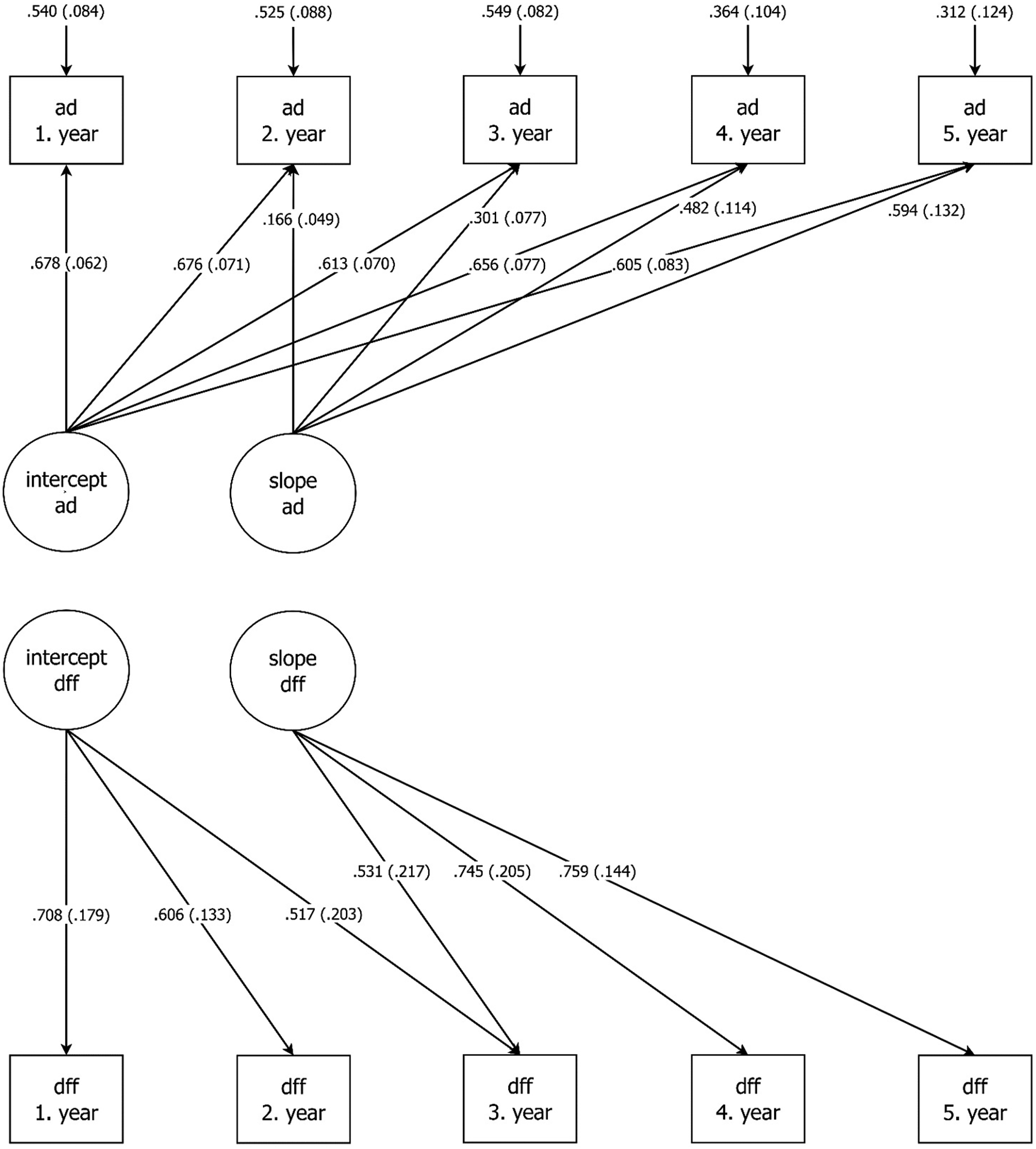
AUDIT-DUDIT (ad) and Drug-free friends (aff) latent growth models; only significant standardised path visible. AUDIT = Alcohol Identification Disorder Test; DUDIT = Drug Use Disorders Identification Test.
Results
Cross-sectional analysis displays a stable pattern of “drug-free friendships” across follow-ups, ranging from 79.3% at 5 years to 87.3% at 4 years (Table 3). Among participants having “drug-free friendships” after 4 years, 36.0% had an “alcohol and drug use” score of 0 in the same year. By contrast, 15.4% of participants without “drug-free friendships” had an “alcohol and drug use” score of 0 (χ2 = 18.27, df = 8, p < .05) (Table 3). In general, there was a clear tendency of lower “alcohol and drug use” scores for participants having “drug-free friendships” after 4 years (χ2 = 18.27, df = 8, p < .05) (Table 3). However, four of the five included annual follow-ups showed no significant difference in “alcohol and drug use” score across having “drug-free friendships” (Table 3).
The initial LGM, including five follow-ups of “alcohol and drug use”, had an acceptable fit (M1) (Table 4) and showed significant variance on both the intercept (2.42, p < .001) and the slope (0.501, p < .05), indicating small interindividual differences in the initial status of “alcohol and drug use” and the change in status over follow-ups. However, only the intercept had a significant mean (2.329, p < .001) and the slope mean was 0 (0.000), implying no change in the scores across follow-ups.
The initial LGM on five follow-ups of “drug-free friendships” could not calculate fit due to too few degrees of freedom (M2) (Table 4). M2 had significant variance on intercept (0.652, p < .05), but not on slope (0.084, p = .404), implying no change across follow-ups. As presented in the method section, this model was kept despite non-significant variance on the slope.
The final model, M3, had a very good fit (Figure 1 and Table 4). We did not find any significant regression path between the “alcohol and drug use” and “drug-free friendships” slope (Figure 1). As previously described in the method section, we allowed the two intercepts to be associated. However, neither this association, nor the allowed association between the slopes was significant.
Discussion
The main finding is the stability in alcohol and drug use across 4 years (i.e., from first to fifth follow-up). Further, drug-free friendships were fairly constant across 4 years and did not affect alcohol and drug use in four of the five follow-ups.
Stability rather than a change in alcohol and drug use
The first model analysing change trajectories in alcohol and drug use showed variations regarding a positive initial alcohol and drug use level. Regarding this development, there is still variation, but the variation is smaller with regard to the regular use of alcohol and drugs. Our finding is contrary to previous research, which often finds several different (e.g., three to four) alcohol and drug use trajectories (Hser et al., 2007; Maisto et al., 2020; Timko et al., 2016; Witkiewitz et al., 2019).
Contrary to our finding, previous studies with follow-up (e.g., 3–4 years) often find a reduction in alcohol or drug use (Dennis & Scott, 2012; McKay & Weiss, 2001; Project MATCH Research Group, 1998). According to Heyman (2013), most people suffering from addiction eventually remit. Although remittance depends on the substance to which one is addicted, Heyman concludes that if the general age of onset is 20 years, most people suffering from addiction are remitted by age 30 years. The mean age of our sample is below 30 years, and it may therefore be possible that substance use levels would have decreased if we had analysed our sample in different age groups or at a later stage during the course. However, other studies suggest that the median time from first to last use of a substance (i.e., obtaining 12 months of abstinence) is 27 years (Dennis et al., 2005).
Drug-free friendships
Our results showed one significant association between alcohol and drug use and drug-free friendship at the fourth year (Table 3). This appears to be contrary to the vast literature on the positive association between social network involvement, social support and recovery (Ellis et al., 2004; McKay, 2017; Ness et al., 2014; Nesvåg & McKay, 2018; Nordfjaern, 2011; van Melick et al., 2013; Vigdal et al., 2022; Weisner et al., 2003). Research suggests either a positive, a negative or mixed association between drug-free relationships and recovery (McCrady, 2004), whereas we mainly found no association between alcohol and drug use, on the one hand, and drug-free friendships, on the other. Thus, the participants in our study may possibly have neither positive, nor negative drug-free friendships, which might explain why the friendships did not influence their alcohol or drug use. However, it may also reflect that the measure used in our study is not sensitive enough to capture this association.
Generally, positive drug-free friendships facilitate recovery maintenance (Lookatch et al., 2019), whereas having unsupportive drug-free friends curtails recovery (Dennis et al., 2007; Groh et al., 2008). In this respect, we may question the quality of the participants’ drug-free friendships in our study. The drug-free friendships reported may have been formed long before participants entered this study. When they were formed, the friendships may have been positive or negative, but the participants did not spend any or much time with them during follow-up. Perchance drug-free friendships may not influence the participants’ alcohol and drug use because they did not contribute any social support (nor were unsupportive). However, taking the abovementioned research into account, it seems very surprising that drug-free friendships, whether positive or negative, only influenced one of the five follow-ups on alcohol and drug use. If these friendships were actively present in these individuals’ life, they would presumably influence alcohol or drug use to some extent.
Gender and debut age
We found that neither gender, nor debut age had any significant association with drug use trajectories. Our result is contrary to previous research, showing that age of onset prior to 21 years, particularly prior to 15 years, is associated with higher substance use levels compared to people with higher onset age (Dennis et al., 2005; Poudel & Gautam, 2017; Scott et al., 2005). However, our sample size is smaller compared to the three previous studies and have a different research design which may explain the difference. Contrary to previous research (Grella et al., 2003; Hser et al., 2007; Simpson et al., 1997), our findings suggest that debut age may not reduce the possibility of recovery because it is not associated with alcohol and drug use trajectories. Studies show that early onset of substance use is a strong predictor of later regular use (Woodcock et al., 2015) and correlated not only with adverse health-related outcomes such as adolescent suicide, but also challenges at school (Piehler et al., 2012). Additionally, early onset has been related to a greater level of family deviance and deviant behaviour (Gordon et al., 2004) and experiencing childhood trauma has been associated with alcohol and drug use challenges (Mandavia et al., 2016). In this context, our findings warrant more research before firm conclusions can be drawn.
In terms of gender, our result implies that gender may not influence alcohol and drug use trajectories, thus indicating equal opportunities for males and females to achieve recovery. Our finding is contrary to previous research, which shows that women tend to have lower risks of relapse after recovery than men (Grella et al., 2008) and that there is a gender difference in substance use levels (Riley et al., 2018; Salom et al., 2016; Zakiniaeiz & Potenza, 2018). Recent studies on gender differences indicate different recovery mechanisms and mediators for women compared to men (Andersson et al., 2021). Thus, we would have expected a difference in alcohol and drug use trajectories between men and women in our study.
Implications of results
The stability in alcohol and drug use trajectories may suggest a need for long-term follow-up to reduce alcohol and drug use gradually over several years. This seems to be in agreement with previous research showing that alcohol and drug use reduction and abstinence takes many years (Dennis & Scott, 2007; Dennis et al., 2005; Heyman, 2013).
Our findings suggest that interventions other than drug-free friendships may be more relevant to facilitating recovery, such as employment or social networks (Ellis et al., 2004; McKay, 2017; Ness et al., 2014; Nesvåg & McKay, 2018; Nordfjaern, 2011; van Melick et al., 2013; Vigdal et al., 2022; Weisner et al., 2003). However, the literature also suggests that drug-free friendships may be positive, negative or mixed (McCrady, 2004). More research than our study is needed before any definite conclusion on excluding drug-free friendships can be drawn, insofar as our results seem counterintuitive given previous research showing positive effects (see limitations). We suggest a similar conclusion for our results on debut age and gender. Studies suggest a relationship between gender and recovery, and that debut age is associated with adverse health-related and social outcomes.
The stability in alcohol and drug use trajectories across 4 years suggests the need for more longitudinal research. It may be warranted to investigate the frequency and quality of drug-free friendships, participant friendship assessment, including what study participants associate with having a friend, and also whether the friendships are positive, negative or both to participants’ recovery.
Strengths and limitations
We consider it a strength that our study is one of the few longitudinal studies with social variables, gender and PSUD. However, the current understanding of gender identities suggests there are more than two genders. Because we only investigated the difference between two genders, we might have missed other gender differences. Our alcohol and drug use measures only yielded sum scores, which may be regarded as a limitation. Further, the DUDIT-C may be regarded as a crude measure of polysubstance use. The variable “drug-free friendships” is a dichotomous variable and does not yield information about the frequency and quality of drug-free friendships and participants’ friendship assessments. Thus, the measure may not be sufficiently sensitive, which may be indicated by the high scores in the cross-sectional analysis (Table 3). Further, the findings are based on a small dataset, and perhaps a more extensive dataset would yield one or more significant associations between SUD and drug-free friendships. For example, small samples have larger standard error estimates which affects the accuracy of statistical inferences. However, small sample size is a common challenge with longitudinal research (McNeish, 2019). Statistical methods were chosen on model complexity, sample size and research questions. The results may also be due to little variation in SUD and drug-free friendships, both at initial levels and in development. Further, a skewed age distribution towards younger people may be part of the reason why our findings differ from previous research. We have limited information about the participants’ diagnostic assessment and thus we have limited information about number of SUDs and the types of SUD they have. Our assessment of participants’ PSUD is based on their AUDIT and DUDIT scores showing that they use more than one substance. However, our assessment is not based on the initial diagnostic evaluation, which is a limitation. Lastly, we did not examine to which degree treatment (duration, amount, intensity) may have influenced the participants alcohol and drug use, which is a shortcoming.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.