
Abstract
COVID-19 was declared a pandemic in March 2020. Multiple cross-sectional studies conducted in various countries in the initial stage of the pandemic found the first lockdown to be associated with changes in alcohol consumption that varied between individuals (e.g., Avery et al., 2020; Capasso et al., 2021; Chodkiewicz et al., 2020; Garnett et al., 2021; Jacob et al., 2021; Stanton et al., 2020; Tran et al., 2020). While many individuals reported they did not change or decreased their drinking, across the cited studies 17%–31% reported to have increased their drinking. As this latter subgroup reported more drinking-associated problems (Chodkiewicz et al., 2020), it is considered at higher risk for alcohol use disorder (AUD).
Increased drinking after the start of the pandemic may have been due to increased anxiety. Several studies conducted in the first few months after the pandemic started have reported that adults who reported drinking more since the pandemic started also reported more general anxiety (Avery et al., 2020; Jacob et al., 2021; Lechner et al., 2020; Stanton et al., 2020; Tran et al., 2020). Wardell et al. (2020) reported a more specific link between health anxiety and increased alcohol consumption. Moreover, Capasso et al. (2021) found that adults drinking more since hearing about the COVID-19 outbreak were more anxious and unable to stop worrying about the outbreak. In general, these results fit well with past research showing that anxiety can cause people to drink more (see for example Anker & Kushner, 2019).
Among people experiencing COVID-19-related anxiety, alcohol consumption may have increased as a way to cope with this anxiety. In line with this idea, Anker and Kushner (2019) described alcohol consumption as being motivated by an effort to cope with anxiety. Indeed, several studies on drinking motives have found that drinking to cope increased after the start of the pandemic, whereas drinking to enhance positive affect, socialise with others, or conform to others decreased (Graupensperger et al., 2021; McPhee et al., 2020; Prestigiacomo et al., 2021). Moreover, both drinking to cope with negative affect (e.g., Irizar et al., 2021; McPhee et al., 2020; Prestigiacomo et al., 2021; Wardell et al., 2020) and, more specifically, drinking to cope with the pandemic (Fruehwirth et al., 2021) have been associated with drinking more during the first lockdown. In addition, drinking to cope with negative affect has been associated with drinking more during the second lockdown (Carbia et al., 2021).
Unlike all aforementioned studies, the present study was conducted one year after the pandemic started, after two lockdowns but with various public-health measures still in effect. Several studies conducted in the first few months of the pandemic (Avery et al., 2020; Capasso et al., 2021; Chodkiewicz et al., 2020; Garnett et al., 2021; Jacob et al., 2021; Stanton et al., 2020; Tran et al., 2020) found that while a majority of participants reported decreased or unchanged alcohol consumption compared to before the pandemic, a significant minority reported increased consumption. At least a proportion of this latter subgroup would likely continue their increased consumption beyond the acute phase of the pandemic. As also suggested by several studies conducted early in the pandemic (Capasso et al., 2021; Carbia et al., 2021; Wardell et al., 2020), this subgroup would be most likely to report anxiety. Specifically, we expected them be more likely to report clinically significant levels of COVID-19-related anxiety, assessed using the Coronavirus Anxiety Scale (CAS) (Lee, 2020). Other studies have generally used questionnaires that ask about general or health anxiety, which may have started before the onset of the pandemic.
In the present study, besides checking the aforementioned assumptions in a sample surveyed one year into the pandemic, we examined the role of drinking motives in the link between COVID-19-related anxiety and alcohol consumption. Given other results from studies conducted soon after the start of the pandemic (Carbia et al., 2021; Fruehwirth et al., 2021; McPhee et al., 2020; Prestigiacomo et al., 2021), we focused on drinking to cope, assessed using the Revised Drinking Motives Questionnaire (DMQ-R; Cooper, 1994). Taken together with the aforementioned anxiety-alcohol studies, these results led us to hypothesise that the association between COVID-19-related anxiety and increased alcohol use one year into the pandemic would be stronger among individuals who are relatively likely to drink to cope with negative affect. While this drinking motive has previously been found to moderate the link between anxiety and alcohol (e.g., Chinneck et al., 2018; Comeau et al., 2001; Hammarberg et al., 2017), none of these past studies were conducted during the COVID-19 coronavirus pandemic hence focused specifically on anxiety experienced in relation to the pandemic. If, in line with our hypothesis, alcohol use would indeed be higher in individuals with more COVID-19-related anxiety and a higher motivation to drink to cope with negative affect, then these individuals in particular would be at risk for drinking-related problems (assessed using the Alcohol Use Disorder Identification Test [AUDIT]) (Saunders et al., 1993). This could mean that these individuals might benefit from learning more adaptive coping strategies, which could possibly help prevent a long-term, pandemic-associated increase in both AUD and anxiety disorder.
Methods
Participants
This study was part of a larger project involving Alexandru Ioan Cuza University in Romania and the University of Groningen in the Netherlands. The project was approved by the Ethics Committee of Psychology of both universities and was carried out in accordance with their guidelines for human subject protection.
Advertisements on Facebook in April and May 2021 invited adults in Romania and the Netherlands to complete an online survey on why people drink (“to understand people's drinking motives”). Additional participants were recruited by sharing the link to the survey via the researchers’ personal networks. Informed consent was provided digitally by 868 of 1210 individuals who opened the survey (the other 28% did not answer the consent question).
The COVID-19 and alcohol questions were completed by 682 (79%) individuals. The preferred language was Romanian for 471 individuals, Dutch for 105 individuals, and English for 106 individuals (see Procedures). However, four individuals indicated that they understood their preferred language less than moderately well, leaving 678 individuals in the final sample.
Measures
COVID-19-related anxiety was assessed using the CAS (Lee, 2020), which had good internal consistency (Cronbach coefficient α: 0.81). Total scores ≥9 are thought to indicate clinically relevant anxiety in the past two weeks.
Alcohol consumption in the past month was assessed by asking about the number of drinks on an average Monday, Tuesday, etc. Data on the past year were collected by asking whether consumption decreased, stayed the same or increased, and using the AUDIT (Cronbach coefficient α: 0.83). The AUDIT assesses drinking-related problems and is used to screen for AUD (Saunders et al., 1993). Total scores ≥8 result in sufficient sensitivity and specificity when screening for a “strong likelihood of hazardous or harmful alcohol consumption”.
Motivations for consuming alcohol were assessed using the Revised Drinking Motives Questionnaire (DMQ-R) (Cooper, 1994), which contains four subscales: Coping with negative affect; Enhancing positive affect; Socializing with others; and Conforming to others (Cronbach coefficient α: 0.83–0.88).
Procedures
The survey was advertised in Romanian and English to Facebook users located in Romania and in Dutch and English to Facebook users located in the Netherlands. After interested individuals opened the survey and indicated their preferred language, the study proceeded in that language. A brief study overview was followed by more detailed information, which (unlike the advertisement) mentioned the pandemic as one factor of interest, and could be downloaded. Subsequently, consent to participate was obtained.
The survey contained several parts: demographics; COVID-19; alcohol; and empathy (not considered here). After completing these parts, participants were debriefed, encouraged to contact the researchers in case of questions and given the option to partake in a lottery for an online 25-RON / 10-EUR gift certificate.
Data analyses
Analyses were performed in SPSS version 25. Gender was originally coded male, female, non-binary, prefer not to say, but recoded to 0 = male, 1 = female, 2 = unknown, as only six individuals chose one of the other options. Age was originally coded <18, 18–25, 26–35, 36–45, 46–55, 56–65, >65 years but recoded to 0 = 18–25 years, 1 = 26 + years, as most participants were young adults (while none were aged <18 years). Language was considered a covariate in all analyses because the three language subgroups differed on several demographic and drinking variables (see Supplementary Table 1). Effect sizes were calculated from relevant F or t statistics and expressed as Cohen's d values.
Before testing our hypothesis on drinking to cope as a moderator of the association between COVID-19-related anxiety and alcohol consumption, we calculated the proportion of participants who reported increased consumption since the start of the pandemic, using their answer to the question of how their consumption changed in the past year. Besides, using three separate analyses of covariance (ANCOVAs), we compared this subgroup to the subgroups whose alcohol consumption decreased or did not change, in terms of AUDIT scores, number of weekly drinking days and number of weekly drinks. Post-hoc simple comparisons between the three subgroups were Bonferroni-corrected.
We also calculated the proportion of participants who reported clinically significant COVID-19-related anxiety, using their CAS score, both in the total sample and in the three aforementioned subgroups. Moreover, we tested the association between COVID-19-related anxiety and alcohol consumption in three ways. First, we examined CAS scores as a predictor of AUDIT scores, number of weekly drinking days and number of weekly drinks using three separate hierarchical linear regressions. Block 1 included the dummy-coded covariate and block 2 included the predictor variable. Second, ANCOVAs were used to examine the clinical relevance of the findings: dichotomised CAS scores were entered as the predictor variable and the three drinking variables were serially entered as outcomes. Third, using another ANCOVA, we compared the CAS scores of the subgroup whose alcohol consumption increased in the past year to the other two subgroups. Post-hoc simple comparisons between the three subgroups were again Bonferroni-corrected.
Finally, we tested our hypothesis on drinking to cope as a moderator of the association between COVID-19-related anxiety and alcohol consumption. In fact, we examined all four drinking motives identified by the DMQ-R as potential moderators. CAS scores and the four DMQ-R subscale scores were all standardised, and four CAS-by-subscale interaction terms were created. In separate regressions, block 1 included the covariate, block 2 the standardised CAS scores, block 3 one of the DMQ-R subscales and block 4 the relevant interaction term.
Of note, as most participants were Romanian (69%), we also conducted sensitivity analyses in the Romanian subsample only. Thus, we repeated all aforementioned analyses using Language as a selection variable rather than as a covariate.
Results
Descriptives
Our final sample was 56% male and 53% of participants were aged 18–25 years. The mean CAS score was 6.02 ± 2.1. The mean AUDIT score was 7.77 ± 5.9. The mean number of days that participants drank was 3.46 ± 2.1 days with a mean of 9.54 ± 10.9 drinks per week. AUDIT scores were strongly positively associated with the number of weekly drinking days (r = 0.55) and with the number of weekly drinks (r = 0.69). The number of weekly drinking days was strongly positively associated with the number of weekly drinks (r = 0.67).
Participants were most likely to drink to socialize with others (M = 13.20 ± 5.1) then to enhance positive affect (M = 11.32 ± 4.9), then to cope with negative affect (M = 9.15 ± 4.6) and then to conform to others (M = 6.62 ± 2.8). All four DMQ-R subscales were positively associated with AUDIT scores (moderately to strongly, r = 0.32–0.58) as well as with the weekly number of drinking days and with the weekly number of drinks (weakly to strongly, r = 0.16–0.58). The highest correlations were with the Coping subscale.
Changed alcohol consumption during the first year of the COVID-19 pandemic
While 42% of participants reported decreased alcohol consumption in the past year and 43% reported unchanged alcohol consumption, 15% reported an increase. Table 1 shows that this latter subgroup, compared to both other subgroups, had higher AUDIT scores and reported more weekly drinking days and more weekly drinks. The rate of clinical AUDIT scores in this subgroup was 52%, compared to 34% and 39% in the subgroups that reported decreased or unchanged alcohol consumption, respectively.
Change in drinking as a function of COVID-19-associated anxiety and drinking
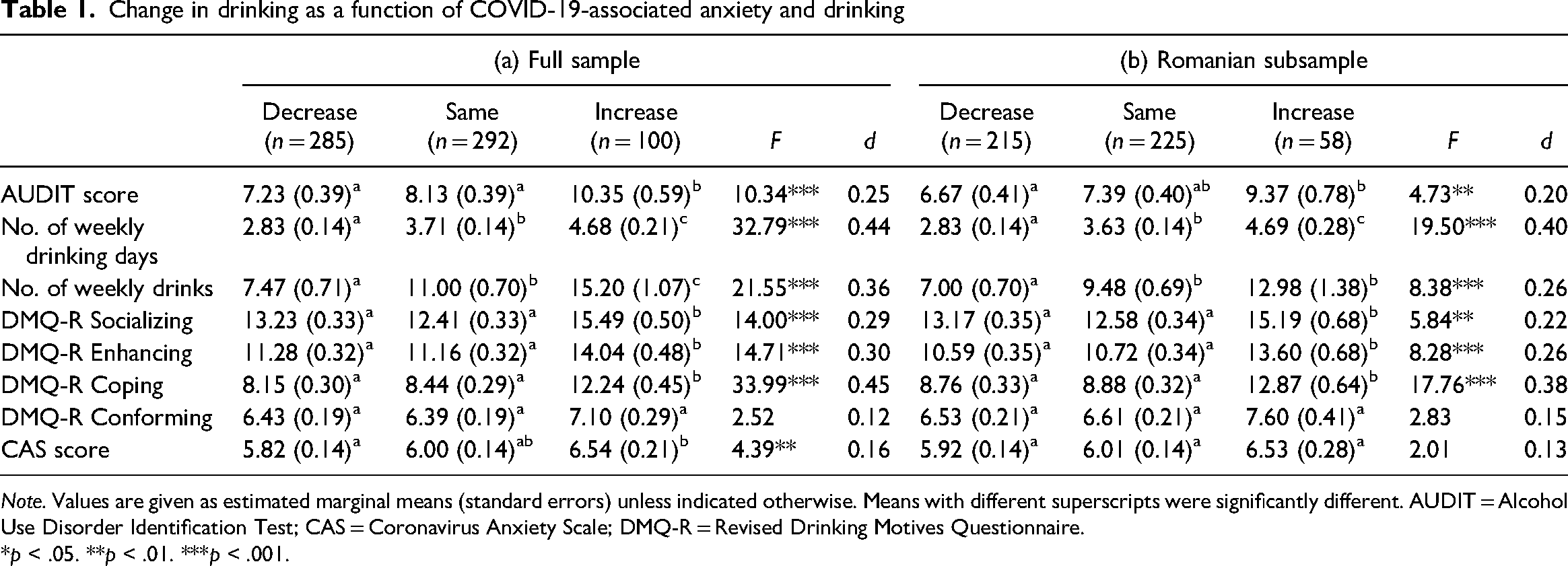
Note. Values are given as estimated marginal means (standard errors) unless indicated otherwise. Means with different superscripts were significantly different. AUDIT = Alcohol Use Disorder Identification Test; CAS = Coronavirus Anxiety Scale; DMQ-R = Revised Drinking Motives Questionnaire.
*p < .05. **p < .01. ***p < .001.
Table 1 also shows that, compared to the other subgroups, the subgroup that reported increased alcohol consumption scored higher on all drinking motives except drinking to conform to others. The largest effect was for drinking to cope with negative affect.
COVID-19-related anxiety and its link with alcohol use
Overall, clinical CAS scores were reported by 11% of participants. In the subgroup that reported increased alcohol consumption, the rate was 19%, compared to 8% and 12% in the subgroups who reported decreased or unchanged alcohol consumption, respectively.
As indicated, we tested the association between COVID-19-related anxiety and alcohol use in three ways. First, in separate regressions, higher CAS scores were associated with higher AUDIT scores (d = 0.50), a higher number of weekly drinking days (d = 0.29) and a higher number of weekly drinks (d = 0.27). See Table 2a for statistical details. Second, in separate ANCOVAs, clinical CAS scores were associated with higher AUDIT scores (F(1,674) = 27.96, p < .0001, d = 0.41), a higher number of weekly drinking days (F(1,668) = 10.55, p < .002, d = 0.25) and a higher number of weekly drinks (F(1,668) = 5.99, p < .02, d = 0.19), indicating that participants with clinically relevant COVID-19-related anxiety consumed more alcohol and reported more drinking-related problems (Figure 1a). Third, the subgroup that reported increased alcohol consumption in the past year had higher CAS scores than the subgroup that reported decreased consumption (p < .01) (Table 1a). The difference with the other subgroup was not significant after Bonferroni correction (p = .06).
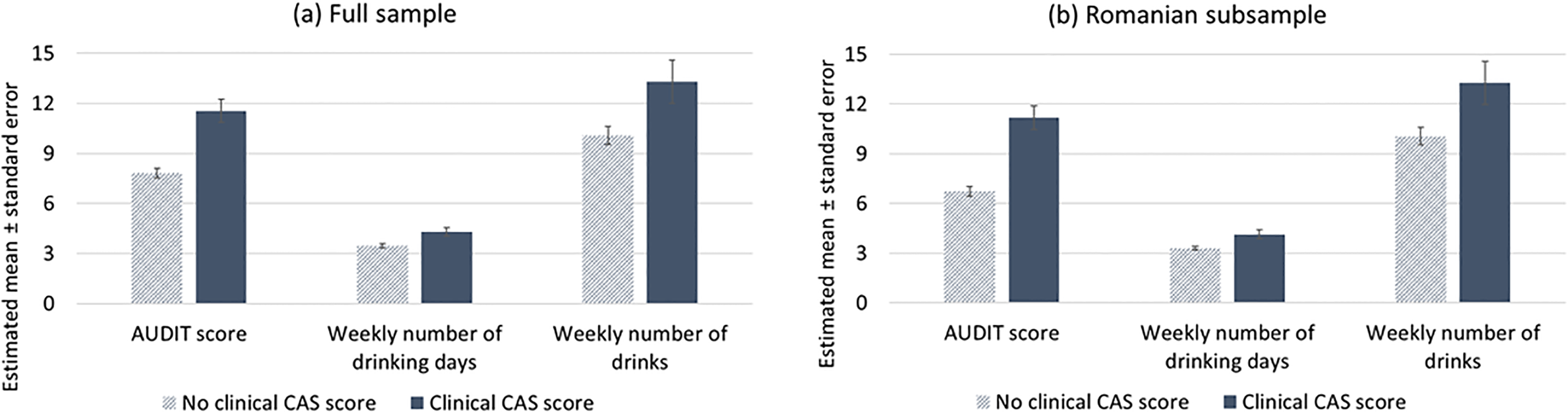
Alcohol use as a function of clinically relevant levels of COVID-19-related anxiety. Note. AUDIT = Alcohol Use Disorder Identification Test; CAS = Coronavirus Anxiety Scale. Results in full sample derived from ANCOVAs that included language (Romanian, Dutch, English) as the covariate. ANCOVAs that also included gender and age as covariates showed comparable results.
Regressions of the various drinking variables onto COVID-19-related anxiety.
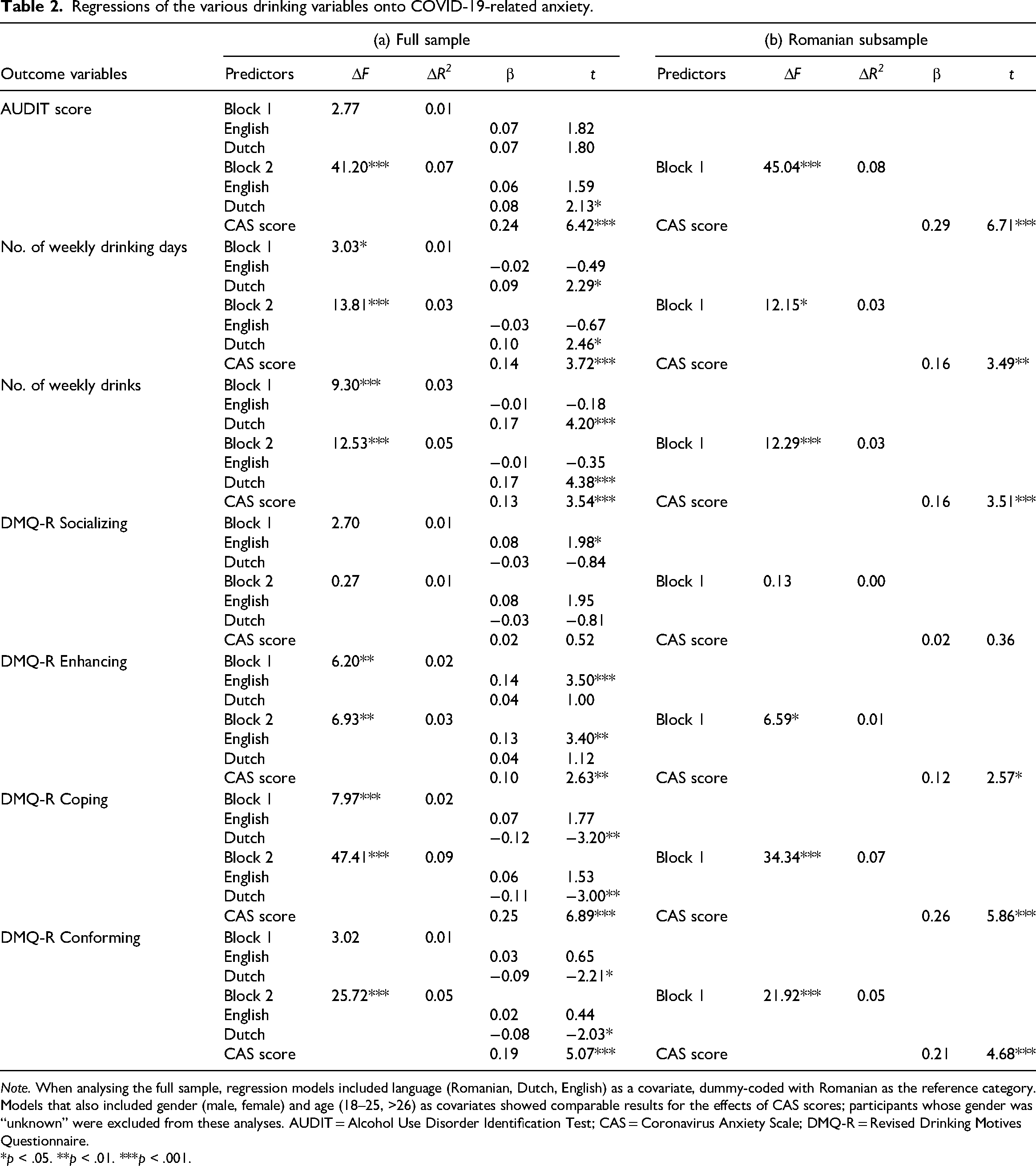
Note. When analysing the full sample, regression models included language (Romanian, Dutch, English) as a covariate, dummy-coded with Romanian as the reference category. Models that also included gender (male, female) and age (18–25, >26) as covariates showed comparable results for the effects of CAS scores; participants whose gender was “unknown” were excluded from these analyses. AUDIT = Alcohol Use Disorder Identification Test; CAS = Coronavirus Anxiety Scale; DMQ-R = Revised Drinking Motives Questionnaire.
*p < .05. **p < .01. ***p < .001.
Table 2a also shows that, in separate regressions, higher CAS scores were associated with higher scores on the DMQ-R Enhancing (d = 0.20), Coping (d = 0.53) and Conforming subscales (d = 0.39), whereas the association with scores on the DMQ-R Socializing subscale was not significant (d = 0.04). Similarly, in separate ANCOVAs, clinical CAS scores were associated with scores on Enhancing (F(1,674) = 3.90, p < .05, d = 0.15), Coping (F(1,674) = 38.89, p < .0001, d = 0.48) and Conforming (F(1,674) = 11.44, p < .002, d = 0.26), while there was no significant association with scores on Socializing (F(1,674) = 0.08, p = .78, d = 0.02). The largest effects were again for drinking to cope with negative affect.
Drinking motives as moderators of the anxiety–alcohol link
All four DMQ-R subscales were positively intercorrelated (r = 0.31–0.72). The highest correlation was between the Socializing and Enhancing subscales; the lowest correlation was between the Conforming and Enhancing subscales.
When examining the four subscales as a moderator of the association between CAS scores and AUDIT scores, the interaction term was not significant for three subscales, namely Socializing (β = −0.02, t(672) = −0.63, p = .53), Enhancing (β = 0.01, t(672) = 0.21, p = .84) and Conforming (β = −0.01, t(672) = −0.11, p = .91). Indeed, Coping was the only drinking motive to moderate the association between CAS scores and AUDIT scores, as indicated by a significant Coping by CAS interaction (β = 0.08, t(672) = 2.02, p < .05). This interaction is visualized in Figure 2a and shows a link between COVID-19-related anxiety and drinking-related problems among participants who were more likely to drink to cope with negative affect but not among participants were less likely to drink to cope with negative affect.
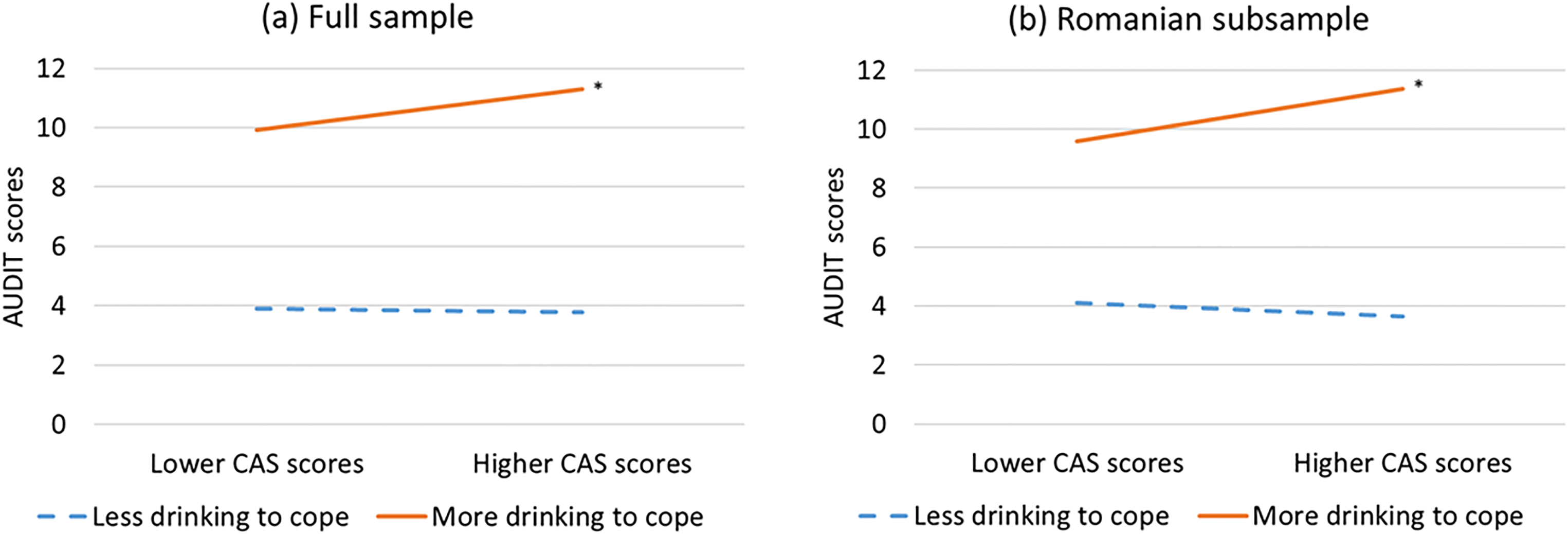
Drinking to cope as a moderator of the anxiety-drinking association. Note. AUDIT = Alcohol Use Disorder Identification Test; CAS = Coronavirus Anxiety Scale. Lower versus higher CAS scores were visualized by taking 1 standard deviation below or above the CAS mean, respectively. Similarly, less versus more drinking to cope was visualized by taking 1 standard deviation below or above the DMQ-R Coping subscale mean. The regression model for the full sample included language as the covariate, dummy-coded with Romanian as the reference category. Models that also included gender (male, female) and age (18–25 years, >26 years) as covariates showed comparable results; participants whose gender was “unknown” were excluded from this model. * p < .05.
Sensitivity analyses
While 43% of Romanian participants reported decreased alcohol consumption in the past year and 45% reported unchanged alcohol consumption, 12% reported an increase. This subgroup included 45% with clinical AUDIT scores, had higher mean AUDIT scores, reported more weekly drinking days and more weekly drinks, and scored higher on all drinking motives except drinking to conform to others (see Table 1b). This is similar to the full sample.
Clinical CAS scores were reported by 13% of Romanian participants. In the subgroup that reported increased alcohol consumption, the rate was 24%. Clinical CAS scores were associated with higher AUDIT scores (F(1,497) = 32.47, p < .0001, d = 0.51), a higher number of weekly drinking days (F(1,477) = 8.02, p < .006, d = 0.26) and a higher number of weekly drinks (F(1,477) = 6.90, p < .01, d = 0.24) (Figure 1b), and also with higher scores on Enhancing (F(1,470) = 5.21, p < .03, d = 0.21), Coping (F(1,470) = 26.98, p < .0001, d = 0.48) and Conforming (F(1,470) = 9.91, p < .003, d = 0.29). Similarly, higher CAS scores were associated with higher AUDIT scores (d = 0.61), a higher number of weekly drinking days (d = 0.32), a higher number of weekly drinks (d = 0.32) and higher scores on the DMQ-R Enhancing (d = 0.24), Coping (d = 0.54) and Conforming subscales (d = 0.43) (Table 2b). Thus, even when only Romanian participants were considered, we found that COVID-19-related anxiety was positively associated with alcohol consumption, drinking-related problems, and a higher motivation to drink to enhance positive affect, cope with negative affect, or conform to others.
When examining the four subscales as a moderator of the association between CAS scores and AUDIT scores in the Romanian participants only, the interaction term was again only significant for the Coping subscale (β = 0.12, t(464) = 2.76, p < .007). There was a link between COVID-19-related anxiety and drinking-related problems among Romanian participants who were more likely to drink to cope with negative affect but not among Romanian participants were less likely to drink to cope with negative affect (Figure 2b). Overall, results obtained in the full sample were replicated in the Romanian subsample.
Discussion
We found that 15% of our participants reported increased alcohol consumption in the first year of the COVID-19 pandemic. In the Introduction, we cited several studies that reported rates of 17%–31% when only considering the first months of the pandemic. Moreover, a study in 21 European countries found an average (substantial) increase in alcohol consumption in 22% of participants during the first months (Kilian et al., 2021). Together, these findings could mean that for many people, drinking more might not have been a temporary reaction to the pandemic. Recent longitudinal data also suggest that a substantial proportion of adults may have continued drinking more as the pandemic continued after the initial lockdown (Riehm et al., 2022).
This might be due to increased anxiety levels. Indeed, we found that participants who reported drinking more during the first year of the pandemic reported more COVID-19-related anxiety and were more likely to report clinical levels of COVID-19-related anxiety than participants who reported drinking less (Table 1). Further, we found that participants with more COVID-19-related anxiety reported more weekly drinking days and more weekly drinks (Table 2). Furthermore, although the proportion of explained variance was small, we found that the subsample with clinical levels of COVID-19-related anxiety reported more problematic alcohol consumption (Figure 1), indicating an increased risk of AUD (Allen et al., 1997). All in all, these findings correspond with those of Capasso et al. (2021), who reported that adults drinking more during the first lockdown were more anxious and unable to stop worrying about the COVID-19 outbreak; with another recent study in young adults in which COVID-19-related worry was cross-sectionally associated with alcohol-related problems (Haag et al., 2022); and with a recent longitudinal study in which COVID-19-related worry during the initial lockdown positively predicted drinking-related problems in young adults three months later (Venanzi et al., 2022). Moreover, the findings are in line with the high co-morbidity of anxiety disorder and AUD (Anker & Kushner, 2019): as participants who increased their drinking after the pandemic started were most likely to report both COVID-19-related anxiety and alcohol problems, they in particular may be at risk for both disorders.
The main and most novel finding of our study was that drinking to cope strengthened the link between COVID-19-related anxiety and drinking-related problems (Figure 2). This drinking motive was previously found to be strongly associated with problematic alcohol use in individuals with an anxiety disorder (Anker & Kushner, 2019). Our present finding is more specific and also timely, as it could be taken to mean that individuals who tend to drink to cope and who develop clinical levels of COVID-19-related anxiety during the pandemic are most likely to drink more during the pandemic and develop alcohol problems. If (and only if) this finding were replicated in a longitudinal study, it could have clinical implications. Interventions that promote more adaptive coping strategies, such as positive reframing (Chodkiewicz et al., 2020), might help reduce both COVID-19-related anxiety and problematic alcohol use.
One limitation of our study, but also of most cited studies, was its cross-sectional nature. This means we could not infer any causal relations from the established anxiety–alcohol link. In one longitudinal study (Graupensperger et al., 2021), the number of drinking days increased but the number of weekly drinks did not change significantly from before to after the start of the first lockdown, which could mean that our retrospective measure of increased drinking (and that of most other cross-sectional studies) was imprecise. Moreover, several factors potentially contributing to increased drinking during the pandemic were not considered, such as having a child at home, social isolation, or depression (Wardell et al., 2020). In addition, as Garnett et al. (2021) found that adults with an anxiety disorder were more likely to report increased drinking soon after social distancing started, increased drinking more may not only be due to the emergence of COVID-19-related anxiety.
We note that we used a convenience sample in which over 50% of participants were young adults who originated from different cultural backgrounds, but who were primarily Romanian. Although a sensitivity analysis showed comparable results in the Romanian subsample, our findings may not generalise to older (Romanian) adults. For example, it is possible that young adults were more likely to increase their alcohol consumption even after the first few months of the COVID-19 pandemic compared to older adults, putting them at higher risk for drinking-related problems.
Another limitation concerns the exclusive use of self-report measures of drinking and anxiety, which are considered relatively sensitive to social desirability bias (Latkin et al., 2017). However, participants could complete the online survey anonymously, which may have promoted accurate disclosure of drinking and anxiety. Besides, the timeliness of the research topic may have reduced social desirability bias.
Overall, our study extends previous anxiety–alcohol research conducted during the first few months of the COVID-19 coronavirus pandemic (Avery et al., 2020; Chodkiewicz et al., 2020; Jacob et al., 2021). Moreover, although we acknowledge its cross-sectional nature, the study provides indirect support for the idea that drinking to cope with COVID-19-related anxiety could explain why a substantial proportion of (young) adults reported increased drinking during the first year of the pandemic.
Supplemental Material
sj-docx-1-nad-10.1177_14550725221147111 - Supplemental material for Increased alcohol use to cope with COVID-19-related anxiety one year into the coronavirus pandemic
Supplemental material, sj-docx-1-nad-10.1177_14550725221147111 for Increased alcohol use to cope with COVID-19-related anxiety one year into the coronavirus pandemic by Marije aan het Rot, Isabelle C. Baltariu and Violeta Enea in Nordic Studies on Alcohol and Drugs
Footnotes
Acknowledgements
The authors thank Nidhi B. Chauhan and Sjoukje Sinnema for assistance in data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.