
Abstract
Injuries and self-destructive behaviour are leading causes of disability and mortality among youth in Finland (Korpilahti & Kolehmainen, 2016) as well as in other Western countries (Dalsgaard et al., 2015; Vincenten, 2005; WHO, 2022). Children and youth with prenatal substance exposure (PSE) are at heightened risk for injuries and poisoning because of many interwoven risk factors deriving from the exposure itself as well as from several child and childcare environment adversities. Despite that, knowledge of the prevalence of injuries and poisoning in comparison to normative youths is lacking.
Gestational exposure to alcohol and/or drugs may cause impaired cognitive functioning manifesting as attention-deficit/hyperactivity disorder (ADHD), difficulties in executive function, and other mental and behavioural problems (Irner, 2012; Mattson et al., 2019; Weyrauch et al., 2017). It is assumed that these problems increase the likelihood of engaging in maladaptive, high-risk and criminal behaviour (Streissguth et al., 2004; Wyper & Pei, 2016). In the study by
Studies among normative samples report an association between inattention, hyperactivity, impulsivity and increased injury-proneness peaking in adolescence and young adulthood (Amiri et al., 2017; Brunkhorst-Kanaan et al., 2021; Chang et al., 2014; Dalsgaard et al., 2015; Mytton et al., 2009; Rivara, 1995). In the study by Rowe et al. (2004), depression and anxiety were also associated with some unintentional injury types. The review by Ruiz-Goikoetxea et al. (2018) suggests that ADHD is also associated with a significantly higher risk of poisoning.
In addition to the risk derived from PSE itself, the risk of injuries is increased by suboptimal parenting and caregiving environments. Studies on infants with PSE report hospitalisations and clinic visits for suspected maltreatment (Austin et al., 2022). Smith et al. (2007) found high levels of maltreatment among preschoolers with PSE placed in foster care. In the study by Crandall et al. (2006), maternal alcohol use and spanking the child were the strongest independent risk factors for child injury during the first year of life. Raitasalo et al. (2015) and Woodside et al. (1993) found a higher rate of inpatient admissions because of injuries and poisoning among small children of mothers with an alcohol problem but without verified alcohol exposure. The rates were even higher if the mother used both alcohol and drugs (Raitasalo et al., 2015), and if both parents were substance abusers (Raitasalo & Holmila, 2017).
Parental substance abuse is strongly related to low education, low household income, single-parent household and mental health problems (Koponen et al., 2020a; Dube et al., 2001; Flannigan et al., 2021; Sarkola et al., 2007), which have been associated with an increased risk of childhood injury (Crandall et al., 2006; Nevriana et al., 2020; Ringbäck Weitoft et al., 2003; Sridharan & Crandall, 2011). Remes et al. (2010) showed that lower parental education was associated with the risk of offspring's death, especially regarding accidental and violent causes of death. In addition, male individuals are at excess risk of injuries (Brehaut et al., 2003; Rivara, 1995; Sridharan & Crandall, 2011) and mortality (Remes et al., 2010).
Many children with PSE are placed in out-of-home care (OHC) (Flannigan et al., 2021; Koponen et al., 2020a; Sarkola et al., 2007). One of the main purposes of OHC is to protect the child from maltreatment and possible injuries in care by the biological parents. Nevertheless, research suggests that children with OHC are at significant risk of ill health, including injuries and poisoning (Randsalu & Laurell, 2018; Sariaslan et al., 2022). In addition, mortality related to substance misuse, accidents and suicide is more common than in the general population (Kalland et al., 2001; Manninen et al., 2015; Vinnerljung, 1995). Outcomes of children in OHC may depend on the OHC type. The meta-analysis by Li et al. (2019) showed that children in foster care perceived their care as better and safer than did children in residential care.
To summarise, previous studies show that children and youths with PSE are exposed to many complex and interwoven environmental adversities, which may increase the risk of injuries and poisoning either directly (maltreatment, suboptimal parenting) or indirectly by increasing mental and behavioural problems (Koponen et. al., 2020a). It is important to understand the relationship between cumulative adversity and hospitalisations. Previous studies have typically focused on single or separate adversities and have been carried out among either normative samples, small children with parental substance abuse problem without verified PSE, or infants or preschoolers with PSE.
This longitudinal register-based cohort study extends knowledge about the prevalence of specialised healthcare for injuries and poisoning among youth with PSE and the associated risk factors. The aims of the study were as follows: (1) to compare in- and outpatient hospital care among youth with PSE (n = 615, aged 15–24 years) with matched unexposed controls (n = 1787); and (2) to investigate associations between single and cumulative risk factors, and hospital care. Our hypothesis was that cumulative child and maternal risks are related to child's risk of injuries and poisoning in both groups.
Methods
Data collection
The study cohorts consist of 615 PSE youths, born between 1992 and 2001, and 1787 matched unexposed age-mate controls. The mothers of the PSE youths were cared for at special antenatal clinics for mothers with substance abuse and drug problems at Helsinki University Hospital (HUS) during pregnancy. At each outpatient hospital visit, substance misuse (i.e., alcohol, cannabis, amphetamines, heroin, buprenorphine, non-medical use of drugs) was monitored by voluntary urine toxicology screenings, laboratory tests reflecting alcohol consumption (i.e., carbohydrate-deficient transferrin (CDT), haemoglobin-acetaldehyde adducts, mean cell volume (MCV), gamma-glutamyl transferase (GGT) (
The control cohort was obtained from the national Medical Birth Register. Three unexposed mother–child dyads were matched with each exposed mother–child dyad in order to have enough controls for comparison according to various background factors (e.g., OHC). The criteria were as follows: no evidence of maternal alcohol and/or substance misuse in any of the national health and social welfare registers; and the same maternal age, parity, number of fetuses, month of delivery and child delivery hospital (Kahila et al., 2010). Because matching was done for maternal characteristics only, children were not matched by sex. The proportion of boys among the born children in Finland is 51.1% (Statistics Finland, 2019). In the study cohorts, the proportion of boys among the PSE group is 49.3% and among the controls 51.7%.
Register data were obtained from the multiple mandatory national health and social welfare registers for each exposed and unexposed mother–child dyad. Data linkage of all registers was done by using the unique identification number assigned to each Finnish citizen at birth or at immigration. Mothers’ and children's identification numbers were concealed and replaced with study numbers after the data linkages. A detailed description of the data collection process is presented in
Ethics
The study was approved by the local ethical committee of HUS (Dnro 333/E8/02) and all register organisations providing data. No study participants were contacted. All register linkages were performed by a statistical authority (Finnish Institute for Health and Welfare, THL) and the data were analysed anonymously by researchers with research permission provided by the register keepers. According to Finnish law, informed consent is not required in register studies when study participants are not contacted.
Variables and register sources
The study included variables reflecting childhood adversities and OHC characteristics considered important for child neurocognitive and emotional development (Miguel et al., 2019; Shonkoff et al., 2009) and associated with injuries and poisoning (e.g., Nevriana et al., 2020; Ringbäck Weitoft et al., 2003). The following official registers were used as sources of information: Population Information System; Medical Birth Register; Care Register for Health Care (previously Hospital Discharge Register); Education Register; Register of Child Welfare; Cause of Death Register; Criminal Records Register; and Register of Social Assistance.
Outcome variable
The outcome variable was a primary diagnosis for injury, poisoning (e.g., drugs and medication) and certain other consequences of external causes (S00-T98): at least one inpatient episode (public and private hospitals, 1992–2016) or outpatient hospital visit (public hospitals, 1998–2016) with International Statistical Classification of Diseases and Related Health Problems ICD-10 codes S00-T98 (1996–2016) and the corresponding ICD-9 codes (1992–1995) based on the Hospital Discharge Register (1992–1993) and the Care Register for Health Care (1994–2016).
External causes of hospital visits
The external causes of hospital visits were as follows:
• External causes of injuries and poisoning: at least one inpatient episode with the following ICD-10 codes (1996–2016) and the corresponding ICD-9 codes (1992–1995): transport accidents (V01-V99); other accidental injury (W00-X59, E881A, E920X); intentional self-harm (X60-X84); assault (X85-Y09); event of undetermined intent (Y10-Y34, E960A); poisoning (E840A, E850A, E930A, E933D, Y90-Y91); and other external cause (Y40-Y89). The abovementioned causes of injuries and poisoning are not recorded for outpatient care in the data source.
• Alleged sexual abuse: at least one out- or inpatient episode with the following ICD-10 codes: examination and observation after alleged rape and seduction (Z044); and problems related with alleged sexual abuse of a child (Z614, Z615). The specific diagnostic code for rape is not commonly used in clinical work. Therefore, information on out- or inpatient visits for alleged sexual abuse was obtained from the Z codes in ICD-10, including factors influencing health status and contact with health services.
External causes of hospital visits for injuries and poisoning permit the classification of environmental events and circumstances as the cause of injury, poisoning and other adverse effects and should be used as an additional code (https://icd.who.int/browse10/2016/en#/XX).
Youth's background factors
Sociodemographic factors
The sociodemographic factors were as follows:
Sex (male, female) from the Medical Birth Register. Mortality (no, yes; date of death) from the Cause of Death Register. Native language (Finnish, Swedish, other) from the Population Information System. Completed secondary education (no, yes) from the Education Register.
Health in infancy
Prenatal substance exposure (alcohol/drugs)
The health of infants was determined as follows:
Fetal alcohol spectrum disorders (FASD) (no, yes), such as fetal alcohol syndrome (FAS), partial fetal alcohol syndrome (PFAS), alcohol-related neurobehavioual disorder (ARND), alcohol-related birth defect (ARBD) from the Register of Congenital Malformations. At least one inpatient episode or outpatient hospital visit with ICD-9 code 7607A or ICD-10 code Q86.0. FAS from the Hospital Discharge Register or Care Register for Health Care. Neonatal abstinence syndrome (NAS) (no, yes): medical records from the HAL clinics, Medical Birth Register and Hospital Discharge Register or Care Register for Health Care including inpatient episodes and outpatient hospital visits with ICD-9 code 7795 or ICD-10 code P96.1. Maternal smoking during pregnancy: exposure to mother's daily smoking (no exposure or mother stopped smoking after the first trimester, mother smoked throughout pregnancy) from the Medical Birth Register. Newborn health: gestational weeks at delivery (<37 weeks, ≥37 weeks); Apgar score at 1 min (0–6, 7–10); birth weight (<2500 g, ≥2500 g) from the Medical Birth Register.
Covariates
Mental or behavioural disorder (ICD-10)
Covariates were as follows:
Primary diagnosis for a mental or behavioural disorder (F00-F99). Primary diagnosis for a neurodevelopmental disorder: (1) F80-F89 Disorders of psychological development; (2) F90-F98 Behavioural and emotional disorders with onset usually occurring in childhood and adolescence. Primary diagnosis for a mental and behavioural disorder with onset in adolescence and adulthood (F10-F69). The primary diagnoses were based on at least one inpatient episode (public and private hospitals, 1992–2016) or one outpatient care episode (public hospitals, 1998–2016) provided with ICD-10 codes F00-F99, F80-F89, F90-F98, F10-F69 (1996–2016) or the corresponding ICD-9 codes (1992–1995) based on the Hospital Discharge Register (1992–1993) and Care Register for Health Care (1994–2016).
Adverse childhood experiences
Adverse childhood experiences were as follows:
Out-of-home care (no OHC, at least one episode; age at first episode; family placement only, institution/institution and family). Information on OHC between 1992 and 2016 is based on the Child Welfare Register. In the Finnish child welfare system, outpatient support is always offered first and OHC is only indicated if outpatient support has failed (Child Welfare Act, 2007). OHC ends at the age of 18 years, but extended aftercare services were available for OHC youth until age 24 years at the time of the study.
Maternal risk factors. Maternal risk factors were as follows:
Marital status at delivery (married, unmarried: single/divorced/widow) from the Medical Birth Register. Socioeconomic status at delivery, based on maternal occupation (high (self-employed/lower-level employee/upper-level employee), low (manual worker/student/pensioner/other)) from the Medical Birth Register. Mental or behavioural disorder: at least one outpatient or inpatient episode with a primary diagnosis for mental or behavioural disorder: ICD-9 codes (1987–1995) 290 and 293–319, and ICD-10 codes (1996–2016) F00-F09 and F20-F99 based on the Hospital Discharge Register or the Care Register for Health Care. Diagnosed substance abuse: at least one outpatient or inpatient episode with a primary or a secondary diagnosis or external cause for alcohol- and/or drug-related abuse: ICD-9 (1987–1995) codes: 291–292, 303–305, 3570, 4255, 5353, 5710, 5711–5713, 6483, 6555, 9650, and 9696–9697 and ICD-10 (1996–2016) codes E24.4, F10-F16, F18-F19, G31.2, G40.5, G40.51, G40.52, G62.1, G72.1, I42.6, K29.2, K70, K85.2, K86, O35.4-O35.5, P04.4, R78.0-R78.5, T40, T43.6, T50.2-T50.3, T51, Z71.4, Z72.1-Z72.2, X45, and X69 based on the Hospital Discharge Register or the Care Register for Health Care. Criminal record (no sentence, at least one sentence during 1985–2018) from the Criminal Records Register. Social assistance (no long-term social assistance, long-term social assistance [10–12 months during a 1-year period]) in 2002–2016 from the Register of Social Assistance. Social assistance is the last-resort financial assistance for individuals and families to guarantee a minimum standard of living.
Statistical methods
Descriptive analyses
In the first phase of the analysis, the total proportion of the PSE group and controls with at least one out- or inpatient hospital care episode due to injury or poisoning (S00-T98) was calculated. The follow-up time was from birth to the end of December 2016. To get more detailed information about the causes of injuries and poisoning, external causes of hospital care episodes among the PSE group and controls were analysed. In the descriptive analyses, Pearson’s chi-square test or Fisher's exact test was used.
Bivariate analyses
Bivariate associations between each possible child and maternal risk factor and hospital care for injuries or poisoning (outpatient or inpatient care, S00-T98) were analysed separately among the PSE and control cohorts to explore whether the risk factors were similar in both groups. Child age at maternal risk factor occurrence (e.g., child's age at mother's first hospital care episode for mental or behavioural disorder) was taken into account in these analyses. The cut points were before/after birth and before/after school age (<7 / ≥7 years), as appropriate. A sum variable of six maternal risk factors (low socioeconomic status, non-marriage, mental or behavioural disorder, diagnosed substance abuse, criminal record and long-term social assistance) was calculated and categorised as 0–1, 2–3 and 4–6 risks.
Cumulative risk factors and multivariable analysis
To analyse the association between cumulative risk exposure and hospital care for injuries and poisoning (outpatient or inpatient care, S00-T98), a risk score for the PSE group and controls was created by summing all maternal and child-related risk factors (nine risks): maternal low socioeconomic status; non-marriage; mental or behavioural disorder; diagnosed substance abuse; criminal record; long-term social assistance; and youth's sex (male); OHC; and mental or behavioural disorder.
In the final hierarchical multivariable models, both the exposed and control cohorts were included, and all main child and maternal risk factors were added step by step.
Cox regression modelling was used in univariate and multivariable analyses with longitudinal data. The follow-up started from birth and lasted until the first out- or inpatient care episode due to injury or poisoning (S00-T98), death or the end of the follow-up on 31 December 2016. The level of statistical significance was set at p < 0.05. SPSS version 28.0 was used.
Results
Cohort description
About half of the 615 PSE group (49.3%) and 1787 controls (51.7%) were male and 59.5% were aged 18–24 years in 2016 (age range 15–24 years). A majority had Finnish as their native language (PSE 95.9%, controls 86.2%), and 17.9% of the PSE group and 23.4% of the controls had completed secondary education. Mortality was similar in both cohorts (1%). Of those in the PSE group, 7.5% (n = 46) had an FASD continuum diagnosis, and 8.1% (n = 50) had a history of NAS diagnosis during the newborn stage. Daily maternal smoking throughout pregnancy (75.3% vs. 18.9%, p < 0.001) and birth weight <2500 g (12.5% vs. 6.7%, p < 0.001) were more common among the PSE group. No differences between the PSE group and controls were found in gestational age at delivery or 1-min Apgar scores. A majority of the exposed group (63.9%) and a minority of the controls (8.2%, p < 0.001) had at least one OHC episode. Almost all (91.9%) of the PSE group had at least one registered maternal risk factor (controls 27.8%, p < 0.001) (
Prevalence of hospital care due to injuries and poisoning
Half (50.4%) of the PSE group and 40.6% of the controls had been in out- or inpatient hospital care at least once for injury or poisoning (S00-T98) during the follow-up from birth to the end of 2016 (p < 0.001). These numbers consist mainly of outpatient hospital care. Inpatient hospital care was quite rare but somewhat more common among the PSE group (15.9% vs. 11.3%, p = 0.003) (Figure 1). No difference between the PSE group and controls was found regarding the mean number of outpatient and inpatient visits or inpatient treatment days (data not shown).
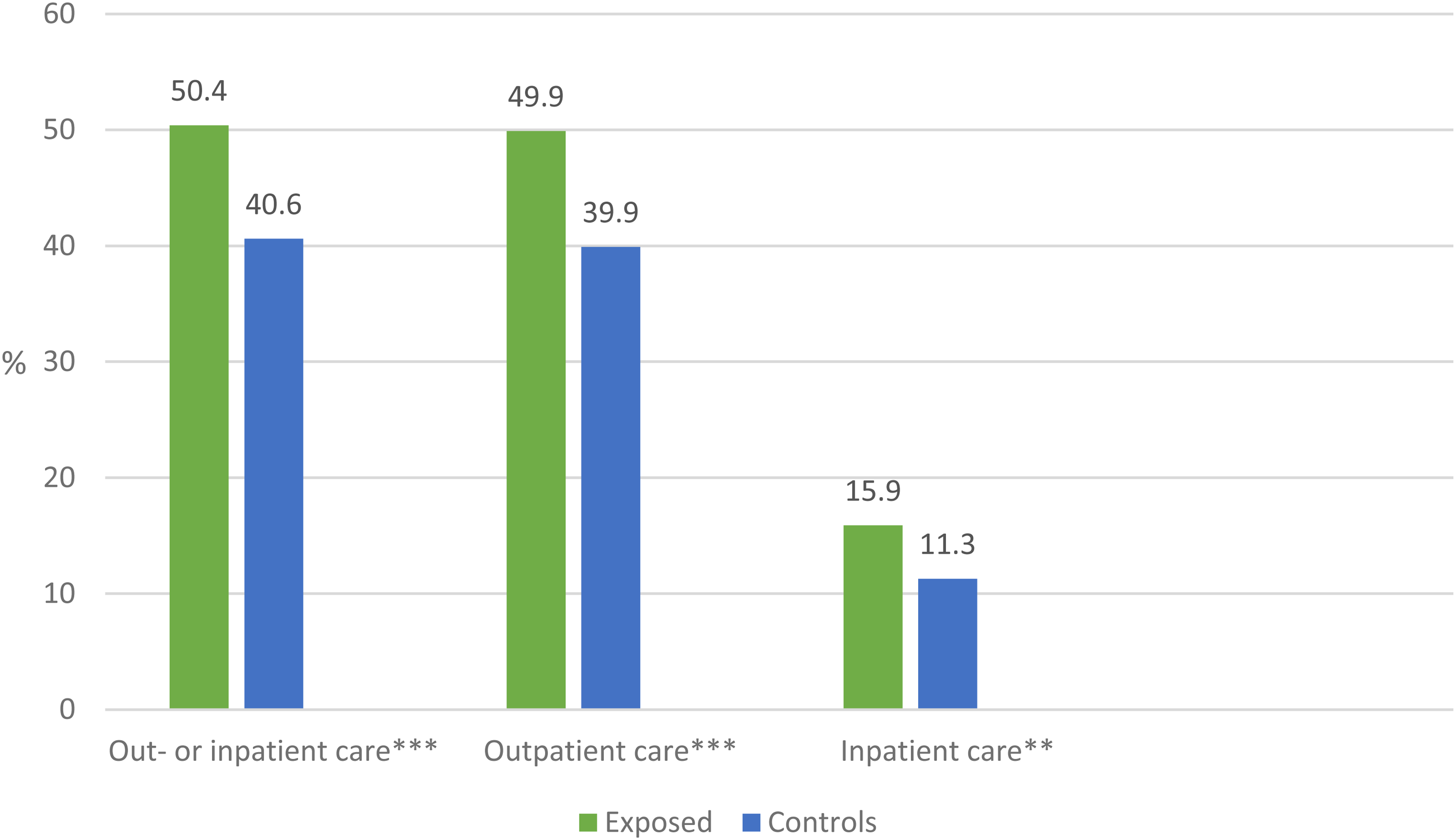
At least one out- or inpatient hospital care episode for injury or poisoning (S00-T98) among the exposed (n = 615) and control youths (n = 1787), (%). **p < 0.01, ***p < 0.001, difference between the exposed and controls.
The median age at first outpatient hospital care episode was 11.4 years (interquartile range [IQR] 4.9–14.6) among the PSE group and 10.9 years (IQR 5.5–14.8) among the controls (p = 0.172). The corresponding numbers for inpatient hospital care were 11.5 years (IQR 3.8–15.1) and 8.6 years (IQR 4.5–13.7, p = 0.268), respectively.
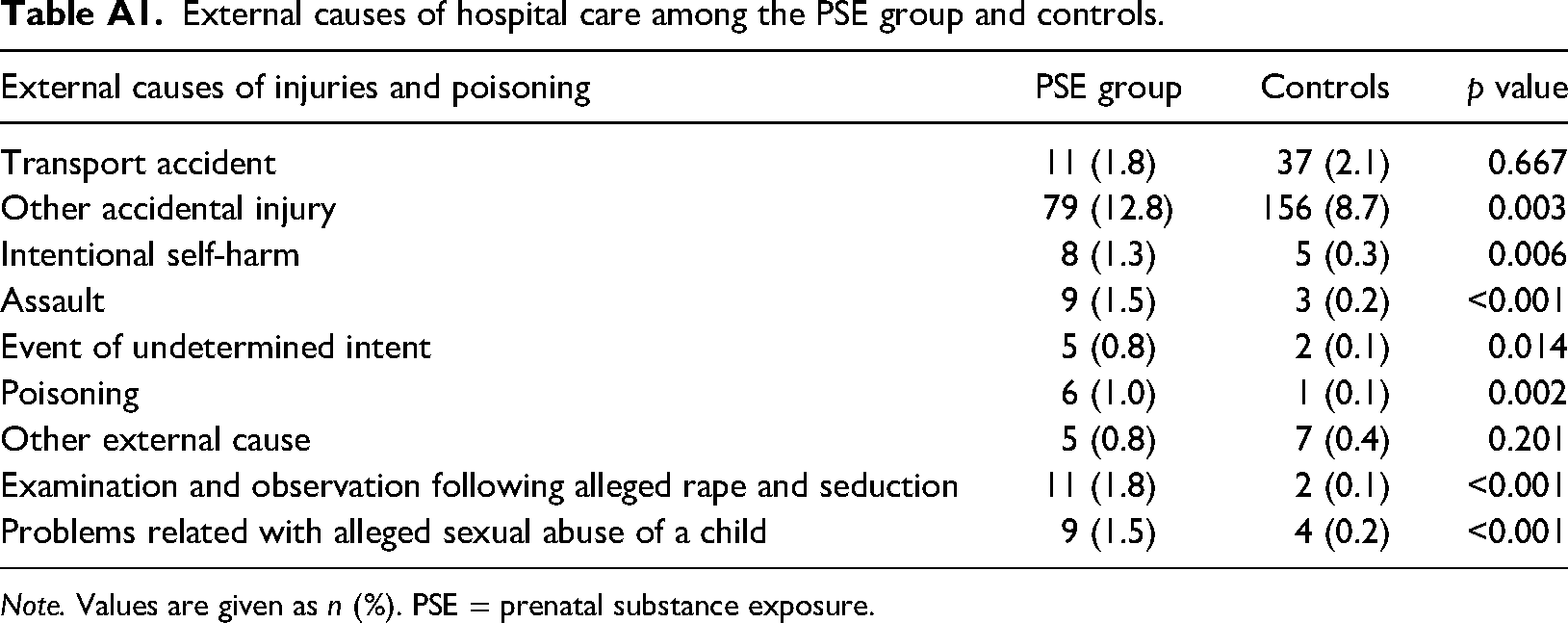
“Other accidental injury” was the most common cause of inpatient hospital care both among the PSE group and controls. No difference was found in transport accidents but all other causes, including alleged sexual abuse, were registered more often for the PSE group (Appendix). The mean age for examination due to alleged rape or seduction was 12.2 years (range 5.6–18.6) among the PSE group and 14.3 years (range 14.3–14.4) among the controls. The mean age for problems due to alleged sexual abuse of a child was 7.1 years (range 3.5–12.8) among the PSE group and 7.8 years (range 3.6–14.3) among the controls.
Bivariate associations between child and maternal risk factors, and injuries or poisoning requiring hospital care
OHC combined with an F90-F98 diagnosis was the strongest risk factor for hospitalisation for injuries and poisoning (S00-T98) among the PSE group (hazard ratio [HR] = 1.65, 95% confidence interval [CI] 1.24–2.19, p < 0.001). The F90-F98 diagnosis category includes hyperkinetic disorders such as ADHD and conduct disorders. OHC was associated with injuries and poisoning regardless of the timing of the first placement, type of OHC or number of placements. Criminal record (HR = 1.52, 95% CI 1.10–2.10, p = 0.010) and long-term social assistance (HR = 1.32, 95% CI 1.02–1.71, p = 0.036) were the strongest maternal risk factors (Table 1).
Bivariate associations between child and maternal risks, and hospital care due to injuries or poisoning (S00-T98) among the PSE (n = 615) and control youths (n = 1787); follow-up from birth to early adulthood, Cox regression hazard model.
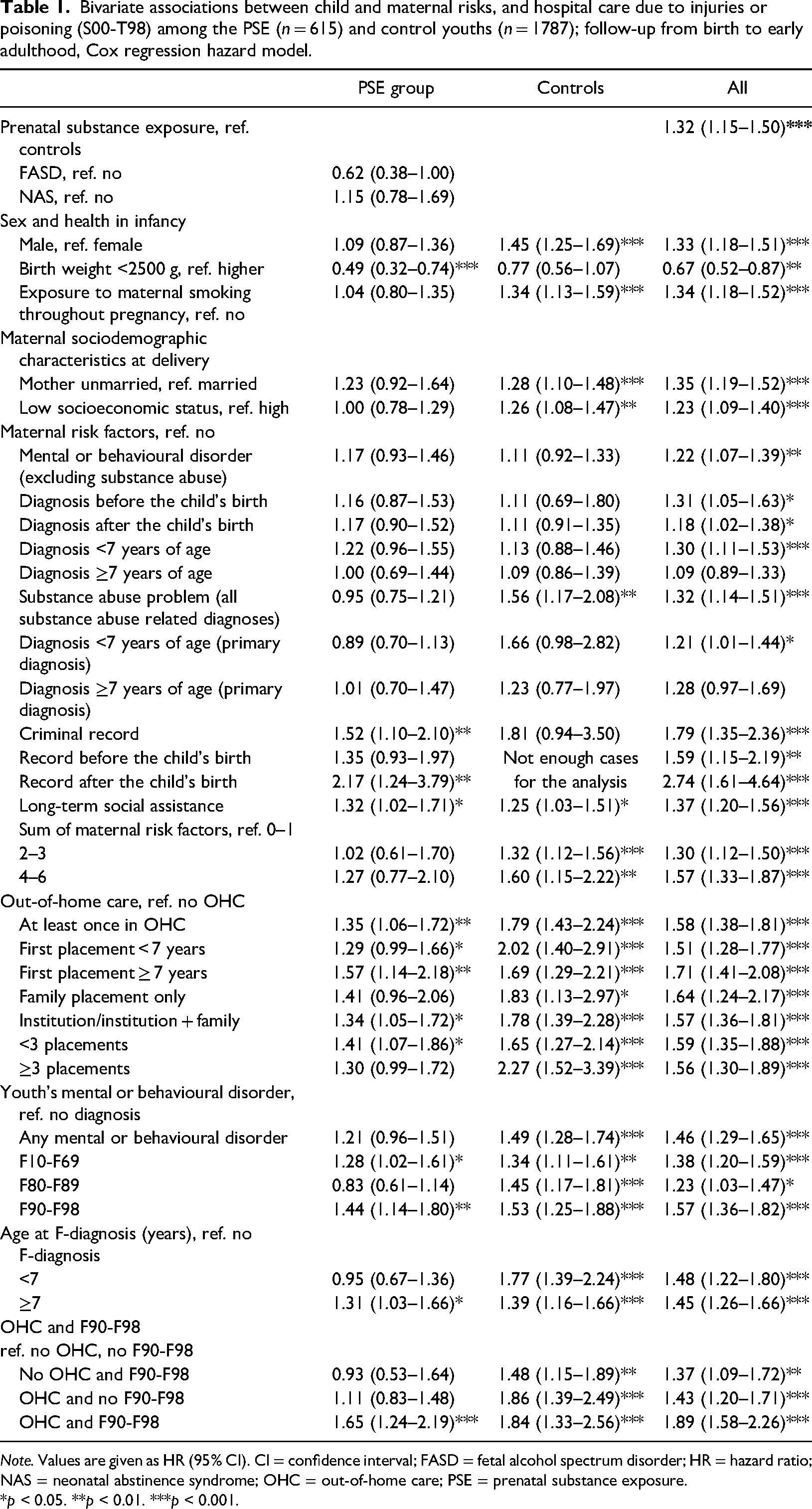
Note. Values are given as HR (95% CI). CI = confidence interval; FASD = fetal alcohol spectrum disorder; HR = hazard ratio; NAS = neonatal abstinence syndrome; OHC = out-of-home care; PSE = prenatal substance exposure.
*p < 0.05. **p < 0.01. ***p < 0.001.
Among the controls, OHC with (HR = 1.84, 95% CI 1.33–2.56, p < 0.001) and without the F90-F98 diagnosis (HR = 1.86, 95% CI 1.39–2.49, p < 0.001) was the strongest risk factor for hospitalisation. In addition, male sex posed a strong risk, as well as several maternal risks, especially maternal substance abuse after delivery (HR = 1.56, 95% CI 1.17–2.08, p = 0.002) (Table 1).
Association between cumulative risk score and hospital care due to injuries or poisoning
The mean and median numbers of risk factors were considerably higher among the PSE group than the controls. The risk score including child and maternal risks had a graded relationship to injuries and poisoning in both groups, but among the PSE group statistical significance was reached only at a very high number of risks (Table 2, Figures 2a and b).
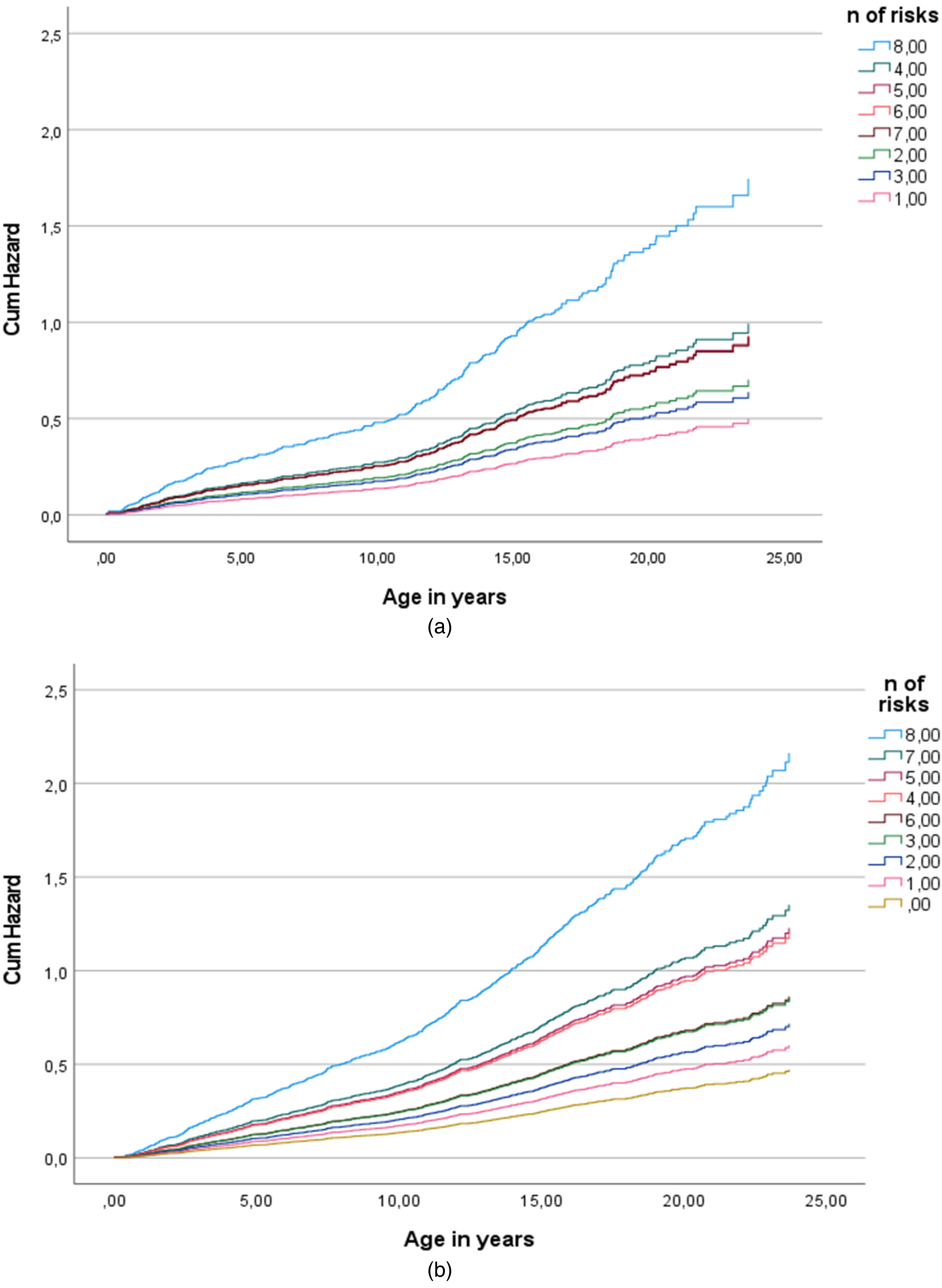
(a) Association between cumulative risk score and hospital care due to injuries or poisoning (S00-T98) among the exposed youths (n = 615), Cox regression hazard model. (b) Association between cumulative risk score and hospital care due to injuries or poisoning (S00-T98) among the control youths (n = 1787), Cox regression hazard model.
Association between cumulative risk score and hospital care for injuries or poisoning (S00-T98) among the PSE (n = 615) and control youths (n = 1787); follow-up from birth to early adulthood, Cox regression hazard model.
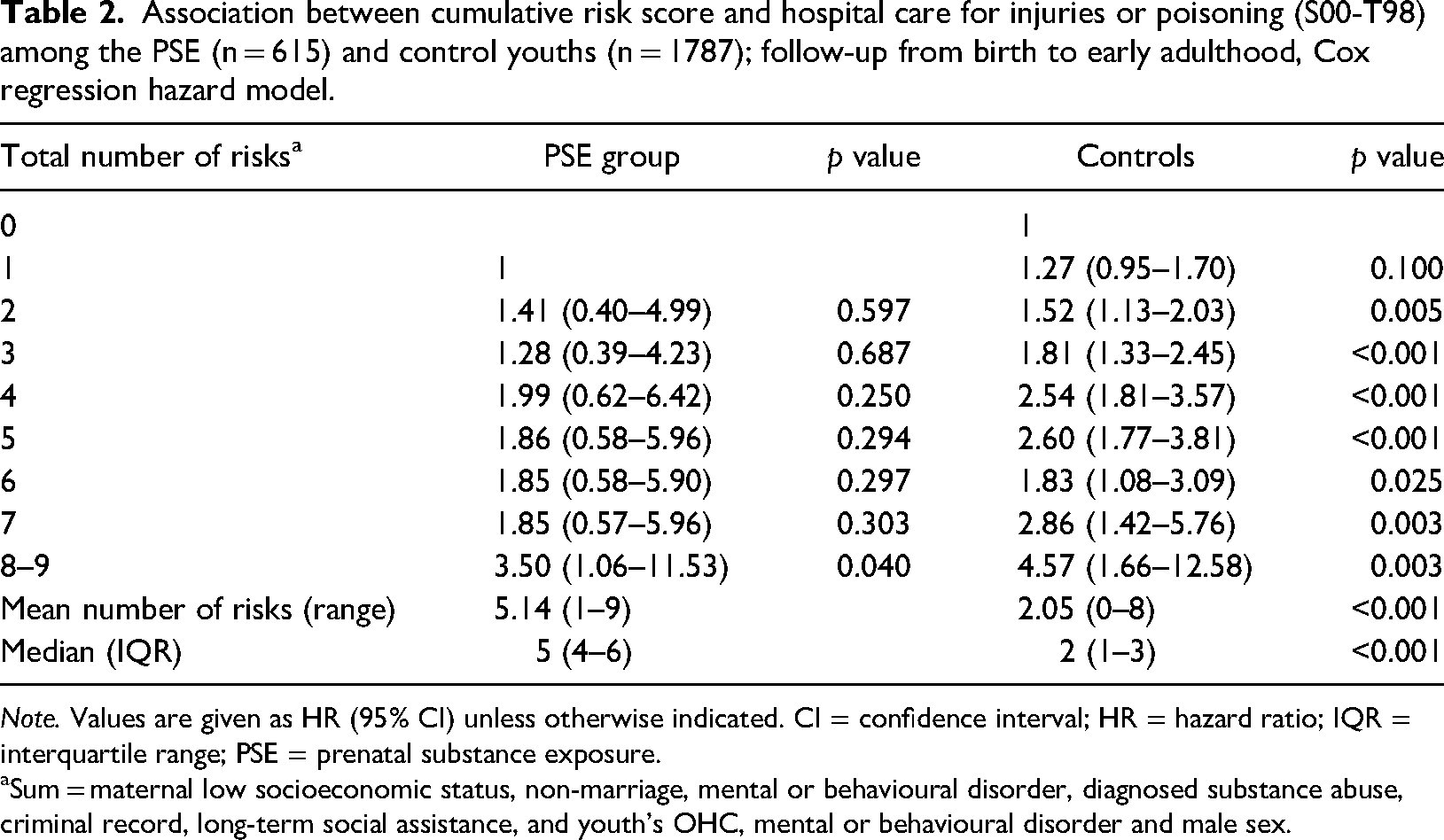
Note. Values are given as HR (95% CI) unless otherwise indicated. CI = confidence interval; HR = hazard ratio; IQR = interquartile range; PSE = prenatal substance exposure.
aSum = maternal low socioeconomic status, non-marriage, mental or behavioural disorder, diagnosed substance abuse, criminal record, long-term social assistance, and youth's OHC, mental or behavioural disorder and male sex.
Multivariable associations between child and maternal risk factors, and hospital care due to injuries and poisoning
Hospital care for injury or poisoning (S00-T98) was more common among the PSE group compared with the controls. However, this difference was attenuated when adjusting for child and maternal risk factors in the models. In the final model, male sex, the cumulative number of maternal risks, OHC and child mental or behavioural disorder were associated with an elevated risk of injuries and poisoning (Table 3).
Multivariable associations between child and maternal risk factors, and hospital care for injuries or poisoning (S00-T98) from birth to early adulthood; Cox regression hazard models, n = 2402; follow-up from birth to early adulthood.
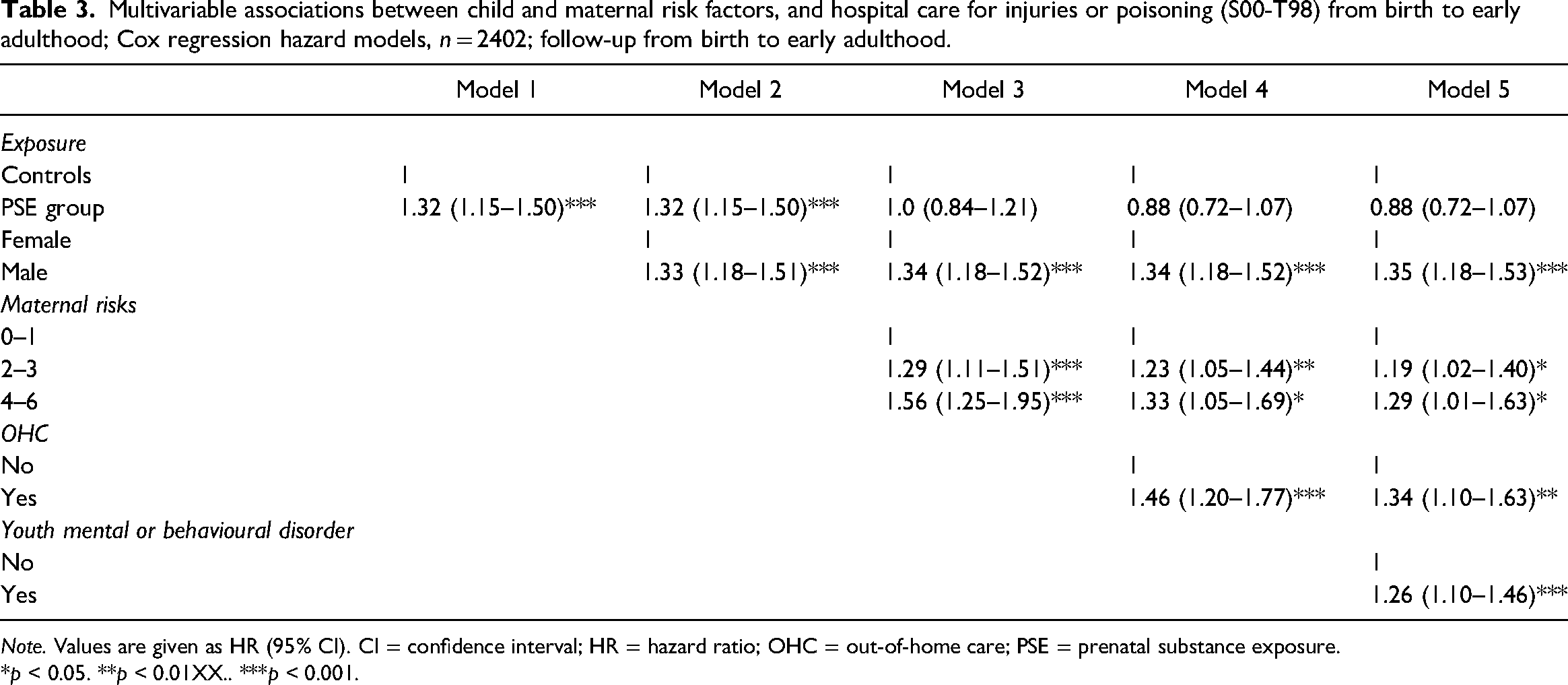
Note. Values are given as HR (95% CI). CI = confidence interval; HR = hazard ratio; OHC = out-of-home care; PSE = prenatal substance exposure.
*p < 0.05. **p < 0.01XX.. ***p < 0.001.
Discussion
This study showed that injuries and poisoning requiring hospital care were more common among the youths with PSE than among the unexposed matched controls. The result is in line with previous studies among small children with a maternal alcohol problem, which showed a high number of hospitalisations due to injuries and poisoning among them (Raitasalo et al., 2015; Raitasalo & Holmila, 2017; Woodside et al., 1993). However, the difference from the controls in the present study was not large, approximately 10 percentage points, and was attenuated after controlling for child and maternal risk factors.
As predicted, the accumulation of child and maternal risk factors was associated with injuries and poisoning among both the PSE group and the controls. Youths with OHC and an F90-F98 diagnosis were at highest risk in both groups. Several studies among normative samples have reported an association between hyperkinetic and conduct problems, included in the F90-F98 category, and an increased risk of injuries in adolescence and young adulthood (Amiri et al., 2017; Brunkhorst-Kanaan et al., 2021; Dalsgaard et al., 2015; Mytton et al., 2009; Rivara, 1995). In addition, OHC has been related with the risk of injuries (Randsalu & Laurell, 2018; Sariaslan et al., 2022). However, this does not mean that OHC causes injuries or poisoning. Both the risk of OHC (
Maternal risk factors were associated with injuries and poisoning among the controls and to a minor extent among the PSE group. The somewhat weaker association among them may be explained at least partly by multicollinearity between PSE and maternal risk factors. Furthermore, the exposed group were placed at younger age, thus decreasing the influence of maternal factors (
The results suggest that PSE may partly explain the higher risk of injuries and poisoning among the exposed youths, but it is not the only predictor. PSE can cause brain abnormalities, and hyperkinetic and other behavioural disorders are common among exposed individuals (Mattson et al., 2019; Riley et al., 2011). According to the definition of ICD-10, hyperkinetic children are prone to risky behaviour. PSE is associated with a complex set of highly interrelated adverse experiences (
Combined evidence from neurobiology and epidemiology shows that recurrent traumatic experiences in childhood have a profound impact on emotional, behavioural, cognitive, social and physical functioning (Anda et al., 2006; Glaser, 2000; Perry et al., 1995). Traumatic experiences cause chronic, overwhelming stress, which without buffering protection provided by supportive adults alters brain architecture and hinders the mind's capacity to function as a well-integrated system (Schore, 2003; Shonkoff et al., 2012; Siegel, 2001). This leads to the inability to regulate affect and behaviour (Schore, 2001) increasing the risk of accidents and injuries. With early and efficient support to families with substance abuse problems, injury risk among their children could be reduced.
Strengths and limitations
Empirical evidence of the prevalence of injuries and poisoning among youth with PSE has been lacking, even though it is estimated that PSE increases the likelihood of engaging in high-risk behaviour (Wyper & Pei, 2016). Previous studies have addressed mainly infants with PSE, preschoolers without verified PSE or normative samples, and have studied the effect of single risk factors. The present longitudinal study enabled comparison between youths with PSE and matched unexposed controls and the assessment of several associated risk factors by using a unique combination of medical records and register data with a large sample size. Free access to publicly funded healthcare, diagnoses made by medical professionals and mandatory registration in national databases ensured the high completeness and validity of the data (Aro et al., 1990; Gissler & Haukka, 2004; Sund, 2012).
Despite the strengths, the study has several limitations. First, we are only able to show associations between the risk factors and hospital-treated injuries and poisoning. No causal relationships can be assured. For example, Rowe et al. (2004) state that mental and behavioural disorders can put children and youth at an increased risk for injuries. Alternatively, injury can contribute to the risk of psychopathology. Second, despite us checking health and social welfare registers carefully for any sign of maternal substance abuse during pregnancy and 1 year before, we cannot rule out unrecognised substance use among the control mothers. This problem is present in all studies on substance use during pregnancy (Behnke et al., 2013).
Conclusion
This study provides novel information about the prevalence of injuries and poisoning among youths with PSE in comparison with matched unexposed controls. In addition, the study provides important evidence of the interrelated risk factors that are associated with injuries and poisoning in both groups and shows that PSE is not the only risk factor. Injuries and poisoning are leading causes of morbidity and mortality in the under-25 age group in the general population. Early and long-term support for disadvantaged families and children is vital to promote child and adolescent health.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Samfundet Folkhälsan i svenska Finland rf., Juho Vainio Foundation, Signe and Ane Gyllenberg Foundation, Medicinska Understödsföreningen Liv och Hälsa rf.
Availability of data and material
Appendix
External causes of hospital care among the PSE group and controls.
| External causes of injuries and poisoning | PSE group | Controls | p value |
|---|---|---|---|
| Transport accident | 11 (1.8) | 37 (2.1) | 0.667 |
| Other accidental injury | 79 (12.8) | 156 (8.7) | 0.003 |
| Intentional self-harm | 8 (1.3) | 5 (0.3) | 0.006 |
| Assault | 9 (1.5) | 3 (0.2) | <0.001 |
| Event of undetermined intent | 5 (0.8) | 2 (0.1) | 0.014 |
| Poisoning | 6 (1.0) | 1 (0.1) | 0.002 |
| Other external cause | 5 (0.8) | 7 (0.4) | 0.201 |
| Examination and observation following alleged rape and seduction | 11 (1.8) | 2 (0.1) | <0.001 |
| Problems related with alleged sexual abuse of a child | 9 (1.5) | 4 (0.2) | <0.001 |
Note. Values are given as n (%). PSE = prenatal substance exposure.