
Abstract
The history of the conceptualisation of the phenomenon of addiction is long and varied. Alcohol “intoxication, addiction, and dependency (AAD)”, for example, has been recorded since antiquity (Nathan et al., 2016). Attitudes towards affected individuals are strongly based on the assumed underlying aetiology of addiction. Its development over time has been described as “frequent pendulum swings” between moral and medical conceptions (Crocq, 2007; Nathan et al., 2016). In recent decades, the concept of addiction as a disease – a medical explanatory approach, often referred to as “medicalisation” – re-emerged in research and public perception around the middle of the 20th century (Campbell, 2012; Edwards, 2010). The medicalisation of addictive behaviour was subsequently reflected in its inclusion in the medical classification systems (International Statistical Classification of Diseases and Related Health Problems (ICD) and Diagnostic and Statistical Manual of Mental Disorders (DSM) (Edwards, 2010). While a moral conception of addiction persisted in parts of society, the focus of addiction research shifted towards a biomedical orientation. Towards the end of the last century, especially as a result of newly developed neuroscientific research methods such as magnetic resonance imaging (MRI) and functional MRI (fMRI), the brain became the primary target organ of addiction research (National Institute on Drug Abuse, 2020, p. 1; Rawson et al., 2014).
The conceptualisation of addiction as a brain disease gained popularity at the latest with the publication of the landmark paper “Addiction is a brain disease, and it matters” (Leshner, 1997) in 1997 by Alan Leshner, the then director of the American National Institute on Drug Abuse (NIDA). He and other proponents of a brain-based view on addictions envisioned improvements in several areas, such as better treatment options, reductions of stigmatisation, and better access to and financing of treatment (Dackis & O’Brien, 2005; Gartner et al., 2012; Leshner, 1997; Rawson et al., 2014; Volkow et al., 2016). The resulting shift from a moral to a medical understanding of addiction, particularly the so-called “brain disease model of addiction” (BDMA), has since been promoted by influential institutions and researchers (Koob & Volkow, 2010; Kuhar, 2015; National Institute on Drug Abuse, 2020; Volkow et al., 2016).
The claim that the characterisation of addiction as a brain disease was not “particularly controversial” in the scientific community was published among others in the journal Nature (Nature, 2014). This has fuelled an engaged discussion among researchers that seems unresolved to date (Hall et al., 2017; Heather et al., 2018, 2022; Heilig et al., 2021a, 2021b; Heim, 2014; Kalant, 2015; Room, 2021). Opponents of the BDMA highlighted the lack of evidence for the model and its utility (Hall & Carter, 2013; Hall et al., 2015a, 2017; Kalant, 2015; Satel & Lilienfeld, 2015, p. 14ff). Furthermore, they critically discussed the implications – hopes and expectations as well as adverse effects – of a brain-based or, more broadly, a medical understanding of addictions (Hall & Carter, 2013; Hall et al., 2015a, 2015b, 2017; Hammer et al., 2013; Heather et al., 2018; Heim, 2014; Levy, 2013; Trujols, 2015). In particular, a possible reduction of stigmatisation as well as the successes of pharmaceutical treatments, access to and funding of treatment in general, political reactions and the role of environmental factors belong to the wide range of implications of a brain disease model of addiction that have been discussed in the scientific literature (Dackis & O’Brien, 2005; Gartner et al., 2012; Hall & Carter, 2013; Hyman, 2007; Racine et al., 2017; Rise & Halkjelsvik, 2019; Rundle et al., 2021; Trujols, 2015; Volkow et al., 2016).
As of its 2018 edition, NIDA changed its terminology from disease to disorder in its flagship publication “Drugs, Brains, and Behavior” (National Institute on Drug Abuse, 2020). Therefore, this paper refers to “brain-based explanations of addiction”. In doing so, we intend to cover all explanatory models that locate addiction primarily in the brain, either as a disease or a disorder. Medical models and medicalisation refer to the classification of addiction as a disease. This is not necessarily located in the brain, but also encompasses brain-based explanations of addiction. Furthermore, NIDA conceptualises addiction as a severe substance use disorder (SUD), in line with the corresponding DSM-5 definition (National Institute on Drug Abuse, 2020, p. 4). However, this distinction is not made by all authors of scientific papers and in practice. SUD and addiction are also sometimes used as synonyms (American Addiction Centers, 2022; Avery et al., 2020; Bough & Pollock, 2018; Dubey et al., 2020).
One of the most prominent characteristics of brain-based understandings of addiction, according to their proponents, is that drug use leads to an “… erosion of free will” (Goldstein & Volkow, 2011). This claim is based on neuroscientific evidence for the effects of drugs predominantly on dopamine receptors in the brain and the impairments of the reward system and the regions responsible for self-control (Goldstein & Volkow, 2011; Koob & Volkow, 2010; Verdejo-García & Bechara, 2009). The resulting compulsive consumption, based on the impairment of self-control, is one of the core elements of brain-based models of addiction (National Institute on Drug Abuse, 2020, p. 4, 6; Wachbroit, 2006, p. 246). In contrast, opponents of this view emphasise the retained ability to take responsibility and make decisions (Heather & Segal, 2017; Heyman, 2010, 2013; Hyman, 2007; Peele, 2016; Uusitalo et al., 2013).
In practice, the question of whether an addicted person is responsible for their condition (“who is to blame for a past event”) and actions (“who is to control future events”) is crucial (Brickman et al., 1982; Koski-Jännes et al., 2012). Medical models of a condition are generally associated with lower levels of personal responsibility than moral or choice models and thus require, among others, treatment approaches based on experts (Blomqvist et al., 2014; Brickman et al., 1982; Lewis, 2016, p. 3; Palm, 2004). It has to be kept in mind, though, that the concept of responsibility encompasses two dimensions, the willingness and the ability to act (Koski-Jännes et al., 2012). Most discussions about the impact of brain-based explanations of addiction on perceived responsibility tend to address the ability to act, especially in connection with treatment and recovery (Hyman, 2007, 2010; Palm, 2004; Peele, 2016; Pickard, 2017; Racine et al., 2017; Satel & Lilienfeld, 2015, p. 58ff).
Primarily, the notion that an addictive substance “hijacks” the brain – especially the reward system – of a person implies that, subsequently, this individual has no choice anymore. The person's ability to act, their agency, is impaired, and consequently their responsibility is reduced in one way or another (Hyman, 2007; Peele, 2016; Uusitalo et al., 2013). This “erosion of free will” (Goldstein & Volkow, 2011) affects a wide range of areas and encompasses a variety of notions and aspects related to responsibility. For instance, the possible impairment of self-efficacy expectation, treatment-seeking and treatment-compliance of affected persons are discussed (Barnett & Fry, 2015; Bell et al., 2014; Dingel et al., 2017; Gartner et al., 2012; Morphett et al., 2017; Wiens & Walker, 2015). In particular, in affected persons who internalised a disease model, a perceived reduction of drinking self-efficacy was found (Wiens & Walker, 2015). In another study, those with a biological conception of their addiction tended to accept treatment better (Dingel et al., 2017). Furthermore, in their study of three different samples of lay people, Rise and Halkjelsvik found that the attribution of moral responsibility to addicted persons was lower in participants who conceptualised addiction as a disease or disorder (Rise & Halkjelsvik, 2019). Treatment providers are reported to consider a disease model to potentially undermine the personal responsibility of addicted persons, as well as increase their sense of helplessness (Barnett & Fry, 2015; Barnett et al., 2018; Bell et al., 2014), but also their treatment-seeking behaviour (Barnett et al., 2018; Bell et al., 2014). Karasaki and colleagues, however, found ambiguities regarding the place of legal and moral responsibility (“volition”) in addiction in their study of treatment providers (Karasaki et al., 2013).
Overall, several empirical investigations into the views of different stakeholder groups on various implications of brain-based explanations of addiction or, more broadly, on disease models have been conducted. For example, a review of treatment providers’ perspectives showed mixed support for a disease model. Moreover, regarding its implications, mixed views with positive (insight increased, stigma reduced) and negative (sense of helplessness, responsibility reduced) components were identified (Barnett et al., 2018).
Further, studies investigating the opinions of affected persons (Dingel et al., 2017; Morphett et al., 2017; Wiens & Walker, 2015) and the general public (Meurk et al., 2013; Meurk, Carter et al., 2014; Racine et al., 2017; Rise & Halkjelsvik, 2019; Rundle et al., 2021) on themes such as stigma, shame and blame, responsibilities, self-efficacy expectation and treatment seeking reported no homogeneous results. “Mixed blessings” of brain-based explanations of addiction, described by Haslam and Kvaale for neurogenetic explanations of mental disorders (Haslam & Kvaale, 2015), seems to represent the findings best.
Addiction researchers, however, constitute a widely under-researched stakeholder group. The necessity to assess their views is grounded in the significant role they play and the wide range of implications of their work. The conception of addiction is largely based on scientific findings and researchers determine the research direction. Further, they develop and evaluate interventions, frame the research results, communicate to the media and the public and shape their understandings, and are important advisors for policy (Douglas, 2009, p. 1ff; Haas, 1997, p. 2; Kuruvilla et al., 2006; Löblová, 2018; Strang, 1992). Therefore: “… what addiction researchers say matters” (Pickard & Ahmed, 2020, p. 1).
Regarding the implications of brain-based explanations of addiction, to our knowledge, two studies assessed addiction researchers’ perspectives. In one of the studies involving 31 Australian addiction neuroscientists (partly also clinicians), about one-third was reported to endorse the BDMA and to consider the concept to be extremely helpful (Bell et al., 2014). Nearly half held an ambivalent view, and the rest evaluated it negatively. Regarding the model's clinical impact, the main implications mentioned by the participants were improvements in treatment and a reduction in punishments, as well as the concern that treatment seeking and the willingness to change behaviour could be hindered. In the second study, involving 20 American nicotine research scientists, the participants were observed predominantly to hold a medicalised view of addiction, but to consider environmental factors to constitute the primary causes of smoking initiation. They further did not expect a medicalised understanding of smoking to reduce stigma (Dingel et al., 2012).
If it matters that addiction is a disease or disorder of the brain, as was claimed by Leshner and others (Heilig et al., 2021a; Kuhar, 2015; Leshner, 1997; National Institute on Drug Abuse, 2020; Volkow & Boyle, 2018; Volkow et al., 2016), the extent to which different stakeholder groups think it matters, as well as the implications of this understanding need to be explored. Brain-based explanations of addiction have now been communicated and advocated by major organisations for a relatively long time (Brick & Erickson, 1998; Hellman & Egerer, 2022; Leshner, 1997; National Institute on Drug Abuse, 2020; Satel & Lilienfeld, 2015, p. 50ff; Volkow & Li, 2004). Given their significant role, there is a particular need to examine researchers’ opinions of what they consider to be the major implications of this view on a larger scale than is currently available. Special attention has to be drawn to the affected individuals’ responsibility, as this represents one of the issues with potentially the most far-reaching practical consequences.
Therefore, the aim of this paper was to complement the aforementioned studies by directly exploring the current status of addiction researchers’ perspectives on implications of brain-based explanations of addiction and the responsibilities of addicted individuals on a comparatively large scale, internationally, and with a multidisciplinary orientation. To this end, addiction researchers were surveyed online about (1) what they consider to be the most important consequences of brain-based explanations of addictions and (2) whether they consider addicted individuals to be responsible for their condition and/or for their actions.
Methods
The study was conducted as a part of the ERA-NET funded study “Addiction in the Brain: Ethically Sound Implementation in Governance” (A-BRAIN).
Ethics approval, including the data protection concept, was granted from the University of Bremen/Germany on December 6, 2018.
Participants
The sample was compiled in August 2018 using a purposeful and feasible approach. It included the editorial board members of all journals listed in the Journal Citation Report 2018 (JCR) of Clarivate Analytics (Clarivate Analytics, 2020) in the categories “substance abuse” (scie & ssci) and “medical ethics” (scie) (n = 2586), and the members of the “International Society of Addiction Journal Editors” (ISAJE) (International Society of Addiction Journal Editors, 2020) (n = 51).
To ensure the representation of a broad range of opinions and scholarly orientations, the sample was expanded to include: (1) National Institutes of Health advisors (NIH; “National Advisory Council on Drug Abuse” (NACD); n = 20) (National Institute on Drug Abuse (NIDA), 2018b); (2) National Institute on Drug Abuse reviewers (NIDA; “Pathophysiological Basis of Mental Disorders and Addictions Study Section, Center for Scientific Review” (PMDA); n = 18) (National Institutes of Health (NIH), 2018); (3) the signatories of the letter to the editor in the journal Nature “Addiction: Not just brain dysfunction” (n = 94) (Heim, 2014); and (4) the speakers at the multidisciplinary “Addiction, the Brain and Society Conference 2009” (n = 26) (Dunbar et al., 2010), which was organised by the Emory University “Science and Society” programme, funded by the Engelhard Foundation. Their aim is “challenging human, social and neuroscientists to bridge the disciplinary divides within addiction research by involving each other with their claims and methods”. In addition, to include experts who might not have been identified thus far, participants were asked to name further researchers from the field (snowballs) they thought should be included in the study (n = 175).
After the elimination of duplicates, the sample was finalised by excluding (1) members of the A-BRAIN project consortium, (2) deceased persons, (3) those with invalid contact information, (4) persons with less than three publications on addictions in the past 15 years (probably other research focus), and (5) persons who responded that they did not consider themselves to be addiction researchers. The final sample included 1440 people from 49 countries.
Instrument and procedure
A literature review identified various aspects discussed in the context of brain-based explanations of addiction, which formed the basis for the questionnaire. The databases PubMed (medical focus), PsychInfo (psychological focus) and Sociological Abstracts (sociological focus) were searched using the search terms “brain disease model of addiction”, “brain disease” AND “addiction”, and “brain disease” AND “SUD” in titles and abstracts. Manuscripts in all languages and published from 2007 (first edition of NIDA's “Drugs, Brains, and Behavior” (National Institute on Drug Abuse (NIDA), 2018a)) to May 2018 were included. From 71 papers, themes were extracted and incorporated in a preliminary questionnaire, which was then pre-tested and revised accordingly.
The final questionnaire was distributed, and data were collected online via a LimeSurvey. Potential participants received a maximum of three personal email invitations to participate in the survey, the invitation and two reminders. The data collection period started in February and ended in August 2019, two weeks after the last responses based on the last reminder had been received.
Participants could choose between English and German. Furthermore, they could select the substance(s)/behaviour(s) for which they wanted to answer from a drop-down list that allowed for multiple choices. The quantitative questions then had to be answered separately for each substance selected. As default options, alcohol, smoking, smokeless tobacco, cannabis and gambling were available. Further substances or behaviours of choice could be added via a separate field.
In addition, details on the following participants’ basic demographic variables were assessed to describe the sample composition: age, sex, country of workplace and academic background (academic degree, grouped according to the main categories of the bepress taxonomy of academic disciplines (bepress, 2019)).
Data and analysis
This paper presents the results of the responses to two of the survey's core questions. From the perspective of addiction researchers:
What are the most important consequences of classifying substance use disorder (SUD) as a “medical disorder that affects the brain”? Do participants agree or disagree with the statements that persons with SUD are responsible for their conditions and actions?
Question (1) was an open question. Question (2) could be answered by choosing one option from a Likert-type scale (very strongly disagree, strongly disagree, partly disagree, partly agree, strongly agree, very strongly agree) or “I don’t know” for each of the previously selected substance(s)/behaviour(s), and by providing comments via a free-text field.
The free-text comments were analysed qualitatively by applying an iterative inductive approach (Mayring, 2015) on a semantic level (Braun & Clarke, 2006, p. 13). In addition, for the responses to question (1), the (deductive) coding scheme reported by Bell et al. (Bell et al., 2014) was applied. They classified the qualitative data from interviews with 31 Australian addiction neuroscientists on the impact of the brain disease model of addiction as exclusively positive, exclusively negative or neutral/ambivalent (both positive and negative implications mentioned).
The initial coding was independently conducted by DO and a student assistant. The overall assessment of the general impact of brain-based explanations of addiction mentioned by the participants was then conducted by DO and JF (a colleague not involved in the study), based on the coding scheme suggested by Bell et al. (Bell et al., 2014). DO and JF discussed all results, resolved discrepancies and agreed upon common codes. This approach is in line with Bengtsson's recommendations (Bengtsson, 2016) to engage a colleague not involved in the study to reduce bias based on the prior knowledge of the coders. The coding was performed using MAXQDA10 software.
The quantitative analyses of the answers to question (2), assessed via a Likert scale, were conducted separately for the substance(s)/behaviour(s) selected by the participants. Frequencies and proportions were calculated using IBM SPSS Statistics 24 software.
Results
Altogether, 190 researchers from 29 countries participated in the online survey (13.2% response rate; 66.8% males, 32.1% females, 1.1% unknown). Of the respondents, 61.6% were from English-speaking countries, predominantly from the USA with 41.6%. They were similar to the invited primary sample (for details, please see Supplementary Table S2). However, no researchers from the African continent, as well as from several other countries with a low number of invited potential participants, such as Nepal, Thailand or Lebanon, participated. In addition, the response rate was slightly higher among men than among women. The sample characteristics regarding gender, country of workplace and academic degrees are summarised in Table 1. Age was excluded due to the high number of missing values (25.3%).
Participants’ characteristics.
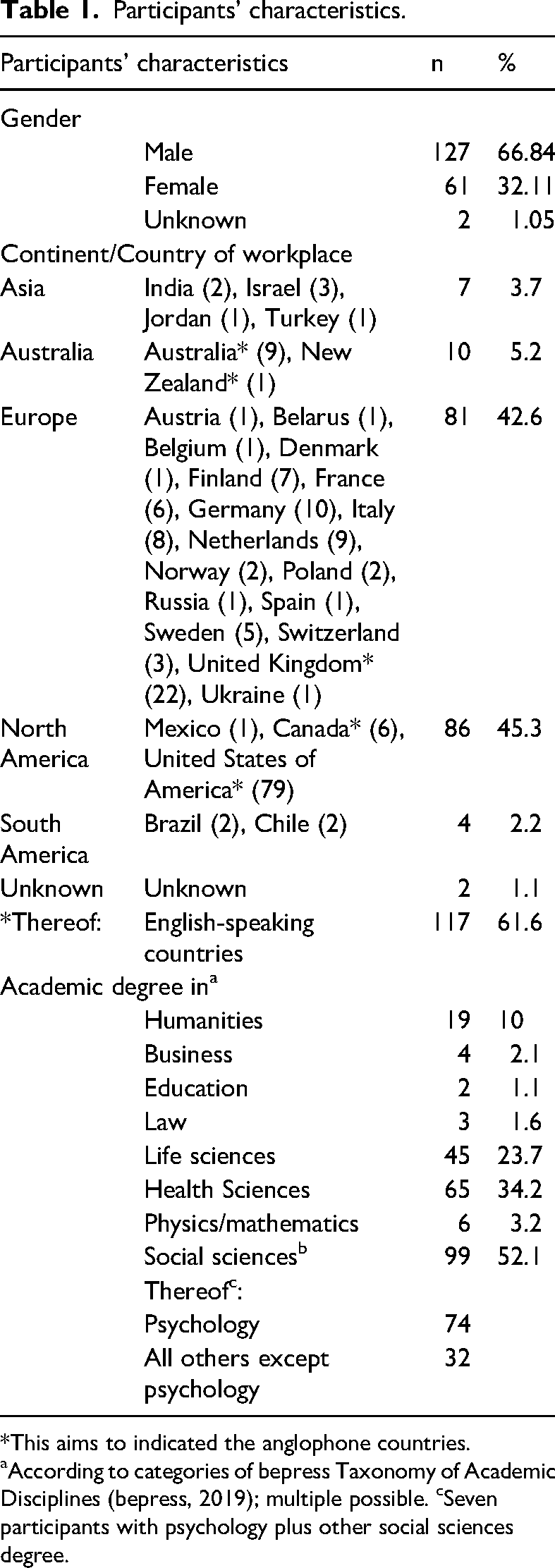
*This aims to indicated the anglophone countries.
aAccording to categories of bepress Taxonomy of Academic Disciplines (bepress, 2019); multiple possible. cSeven participants with psychology plus other social sciences degree.
Implications of brain-based explanations of addiction
A total of 138 participants shared their views on what they considered to be the most important consequences of brain-based explanations of SUDs. The qualitative content analysis of the answers yielded statements relating to three main thematic areas: (1) treatment/interventions (n = 116); (2) society's reaction (n = 61); and (3) affected persons (n = 39). Two respondents stated that they didn’t know and three others that they expected no changes.
In terms of treatment approaches (area 1), the largest proportion of the participants (n = 46) expected a medicalisation of addiction and expressed concerns about the neglect of other contributing factors, for example:
“This approach ignores the environmental and biopsychosocial determinants of substance use initiation, maintenance and harm. A medical understanding of substance use discounts the importance of psychosocial intervention and natural/spontaneous recovery, and the importance of health and protective environments such as addressing poverty, housing, and social exclusion.” (S100) “A higher number of persons affected by alcohol use disorder would require and receive medical treatment for their mental disorder. A higher number of physicians would prescribe medications for the treatment of this mental disorder.” (S117) “Treatment would be more widely available. Treatment options would be more diverse (e.g., pharmacotherapeutics). Treatment options would be of longer duration…” (S12) “Pathological approach to a social problem. However, it would probably help most severe cases to get proper support.” (S245) “this could lead to less stigma and could possibly reduce the perception that addiction is a moral failure” (S212) “less stigma and blaming of the individual” (S242) “I am hopeful that medicalisation of addiction could reduce stigma” (S40) “Would de-stigmatise the addiction process, allowing dependent people to more openly deal with their dependency” (S263) “has one of the biggest stigma within mental disorders” (S82) “and yet the stigma persists” (S55) “I think that people would stigmatise addiction or SUD anew – as ‘brain-damage’, as ‘something wrong with a person's brain’. I do not think that scientific constructs will de-stigmatise this group of disorders” (S174) “Seeing SUD as a medical disorder (primary or secondary) can help patients and families to see the SUD differently, take away part of the culpability, and improve access/adherence to treatment (not only medical!). But also can give patients a ‘passive role’ where they have no choice (which is not correct in my view).” (S195) “… it can disempower people who have the capacity to abstain or control substance use in the face of the biological risk.” (S228) “I am afraid that this may reduce the involvement of addicts in their own treatment. Addicts may be less likely to use psychological therapy (especially cognitive-behavioural) and group support. This may lead to some kind of passive medical treatment. External locus of health control is usually less effective…” (S92)
Others envisioned that more treatment options (n = 10) and new or better medications (n = 16) would be available. Furthermore, 44 expected that there would be improved access to and funding of treatment. This was predominantly acknowledged as an advantage, but not exclusively seen as positive by all participants. Moreover, medications were considered as one helpful element of a multi-component treatment strategy. Examples of some of the participants’ responses are listed hereafter:
Regarding society's reactions (area 2), stigmatisation/blame/discrimination was the dominant theme mentioned (n = 44). A reduction was expected by 32 participants, an increase by seven, new forms of stigma by two and no change by two participants. One participant, however, expected blame to be reduced, but stigma to increase. Some of the participants responded as follows:
The mentioned implications of brain-based explanations of addictions on affected individuals (area 3) mainly concerned a reduction of agency (n = 18). Eleven participants expected the treatment-seeking behaviour of addicted persons to increase and two expected a decrease. Examples of the participants’ responses are:
The overall evaluation of the issues mentioned by the respondents in terms of whether the implications were positive, negative or neutral/ambivalent/both (positive and negative, summarised as “ambivalent”), as suggested by Bell et al. (Bell et al., 2014), is shown in Table 2. A total of 63 (45.7%) researchers mentioned only positive implications, 45 (32.6%) expected only negative ones and 22 (15.9%) saw both positive and negative or neutral consequences. Two (1.5%) participants stated that they didn’t know, 3 (2.2%) expected no changes and the statements of 3 (2.2%) further respondents were unclear and could thus not be included in one of the above categories.
Responsibility of addicted persons for condition and actions
The descriptive analysis of the perceived responsibility for the condition and actions of addicted individuals, assessed using a Likert scale, showed that slightly less than 60% of all participating researchers attributed the responsibility for the condition (substance use disorder) to the affected person, whereas about 80% perceived addicted individuals as being responsible for their actions (Figure 1; Supplementary Table S1). Only minor deviations could be observed between the different substances. Very strong agreement/disagreement was rarely voiced, while partial and strong agreement/disagreement predominated. Participants who responded for several substances tended to take the same attitude for all substances, albeit sometimes to different degrees.
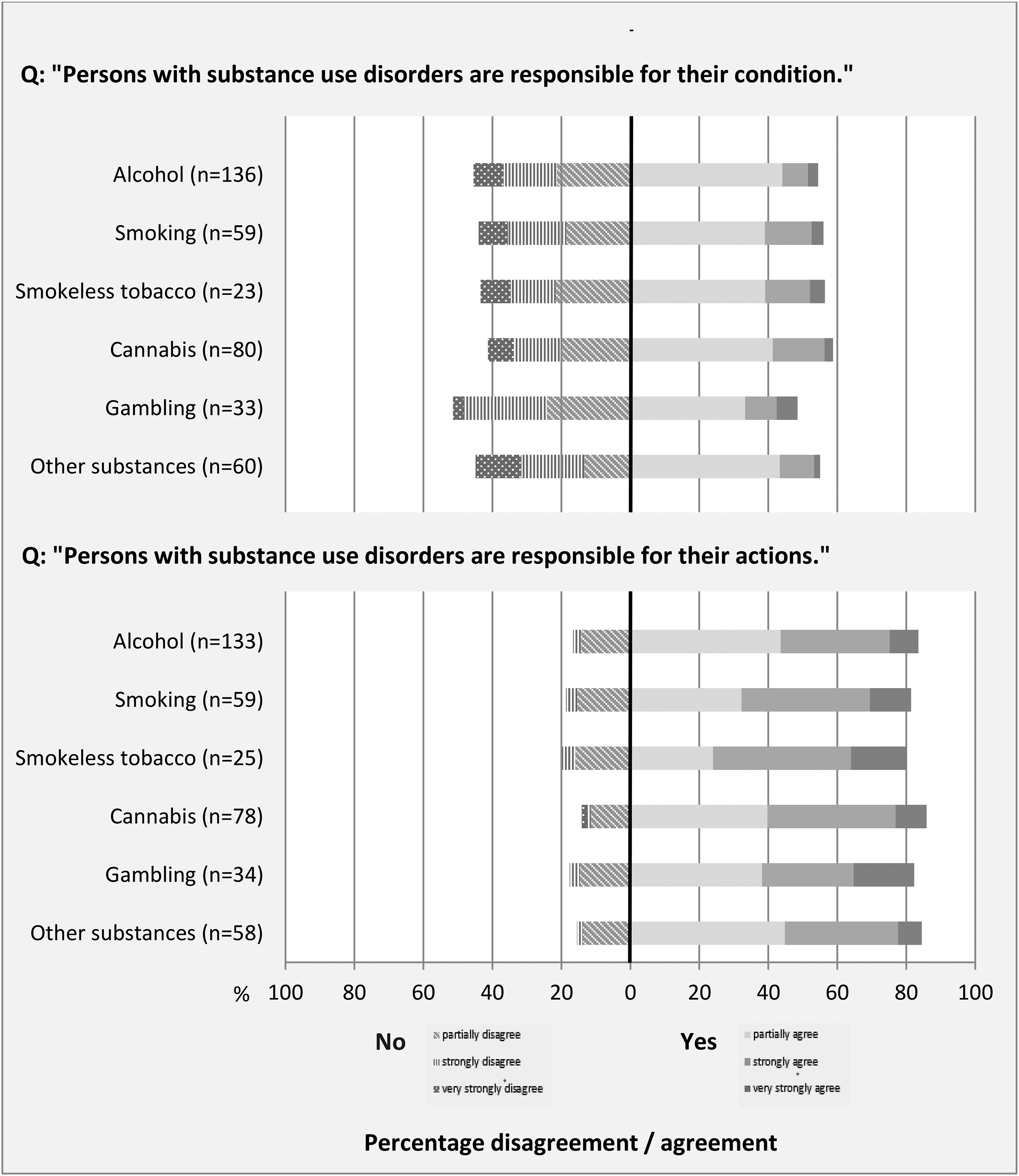
Responsibility of addicted persons for their condition and their actions as perceived by addiction researchers.
Implications of brain-based explanations of addiction according to addiction researchers: overall evaluation.
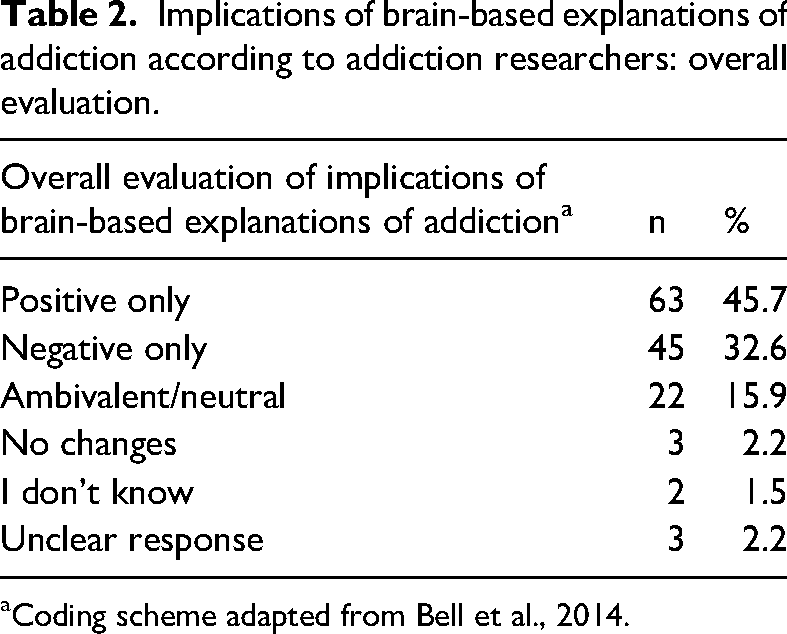
Coding scheme adapted from Bell et al., 2014.
In total, 39 participants provided additional comments that helped frame the results. In the course of the qualitative analysis, four main categories of recurrent themes emerged: (1) a mono-causal, simplistic approach was rejected by nine participants. (2) Ten participants referred to treatment and the healthcare system, with four stressing the responsibility of society, government and professionals. A further four emphasised that help-seeking has also to be considered as taking responsibility and two demanded empowerment or education about risks in this context. (3) Eight researchers highlighted the role of stage/severity in the ability of addicted individuals to take responsibility. (4) Nine participants in the study emphasised that taking responsibility is not to be understood in a moral sense such as assigning blame or punishment, but in the sense of taking control: “responsibility without blame” (quote from respondent S71).
Discussion and conclusions
Brain-based explanations of addiction have now been promoted for many years (Brick & Erickson, 1998; Hellman & Egerer, 2022; Leshner, 1997; National Institute on Drug Abuse, 2020; Satel & Lilienfeld, 2015, p. 50ff; Volkow & Li, 2004). After this considerable period of time, the current exploration of 190 addiction researchers’ views on the concepts’ perceived most important implications and of affected persons’ responsibilities yielded interesting results. The international nature of the study with participants from 29 countries and the broad range of scientific disciplines covered complements previous investigations of addiction researchers, namely 20 American scientists in tobacco research (Dingel et al., 2012) and 31 Australian addiction neuroscientists (Bell et al., 2014; Carter et al., 2014).
The two most frequently mentioned benefits of classifying addiction as a brain disease were better treatment access and adherence, and a reduction of stigma and blame. In addition, the development of new and potentially better medications and more treatment options echo the main hopes and expectations placed in the model by its advocates (Dackis & O’Brien, 2005; Gartner et al., 2012; Leshner, 1997; Volkow et al., 2016).
These views of addiction researchers are only partly in line with previous research among various stakeholder groups, especially in the case of stigmatisation. While participants in some studies did not expect stigma to decrease with a brain-disease or otherwise medicalised view of addictions (Dingel et al., 2012; Meurk, Partridge et al., 2014; Morphett et al., 2017; Rundle et al., 2021; Wiens & Walker, 2015), in others they did (Barnett et al., 2018; Dingel et al., 2017). Regarding better access to treatment as a result of the framing of addiction as a disease or disorder, there seems to be a consensus among supporters and opponents of the model (Dackis & O’Brien, 2005; Hall et al., 2003; Volkow & Koob, 2015). In our study, the value placed on better treatment options was mainly based on medications as an additional part of a multi-component strategy rather than on the prospect of the success of purely medical procedures.
On the other hand, many participants seemed to be concerned about a medicalisation of addiction due to the focus on brain changes and the accompanying neglect of psycho-social factors. Moreover, the impairment of agency and responsibility of affected individuals was considered a major problem of brain-based explanations of addiction. A passive role with less personal engagement may result, which could significantly challenge all treatment and support efforts, whether in the healthcare system, in society or in the individual's social environment.
The overall evaluation of the implications mentioned by the respondents did not show a clear tendency toward positive or negative effects of a brain-based approach. Approximately 46% mentioned exclusively positive consequences, approximately 33% only negative ones and approximately 16% were ambivalent, meaning they either named both positive and negative issues or neutral consequences. A comparable mixed result was also found by Bell et al., but with a stronger tendency to an ambivalent view among their participants and a smaller percentage of positive evaluations (Bell et al., 2014). It should be kept in mind, however, that Bell et al. interpreted their qualitative results as an evaluation of brain-based explanations of addiction in general and as an endorsement of the BDMA by their respondents in particular (Bell et al., 2014). This does not apply to the present study. Instead, the implications mentioned by the participants here indicate where they believe the problems and the utility of this concept lie – and thus the areas that need to be addressed in future research and practice.
Altogether, the perceptions of addiction researchers regarding the most important implications of brain-based explanations of addiction can be summarised as “mixed blessings”, as described by Haslam and Kvaale for neurogenetic explanations of mental disorders (Haslam & Kvaale, 2015). The awareness and evaluation of what is perceived as most important – after a prolonged promotion of brain-based explanations of addiction and its controversial discussion in the scientific literature – might reflect the heterogeneity of the addiction research community. Still, it also clearly shows that simplistic approaches based solely on neuroscientific evidence are not the majority opinion, even if some of their benefits are acknowledged.
The finding with the potentially most considerable practical relevance is the participants’ evaluation of affected individuals’ responsibilities, especially the strong attribution of responsibility for their actions (about 80%). This can be interpreted in two ways. Either the claim of the “hijacked brain” with a resulting substantial loss of control (Dackis & O’Brien, 2005) is generally not endorsed by the majority of the study participants, or else they do not believe that brain changes in addicted individuals induce an impairment of agency and responsibility. Further research is needed to clarify these issues.
Regardless of the explanation for these findings, their implications are far-reaching and important. Preserved responsibility of addicted persons, first and foremost, implies that they are supposed to take the leading role in their treatment – and not an expert (Blomqvist et al., 2014; Brickman et al., 1982). Addicted individuals remain active agents, which also might mean that they are responsible for seeking help instead of solving their problems all on their own. However, this view does not necessarily reflect a moral conception of addiction. As some participants state, a “responsibility without blame” framework seems to be an option that acknowledges that there is a choice but avoids a “critical moral stance” against this choice (Pickard, 2017).
According to test analyses, there were no differences in participants’ perceptions that could be explained by their academic degree, gender or country. However, due to some very small cell sizes, the multivariate logistic regression analyses were considered to be severely limited. Therefore, we did not include these results in the main body of this paper.
As the aim of this study was explicitly not to focus on severe cases only, the term SUD was used instead of addiction in the questionnaire (National Institute on Drug Abuse, 2020, p. 4). Post-hoc analyses of all free-text contributions from all participants confirmed the authors’ assumption that SUD and addiction were used interchangeably. In their responses, some participants used SUD, some used addiction, and some used addiction and SUD in the same context as obvious synonyms. Therefore, in this paper we used the term “brain-based explanations of addiction” when referring to our research findings.
The present study has some limitations. The first concerns the definition and identification of the target group. Addiction research is a broad, interdisciplinary field with no clear boundaries. The sampling process was thus designed to include as many academic disciplines as possible, as well as competing opinions towards brain-based explanations of addictions. In addition, a snowball-mechanism that allowed respondents to name further possible participants was meant to account for missing experts in the primary sample. Nevertheless, it cannot be completely ruled out that important researchers were inadvertently not included.
Further, while the response rate of 13.2% is slightly higher than in studies with comparable target groups and data collection strategies (Mulligan et al., 2013), it is not high enough to ensure representativity. The study is thus exploratory by nature.
The fact that almost two-thirds of the participants were from English-speaking countries, predominantly from the USA, limits the generalisability of the results to other countries.
The study also has methodological limitations inherent in qualitative research that predominantly relate to the basic approach and the instrument chosen. The content analysis of the free-text comments provided by the participants followed an iterative-inductive approach as recommended for expert interviews (Gläser & Laudel, 2010) and described by Mayring (Mayring, 2015). The core underlying assumption of the approach is the rather quantitative idea that the more often an issue is mentioned, the more importance has to be assigned to it (Seale, 1999, p. 119ff). This is not undisputed (Braun & Clarke, 2006, p. 10; Kuckartz, 2018, p. 54), as marginal or low-prevalent themes – even if mentioned by only a single participant – might, in reality, be more important to, for example, affected persons than frequently mentioned issues (Braun & Clarke, 2006, p. 19). The focus of this paper was, however, to identify issues that were considered important by a relatively large proportion of respondents and the subsequent description of their opinions. The exhaustive presentation of marginal themes would have exceeded the scope of this paper.
The individuals who coded the data were naturally shaped by their prior knowledge about the discussions in the field. This is a general quality – and sometimes a limitation – of qualitative research (Bengtsson, 2016; Braun & Clarke, 2013, p. 20, 279; Kuckartz, 2018, p. 71, 206; Seale, 1999, p. 23). It was accounted for by choosing two coders with different levels of background knowledge, as recommended by Bengtsson (Bengtsson, 2016).
The quantitative approach to evaluating responsibilities also has limitations. Likert-type scale responses give us an overview or trend of participants’ (dis)agreement with statements, but they are not a method for a differentiated investigation. For example, it was not possible to account for different stages and severities of addictions or to address the implications of the statements, such as the issue of blame in the context of preserved responsibility. Different aspects and conceptions of responsibility could not be investigated in depth. In addition, the forced-choice approach to the Likert scale did not allow for neutral positions, and the inclusion of partial (dis-)agreement as a yes or no requires a nuanced interpretation. The multiple-choice questions were therefore complemented by free-text fields (“mixed methods light” (Creswell & Plano Clark, 2018)) to allow participants to comment, with the aim to increase the depth of understanding, frame the results and add further aspects (Rhodes & Coomber, 2010).
The special contribution of this study is that it examines and summarises the views of a comparatively large and interdisciplinary group of researchers. After a long period of promoting brain-based explanations of addiction and focusing on neuroscientific approaches in research funding (Hall et al., 2015b, 2017; Vrecko, 2010), we focus on the implication now perceived as important. All in all, both limitations and potentials, “mixed blessings” (Haslam & Kvaale, 2015), were acknowledged.
Based on these findings, we conclude that, especially in the treatment field, a multicomponent approach needs to be further pursued. The strategic utilisation of brain-based explanations, as was found among treatment providers (Barnett et al., 2018), would also make sense based on the views expressed by addiction researchers in this study. A predominantly brain-based view, and thus a medical treatment approach, was not the majority approach supported by the participants. In summary, the medicalisation of addiction was viewed as a major problem. The possible neglect of other than biomedical factors that contribute to the development and maintenance of addiction therefore constitutes a major concern.
Furthermore, special attention has to be paid to the role of the addicted individual and the effects of a brain-based view of addiction on various aspects of their agency. For instance, the danger of taking on a passive role and of disempowerment, and the possibly resulting reduced involvement of affected persons in their therapy need to be made more aware and addressed in the future. Since a clear majority of the respondents attributed the responsibility for actions to those affected, an “expert model” in treatment (Blomqvist et al., 2014; Brickman et al., 1982) needs to be replaced. Treatment concepts of responsibly involving the addicted persons need to be further developed, and various aspects of responsibility, which could not be investigated in depth in this study, need to be identified and addressed.
Given the special role and responsibility that researchers, the target group of this study, have, it is important to also reconsider research priorities. A strong focus of research funding for neuroscientifically oriented research has been discussed in the literature (Hall et al., 2015b, 2017; Vrecko, 2010). This needs to be replaced by approaches that reflect all aspects involved in developing, maintaining and treating addiction. Guidelines for research priorities, such as those based on a study involving members of the Lancet Mental Health Group (Tomlinson et al., 2009), need to be further developed. In light of the results presented, a reconsideration of future research priorities, which should include neuroscientific as well as psychological and social factors, seems to be required.
The further development of an ethically sound integration of brain-based explanations of addiction into a multidisciplinary concept still seems to be warranted. It needs to materialise in research (funding) as well as practice.
Supplemental Material
sj-docx-1-nad-10.1177_14550725231188802 - Supplemental material for A survey of international addiction researchers’ views on implications of brain-based explanations of addiction and the responsibility of affected persons
Supplemental material, sj-docx-1-nad-10.1177_14550725231188802 for A survey of international addiction researchers’ views on implications of brain-based explanations of addiction and the responsibility of affected persons by Doris Ochterbeck, Jennifer Frense and Sarah Forberger in Nordic Studies on Alcohol and Drugs
Supplemental Material
sj-docx-2-nad-10.1177_14550725231188802 - Supplemental material for A survey of international addiction researchers’ views on implications of brain-based explanations of addiction and the responsibility of affected persons
Supplemental material, sj-docx-2-nad-10.1177_14550725231188802 for A survey of international addiction researchers’ views on implications of brain-based explanations of addiction and the responsibility of affected persons by Doris Ochterbeck, Jennifer Frense and Sarah Forberger in Nordic Studies on Alcohol and Drugs
Footnotes
Acknowledgements
The authors would like to express their sincere thanks to Dr. Christoph Buck (Leibniz Institute for Prevention Research and Epidemiology – BIPS, Bremen, Germany) for the support provided with the statistics, and Dr. Florence Samkange-Zeeb (Leibniz Institute for Prevention Research and Epidemiology – BIPS, Bremen, Germany) for her valuable language editing and comments.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The presented results are part of work package 1.2 “epistemic communities and stakeholders” of the ERA-NET funded study “Addiction in the Brain: Ethically Sound Implementation in Governance” (A-BRAIN; Project PI: Matilda Hellman; Site PIs: Patricia Conrod, Sarah Forberger, Matilda Hellman, Christian Hendershot). This work package is funded by the German Ministry for Education and Research (Bundesministerium für Bildung und Forschung, NEURON JTC, 14 March 2018, funding reference number: 10GP1823).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.