
Abstract
School dropout is a serious public health, economic and labour market concern and is associated with negative outcomes on both the individual and societal levels (Chou et al., 2006; De Ridder et al., 2012; Egger et al., 2003; Jaafar et al., 2013; Mussida et al., 2019). In Organisation for Economic Co-operating and Development (OECD) countries, almost one in five students do not complete upper secondary school (OECD, 2022). To more effectively challenge the problem with school dropout, it is important to gain better insight into the risk factors for dropout, as these may be targeted to promote completion of upper secondary school, and thus contribute to better prospects for adolescents at-risk for negative educational outcomes (Gubbels et al., 2019).
Although several studies indicate that early school leaving may contribute to the development of risky substance use (RSU), it is also established that RSU is a common risk factor that may precede school dropout (Esch et al., 2014; Horwood et al., 2010). Previous studies have found that different expressions of RSU are associated with school dropout, however potentially with different magnitude (Davis et al., 2022). Cannabis use appears to be fairly consistently associated with school dropout (Coffey & Patton, 2016; Horwood et al., 2010). A meta-analytic study indicated that early use of cannabis accounted for 17% of the overall rate of school dropout, when adjusting for sociodemographic characteristics, child cognitive ability and family functioning (Horwood et al., 2010). Regarding alcohol use, the literature is more inconclusive. Whereas a literature review reported that alcohol consumption was not associated with school dropout (Esch et al., 2014), several studies have reported positive associations between alcohol use and dropout (Grant et al., 2012; Kelly et al., 2015; Rose et al., 2014; Waldron et al., 2018). For example, a longitudinal analysis – conducted before the abovementioned literature review – reported that students aged 14–15 years with mainly alcohol use were at higher risk of school dropout at age 19–23 years compared with abstinent students (Kelly et al., 2015). These effects were independent of school commitment, academic failure, peer drug use and other control variables. Several other studies have documented that substance use disorders (which include abuse or dependence, and thus represent the extreme end on a continuum of substance use) are linked with school dropout, even after adjustment for sociodemographic characteristics, childhood adversities and prior mental disorders (Breslau et al., 2008, 2011; Kessler et al., 1995; Porche et al., 2011).
Thus, there is emerging evidence of an association between RSU and school dropout, but more research is needed to better understand the nature of this association. For many individuals, RSU represents only one part of a larger pattern of maladjustment during adolescence, in which externalising problems – and to some extent internalising problems – are also present (Chassin et al., 2013; Dennermalm et al., 2022; Heradstveit et al., 2018, 2019). While internalising problems include emotional and peer problems, externalising problems are characterised by conduct problems, as well as problems with hyperactivity and impulsivity (Achenbach et al., 2016; Goodman et al., 2010). It should be noted that externalising problems appear to be a much stronger correlate of adolescent RSU compared with internalising problems (Heradstveit et al., 2018; Pedersen et al., 2018). Correspondingly, a recent review of the literature specified that RSU and externalising problems are strongly associated with school dropout, while internalising problems also have an association with subsequent school dropout, but with smaller magnitude (Esch et al., 2014). In addition, internalising problems often develop as a consequence of school dropout (Esch et al., 2014). These findings are aligned with a recent study that reported a consistent but small association between symptoms of depression and school dropout in late adolescence (Askeland et al., 2022), and which also noted that co-occurring externalising problems amplified the association between depression and school dropout and vice versa. Importantly, a Norwegian longitudinal study reported that youth with externalising problems had a 38%–40% lower probability of completing upper secondary school compared to their healthy peers, whereas the corresponding number was 26%–29% for youth with internalising problems (von Simson et al., 2022). This study did, however, not include RSU in their analyses.
Given the high co-occurrence between RSU and internalising and externalising mental health problems (Chassin et al., 2013; Heradstveit et al., 2019; Skogen et al., 2014), it seems particularly important to include these factors in the analytic approach. A recent longitudinal study from Australia reported that a considerable proportion of the association between adolescent substance use and subsequent school dropout was explained by shared effects with parental education and childhood externalising problems (Davis et al., 2022). Similarly, a longitudinal study from the United States reported that psychiatric and substance use disorders predicted school dropout, but the unique association was restricted to externalising mental disorders (i.e., conduct disorders and attention-deficit/hyperactivity disorders) (Breslau et al., 2011). More research is needed to further disentangle the unique and shared effects of RSU and externalising and internalising mental health problems on school dropout.
The primary purpose of this paper was to assess to what extent RSU acts as an important risk factor for school dropout in a prospective study of Norwegian adolescents, as well as how externalising and internalising mental health problems influenced this association. The study utilised a unique linkage between a large population-based survey with baseline data on substance use, and an administrative registry with data on school dropout. As sex and socioeconomic status are associated with both RSU and school dropout (Askeland et al., 2022; Cairns et al., 1989), these variables were included as covariates in our analyses. Age at measurement of RSU is also important, as early substance use generally is less normative compared with substance use during later adolescence (Skogen et al., 2014), and thus may act as a more potent predictor of adverse educational outcomes. Therefore, age was accounted for in all analyses. Based on existing knowledge, we hypothesised that there is a positive association between RSU and school dropout. We also hypothesised that this association would be more attenuated by accounting for co-occurring externalising problems than co-occurring internalising problems.
Methods and materials
Procedure
Data stem from a linkage between (1) the youth@hordaland-survey, which was conducted during spring 2012 in Hordaland County, Western Norway, and (2) information from the official Norwegian educational database (NUDB) from 2012 to 2019.
All adolescents born during 1993–1995 were invited to participate in the youth@hordaland-survey. Adolescents attending school were invited via their school email address, while those not in school were invited by postal mail. The main aim of the survey was to gather information on mental health and health service use among adolescents. One school hour was allocated to complete the questionnaire, and school personnel were present during the data collection, while survey members were available on telephone.
Sample
Of the 19,430 adolescents invited to participate, 10,257 agreed and filled out the questionnaire, yielding a participation rate of 52.8%, and comprising the total sample for the present study. Of these, 9166 consented to registry linkage, and 9157 participants with valid information on the educational variables were included in the present study. The subsample that consented to registry linkage was similar to the total sample on sex and age distribution and self-reported sociodemographic variables (Nilsen et al., 2020). It should be noted that the Norwegian context of youth substance use is somewhat different from many other Western countries, in the respect that Norway has a restrictive alcohol policy (Enstad et al., 2019). In addition, drug possession and consumption are illegal in Norway and these regulations are enforced (EMCDDA, 2017).
School dropout
Norwegian students normally finish the general tracks in upper secondary school in three years and the vocational tracks in three or four years, depending on the programme they follow. Completion of upper secondary school was defined according to the national definition used by Statistics Norway (Statistics Norway, 2020) as graduation within five years of beginning upper secondary school for students enrolled in general tracks and within six years for students enrolled in vocational tracks. When a participant had not completed upper secondary school within five/six years, this was defined as school dropout. For more details of our operationalising of this variable, see Askeland et al. (2022).
Instruments
Demographic information
Information about sex and date of birth was provided by the personal identity number in the Norwegian National Population Register. We calculated age by the time interval between the date of birth and date of participation. Three groups were created: 16-year-olds (age range = 16–16.99 years); 17-year-olds (age range = 17–17.99 years); and 18–19-year-olds (age range = 18–19.34 years). Socioeconomic status included three variables. Two variables of registry-based parental educational status were retrieved from the NUDB, namely mothers’ and fathers’ highest education when the participants aged were 16 years. These variables were categorised into “lower”, “upper secondary” and “higher” in accordance with levels retrieved from the International Standard Classification of Education (ISCED) 2011 (UNESCO Institute for Statistics, 2012). A variable for self-reported perceived economic well-being was retrieved from the youth@hordaland-survey, and categorised into “poorer than others”, “equal to others” and “better than others”.
Risky substance use
RSU was measured as part of the youth@hordaland-survey, with five variables that are thoroughly described in a previous article (Heradstveit et al., 2019). We used four indicators of RSU, that included the following: (1) illicit drug use; (2) high-level alcohol consumption; (3) frequent alcohol intoxication; (4) a positive CRAFFT-score; and (5) a composite score of the total number of indicators of RSU, using each of the items 1–4 as indicators.
Illicit drug use was based on a single item: “Have you ever tried hash, marijuana or other narcotic substances?” (Yes/No). High-level alcohol consumption was based on a variable that added up five items measuring how many glasses of beer, cider, wine, spirits and illegally distilled spirits the adolescents usually consumed during a period of 14 days. The variable separated those above the 80th sex-specific percentile on alcohol consumption among adolescents with any usual alcohol consumption, from those below. Frequent alcohol intoxication was based on a single item: “Have you ever consumed so much alcohol that you were clearly intoxicated (drunk)?” The original item had five categories ranging from “No, never” to “Yes, more than 10 times”. Frequent alcohol intoxication was defined as drinking so much that one was clearly intoxicated more than 10 times, and on this basis, a dichotomous variable was created. Positive CRAFFT score was based on the six-item, validated CRAFFT scale (Knight et al., 2002). CRAFFT represents the key words of the six items included in the scale, which is Car, Relax, Alone, Forget, Friends, Trouble. This scale has been designed to identify potential alcohol-and drug-related problems among adolescents and has been demonstrated to have acceptable sensitivity and specificity at a cut-off value of ≥2 (Dhalla et al., 2011; Knight et al., 2002; Skogen et al., 2013). A dichotomous variable separating those above and below this CRAFFT cut-off value (≥2) was calculated. Finally, an ordinal variable for level of total symptoms of RSU was constructed (ranging from 0 to 4), in which we summed up the number of positive scores on lifetime illicit drug use, high-level alcohol consumption, frequent alcohol intoxication and positive CRAFFT score.
Externalising and internalising problems
Externalising and internalising mental health problems were measured by the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997). The SDQ is a screening questionnaire consisting of 25 items that describe positive and negative characteristics of children and youth within the following five subscales: (1) emotional problems; (2) conduct problems; (3) hyperactivity/inattention problems; (4) peer/relationship problems; and (5) pro-social behaviour (not used in the current study). Each item is scored on a 3-point scale – not true, somewhat true and certainly true – with total subscale scores each in the range of 0–10. The SDQ instrument has been validated and demonstrates good psychometric qualities (Muris et al., 2003). The use of broader internalising and externalising scales from the SDQ is found to be acceptable in low-risk samples (Goodman et al., 2010), has a good fit with the included subscales (Van Roy et al., 2008) and the scales are relatively “uncontaminated” by one another (Goodman & Scott, 1999). Accordingly, an externalising problems scale was constructed by merging the subscales of conduct problems and hyperactivity/inattention problems, while an internalising problems scale was constructed by merging the subscales of emotional problems and peer/relationship problems.
In our sample, both the Cronbach's α and the McDonalds’ omega coefficients for the internal consistency were 0.81 for the externalising problem scale and 0.82 for the internalising problems scale. For the regression analyses, we used the continuous scales for externalising problems (range = 0–18, mean = 5.37, median = 5, interquartile range = 3–7) and internalising problems (range = 0–10, mean = 4.80, median = 4, interquartile range = 2–7).
Statistical analysis
First, we provided descriptive statistics for the sociodemographic variables, school dropout and RSU for the total sample, as well as stratified by age groups. We used chi-square tests to indicate significant differences across the age groups.
Second, unadjusted rates of school dropout were visualised in margin plots across number of indicators of RSU (Figure 1). The figure was stratified by age due to the significant interaction between RSU and age on the association with school dropout.
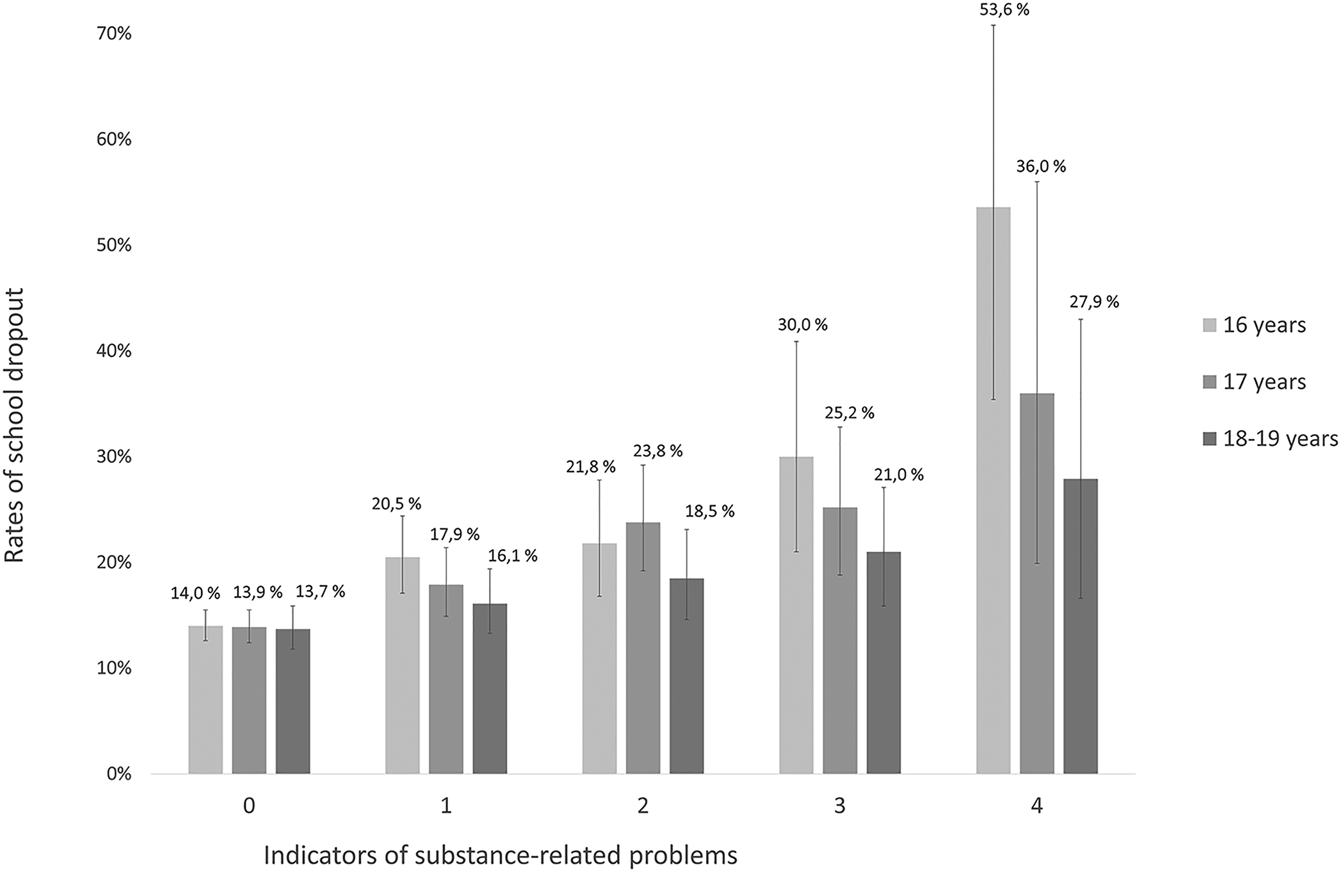
Unadjusted rates of school dropout across combined indicators of risky substance use across age groups (n = 9157).
Third, we used logistic regression analyses to investigate the associations between RSU and school dropout. In Model 1, these associations were adjusted for age, sex and SES. In Model 2, we added internalising problems and in Model 3 we added externalising problems to model 1. In Model 4, we added to Model 1 both internalising and externalising problems. Five separate analyses were conducted per model, one analysis per indicator of RSU, totalling 20 analyses.
In exploratory sensitivity analyses, we repeated the logistic regression analyses of associations between RSU and school dropout, adding the interaction terms between “RSU and age”. Thus, five interaction analyses were run, that included one analysis for each of the measures of RSU. In these analyses we only included sociodemographic variables as covariates. We found a significant association between age and frequent alcohol intoxication (p = .002) and between age and total symptoms of RSU (p = .004). On this basis, we conducted additional analyses for the association between frequent alcohol intoxication and school dropout, and for the association between total symptoms of RSU and school dropout, stratified by age groups.
All analyses were performed using Stata Statistical Software, version 16 (StataCorp, 2019).
Ethics
The study and the linkage to the Norwegian Education Database (NUDB) was approved by the Regional Committee for Medical and Health Research Ethics (REC) in Western Norway, and the Norwegian Centre for Research Data (NSD). In addition, a Data Protection Impact Assessment was conducted for the linkage. By Norwegian rules and regulations, adolescents aged 16 years and older can make decisions regarding their health, including participation in health studies. Thus, the adolescents gave consent to participate, while parents/guardians received written information about the study in advance.
Results
The sample
A total of 9157 individuals were included in our sample, with slightly more girls than boys, and with somewhat more individuals in the younger age groups (16–17-year-olds; 17–18-year-olds) compared with the oldest age group (18–19-year-olds) (mean age = 17.41) (Table 1). Boys had higher rates of school dropout (20.1%) compared with girls (14.1%), and these rates were similar across age groups. Sex and perceived economic well-being were also similar across age groups. Rates of RSU were markedly higher in the older age groups. Specifically, among 18–19-year-old adolescents, 51.1% had at least one indicator of RSU compared with 33.6% of 17–18-year-olds and 26.0% of 16–17-year-olds.
Descriptive characteristics of the sample (n = 9157). a
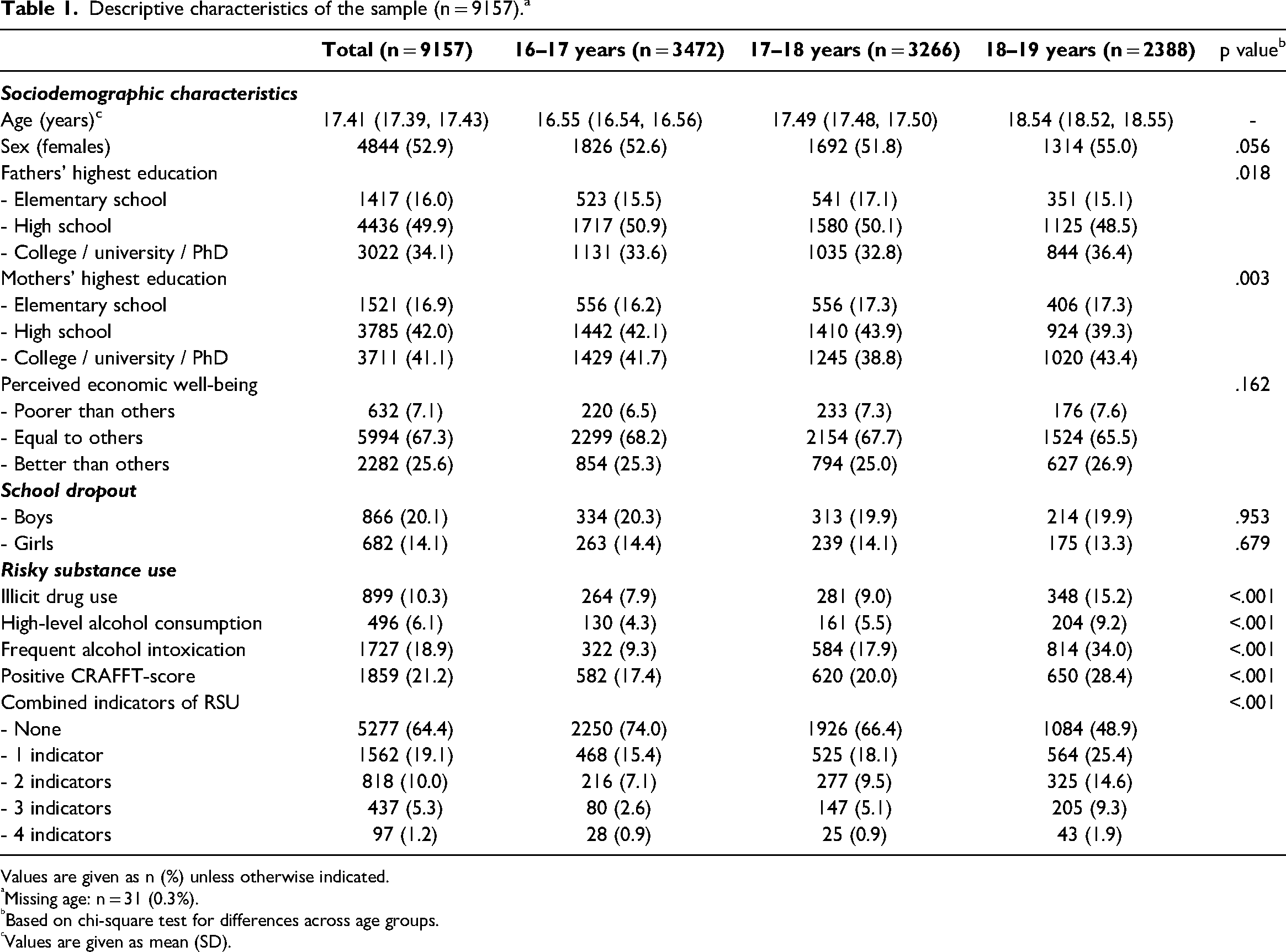
Values are given as n (%) unless otherwise indicated.
Missing age: n = 31 (0.3%).
Based on chi-square test for differences across age groups.
Values are given as mean (SD).
Risky substance use and school dropout
Figure 1 shows that rates of school dropout increased with increasing number of indicators of RSU. While this pattern was seen across the age groups, it was most robust in the youngest age group.
As shown in Table 2, all single indicators of RSU were associated with school dropout in Model 1 (adjusted odds ratios [AOR] = 1.26–2.25). Internalising problems (Model 2) only slightly attenuated these associations. The adjustment for externalising problems (Model 3) attenuated these associations considerably. However, all single indicators of RSU (except frequent alcohol intoxication) remained positively associated with school dropout in Model 4, i.e., after the full adjustment of sociodemographic variables and mental health problems.
Associations between symptoms of RSU and school dropout (n = 9157).
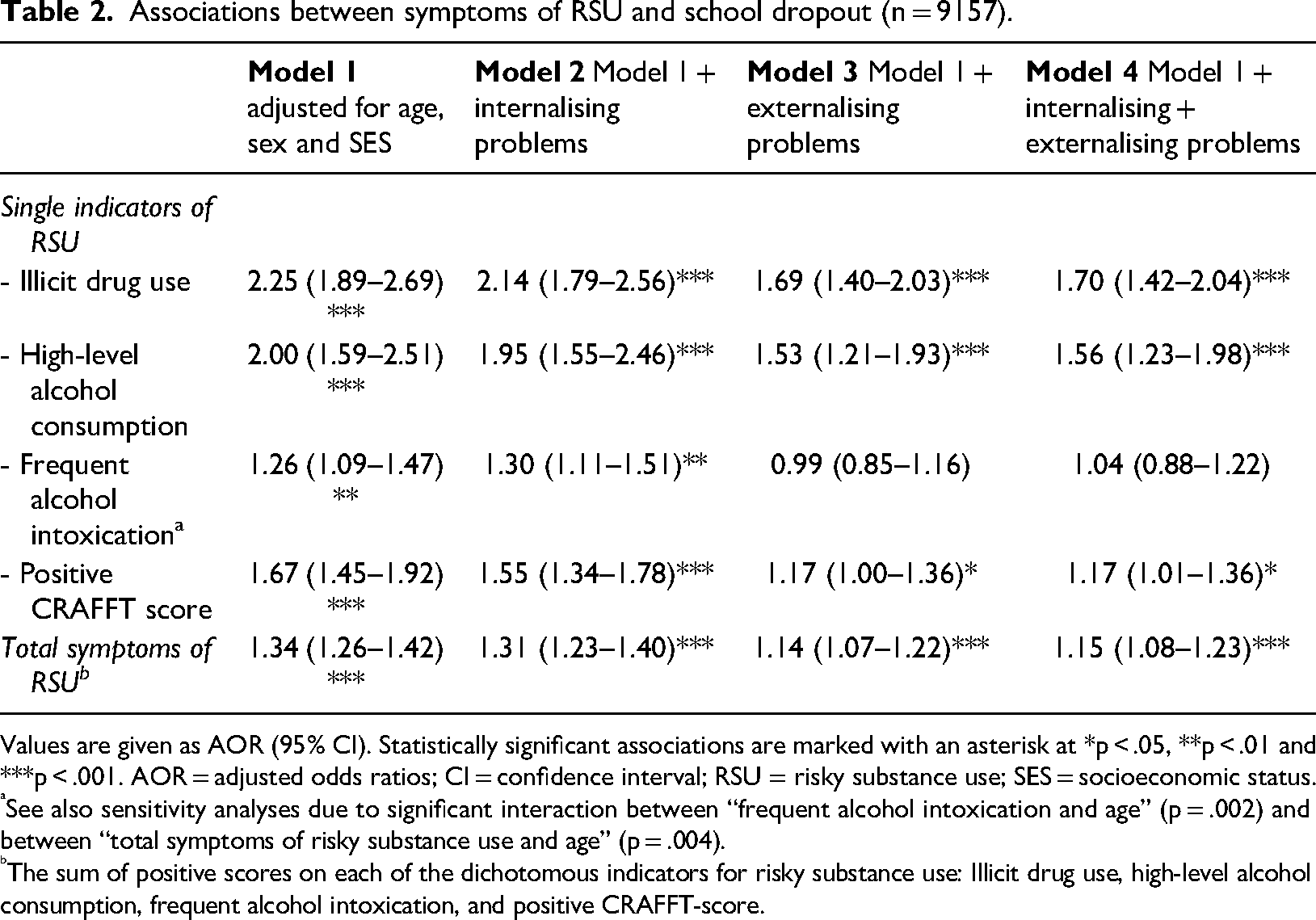
Values are given as AOR (95% CI). Statistically significant associations are marked with an asterisk at *p < .05, **p < .01 and ***p < .001. AOR = adjusted odds ratios; CI = confidence interval; RSU = risky substance use; SES = socioeconomic status.
See also sensitivity analyses due to significant interaction between “frequent alcohol intoxication and age” (p = .002) and between “total symptoms of risky substance use and age” (p = .004).
The sum of positive scores on each of the dichotomous indicators for risky substance use: Illicit drug use, high-level alcohol consumption, frequent alcohol intoxication, and positive CRAFFT-score.
The analyses of total indicators of RSU showed positive associations between all levels of RSU and school dropout in Model 1 (AOR = 1.46–2.42). This association was only slightly attenuated after the adjustment for internalising problems (Model 2). The adjustment for externalising problems robustly attenuated the association (Model 3), but the association remained statistically significant even in the fully adjusted model (Model 4: AOR = 1.14, 95% confidence interval [CI] = 1.06–1.23).
Sensitivity analyses showed that frequent alcohol intoxication was uniquely associated with school dropout for the youngest age group (16–17-year-olds; AOR = 1.51, 95% CI = 1.12–2.05, p < .01), but not for the other age groups (p values = .33–.67). Total symptoms of RSU were uniquely associated with school dropout for 16–17-year-olds (AOR = 1.28, 95% CI = 1.14–1.45) and 17–18-year-olds (AOR = 1.13, 95% CI = 1.01–1.27), but not for the oldest age group (18–19-year-olds; p = .25).
Discussion
The main finding of the present prospective, registry-linked survey study was that RSU predicted school dropout among Norwegian adolescents in upper secondary school. All measures (except frequent alcohol intoxication) also demonstrated unique associations with school dropout after accounting for externalising and internalising mental health problems. Sensitivity analyses revealed that the associations between RSU and school dropout were most robust for the youngest students. Thus, for the youngest age group, all measures of RSU were associated with school dropout.
Our findings support several previous contributions that have found that RSU prospectively predicts school dropout (Breslau et al., 2008, 2011; Esch et al., 2014; Grant et al., 2012; Horwood et al., 2010; Kelly et al., 2015; Kessler et al., 1995; Porche et al., 2011; Rose et al., 2014; Waldron et al., 2018). Our study lends support to previous studies that report associations between illicit drug use, such as cannabis use, and school dropout (Coffey & Patton, 2016; Horwood et al., 2010), as we found that lifetime illicit drug use was a consistent predictor for school dropout. The research literature is more inconclusive regarding whether alcohol use is also associated with school dropout. For example, a literature review noted that none of the included studies reported significant associations between alcohol consumption and school dropout (Esch et al., 2014). On the other hand, other studies have indeed reported associations between alcohol use and school dropout (Grant et al., 2012; Kelly et al., 2015; Rose et al., 2014; Waldron et al., 2018), and the present investigation lends support to these findings. However, whereas high-level alcohol consumption was a unique predictor for school dropout across the age groups, frequent alcohol intoxication was only uniquely associated with school dropout for the youngest age group.
A possible interpretation for the lack of a significant association between frequent alcohol intoxication and school dropout for the older students is that alcohol intoxication is much more common among the older students compared with the youngest age group. Hence, where it represents a less normative drinking pattern, it is also more likely to act as a risk factor. This interpretation is consistent with a recent Australian prospective study, which reported that they did not find effects of adolescent alcohol use on school dropout, noting that heavy drinking or experiencing alcohol problems in adolescence could be more predictive of early school dropout than any use (Davis et al., 2022). These findings also lend some support to previous studies that point to more detrimental outcomes related to early adolescent substance use compared with substance use later on (Karlsson et al., 2018).
Another explanation that is not mutually exclusive with the abovementioned explanation is related to a potential survival bias in our sample. Our findings suggest that approximately 50% of the youngest students (16–17-year-olds) with a maximum score on the total symptoms of RSU subsequently ended up dropping out of school. As the youth@hordaland-survey was primarily school-based, it is plausible that several individuals who would otherwise be included in the oldest age group of the sample did not participate due to having already dropped out of school. Thus, adolescents in the oldest age group, with very high scores on RSU, are likely not fully representative of the general adolescent population, but rather comprise individuals that have – to a larger degree than what is expected – survived a risk of school dropout. Therefore, as the youngest age group of our sample is least affected by this survival bias, it can be argued that the results related to this group provide a better representation of the true association between RSU and school dropout. In short, we would argue that the high rates of school dropout in the youngest age group of adolescents with high levels of RSU suggest a relatively strong association between adolescent RSU and school dropout.
Finally, our findings add to studies that report externalising problems to have relatively stronger associations with adolescent RSU compared with internalising problems (Heradstveit et al., 2018; Pedersen et al., 2018). Specifically, we found that a considerable proportion of the association between adolescent RSU and later school dropout could be explained by a shared effect between RSU and externalising problems. This was evident as the adjustment of externalising problems robustly attenuated the association between RSU and school dropout, whereas the shared effect with internalising problems was negligible. These findings should not be interpreted to indicate that internalising problems are unimportant as predictors of school dropout per se, but rather that the specific association between RSU and school dropout is strongly related to externalising, and not internalising, problems.
Implications
In short, our study underscores RSU as an important factor for school dropout, which highlights the need for specific efforts to reduce substance use and related problems among adolescents (Gohari et al., 2021). The present study indicates that symptoms of RSU in upper secondary school are uniquely related to dropout, regardless of co-occurring externalising and/or internalising problems. The association between RSU and school dropout was most robust among the youngest students. Despite the complexity of interpreting this age effect, our findings highlight the need for preventive interventions that aim to reduce substance use in the youngest age segment of upper secondary school. It should also be noted that as there was a substantial shared effect of RSU and externalising problems on school dropout, we encourage prevention efforts aimed at reducing student substance use to also address interventions that target co-occurring externalising problems. Future studies are encouraged to further disentangle the bi-directionality and temporal order of the associations between RSU, externalising and internalising problems, and school dropout.
Strengths and limitations
An important strength of the study is the use of a high-quality registry to define graduation from upper secondary school, as well as to specify level of parental education. This registry was linked to a large population-based survey that used a well-validated mental health measure (Goodman & Scott, 1999). The prospective design of the study, where symptoms of RSU were assessed while the adolescents were attending upper secondary education, is a further strength. Importantly, while the directionality between RSU and school engagement could have a bidirectional nature (Valkov, 2018), RSU was known to have preceded dropout in the present study.
There are also some limitations. Several studies have shown evidence for mental health problems preceding RSU, especially externalising problems (Heradstveit et al., 2018). However, there is also evidence of a bidirectional relationship between RSU and mental health problems in adolescence (Borges et al., 2018). Including measures of RSU and mental health problems at several time points would be needed to better establish the temporal order of these associations.
Although our data do not allow in-depth investigations on the extent to which the measured use of substances in our study is generalisable to the full population, our estimates of substance use is roughly similar to other investigations (Bye & Bretteville-Jensen, 2020; Sandøy, 2022). Our measure of “illicit drug use” included lifetime use of any illicit drugs, from cannabis on one side to heavier substances, such as cocaine or heroin, on the other. A more fine-grained measure of illicit drugs could have distinguished between type of drugs as well as frequency of use. However, such measures were not available in the survey. In addition, the relatively low frequency of adolescents who reported illicit drug use in our sample supports the usefulness of this broad categorisation.
Another important limitation concerns the generalisability of the results. With the relatively low response rate of 53%, it is possible that selective non-participation could be present. Although it was possible to complete the youth@hordaland questionnaire at any time during the data collection period, the survey was primarily school-based. It is therefore likely that those adolescents who did not participate in the survey were at higher risk of school dropout. It is also possible that some adolescents had already dropped out before the time of the survey, especially in the oldest age group. In the younger age groups, this survival bias is less likely to affect the results, as fewer students have had the possibility to drop out from school due to RSU. Thus, it is likely that the present study underestimates the association between RSU and school dropout for the oldest students, something that is important to consider when interpreting our findings. Desirability bias may be also a possibility, as the survey was completed in the presence of school personnel for many of the participants.
Conclusions
The present prospective and registry-linked survey study indicates that adolescent RSU is a strong predictor for school dropout, and that externalising problems contribute to a considerable proportion of this effect. Thus, adolescent RSU is an important issue to address in efforts to strengthen youth completion of upper secondary school. Prevention efforts to reduce student substance use could improve academic outcomes among upper secondary school students, and such efforts should also target co-occurring externalising problems. Such efforts may include interventions that aim to strengthen factors that have the potential to both protect against RSU and school dropout, for example related to increasing school connectedness, prosocial peer relations and goal orientation among vulnerable students. In this respect it should be noted that there is a need for more research on factors that promote school completion among students at risk of dropout.
Footnotes
Acknowledgements
We wish to thank the participants of the youth@hordaland-survey.
Availability of data and materials
Data and analysis code for this study are not available.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Western Norway Regional Health Authority (grant no. F-12136).