
Abstract
Aims:
High alcohol consumption and use of illicit drugs among young people is of great concern and there is a need to identify arenas where this group can be reached by preventive measures. The aim of the present study was to study prevalence of risky alcohol consumption, illicit drug use, and risky sexual behaviour (RSB) among young people visiting youth health clinics in Stockholm county. Another aim was to explore the association between risky alcohol consumption, illicit drug use and RSB.
Methods:
During autumn 2016, an anonymous questionnaire comprising questions about alcohol, illicit drugs and risky sexual behaviour was given to visitors at 11 youth health clinics in Stockholm county.
Results:
A total of 328 youths (M = 18.8 years, 89% girls) answered the questionnaire. Results show that 61.7% had risky alcohol consumption and 41.8% had tried illicit drugs. Risky sexual behaviour was more prevalent among respondents with risky alcohol consumption, and it was more common among non-students than students.
Conclusions:
Findings indicate that a large proportion of visitors at youth health clinics in Stockholm county has a risky alcohol consumption and experiences of other drugs, and also that risky alcohol consumption is associated with three of five RSB outcomes. Non-students seemed to be a particularly exposed risk group with regard to both risky alcohol consumption and RSB. Overall, the results indicate that youth health clinics are an important arena for alcohol prevention.
Young people are generally more likely to engage in risk behaviours than individuals of other ages (Chick & Reyna, 2012). Risk behaviour may manifest as use of alcohol and illicit drugs, and risky sexual behaviour (RSB). Consumption of alcohol is not evenly distributed across different groups in the population. For example, men drink more alcohol than women and young people drink more alcohol than older people. However, during recent years population studies show that the gender gap in alcohol consumption has decreased, especially with regard to young people (CAN, 2019; European Monitoring Centre for Drugs and Drug Addiction, 2016). Despite a decreased alcohol consumption in younger age groups in Sweden in recent years (CAN, 2019; Folkhälsomyndigheten, 2018), the largest proportion of risk consumers is still found among young adults (Guttormsson & Gröndahl, 2018). Studies of young adults show that high alcohol consumption is common and often characterised by binge drinking (Andersson, Wirehn, Olvander, Ekman, & Bendtsen, 2009; Hingson, Zha, & Smyth, 2017; Knight et al., 2002; White, Kraus, & Swartzwelder, 2006). International research shows that approximately 23% of university students indulged in frequent binge drinking (i.e., consuming five or more “drinks” of alcohol on one occasion) (Wechsler, Lee, Kuo, & Lee, 2000) and a more recent study indicates that the proportion may be even higher (37.4%) (Hingson et al., 2017). In Sweden, surveys suggest that 44% of men and 27% of women, aged between 16 and 29 years, had engaged in binge drinking during the last 30 days (Ramstedt, Lindell, & Raninen, 2013). Also, a Swedish study among university students showed that 45% exceeded the cut-off for risky alcohol consumption in Audit-C (Folkhälsomyndigheten, 2014). Recent research suggests that there is no clear lower threshold for when alcohol consumption is not associated with a risk of disease (Wood et al., 2018), which supports the argument for working to limit alcohol consumption, especially among young people.
Although the use of substances may facilitate sexual contact (Bellis & Hughes, 2004; Foxman, Aral, & Holmes, 2006; Sumnall, Beynon, Conchie, Riley, & Cole, 2007), substance use in younger ages is associated with a variety of adverse consequences. In the short term, these are often a result of acute intoxication, while in the long term, negative psychosocial outcomes and addiction can emerge (Bonomo et al., 2001; Dawson, Goldstein, Chou, Ruan, & Grant, 2008; Gates, Sabioni, Copeland, Le Foll, & Gowing, 2016; Guttmannova et al., 2012; Miller, Naimi, Brewer, & Jones, 2007; Nilses, Blom, Heimer, & Danielsson, 2011). Furthermore, alcohol and illicit drug use are associated with RSB, defined in previous research as, for example, multiple partners, casual unprotected sexual activity and an early sexual debut (Berhan & Berhan, 2015; Noar, Cole, & Carlyle, 2006; Rehm, Shield, Joharchi, & Shuper, 2012). Risky sexual behaviour can lead to several health problems, such as sexually transmitted infections, including HIV, and unintended pregnancies (Johnson, Barrett, Horricks, Akintan, & Van Blyderveen, 2014), which in turn may lead to stress and related health problems (Hall, Kusunoki, Gatny, & Barber, 2015). The Public Health Agency of Sweden has conducted a survey investigating sexual health among 7865 young people aged 16–29 years. Results showed that 81% of young people reported being sexually active, and the average age for the sex debut was 16 years. The average number of sexual partners during the last year was two. Respondents reported having had unprotected sex with an average of one partner during the last year. Almost half (48%) of young women and 39% of young men reported having had unprotected sex during the last year. In the survey 19% reported having used alcohol the last time they engaged in sex (Folkhälsomyndigheten, 2017). Young people who drink heavily or use cannabis are more likely to expose themselves to RSB (Brodbeck, Matter, & Moggi, 2006b; Brookmeyer & Henrich, 2009; Patrick, O’Malley, Johnston, Terry-McElrath, & Schulenberg, 2012; Rehm et al., 2012) and studies show that college students are more likely to be sexually active and less likely to use condoms on days when they drink alcohol (Kiene, Barta, Tennen, & Armeli, 2009; Patrick & Maggs, 2009). Experimental studies have shown that high blood alcohol levels increase the risk of unprotected sexual activity (Rehm et al., 2012). As in previous studies, alcohol consumption was associated with a higher risk of unplanned pregnancy (Reardon, Coleman, & Cougle, 2004) and sexually transmitted infections (Cook, Pollock, Rao, & Clark, 2002; Tapert, Aarons, Sedlar, & Brown, 2001). Longitudinal research also indicates that alcohol consumption in adolescence increases the risk of later RSB (Muchimba, Haberstick, Corley, & McQueen, 2013).
In Sweden, there are about 230 youth health clinics, of which 34 are located in Stockholm county. The clinics are outpatient healthcare units and are annually visited by about 200,000 adolescents and young adults. Youth health clinics in this form, as far as we know, only exist in Sweden. There is no exact equivalent in the other Nordic countries (Nordic Council, 2019). At the clinics, about 85% of the visitors are girls or young women (Wiksten-Almströmer, 2006). The clinics are open during office hours, and sometimes during evenings or weekends, and also offer weekly drop-in occasions. The clinics most often target youths between 12 and 23 years of age and the main function is to offer advice on contraceptives and strategies to prevent sexually transmitted infections (STIs). However, many conversations during visits to the clinics also address stress, anxiety, identity and sexuality in adolescents and young adults in a broader perspective (Leijen, Rasmussen, & Wendt, 2013). Several professions are represented at the youth health clinics, primarily midwives, social counsellors and/or psychologists, and physicians (Föreningen för Sveriges ungdomsmottagningar, 2018). A recent Swedish study among professionals at youth health clinics in Stockholm indicated that, in addition to performing preventive efforts targeting RBS and STIs and promoting strategies for safe sexual behaviour, midwives and counsellors often address mental health problems, excessive alcohol consumption and illicit drug use in their conversations with young people who visit the clinics (Kvillemo, Skoglund, Gripenberg, & Strandberg, 2018). Furthermore, a previous survey among young people visiting youth health clinics indicated that both alcohol and illicit drug use were more prevalent in this group than among same-aged peers. The survey indicated that 75% scored above the cut-off values for risky alcohol consumption in Audit-C (Karolinska Institutets folkhälsoakademi, 2010).
Alcohol and illicit drug prevention is implemented at several levels in Swedish society: local, regional, and national. The research group Stockholm Prevents Alcohol and Drug Problems (STAD) develops, implements, and evaluates promising alcohol and illicit drug preventive interventions in a range of settings, for instance recreational venues (Gripenberg Abdon, Wallin, & Andréasson, 2011; Wallin, Gripenberg, & Andreasson, 2002), sports arenas (Durbeej, Elgan, Jalling, & Gripenberg, 2017), and primary healthcare (Wåhlin & Andreasson, 2015). STAD works continuously to identify new arenas for preventive interventions with the aim of reaching risk groups. Altogether, youth health clinics seem to be a suitable arena for reaching young people, especially given that this group is difficult to reach with preventive efforts (Ramstedt et al., 2013). However, this is a relatively unexplored field and studies are largely lacking on the preventive work carried out at these clinics (Leijen, Rasmussen, & Wendt, 2013).
Against this background, the aim of the present study was twofold. Firstly, we wanted to assess the prevalence of risky alcohol consumption, and other risk behaviours such as illicit drug use and RSB, among young people visiting youth health clinics in Stockholm county. In the present study the test group was defined as young people in the age range 15–23 years. The reason is that 15 years is the age at which one can decide on one’s own participation in research and that 23 years is often the upper age limit for which the clinics apply. We wanted to study whether RSB was more common (1) among youths with risky alcohol consumption, and (2) among youths who had tried other drugs, and whether there were differences related to gender or educational status. Second, we aimed to explore the association between risky alcohol consumption, illicit drug use and RSB, while also controlling for other factors in the sample.
Method
Participants and procedures
In early 2016, 27 out of 34 youth health clinics in Stockholm county were contacted by email and invited to participate in the study. Seven clinics were not contacted due to geographical distance. After a first meeting at the contacted clinics, during which STAD informed staff about the study, 11 youth health clinics decided to participate and agreed to ask their visitors to be enrolled in the study. During two weeks in September/October 2016 questionnaire data were collected from clinic visitors. The data collection was conducted either by staff from STAD during drop-in occasions (at seven of the clinics) or by the clinic staff (at four of the clinics). Thirty questionnaires were sent to each clinic who chose to administer the questionnaire themselves. When the questionnaires were answered staff from STAD personally collected them. At the clinics where staff from STAD administered the questionnaires the data collection took place at drop-in occasions, two hours at each drop-in and at two occasions per clinic. The intention was to ask every visitor until enough data had been collected. Based on a priori assumptions and the knowledge that we could not burden the clinics with the collection of too many questionnaires, we agreed that 30 questionnaires per clinic would suffice. Individuals eligible for enrolment (i.e., over 15 years of age) initially received verbal information about the study; if they agreed to participate, they were given additional written information. The information included the aim of the study, that participation was voluntary and anonymous, and that they could stop participating at any time. Participants were also informed about how to contact researchers if they had questions about the study and where to turn if participation raised concerns. Based on information from clinic staff and summaries from the drop-in data collections we estimate that less than 10% of the youths visiting the clinics during the data collection period (either during the chosen drop-in occasions or on days when the staff at the clinic handled data collection) did not participate. Reasons for not participating were either that the youth chose not to or did not have time, or that the research team did not have time to ask.
Measures
The questionnaire used in the present study was developed by STAD during spring 2016. It was pilot tested by two people at one of the participating youth health clinics. The questionnaire was adjusted based on both the pilot test and discussions within the research team at STAD. The questionnaire took about 15 minutes to fill out and included questions about age, gender, and current occupation (studying, working, etc.). Respondents were also asked about their age of sexual debut and age of alcohol and illicit drug use debut.
Risky alcohol consumption was measured with Audit-C, which comprises three questions about frequency and amount of alcohol consumption (Bergman & Källmen, 2002). Respondents were asked (1) “How often do you drink alcohol?” with response options ranging from 0 (never) to 4 (four times a week or more often), (2) “How many ‘glasses’ of alcohol do you drink on a typical drinking occasion?” with response options ranging from 0 (1–2) to 4 (10 or more), and (3) “How often do you drink six or more such ‘glasses’ on the same occasion?” with response options ranging from 0 (never) to 4 (daily or almost daily). The maximum total score for Audit-C is 12 and is calculated by summing up the scores for all items. The cut-off scores for risky alcohol consumption used in the present study were 4 for girls and 5 for boys (Reinert & Allen, 2007; Socialdepartementet, 2013). Cronbach’s alpha for Audit-C in this sample was 0.7.
Sex under the influence of alcohol or other drugs. Youths were asked “Have you ever had sex under the influence of alcohol?” (yes/no), “How often are you under the influence of alcohol when you have sex?” with response options 0 (never), 1 (rarely), 2 (sometimes), 3 (often), and 4 (always). Respondents were also asked if they had ever had sex under the influence of a drug other than alcohol (yes/no).
Risky sexual behaviour was measured with two items: “How often do you use a condom (or other protection) when you have sex with a new or casual partner?”, with response options 0 (never), 1 (rarely), 2 (usually) and 3 (always), and “Have you ever had a sexually transmitted infection?” with response options yes/no/don’t know.
Risky sexual behaviour under the influence of alcohol was measured with two items. Respondents were asked whether they had ever, under the influence of alcohol, “Forgotten to use a condom (or other protection)?”, or “Abstained from using a condom (or other protection)?” with response options yes/no/can’t answer/don’t want to answer.
Three demographic variables were used in the analyses: age, gender (0 = girl, 1 = boy) and educational status (0 = student, 1 = non-student).
Statistical analyses
Descriptive statistics show the prevalence (numbers and percentages) of different risk behaviours, and values with standard deviations for debut age. The chi-squared test was used to explore whether risk behaviours were more prevalent among risk consumers of alcohol. Multivariate logistic regressions were run to explore the association between risky alcohol consumption/other variables and RSB within the present sample. The purpose of using the regression models was to investigate the influence of the various factors simultaneously and also to explore possible interaction effects. The binary outcome variables were modelled as logistic regressions of the binary predictor variables. All analyses were run using SPSS 23.
Ethics
All procedures were performed in accordance with the ethical standards of the institutional and/or national research committees, the 1964 Helsinki Declaration and its later amendments, or comparable ethical standards. Informed consent was obtained from all the participants included in the study. The study was approved by the Ethics Committee of the Karolinska Institute (No. 2016/818–31/5).
Result
The questionnaire was filled out by 328 individuals aged 15–27 years (mean = 18.8 years), of whom 290 (89.0%) were girls, 33 (10.1%) were boys, and three (0.9%) had another gender identity. The majority of the respondents were heterosexual (86.4%), lived with their parents (75.6%), had no children (99.1%), and were students (64.3%). Among those who did not study, about a third were working (31.4%), and 3% were unemployed. The sample is described in regard to the studied behaviours in Table 1.
About the sample (n = 328).
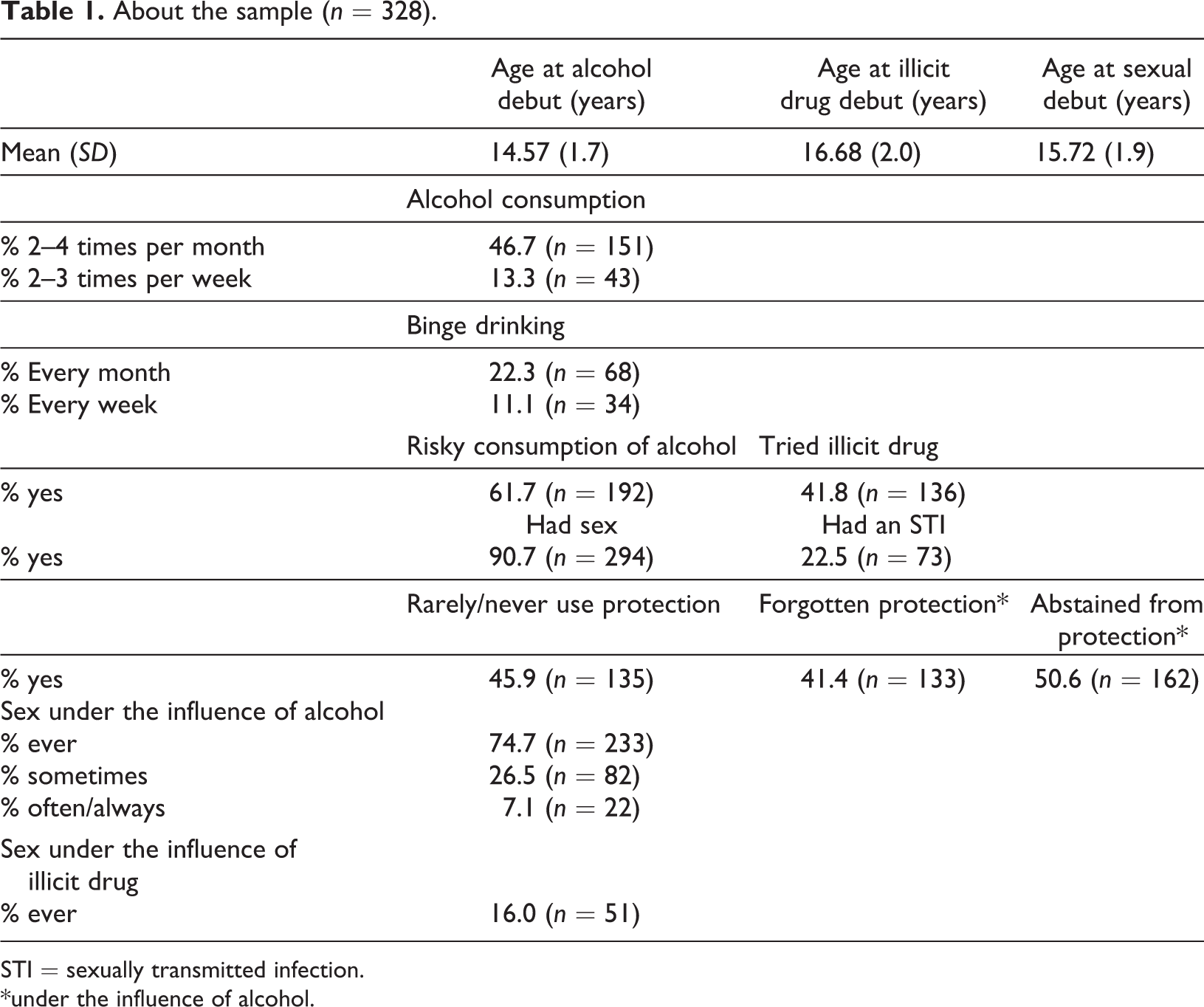
STI = sexually transmitted infection.
*under the influence of alcohol.
Prevalence of risk behaviours among respondents with risky alcohol consumption
According to cut-off scores for Audit-C (4 for girls and 5 for boys) (Berman, Wennberg, & Källmen, 2012; Reinert & Allen, 2007; Rumpf, Wohlert, Freyer-Adam, Grothues, & Bischof, 2013), 61.7% (n = 192) of the total sample reported risky alcohol consumption. The proportion of respondents having had sex under the influence of alcohol was significantly higher among those reporting a risky alcohol consumption than among those below the Audit-C cut-off score (90.3% vs. 49.6%, chi2 = 62.119, p < .001). Moreover, respondents with a risky alcohol consumption had, to a greater extent, had sex under the influence of other drugs (20.9% vs. 6.8%, chi2 = 10.997, p < .01). A significantly higher proportion of respondents with a risky alcohol consumption had also forgotten to use or abstained from using protection when having sex under the influence of alcohol, had had an STI and reported that they rarely or never used protection when having sex with a new or casual partner. As regards having had unprotected sex in the last 12 months and early sexual debut (< 15 years), there were no statistically significant differences between risk consumers and non-risk consumers of alcohol (p = .218 and p = .067, respectively) (see Table 2).
Risky sexual behaviour, comparisons between risk consumers and non-risk consumers of alcohol according to Audit-C, % (n).
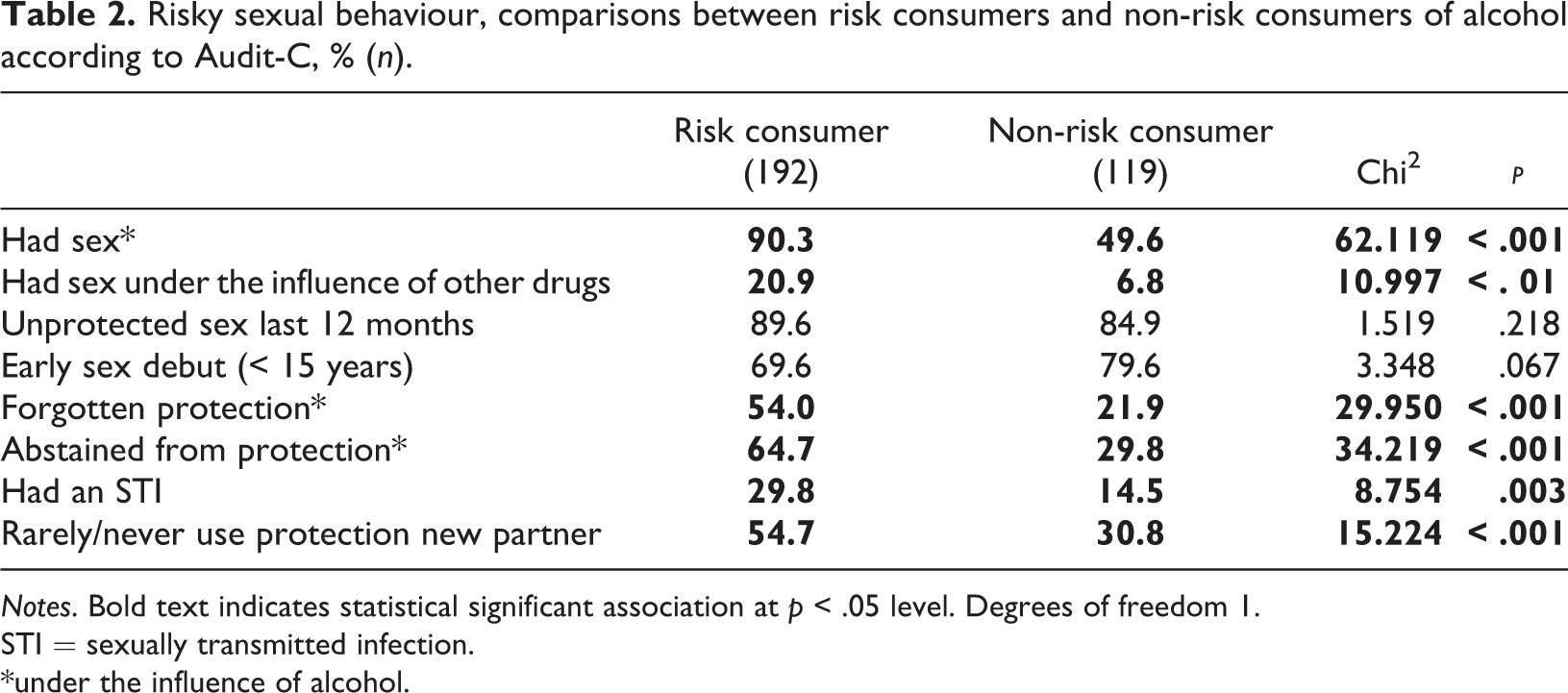
Notes. Bold text indicates statistical significant association at p < .05 level. Degrees of freedom 1.
STI = sexually transmitted infection.
*under the influence of alcohol.
Prevalence of risk behaviours among respondents who had tried other drugs
More than 40% (41.8%, n = 136) of the total sample reported having ever tried a drug other than alcohol. A significantly higher proportion of respondents who had tried another drug had also forgotten to use or abstained from using protection when having sex under the influence of alcohol, reported having had an STI, an early sexual debut, and that they rarely or never used protection when having sex with a new or casual partner. There were no statistically significant differences for having had unprotected sex in the last 12 months (p = .135) (see Table 3).
Risky sexual behaviour, comparisons between respondents who have tried other drugs and who have not tried other drugs, % (n).
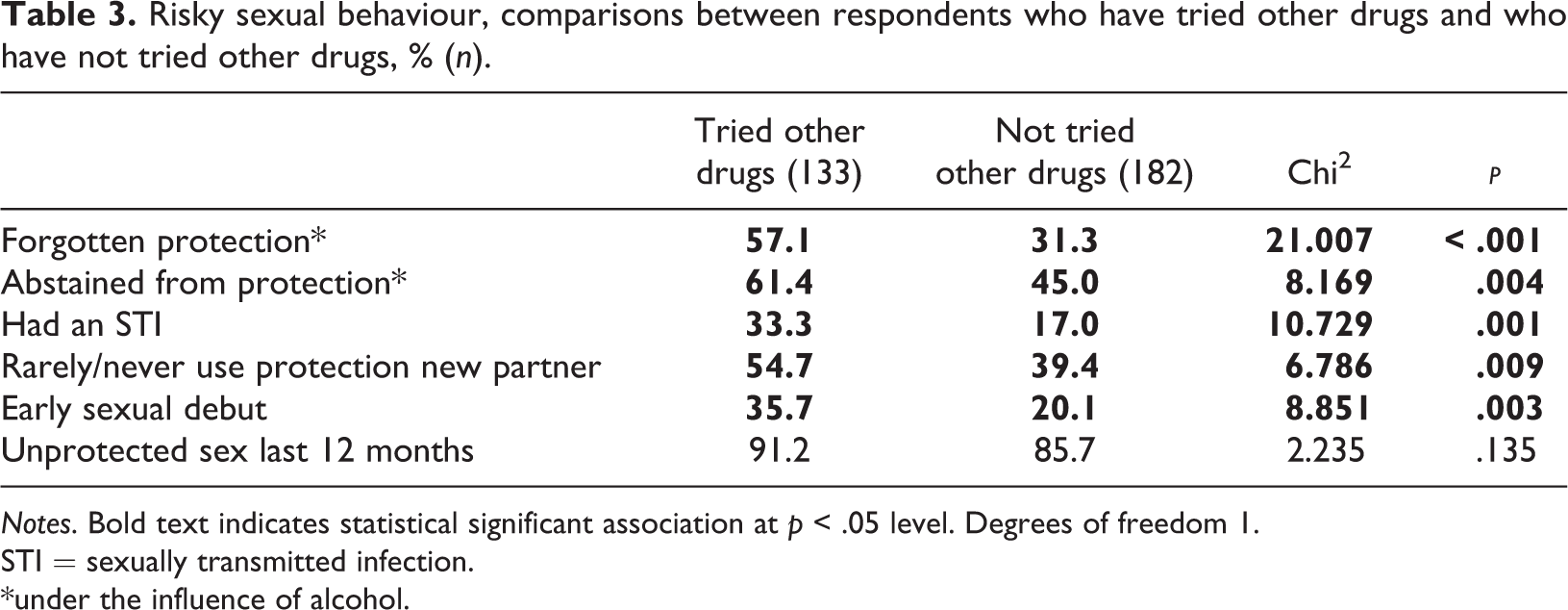
Notes. Bold text indicates statistical significant association at p < .05 level. Degrees of freedom 1.
STI = sexually transmitted infection.
*under the influence of alcohol.
Students vs. non-students
The proportion of respondents who reported risky alcohol consumption was significantly higher among non-students (a majority of whom reported they were working) than among respondents who were currently in school (high school or university) (74.5% vs. 55.0%, chi2 = 10.623, p < .01). A significantly higher proportion among non-students had also forgotten to use or abstained from using protection when having sex, had had an STI and reported that they rarely or never used protection when having sex with a new or casual partner. There were no statistically significant differences between non-students and students for having had unprotected sex in the last 12 months or for early sexual debut (p = .202 and p = .745, respectively) (see Table 4). Also, analyses showed that the mean age was significantly higher among non-students compared to students (20.24 [SD 1.58] vs. 18.01 [SD 1.95] years, p < .001).
Risky sexual behaviour, comparisons between students and non-students, % (n).
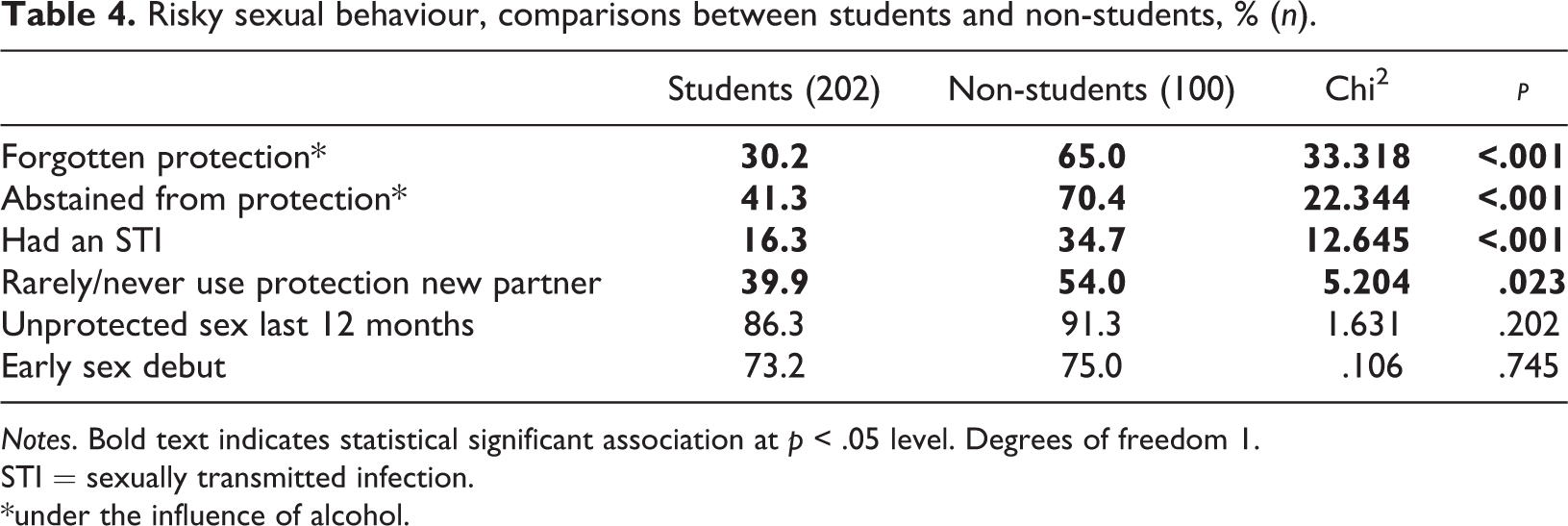
Notes. Bold text indicates statistical significant association at p < .05 level. Degrees of freedom 1.
STI = sexually transmitted infection.
*under the influence of alcohol.
Gender differences
We found no statistically significant differences in the proportion of girls and boys who engaged in risky alcohol consumption (p = .117), nor in the proportion of girls and boys who reported that they had tried a drug other than alcohol (p = .318). There were no statistically significant gender differences for any of the RSB variables. It should be noted that the number of participating boys was very low.
Factors associated with RSB
Results from the multivariate logistic regression are displayed in Tables 5–9. The adjusted models were also run with the inclusion of potential interaction variables (educational status × risk consumption and educational status × age), but since none of the interaction variables was significantly associated with any of the RSB outcomes, this was omitted from the final analyses.
Crude and adjusted ORs with 95% CIs for having forgotten protection when having sex under the influence of alcohol.
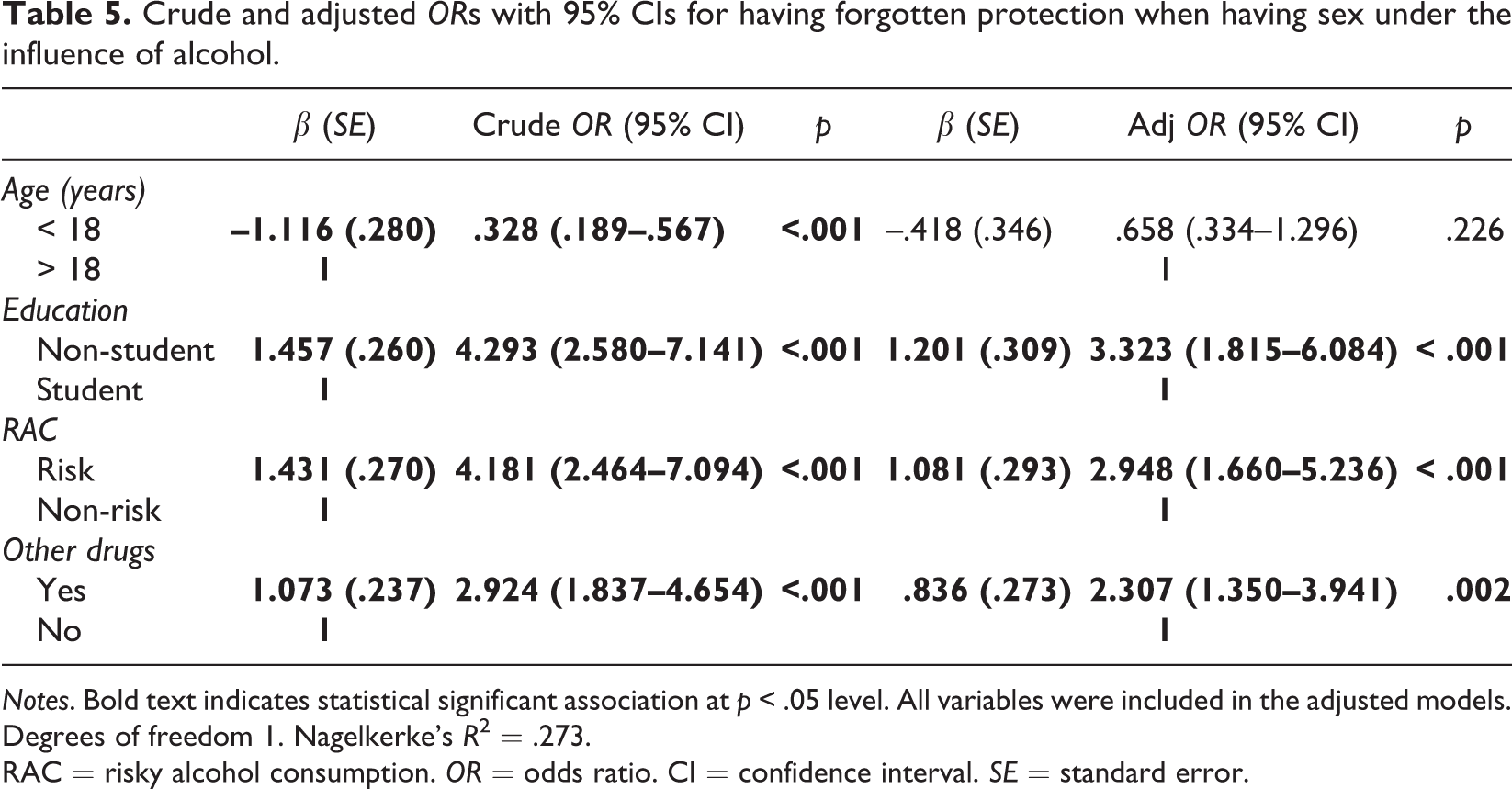
Notes. Bold text indicates statistical significant association at p < .05 level. All variables were included in the adjusted models. Degrees of freedom 1. Nagelkerke’s R2 = .273.
RAC = risky alcohol consumption. OR = odds ratio. CI = confidence interval. SE = standard error.
Crude and adjusted ORs with 95% CIs for having abstained from using protection when having sex under the influence of alcohol.
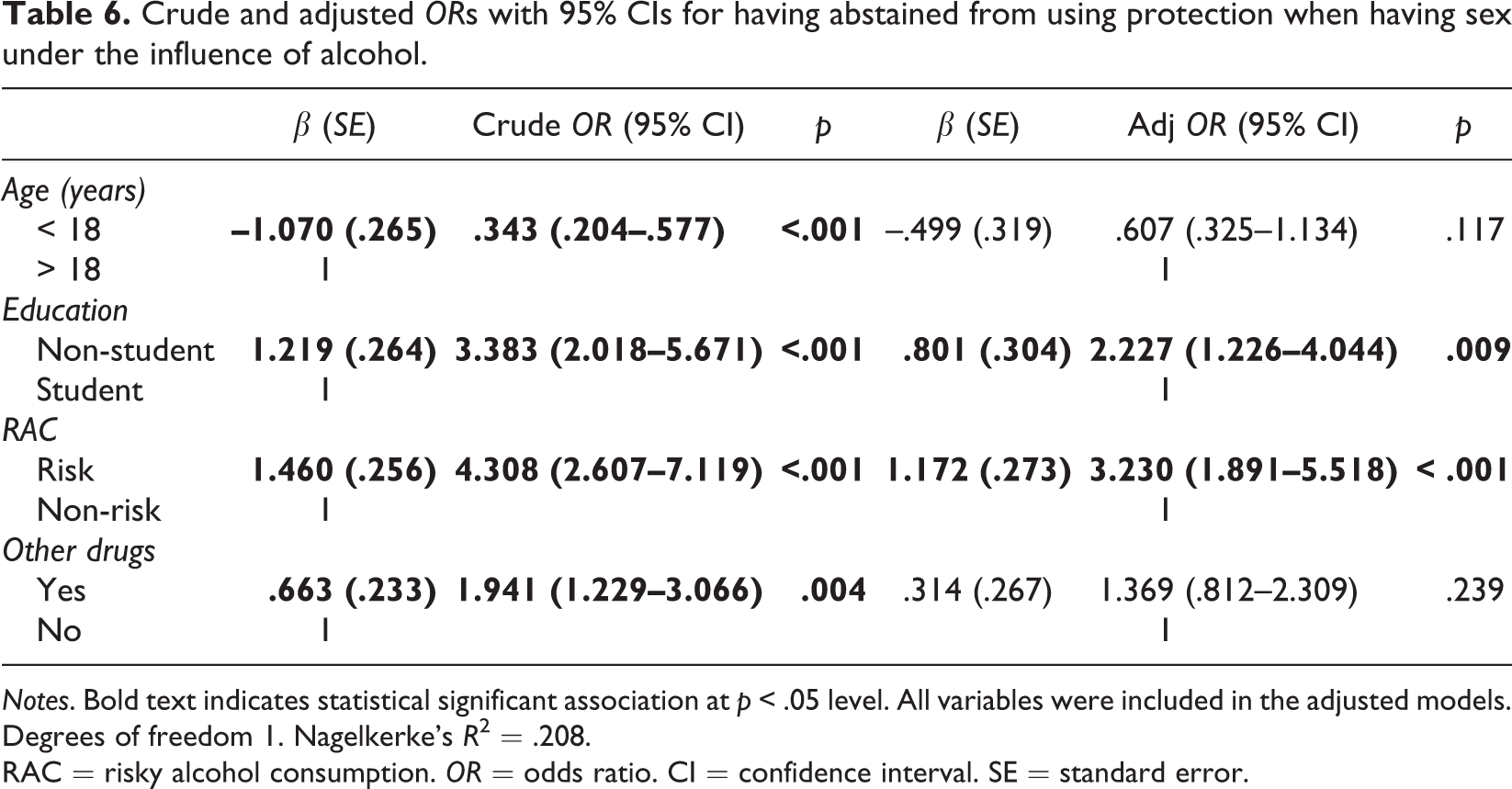
Notes. Bold text indicates statistical significant association at p < .05 level. All variables were included in the adjusted models. Degrees of freedom 1. Nagelkerke’s R2 = .208.
RAC = risky alcohol consumption. OR = odds ratio. CI = confidence interval. SE = standard error.
Crude and adjusted ORs with 95% CIs for having had an STI.
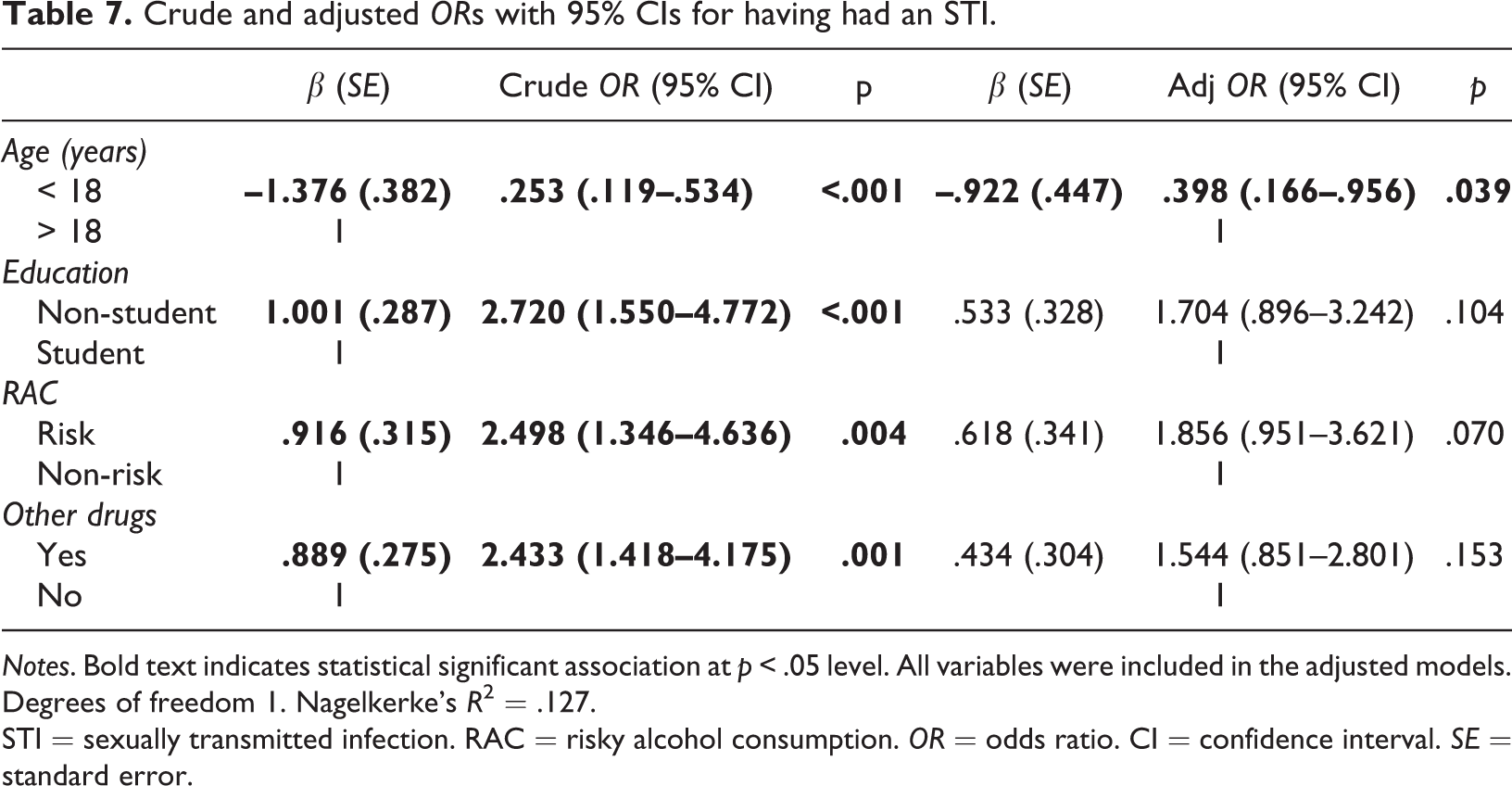
Notes. Bold text indicates statistical significant association at p < .05 level. All variables were included in the adjusted models. Degrees of freedom 1. Nagelkerke’s R2 = .127.
STI = sexually transmitted infection. RAC = risky alcohol consumption. OR = odds ratio. CI = confidence interval. SE = standard error.
Crude and adjusted ORs with 95% CIs for rarely or never using protection when having sex with a new or casual partner.
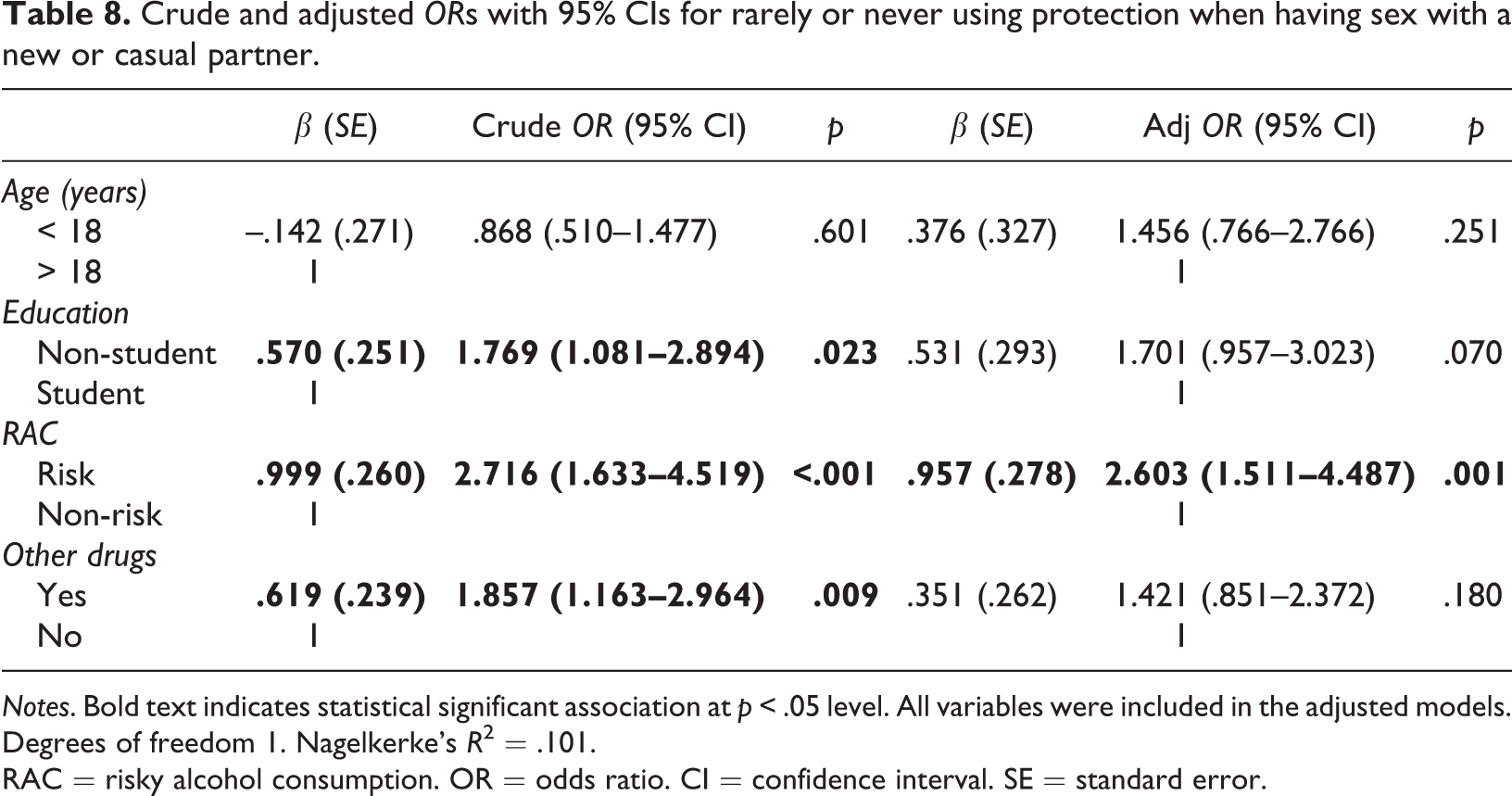
Notes. Bold text indicates statistical significant association at p < .05 level. All variables were included in the adjusted models. Degrees of freedom 1. Nagelkerke’s R2 = .101.
RAC = risky alcohol consumption. OR = odds ratio. CI = confidence interval. SE = standard error.
Crude and adjusted ORs with 95% CIs for early sexual debut (< 15 years).
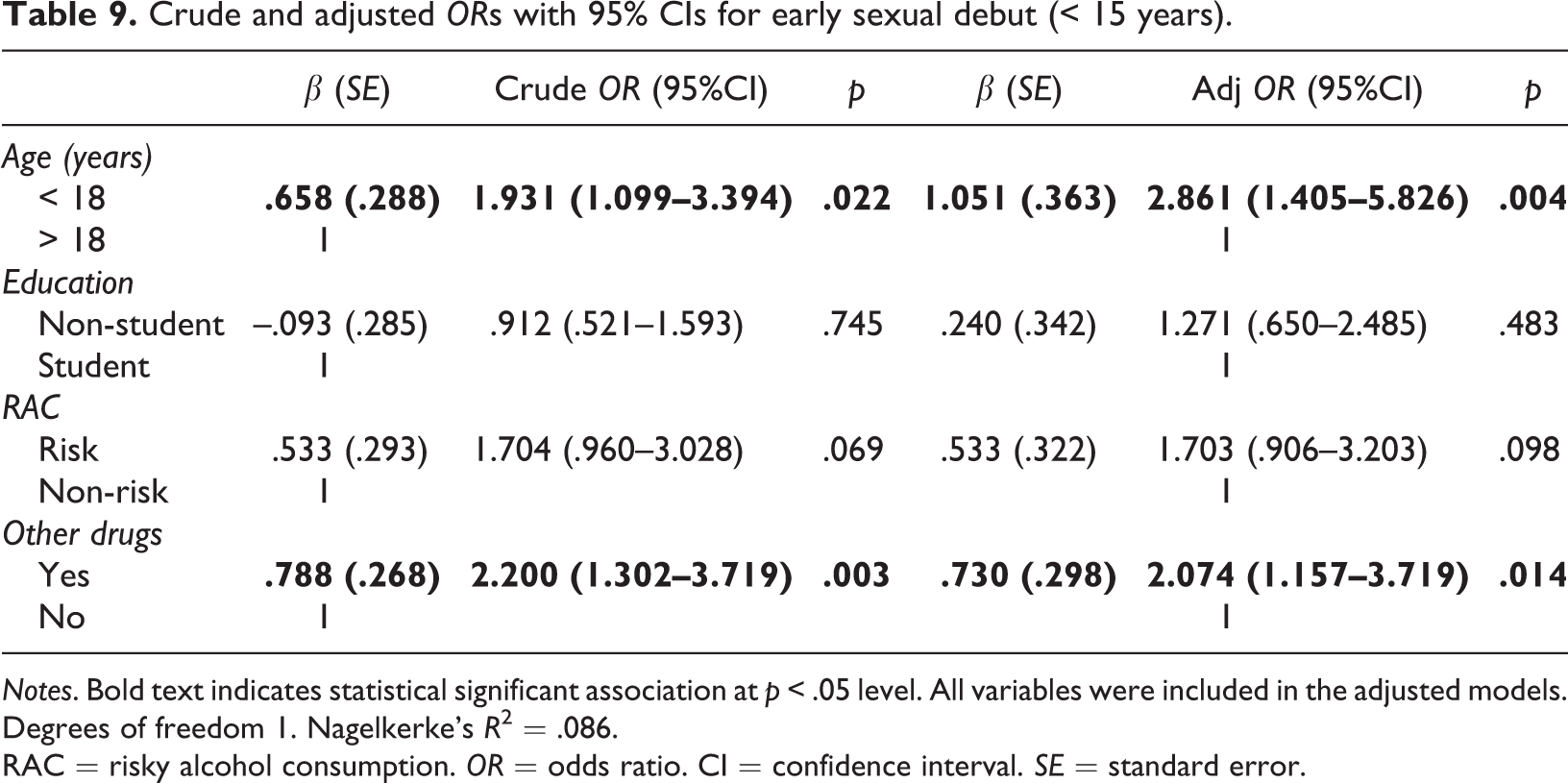
Notes. Bold text indicates statistical significant association at p < .05 level. All variables were included in the adjusted models. Degrees of freedom 1. Nagelkerke’s R2 = .086.
RAC = risky alcohol consumption. OR = odds ratio. CI = confidence interval. SE = standard error.
The results showed that respondents with a risky alcohol consumption were more likely to forget protection when having sex under the influence of alcohol (compared with non-risk consumers) (OR = 2.948). Also, having tried a drug other than alcohol significantly increased the likelihood of forgetting protection when having sex (OR = 2.307). In addition, non-students were more likely to forget protection when having sex than students (OR = 3.323). All variables were significant in the crude model, but age did not add significantly to the adjusted model (Table 5).
The results showed that respondents with a risky alcohol consumption were more likely to abstain from using protection when having sex under the influence of alcohol (compared with non-risk consumers) (OR = 3.230). In addition, non-students were more likely to abstain from protection when having sex, compared with students (OR = 2.227). All variables added significantly to the crude model, but in the adjusted model neither age nor having tried other drugs added significantly (Table 6).
In the adjusted model for STIs, only age added significantly; respondents under the age of 18 were less likely to have had an STI (compared with those over 18 years of age) (OR = 0.398). Risky alcohol consumption was not significantly associated with having had an STI, nor were any of the other included variables (Table 7).
The results showed that respondents with a risky alcohol consumption were more likely to rarely or never use protection when having sex with a new or casual partner (OR = 2.603). None of the other variables added significantly to the adjusted model (Table 8).
According to both crude and adjusted models, respondents under the age of 18 were more likely to have had an early sexual debut (OR = 2.861). Also, having tried a drug other than alcohol significantly increased the likelihood of early sexual debut (OR = 2.074). Risky alcohol consumption and educational status were not significantly associated with early sexual debut, either in the crude or in the adjusted model (Table 9).
Discussion
Summary of results
The results from the present study indicate that many youths visiting youth health clinics in Stockholm county have several risk behaviours, e.g., risky alcohol consumption, illicit drug use, and RSB. This is perhaps not surprising, as the aim of the work at youth health clinics is to help young people with issues concerning sexuality and health in a broad perspective. However, it emphasises the importance of alcohol and drug prevention work in this arena. Over 60% of the respondents reported risky alcohol consumption according to Audit-C. Risky behaviours were unevenly distributed with regard to educational status, showing higher figures among non-students than among students. Risky sexual behaviour was more common among respondents with risky alcohol consumption than among non-risk consumers. Moreover, after controlling for other factors, regression analyses showed that risky alcohol consumption was associated with a number of risky sexual behaviours, i.e., forgetting to use or abstaining from using protection when having sex under the influence of alcohol, and rarely or never using protection when having sex with a new or casual partner. Moreover, illicit drug use was associated with forgetting to use protection when having sex under the influence of alcohol, as was educational status (i.e., non-students); the latter was also associated with abstaining from using protection when having sex under the influence of alcohol. The factors significantly associated with early sexual debut were age and illicit drug use, respectively, while only age was associated with having had an STI. No gender differences were found regarding any of the studied risk behaviours. The result of non-significant gender differences regarding risky alcohol consumption may support the reduced gender gap during recent years (CAN, 2019; EMCDDA, 2016).
Comparison with previous research
The prevalence of risk behaviours among the respondents was in line with previous studies indicating that elevated levels of alcohol consumption are more prevalent among visitors at youth health clinics than among same-aged peers (Björnson & Haag, 2009; Karolinska Institutets folkhälsoakademi, 2010; Palm et al., 2016). As mentioned above, over 60% of the respondents reported risky alcohol consumption according to Audit-C. These figures are even higher than for young people who start a contact with outpatient care for alcohol and drug problems (Anderberg & Dahlberg, 2018). And in comparison, a Swedish study among university students showed that 45% exceeded the limit for risky alcohol consumption (Folkhälsomyndigheten, 2014). Studies among young people in general show that high alcohol consumption is common and often characterised by binge drinking (Andersson et al., 2009; Hingson et al., 2017; Knight et al., 2002; White et al., 2006), which was also common in the present sample, with 33% of respondents reporting binge drinking every month. Further, more than 40% had tried a drug other than alcohol, which is higher than the figure for the general population. A national survey in 2018 among Swedish high school students aged 16–17 years showed that 13% of the girls and 17% of the boys had tried a drug other than alcohol (CAN, 2019). This gives reason for great concern, that such a large proportion of young people (consisting mostly of girls) in the present study have tried some form of illicit drug. Moreover, data from a national survey in 2018 in the general Swedish population showed that 8.9% of people aged 16–29 years had tried cannabis in the last 12 months (Folkhälsomyndigheten, 2019). About three out of four respondents reported having had sex under the influence of alcohol. In comparison, a population survey among young people aged 16–29 years by the Public Health Agency of Sweden showed that 19% had used alcohol the last time they engaged in sex (Folkhälsomyndigheten, 2017). Although not equivalent, the difference in numbers is evident. Furthermore, individuals with a risky alcohol consumption reported RSB to a higher extent than those with non-risky alcohol consumption. These findings were expected and in line with previous research (Bellis & Hughes, 2004; Brookmeyer & Henrich, 2009; Chaney, Vail-Smith, Martin, & Cremeens-Matthews, 2016; Tapert et al., 2001; Thompson, Kao, & Thomas, 2005). Altogether, this shows that Youth health clinics is an important arena for preventive work and also for referring young people to treatment when such is needed. It is important that young people who have a risky alcohol consumption and/or use drugs receive relevant support for these problems. The youth health clinics have an important role in identifying the young people who need additional support and treatment for their alcohol and/or drug consumption, and in referring them to additional treatment at, for example, specialised outpatient clinics when such is needed. This can be particularly relevant for girls and young women. Today, girls who start outpatient treatment for alcohol and drug problems generally have more serious problems than boys (Anderberg & Dahlberg, 2018). Also, girls constitute a considerably smaller proportion in treatment, which suggests they do not get the help they need. If attention is payed earlier to alcohol and drug use among girls (e.g., at youth health clinics) they would probably be able to get relevant help at an earlier stage and thereby prevent future addiction problems.
However, we also found that risky alcohol consumption and RSB were significantly more common among non-students than among students. This is an interesting finding in the light of colleges and universities being environments that are often associated with excessive alcohol consumption (Labrie, Hummer, & Pedersen, 2007; Lorant, Nicaise, Soto, & d’Hoore, 2013). By controlling for other variables, running regression analyses, we were able to investigate the importance of a number of factors associated with RSB in the current sample. Risky alcohol consumption was significantly associated with three out of five types or indicators of RSB, which is in line with previous research (Brookmeyer & Henrich, 2009; Patrick et al., 2012; Rehm et al., 2012). The fact that risky alcohol consumption was not significantly associated with an early sexual debut indicates that this type of RSB may have other underlying reasons, e.g., a general orientation towards risk behaviours or impulsivity (Birthrong & Latzman, 2014; Charnigo et al., 2013). The finding that risky alcohol consumption was not independently associated with having had an STI in the current sample is a bit surprising, since risky alcohol consumption was associated with unprotected sex under the influence of alcohol (forgetting or abstaining from using protection), and unprotected sex is associated with STIs (Hall et al., 2015). Previous studies have also shown associations between alcohol consumption and STIs (Cook et al., 2002; Tapert et al., 2001). However, risky alcohol consumption was significantly associated with having had an STI in the crude model and almost reached a significant level in the adjusted model, indicating that a larger sample would probably have reached significance. Illicit drug use was associated with forgetting to use protection during sex under the influence of alcohol, and having had an early sexual debut. It was not significantly associated with the other three RSB outcomes. Illicit drug use has in previous studies been found to be associated with RSB (Brodbeck, Matter, & Moggi, 2006a; Brook, Brook, Pahl, & Montoya, 2002) and it is possible that a larger sample would have generated statistically significant associations with regard to other types or indicators of RSB in the current sample as well.
The findings that educational status (non-student) was associated both with forgetting to use and abstaining from using protection when having sex under the influence of alcohol, and that risky alcohol consumption was more prevalent among non-students are interesting. To the best of our knowledge, these results have not been obtained in previous studies and need further investigation in order to be more fully explained. An explanation could be the higher average age of the non-student group, and also that they have an income. We did not have enough statistical power in the present study to draw conclusions from subgroup analyses; however, it is an important aspect to keep in mind in the planning of future studies. That said, almost all non-students in the current study reported that they were currently working, i.e., presumably socially integrated and probably with certain demands of sobriety from employers. These circumstances indicate that the risk behaviours may not be a reflection of an underlying severe problematic or negative mental state (Gerhardstein, Griffin, & Hormes, 2011; Kelly et al., 1993), but could perhaps be associated with external factors. Apart from risk factors at the individual level, environmental factors can influence different risk behaviours. An example is that the availability of alcohol affects alcohol consumption (Babor, 2010). Generally, many youths are employed in the restaurant sector (Statistiska Centralbyrån, 2018), where alcohol is highly available and high rates of problem drinking have been found among employees, as compared with most other sectors (Duke, Ames, Moore, & Cunradi, 2013; Norström, Sundin, Müller, & Leifman, 2012). This could partially explain the high proportion of risk consumers of alcohol in the group of non-students. Unfortunately, we do not know in which sectors the non-students in our sample were employed, to what extent they were working, or what times during the day. Thus, we cannot say whether the risk behaviours were related to working conditions or working environment, or to other social or intrapersonal factors. In the regression models, we tested the inclusion of the interaction variable risky alcohol consumption × educational status, but it did not significantly contribute to the model for any of the RSB outcome variables. Further research regarding the reasons for non-students being especially vulnerable to risky alcohol consumption as well as RSB is needed, in order to effectively address risk behaviours among young people who are not studying. Overall, this is a relatively unexplored area and future research could also include larger longitudinal studies in this context and around this target group, to enable subgroup analyses and studies of risk behaviours over time. Youth health clinics appear to be an important arena for reaching young people with preventive efforts. Also, because of the geographical spread of the clinics they have the opportunity to reach young people from different milieus and with various social backgrounds, which should be noted in the research and performance of effective prevention methods.
Limitations
There are a number of limitations to this study. First, all participating youth health clinics were located in Stockholm, and the respondents are thus not a representative sample of the whole country (or the rest of the world). However, the participants are from various clinics throughout Stockholm, and although not nationally representative, are probably representative of visitors to youth health clinics in Stockholm county. Second, the data collection was not based on random sampling, which may have led to selection bias. However, the data collection method was the best available in the context. Sending questionnaires home to a random sample of young people who have visited youth health clinics would not be an option, since the work at youth health clinics is based on anonymity and parents are not necessarily informed about their children’s visits. Also, the fact that almost everyone who was asked to participate agreed to do so contributed to minimising the risk of selection bias. Third, the fact that we did not find differences in risky alcohol consumption or RSB relating to gender may be due to the low number of participating boys, which is a weakness in the study. Fourth, we do not know to what extent the non-students were working, what times during the day, or in which sectors they were employed, which limited the possibility to interpret the differences in behaviours between students and non-students. Last, but not least, the current study was cross-sectional, limiting the possibility to detect causal relationships between different variables.
Conclusion
In line with previous research, our findings indicate that a large proportion of visitors to Swedish youth health clinics in Stockholm county have a risky alcohol consumption and have tried drugs other than alcohol. Risky alcohol consumption was significantly associated with three of the five included RSB outcomes, while illicit drug use was associated with two. Non-students appeared as a particularly exposed risk group with regard to both risky alcohol consumption and RSB, calling for further investigation into reasons for this and ways to prevent risk behaviours in this group.
Footnotes
Acknowledgement
We are grateful to the participants who took the time to complete the questionnaire and thus made this study possible.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Public Health Agency of Sweden.
Supplemental material
The data that support the findings of this study are available from Centre for Psychiatry Research, an organized collaboration between Karolinska Institutet and Stockholm county council, but restrictions apply to the availability of these data, which were used under ethical permission for the current study, and so are not publicly available. However, data are available from the authors upon reasonable request and with permission from Centre for Psychiatry Research.