
Abstract
Introduction
The Swedish strategy to handle the COVID-19 pandemic was mild in an international perspective, using voluntary and stepwise measures rather than lockdowns of society. Yet, numerous far-reaching restrictions were implemented in 2020 (Yarmol-Matusiak et al., 2021). For example, non-necessary travelling abroad as well as within the country, was dissuaded and the number of people allowed to meet for general gatherings were restricted to 50 and later to eight. A recommendation to work from home and to meet as few persons as possible from outside the household was issued, especially for those aged 70 years or above (Public Health Agency of Sweden, 2024). Restrictions were also implemented regarding the service of alcohol at on-licensed premises to avoid crowding. Thus, guests were not allowed to stand by the bar and opening hours were restricted (Public Health Agency of Sweden, 2020).
The outbreak and the restrictions had many consequences for the daily life of most Swedes, including possibilities to buy and consume alcohol. The restrictions on travelling greatly reduced the opportunity to buy cheap alcohol from abroad with travellers’ imports decreasing by 61% in 2020 compared to 2019, and purchases of smuggled alcohol decreasing by 44% (Trolldal & Åström, 2021). Furthermore, the restrictions regarding on-licensed premises were followed by a decline in drinking at these premises by 35% (Trolldal & Åström, 2021).
In addition to these restrictions on alcohol sales, regulations and recommendations regarding social activities, such as parties and festivals, reduced the opportunities to drink alcohol in Sweden. When summarising all statistics on sales and acquisition of alcohol in Sweden during 2020 as a whole, the total recorded sales within the country increased compared to 2019 with respect to pure alcohol per inhabitant aged 15 years and above, but the acquisition of alcohol from unrecorded sources decreased to a larger extent. The net effect was a decrease in consumption by 6% (Trolldal & Åström, 2021). This was in accordance with results based on self-reported consumption, where a decrease by 7% was found during 2020 compared to 2019 (Guttormsson, 2021). This decline was in line with studies in Finland (Jääskeläinen et al., 2022) and other European countries (Kilian et al., 2022; Leifman et al., 2022).
However, alcohol-related harm did not decline in Sweden as expected from the decline in drinking at least not in terms of alcohol-related mortality (Norström & Ramstedt, 2024). This suggests that, although most people drank less during the pandemic, some groups increased their drinking and thereby counteracted an expected decline in alcohol-related harm. This idea was also supported by the fact that there was no clear decrease in treatment seeking for alcohol-related issues during the pandemic despite declining drinking in general (Andersson & Håkansson, 2022).
The present study examined whether drinking increased due to the COVID-19 pandemic in Sweden in two groups that have been considered particularly vulnerable in this context and have been the focus of previous studies. These groups are those who had experienced financial problems, including unemployment, and those who had faced mental health issues due to the pandemic (Kilian et al., 2021; Lindqvist Bagge et al., 2024).
Financial problems affected many people in Sweden due to the pandemic following the economic crisis that was developed in several parts of the economy when the pandemic begun to spread on a larger scale. The job market became more uncertain, with rising levels of economic insecurity and unemployment (Campa et al., 2021; Juranek et al., 2021).
Unemployment is primarily associated with an increased alcohol consumption as a coping mechanism in this context (Amiri, 2022). However, unemployment, and financial difficulties in general, could also imply lower purchasing power in relation to alcohol and therefore a decrease in consumption (Babor et al., 2023; Rehm et al., 2020). In other words, the effect of financial difficulties, including unemployment, could be two-fold (de Goeij et al. 2015).
An increase in mental health problems due to the COVID-19 pandemic was found in many countries (Ahmed et al., 2023; Ornell et al. 2020; Salari et al., 2020), including Sweden (McCracken et al., 2020; Lindqvist Bagge et al., 2024). The main explanations for this development are the rise in social isolation and stress due to the pandemic and the restrictions. However, several studies of the pandemic found that mental health problems were associated with an increased alcohol consumption in many countries, such as in Australia (Batterham et al., 2022; Neill et al., 2020) the USA (Venanzi et al., 2022), Canada (Minhas et al., 2021; Wardell et al., 2020), the UK (Jacob et al., 2021) and the Netherlands (aan het Rot et al., 2023). The association between mental health problems and increased alcohol consumption has also been found during previous societal crises (Bell & Britton, 2014; Cerdá et al., 2011; de Goeij et al., 2015; Gonçalves et al., 2020; Keyes et al., 2012). However, evidence from the Swedish context is lacking. Against this background, the present study aimed to assess to what extent groups affected by financial difficulties, including unemployment, and/or mental health problems during the first year of the pandemic in Sweden increased their drinking despite the relatively less extensive restrictions compared to other countries. Given the likely overlap between financial difficulties and mental health problems (Kim & von dem Knesebeck, 2016), we also explored the possibility of a joint effect when estimating their association with alcohol consumption. More specifically, we used retrospective self-reported data from a large Swedish general cross-sectional population survey conducted during the second half of year 2020 (July to December) to answer the following questions:
Were experiences of financial problems due to the pandemic in Sweden related to an elevated risk of increasing drinking, and was the association modified by taking mental health into account? Were experiences of mental health problems due to the pandemic in Sweden related to an elevated risk of increasing drinking, and was the association modified by financial problems?
Given the indications in previous research that especially financial difficulties may also lead to a decline in drinking, we performed additional analyses assessing the likelihood of reporting decreasing consumption in relation to experiences of financial and mental health problems.
We hypothesised that experiencing mental health problems due to the pandemic was associated with increased alcohol consumption, whereas experiencing financial difficulties was related to both increasing and declining consumption.
Methods
Data
Data originates from a national cross-sectional general population survey encompassing 18,000 respondents each year. The survey has been in progress since the year 2001. The sample is randomly drawn from a register that covers approximately 70% of Swedish telephone numbers, in the population aged 17–84 years. Every fourth week, a base sample of one million telephone numbers stratified by age and gender is drawn. Within each stratum, a random sample is selected. From this sample, a weekly random sample of individuals is drawn. Each sample is in use for 4 weeks (Nyfjäll & Trolldal, 2022).
A message is sent to every person in the sample who has a mobile telephone. The message includes information about the survey and a link to a self-administrated questionnaire. Those who did not answer the questionnaire, or who only had a landline, were called by telephone after a week for an interview by telephone that included the same questions. Interviews are conducted until 1500 respondents have answered the questionnaire each month. The telephone interview took on average approximately 9 min depending on how many follow-up questions the respondent answered. The response rate was 33% in 2020. To assess the quality of the survey in terms of obtaining valid estimates of alcohol consumption, questions about purchases from monopoly stores were included. The aggregated self-reported purchases were compared with actual sales data from these stores. In 2020, the self-reported data closely aligned with the sales figures, with coverage rates of 87% for spirits, 94% for strong beer and 99% for wine.
During the second half of year 2020 (July to December) three specific questions regarding the pandemic and the effect on alcohol consumption, financial difficulties and mental health problems were added to the survey. The total number of respondents was 9122 during the study period. The study was approved by the Swedish Ethical Review Authority (Dnr 2020-04861).
Measurements
The three pandemic-specific questions on alcohol consumption, financial difficulties and mental health problems included the time frame from mid-March, when the pandemic began, to the point in time when the respondents answered the survey in the second half of 2020.
Outcome variables
The outcome variables of changes in alcohol consumption, were measured with the following question:
How have your alcohol consumption changed after the COVID-19 pandemic started in Sweden in mid-March compared to the same time-period last year?
The rationale for asking respondents to compare their consumption during the pandemic with the same time-period the previous year was to account for seasonal variations in alcohol consumption. The response options were: Increased/Not changed/Decreased/ Have stopped drinking alcohol during the pandemic/Have not consumed any alcohol during the pandemic, nor during the same period last year/Don’t know.
The response categories were divided into three groups: increased consumption, decreased consumption and no change. The categories were further divided into the following three main binary outcome measures: (a) any change in alcohol consumption (compared to no change); (b) increased alcohol consumption (compared to no change or a decrease); and (c) decreased alcohol consumption (compared to no change or an increase).
Exposure variables
To measure financial difficulties due to the pandemic, we used the following question that was inspired the question used by Kilian et al. (2021) in their study of the pandemic in 21 countries.
Have you experienced any negative consequences when it comes to your work or economy due to the COVID-19 pandemic? (For example, being out of work or reduced income.) Grade your answer on the scale, from 0 to 5: Not at all 0/1/2/3/4/5 To a very high degree/Don’t know. Has your mental health been negatively affected due to the situation around the COVID-19 pandemic? The same response options as above were given.
Mental health problems due to the pandemic were measured by this question:
The answers to these two questions were coded into two separate variables with three values each: those who did not experience any negative effects (0); those who experienced negative effects to a low or medium degree (1–3); and those who experienced negative effects to a high degree (4–5). The respondents who answered “Don’t know” were coded as missing cases and were excluded from the analyses.
Covariates
The following covariates were used in the analysis: gender, defined as the respondents’ legal gender (women, men), age (17–29, 30–49, 50–64 and 65–84 years) and highest completed education level (compulsory school (≤9 years), upper secondary school (11–12 years), tertiary education (13+)). Those who had completed compulsory school or upper secondary school, but were still studying, were upgraded one level, if they were aged 21 or 27 years at a maximum, respectively. In addition, a variable measuring the number of months the pandemic had lasted when the respondent answered the questions was also included, to account for the varying durations of the pandemic's impact on respondents.
Statistical analysis
Descriptive data of the study sample is presented in percentages. Binary logistic regression analysis was used to assess how alcohol consumption was affected by experiences of financial problems and mental health problems due to the pandemic. Changes in consumption included the three main outcome variables (any change, increased consumption, decreased consumption). Estimates are expressed as odds ratios (OR) with 95% confidence intervals (95% CI). The ORs express the odds of changes in alcohol consumption for each category of the exposure variable in comparison to the reference group. The logistic regression analyses were conducted in three steps. First, the relationship between each exposure variable and changes in alcohol consumption was analysed without any adjustment for covariates in a crude model (Model 1). Second, both exposure variables were included in the same model (Model 2). Third, fully adjusted models were used including the three covariates gender, age groups, level of education and participation month (Model 3).
Next, to assess a possible joint effect of experiencing both financial difficulties and mental health problems, a combined variable was included using a common reference category for the two exposures. The reference category was those not experiencing financial difficulties or mental health problems. Interactions on the additive scale were then calculated using Rothman's formula for relative excess risk due to interaction (RERI) (Rothman, 1986). The joint effect was calculated for the following two double-exposed groups: (a) the group experiencing low to medium degree of negative effects on the financial situation and on mental health due to the pandemic and (b) the group experiencing high degree of negative effects on the financial situation and on mental health due to the pandemic. The formula for the two joint effects was: (a) RERI = OR11 − OR10 − OR01 + 1 and (b) RERI = OR22 – OR02 – OR20 + 1. The RERI measures estimate whether the OR of the two factors together (OR11/OR22) is larger (or smaller) than the sum of the ORs of the two factors considered individually (OR01/OR02, OR10/OR20). CIs for RERI were calculated using the delta method (Hosmer & Lemeshow, 1992) as recommended by VanderWeel and Knol (2014).
Women, older people, highly educated, inhabitants born in Sweden, as well as people who live in rural areas, were over-represented among the respondents in the survey. Therefore, the data were weighted to account for the distribution of age (four categories), gender (2), population density in the municipality the respondents live (3), country of birth (born in Sweden or not) (2) and education level (2) (Nyfjäll & Trolldal, 2022). Stata, version 16.1, statistical software (StataCorp, 2019) was used in the analyses.
Results
The distribution of respondents
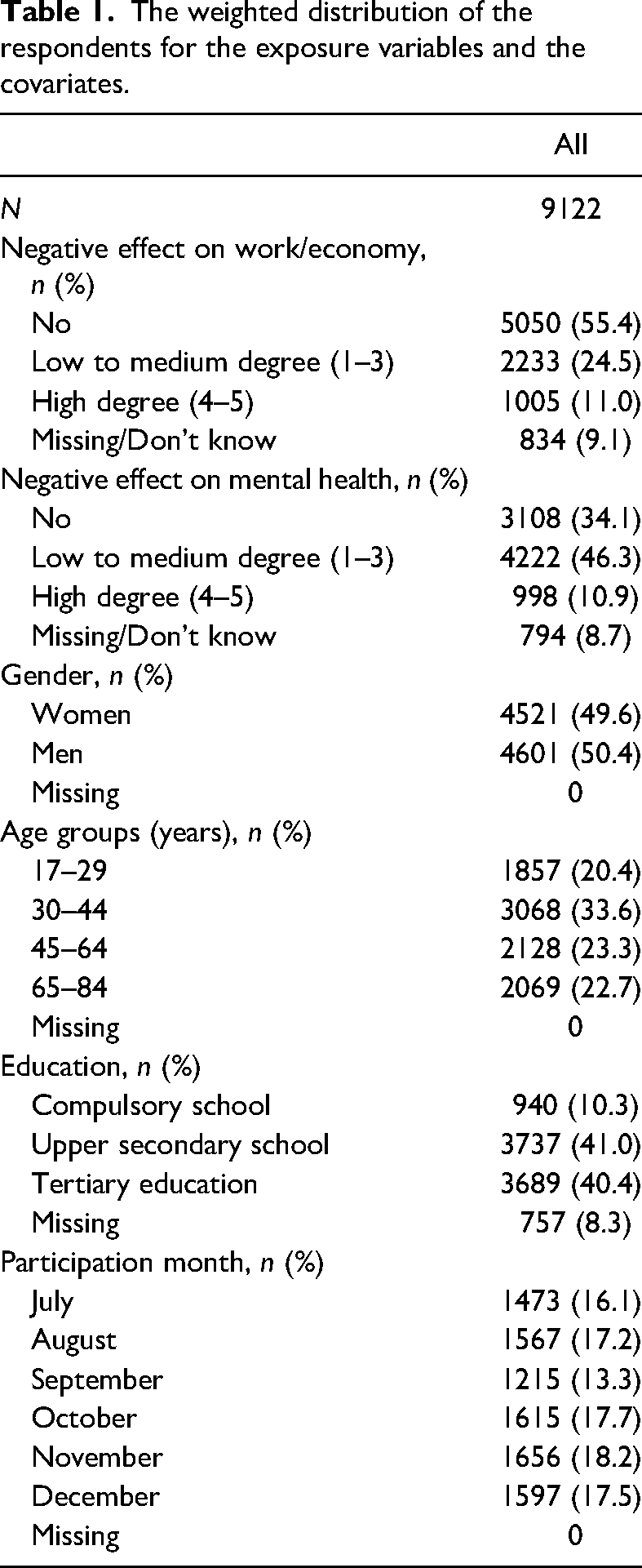
The weighted distribution of respondents for the exposure variables and the covariates is shown in Table 1. More than one-third (35.5%) of respondents reported financial problems due to the pandemic and a majority experienced negative effects on their mental health (57.2%). Approximately 11% experienced negative effects to a high degree for both financial and mental health problems. About 9% of the respondents did not respond to the questions or responded that they “don’t know”.
The weighted distribution of the respondents for the exposure variables and the covariates.
Changes in alcohol consumption
A clear majority (69%) of respondents reported no change in alcohol consumption during the study period 2020 compared to the same period 2019 (not shown). Among those reporting a change it was more common to report a decrease (17%) than an increase in drinking (5%). In addition, 9% answered that they did not know if they had changed their consumption.
The proportion of respondents who increased their consumption was larger among those who had experienced financial or mental health problems due to the pandemic and this proportion increased by severity in negative experiences (Table 2). A similar pattern was found in relation to decreasing consumption although with a somewhat weaker gradient. Thus, the proportion with any change in drinking increased with severity in experiences of financial and mental health problems and the proportion with unchanged drinking declined.
Changes in alcohol consumption divided by experienced financial difficulties and mental health problems.
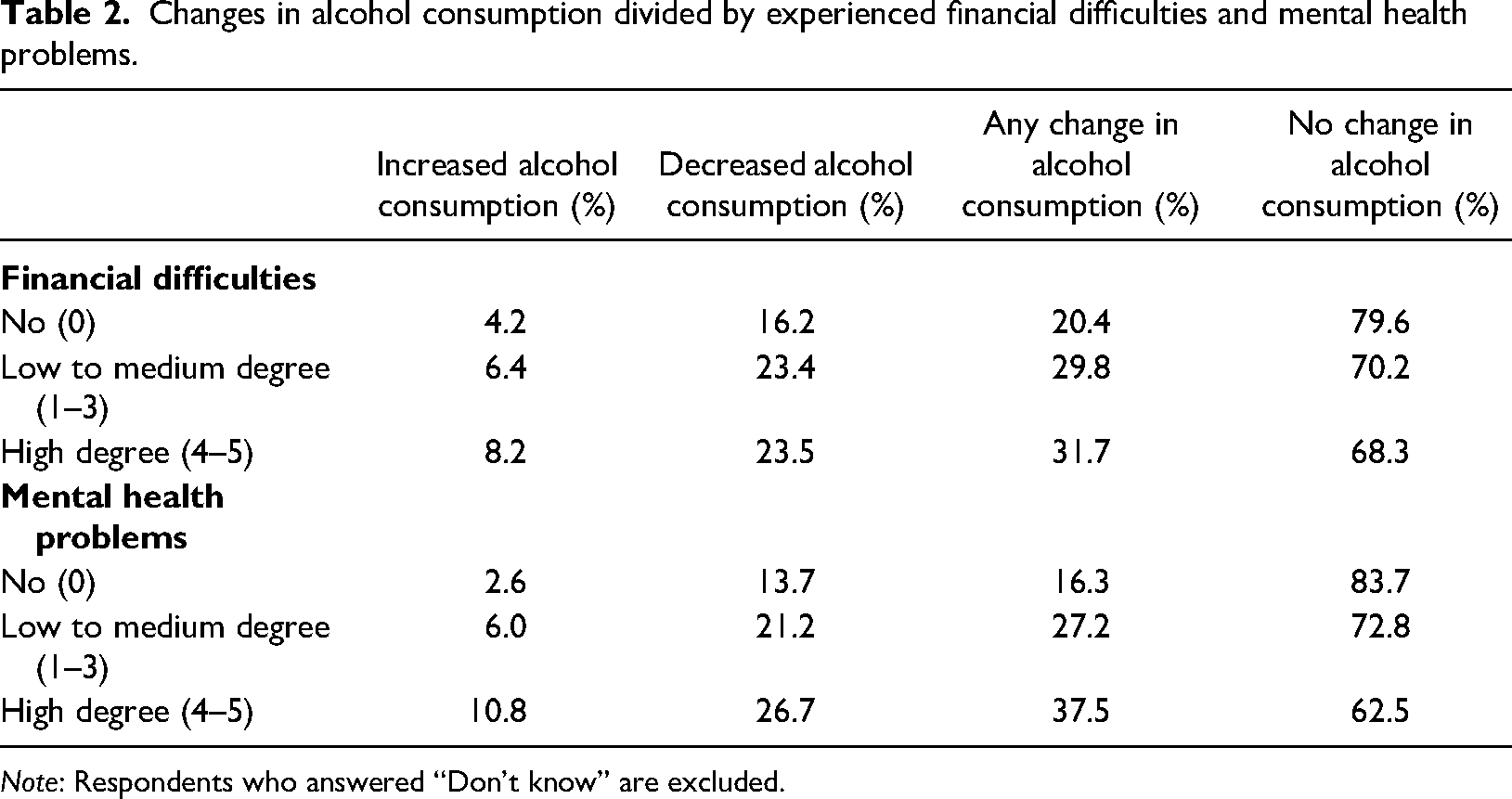
Note: Respondents who answered “Don’t know” are excluded.
Findings from logistic regression
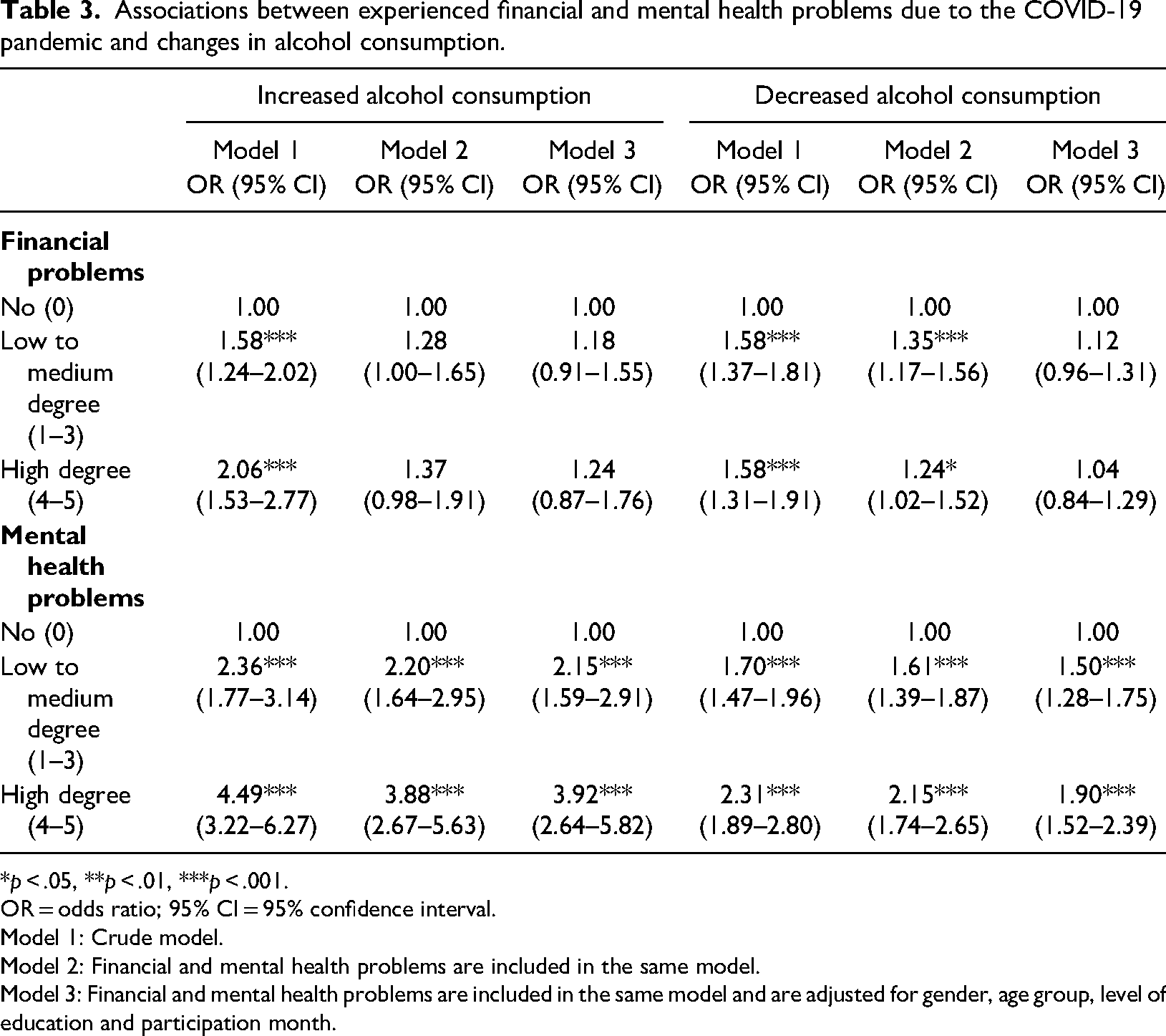
The findings from the logistic regression models are presented in Table 3. The results from the crude model (Model 1) resemble the results presented in Table 2. Respondents reporting experiences of financial and mental health problems due to the COVID-19 pandemic had significantly higher OR of an increase in alcohol consumption compared to those who did not experience such negative consequences. In general, the OR increased with severity of the negative consequences. Respondents who experienced negative consequences to a high degree had the highest OR of changes in alcohol consumption followed by those who experienced negative consequences to a low or medium degree. Experiencing financial problems to a low or medium degree was associated with 58% higher OR (OR = 1.58, 95% CI = 1.24–2.02) of increasing alcohol consumption, whereas experiencing financial problems to a high degree was associated with two times higher OR (OR = 2.06. 95% CI = 1.53–2.77). The corresponding OR for experiencing negative consequences on mental health was 2.36 (95% CI = 1.77–3.14) for a low to medium degree and 4.49 (95% CI = 3.22–6.27) for a high degree.
Associations between experienced financial and mental health problems due to the COVID-19 pandemic and changes in alcohol consumption.
*p < .05, **p < .01, ***p < .001.
OR = odds ratio; 95% CI = 95% confidence interval.
Model 1: Crude model.
Model 2: Financial and mental health problems are included in the same model.
Model 3: Financial and mental health problems are included in the same model and are adjusted for gender, age group, level of education and participation month.
When including both financial and mental health problems in the same model (Model 2), the strength of these associations decreased only slightly for experiencing negative consequences on mental health but more strongly for financial problems. Thus, the OR for increasing drinking due to financial problems to a low to medium degree decreased from 1.58 (95% CI = 1.24–2.02) to 1.28 (95% CI = 1.00–1.65) and from 2.06 (95% CI = 1.53–2.77) to 1.37 (95% CI = 0.98–1.91) for experiencing financial problems to a high degree. When also adjusting for gender, age group, level of education and participation month in Model 3, the OR was only significant for mental health problems, whereas statistical significance was not reached for financial problems.
The corresponding models estimating the association between financial problems and mental health problems in relation to decreased alcohol consumption showed a similar pattern. Thus, in the full Model 3, only experiences of mental health problems were significantly related to increased and decreased consumption. However, the estimate for mental health problems was larger for an increase in consumption (OR = 3.92; 95% CI = 2.64–5.82) in the full model than for decreasing consumption (OR = 1.90; 95% CI = 1.52–2.39).
Joint effects
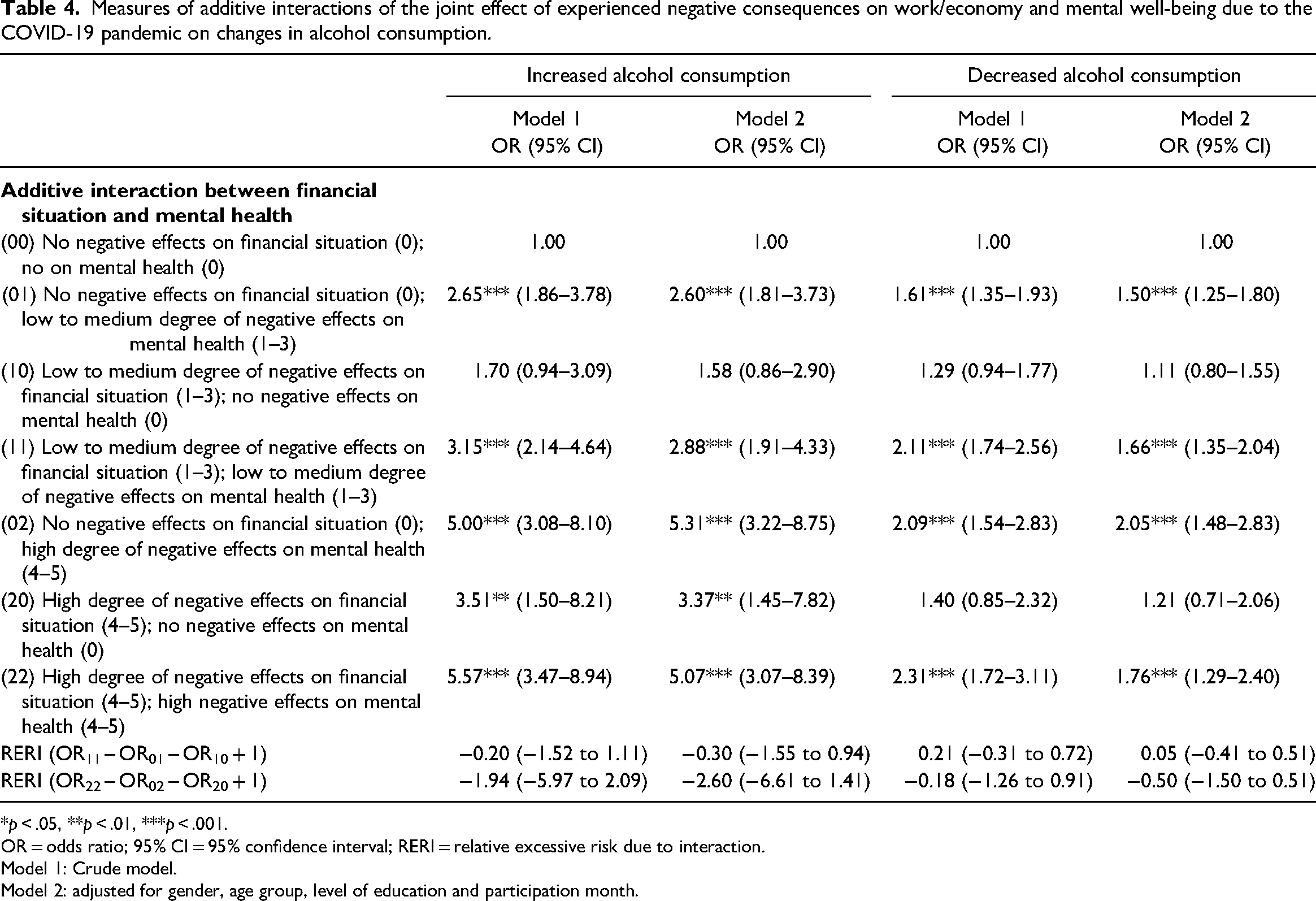
No joint effect was found for experiencing both financial problems and problems with mental health due to the COVID-19 pandemic in relation to increasing or decreasing alcohol consumption (Table 4). Hence, compared to the reference category (i.e., those that did not experience financial problems and negative consequences on mental health), the OR of the double exposed group (i.e., those who experienced both financial problems and mental health problems to a high degree) was not larger than the sum of the OR for the two single exposed groups. Similar results were found for the double exposed group that experienced negative consequences to a low to medium degree with respect to both financial and mental health problems.
Measures of additive interactions of the joint effect of experienced negative consequences on work/economy and mental well-being due to the COVID-19 pandemic on changes in alcohol consumption.
*p < .05, **p < .01, ***p < .001.
OR = odds ratio; 95% CI = 95% confidence interval; RERI = relative excessive risk due to interaction.
Model 1: Crude model.
Model 2: adjusted for gender, age group, level of education and participation month.
Discussion
Although the opportunities to buy and consume alcohol decreased in Sweden during the COVID-19 pandemic, those who experienced financial concerns, including unemployment, and those affected by mental health issues have been considered at risk for increased consumption as a coping strategy (Kilian et al., 2021; Lindqvist Bagge et al., 2024).
This concern is further supported by the observation that alcohol-related harm did not decrease as would have been expected given the decline in population-level drinking (Norström & Ramstedt, 2024). The present study therefore aimed to assess whether drinking increased among those affected by financial difficulties and mental health problems during the first year of the pandemic in Sweden, using data from a large general and representative population survey.
A larger part of the survey sample reported decreasing rather than increasing consumption, which is in line with previous findings of declining per capita alcohol consumption in Sweden during 2020 (Leifman et al., 2022; Trolldal & Åström, 2021).
In accordance with our hypothesis, a key finding was that negative impacts on mental health due to the pandemic were associated with increased drinking compared to those who did not report such impacts. This may be explained by alcohol consumption being a coping mechanism for the worries and anxieties triggered by the pandemic in this group (Avery et al., 2020). Furthermore, the results resemble those found in several other studies from various countries (Jacob et al., 2021; Minhas et al., 2021).
An intriguing finding was that experiences of mental health problems were also associated with an increased likelihood of decreasing consumption. To our knowledge, a decrease in consumption among individuals with mental health issues due to the pandemic has not been reported in previous research. These results could be related to specific circumstances during the pandemic such as social isolation and lower alcohol availability, which might have affected younger age groups to a larger extent. Additional analyses (analyses not shown; available from the corresponding author upon request) showed that the group with mental health problems who decreased their consumption was significantly younger than the group with an increased consumption.
A possible explanation could be that younger age groups normally drink alcohol in social settings with friends (e.g., in restaurants and bars) to a larger extent compared with older age groups (Ramstedt et al., 2018). When these opportunities for social interactions disappeared during the pandemic, the younger individuals contact with friends diminished, potentially impacting their mental health at the same time as drastically reducing opportunities for social drinking.
Overall, this variability in the results offers a nuanced perspective on the inherently complex relationship between COVID-19-related mental health issues and alcohol consumption. It also offers a complement to studies using aggregate level data showing no effect of the pandemic on mental health in terms of suicide and alcohol-related harm in terms of alcohol-related mortality (Norström & Ramstedt, 2024).
Another key finding was that the association between financial problems due to the pandemic and changes in drinking did not remain statistically significant when adjusting for mental health problems and the covariates. For example, when mental health was included in the model assessing the association between financial problems and increased drinking in Model 2, the increase was no longer statistically significant. This indicates that mental health problem was a mediator between financial problems and increased alcohol consumption. It is likely that financial problems may lead to a stressful situation impacting an individual's mental health status, which in turn impacts changes in drinking patterns. Associations between unemployment and mental health problems have been found in several former studies (Amiri, 2022; de Goeij et al., 2015). All in all, mental health problems due to the pandemic had a larger impact on changes in alcohol consumption than financial problems, including unemployment.
Additionally, our results could also be explained by the fact that the question of financial problems included both negative effects on the work situation (unemployment) and the financial situation (less money) and thus included mechanisms operating in opposite directions in relation to alcohol use (de Goeij et al., 2015).
A major strength of the present study was the use of a large and representative population sample and not a convenience sample, which was relatively common in other surveys addressing the effect of the pandemic (Kilian et al., 2021). The use of an extensive weighting procedure was another strength of this study.
There were some limitations to this study that need to be acknowledged. To begin with, it was based on cross-sectional data with well-known limitations for drawing causal conclusions. Although associations between experienced mental health problems due to the pandemic and changes in alcohol consumption were revealed, we cannot rule out a reversed association, such that changes in alcohol consumption led to increased mental health problems. In addition, we cannot rule out that the association between mental health problems and changes in drinking is explained by some other unmeasured factor. Another limitation was that respondents were asked retrospectively about whether their drinking changed compared to the same period in the previous year, implying a risk of bias and memory effects. However, retrospectively reported pandemic-related changes in alcohol use demonstrated fairly good accuracy in a comparison of retrospective reports and prospective data, especially reports of increasing drinking (Bartel et al., 2021). Even more reassuring in this case was that a larger proportion of respondents reported less drinking, which was in line with the overall decline in drinking based on sales statistics and data on acquisition from other sources (Trolldal & Åström, 2021).
Although the use of single-item measures used in this study has limitations in regard to reliability, similar measures have been employed in other studies examining related issues during the pandemic (Kilian et al., 2021).
The response rate is also of concern. However, to decrease the potential bias related to the non-response, all analyses included the extensive post-stratification weight that aimed to match the general population in terms of the under-represented subgroups of the analytic sample.
Conclusions
Our findings revealed a complex and heterogeneous association between mental health problems and changes in alcohol consumption at the individual level during the COVID-19 pandemic. While some individuals with mental health problems due to the pandemic increased their alcohol intake, likely as a coping mechanism, others reduced their consumption. This reduction may have been influenced by pandemic-related factors such as restricted alcohol availability or altered social routines. Taken together, this nuanced pattern highlights the importance of accounting for individual and contextual factors when examining the interplay between mental health and substance use during times of societal crises. Accordingly, further research is needed to increase our understanding of the mechanisms underlying these divergent patterns.
Footnotes
Data availability
The data used in the analysis are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Systembolaget's Research Council (Systembolagets Alkoholforskningsråd) SRA, Dnr 2020-0028.