
Abstract
Aims:
(1) To describe the time trends of monthly cannabis use and (2) to analyse the association between the trends of monthly cannabis use and trends of different explanatory factors among adolescents in Estonia in 2003–2019.
Methods:
Nationally representative data from five waves of the cross-sectional European School Survey Project on Alcohol and Other Drugs (ESPAD) among 15–16-year-old adolescents (n = 11,348) in Estonia were analysed. Tests for trends were used to assess significant changes in monthly cannabis use and explanatory variables over time. Logistic regression analysis was used to analyse the association between monthly cannabis use and perceived easiness of getting cannabis, perceived health risk of cannabis use, parental factors, risk behaviours, and leisure time activities. The model included interaction terms between the study year and each explanatory variable. Gender-adjusted odds ratios (OR) with 95% confidence intervals (CI) were calculated.
Results:
Monthly cannabis use increased from 5.3% in 2003 to 7.7% in 2015 and thereafter decreased to 6.6% in 2019 among adolescents in Estonia (P = 0.007). The association between monthly cannabis use and alcohol use was significant over the study period and the interaction of alcohol use with study year indicated significantly increased effect of alcohol use over time (P = 0.038). The association between monthly cannabis use and perceived easiness of obtaining cannabis, perceived low health risk from cannabis use and smoking was significant, but remained unchanged over the study period. The relationship between monthly cannabis use and low parental control was significant in two last study years but did not show any changes over time.
Conclusions:
The findings of this study demonstrate the need for the implementation of multi-component substance use prevention programmes among adolescents in Estonia that also pay attention to the factors associated with the cannabis use.
Cannabis use during adolescence has serious implications for the developing brain, thereby requiring the continued attention of public health authorities (Debenham et al., 2019; Meier et al., 2012; Munk et al., 2017; Volkow et al., 2014). Moreover, the effect of cannabis may be more harmful due to the high concentration of neurotoxic tetrahydrocannabinol that has been found in cannabis recently (European Monitoring Centre for Drugs and Drug Addiction, 2020a; Rømer Thomsen et al., 2019). Besides the neurological and cerebrovascular effects of cannabis use in the early years adolescence, it may also lead to misuse and dependence of other addictive substances (Agrawal et al., 2008; Agrawal et al., 2004; Lynskey & Fergusson, 1995) and mental health risks in adulthood (Degenhardt et al., 2013; Foti et al., 2010; Mustonen et al., 2018).
Substance-specific epidemiological evidence contributes towards the estimation of the contribution of cannabis use to the burden of disease and related outcomes in society (Danielsson et al., 2014; Lachenmeier & Rehm, 2015; Lim et al., 2012). Cannabis is the most frequently used illicit drug among adolescents in European countries (ESPAD Group, 2020b) as well as in other developed countries around the world, such as the USA (National Institute on Drug Abuse, 2020), Canada (Government of Canada, 2017), and Australia (Australian Institute of Health and Welfare, 2019). According to the European School Survey Project on Alcohol and Other Drugs (ESPAD), the average prevalence of monthly cannabis use among adolescents in the participating countries increased from 7.0% in 2003 to 7.6% in 2011, and thereafter decreased slightly to 7.4% in 2019 (ESPAD Group, 2020b). These prevalence rates differ between countries greatly, and the reasons for that are unclear. While the lifetime cannabis use among Estonian adolescents was somewhat higher than the ESPAD average, the prevalence of monthly cannabis use was comparable to the ESPAD average in 2019. Compared to neighbouring countries, monthly cannabis use in Estonia was similar to Lithuania but lower than in Latvia; however, it was two times higher than in Finland and Sweden (ESPAD Group, 2020b).
Research evidence has shown that cannabis use among adolescents is associated with different factors such as personal and parental factors, other risk behaviours and leisure time activities. Considering personal factors, perceived easiness of obtaining cannabis as well as low perceived health risk from cannabis use, has previously been associated with higher cannabis use among adolescents (Burdzovic Andreas, 2019; Burdzovic Andreas & Bretteville-Jensen, 2017; Karlsson et al., 2018; Agaku et al., 2015). Furthermore, higher levels of parental monitoring have been found to be associated with lower levels of cannabis use among adolescents (Burdzovic Andreas & Bretteville-Jensen, 2017; Gaete & Araya, 2017). On the other hand, permissive parenting methods may offer even more protection against adolescents’ substance use than authoritative parenting style (Calafat et al., 2014).
In addition, cannabis use among adolescents is found to be strongly associated with other risk behaviours such as the use of tobacco and nicotine products in general (Raitasalo et al., 2020), alcohol consumption (Burdzovic Andreas et al., 2016) and leisure time activities (Kristjansson et al., 2010). The Icelandic model has shown that organised participation in leisure time activities may confer some protection against adolescent substance use (Kristjansson et al., 2010). Therefore, it is essential to have evidence-based information about adolescents’ cannabis use and associated factors to understand how these factors are associated with the trend of monthly cannabis use, i.e., active cannabis use. A better understanding of the factors and trends will lead to stronger prevention programmes that focus on adolescents’ cannabis use. To our knowledge, this is the first in-depth analysis of Estonian adolescents’ cannabis use and associated factors over a longer time period.
The aims of this study were (1) to assess the time trends of monthly cannabis use and potential explanatory factors and (2) to analyse the association between monthly cannabis use and explanatory factors, and whether this relationship has changed over time.
Methods
Study population and design
This study used individual-level data of 15–16-year-old adolescents from the European School Survey Project on Alcohol and Other Drugs (ESPAD), which is a cross-sectional survey that has been performed every four years since 1995 in European countries.
Proportionate stratified sampling according to the geographical regions (NUTS3 level) was used and from each sampled school one 8th and one 9th grade was sampled. Thus, the final unit in the sampling procedure was school class. Participation rates of schools in Estonia have ranged from 84% (2019) to more than 90% over the study period. The parents were informed of the inclusion of their children in the survey sample, and passive informed consent was issued. Participation in the survey was anonymous and voluntary.
Throughout all the survey years, self-administered paper and pencil questionnaires in Estonian and Russian language have been used. Research assistants, pre-trained according to the standard ESPAD instructions, were responsible for the data collection in a classroom. After completing the questionnaire, students sealed it into an envelope to preserve anonymity. The completed questionnaires were checked after data entry and were centrally cleaned by the Swedish Council for Information on Alcohol and Other Drugs until 2015, after that this was done by the National Research Council of Italy (ESPAD Group, 2020b).
This study used secondary data from the years 2003, 2007, 2011, 2015, and 2019 in Estonia. In total, the study population consisted of 11,348 adolescents: 5833 boys (51.4%) and 5515 girls (48.6%). The data from study years 1995 and 1999 were omitted from the analysis as the questionnaires did not include the questions concerning monthly cannabis use in these years in Estonia.
Study variables
Outcome variable
Monthly cannabis use as the main outcome variable was measured by asking “On how many occasions (if any) have you used cannabis during the last 30 days?” with seven response alternatives, ranging from “never” to “40 times or more”. The responses were dichotomised to “yes” (at least once) and “no” (never).
Explanatory variables
All explanatory variables were dichotomised to simplify the interpretation of the results. However, dichotomising the explanatory variables could lead to model underestimation and therefore, the results should be interpreted as minimum estimates.
Personal factors
Perceived availability of cannabis was assessed by asking the question: “How difficult do you think it would be for you to get cannabis if you wanted?” (1 = impossible, 2 = very difficult, 3 = fairly difficult, 4 = fairly easy, 5 = very easy, 6 = do not know). Individuals who responded “do not know” were coded as missing. The responses “fairly easy” or “very easy” were coded as 1 (Easiness of getting cannabis), all the other responses were coded as 0.
Perceived health risk of cannabis use was assessed by asking: “How much do you think people risk harming themselves (physically or in other ways), if they try cannabis once or twice?” (1 = no risk, 2 = slight risk, 3 = moderate risk, 4 = great risk, 5 = do not know). Individuals who responded “do not know” were coded as missing. The responses “no risk” or “slight risk” were coded as 1 (Low health risk perception), all the other responses were coded as 0.
Parental factors
Parental control was assessed with the question: “Do your parents know where you spend Saturday nights?” (1 = know always, 2 = know quite often, 3 = know sometimes, 4 = usually do not know). Individuals who answered “know sometimes” or “usually do not know” were coded as 1 (Low parental control), all the other responses were coded as 0.
Parental rules set outside the home were measured by asking: “How often do your parent(s) set definite rules about what you can do outside the home?” (1 = almost always, 2 = often, 3 = sometimes, 4 = seldom, 5 = almost never). Individuals who answered “seldom” or “almost never” were coded as 1 (Lack of rules outside the home), all the other responses were coded as 0.
Behavioural risk factors
Alcohol consumption in last month was measured by asking: “On how many occasions (if any) have you had any alcoholic beverage to drink during the last 30 days?” with seven response alternatives, ranging from “never” to “40 times or more”. Individuals who answered “at least once or more often” were coded as 1 (Alcohol consumption), and “never” was coded as 0.
Daily smoking of cigarettes in last month was assessed by asking the question “How often have you smoked cigarettes (excluding e-cigarettes) during the last 30 days?” with seven response alternatives, ranging from “not at all” to “more than 20 cigarettes per day”. The responses “at least one per day” were coded as 1 (Daily smoking), “less than one cigarette per day” or “no at all” were coded as 0.
Leisure time activities
Active participation in sports was measured by asking: “How often (if at all) do you participate actively in sports, athletics or exercising?” (1 = never, 2 = a few times a year, 3 = once or twice a month, 4 = at least once a week, 5 = almost every day). The responses “almost every day” were coded as 1 (Sports activity), all the other responses were coded as 0.
Engagement in hobbies was measured by asking: “How often (if at all) do you do other hobbies (play an instrument, sing, draw, write)?” (1 = never, 2 = a few times a year, 3 = once or twice a month, 4 = at least once a week, 5 = almost every day). The responses “almost every day” were coded as 1 (Engagement in hobbies), all the other responses were coded as 0.
Control variable
Gender (boy, girl) was based on the question: “What is your sex?”
Statistical analysis
In the statistical analysis, a Cochran-Armitage test was used to assess the linear time trend in monthly cannabis use over the study period. A chi-square test was used to assess any changes in explanatory factors in 2003–2019.
The associations between monthly cannabis use and the explanatory factors were evaluated using a logistic regression analysis. The dependent variable was monthly cannabis use (yes vs. no), and the independent variables were: perceived availability of cannabis, perceived health risk from cannabis use, parental factors, risk behaviours, and leisure time activities. The model also included interaction terms between time as a categorical variable and each independent variable. Gender-adjusted odds ratios (OR) with 95% confidence intervals (CI) for each study year were calculated.
All questionnaires, which contained answers to the questions concerning monthly cannabis use, were used in the analysis (n = 11,348). The data were analysed using the statistical package Stata 14.2 (StataCorp LLC, 2016).
Results
Trends in monthly cannabis use and explanatory factors in 2003–2019
Monthly cannabis use increased from 5.3% in 2003 to 7.7% in 2015 and thereafter decreased to 6.6% in 2019 among adolescents in Estonia (P = 0.007) (Table 1).
The prevalence (%) of the explanatory and control variables among adolescents in Estonia, 2003–2019.
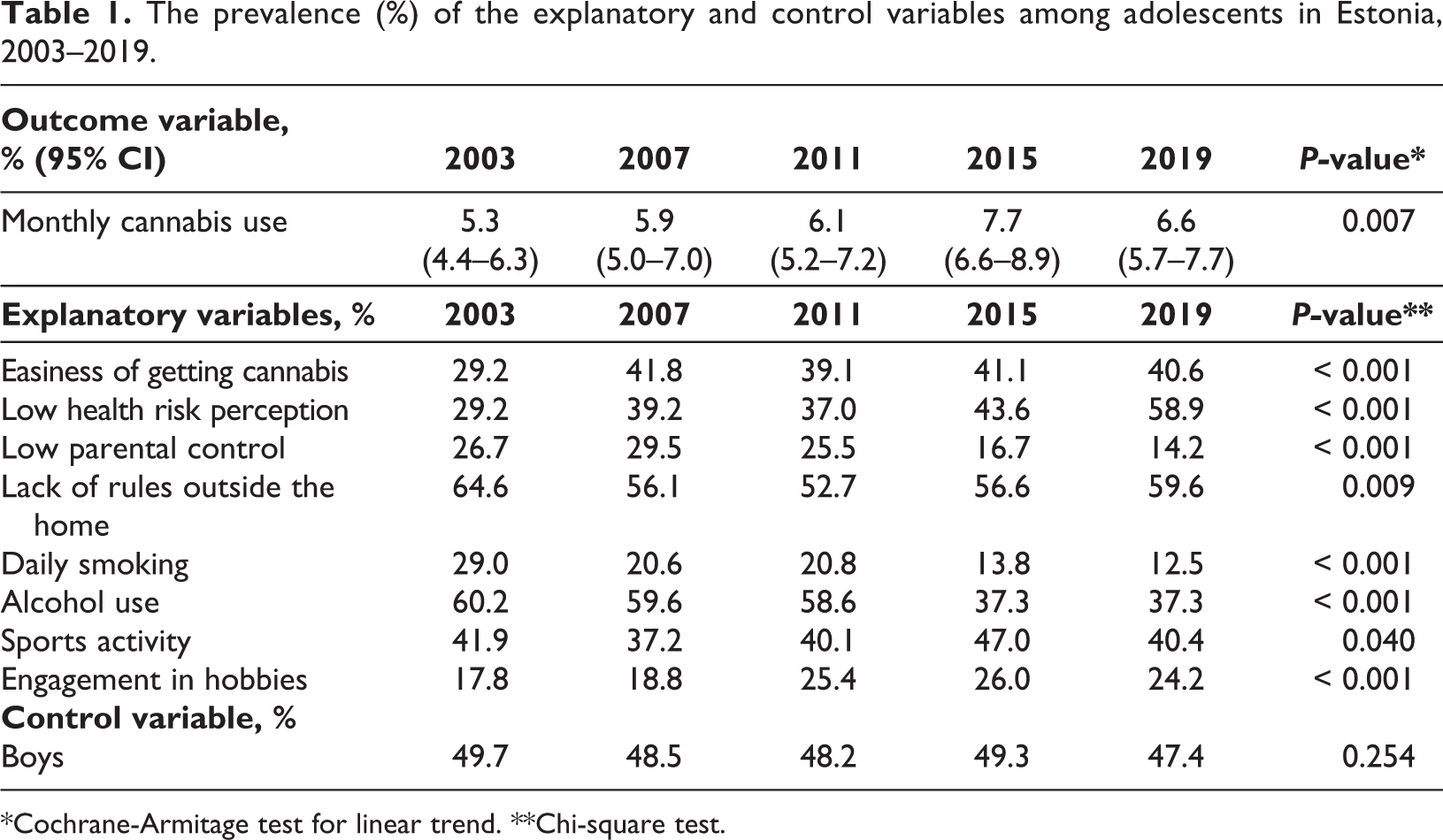
*Cochrane-Armitage test for linear trend. **Chi-square test.
Perceived easiness of getting cannabis and perceived low health risks from cannabis use increased over the study period. Compared to 2003, in 2019 there was significantly fewer adolescents reporting that their parents do not usually know about their whereabouts on Saturday nights, or that they had no clear rules while being out of the house.
Daily cigarette smoking declined from 29.0% to 12.5%, as did alcohol use, which declined from 60.2% to 37.3% between 2003 and 2019. Concerning leisure time activities, there appeared to be a statistically significant increase towards more frequent engagement in hobbies, while engagement in sports did not reveal a clear trend.
The associations between monthly cannabis use and various explanatory factors
Table 2 illustrates the relationships between monthly cannabis use and the explanatory factors in 2003–2019.
Logistic regression model* of the relationships between the explanatory variables and monthly cannabis use among adolescents in Estonia 2003–2019.
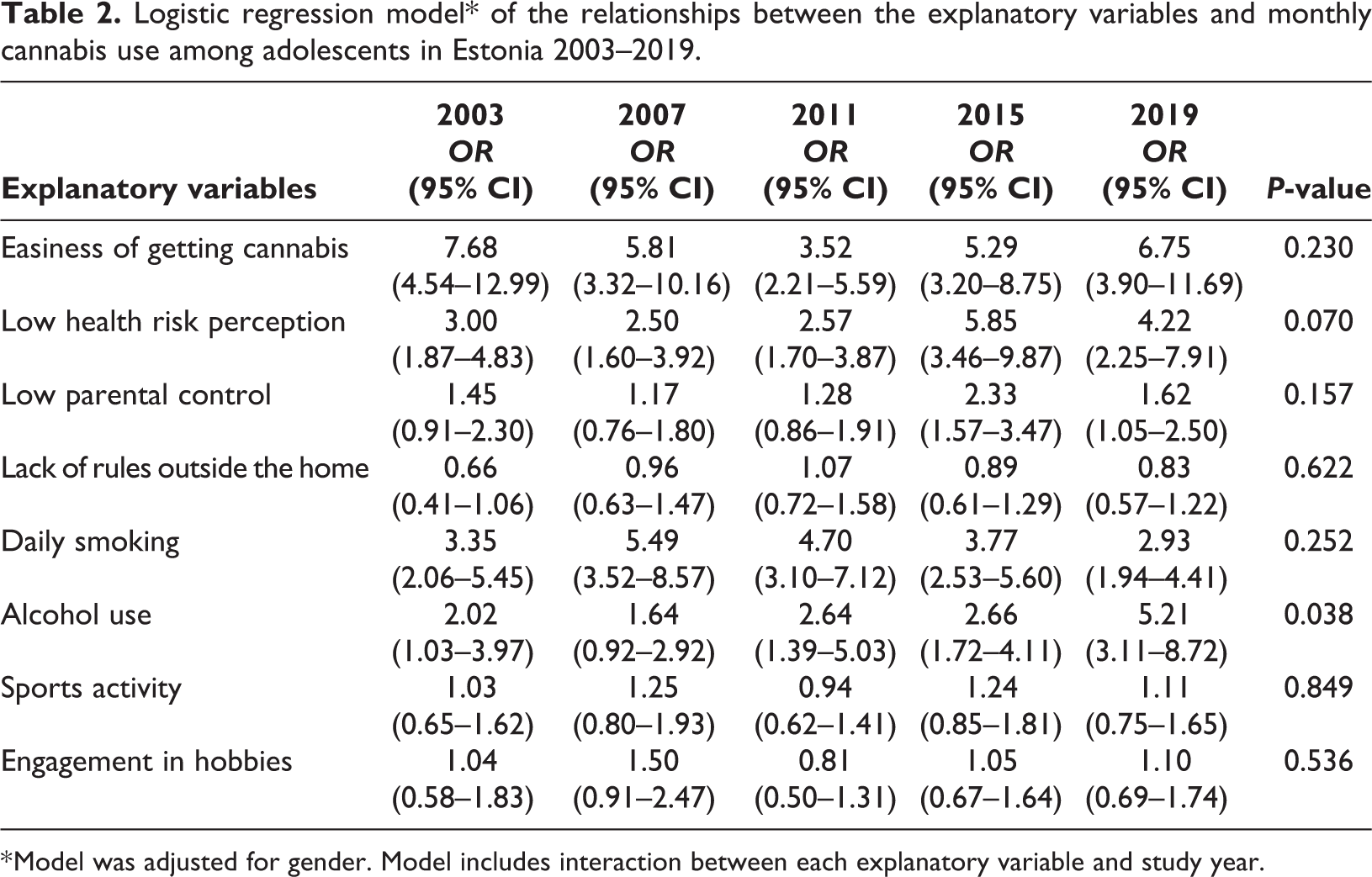
* Model was adjusted for gender. Model includes interaction between each explanatory variable and study year.
Perceived easiness of getting cannabis was significantly associated with monthly cannabis use in 2003–2019, and may increase the odds of monthly cannabis use by up to eight times. This association did not change throughout the study period (P = 0.230). Similarly, low perceived health risk from cannabis use may increase the odds of monthly cannabis use by up to six times and this association remained unchanged over time (P = 0.070).
Since 2015, low parental control was associated with higher probability of monthly cannabis use. There was no apparent association between lack of parental rules outside the home and monthly cannabis use. Daily cigarette smoking in last month increased the odds of monthly cannabis use significantly, and this relationship did not change over time. Alcohol use in last month increased the odds of monthly cannabis use by five times. In contrast to cigarette smoking, the association between alcohol use and monthly cannabis use became stronger over time, with the odds of monthly cannabis use doubling from 2003 to 2019 (P = 0.038). Neither participation in sports nor engagement in hobbies were associated with monthly cannabis use.
Discussion
This study described the time trends of monthly cannabis use and various explanatory factors (perceived easiness of getting cannabis, perceived health risks from cannabis use, parental factors, other risk behaviours and leisure time activities) and how these factors were related to the trends of monthly cannabis use among adolescents in Estonia in 2003–2019.
Trends in monthly cannabis use and explanatory factors in 2003–2019
Monthly cannabis use among adolescents in Estonia increased from 2003 to 2015 and thereafter slightly decreased in 2019. Whether this will remain the case in Estonia will become clear in the coming years. In 2019, the lowest prevalence of monthly cannabis use in European countries was in Iceland (2.1%) and Sweden (2.9%), and the highest in Italy (15.0%) and France (13.0%) (ESPAD Group, 2020a).
In Estonia, drug prevention education has been part of the basic school curriculum for more than ten years. In addition, several evidence-based intervention programs for schoolchildren have been implemented since 2013. (National Institute for Health Development, 2019). Implementing programmes that achieve the desired results is a time-consuming process; therefore, it is important that the programmes that have already been implemented are long-term and have secure funding. At the same time, several factors associated with monthly cannabis use have changed over time. Between 2003 and 2019, the proportion of Estonian adolescents who perceived getting cannabis to be easy increased significantly, whereas the ESPAD average has stabilised between 2007 and 2019 (ESPAD Group, 2020b).
In 2019, about one third of Estonian adolescents perceived getting cannabis to be easy, which was comparable to the ESPAD average in Latvia, Norway and Sweden, but was higher than in Lithuania (24%) and Finland (24%) (ESPAD Group, 2020b). Although the easiness of obtaining cannabis in Estonia was similar to Norway and Sweden, Estonia had considerably higher monthly cannabis use at the same time. This could mean that, besides availability, there might be some additional protective factors affecting adolescents’ cannabis use in Nordic countries. Thus, it is crucial to explore these protective factors which could be applied in prevention strategies in Estonia.
In addition, the increase in the perceived easiness of getting cannabis may be influenced by the expansion of adolescents’ social networks, which are easily accessed via smartphones (Friis Søgaard et al., 2019). Wider social circles with the help of social media allow for easier access to cannabis. Furthermore, with economic growth in the country children get more “pocket money”, while the price of cannabis has not changed by much (European Monitoring Centre for Drugs and Drug Addiction, 2020b; Vorobjov & Tamson, 2020).
Between 2003 and 2019, the prevalence of perceived low health risk from occasional cannabis use doubled among Estonian adolescents. A similar increase has been found among adolescents in Norway, Finland, Sweden and Lithuania between 2007 and 2015 (Burdzovic Andreas, 2019) as well as in Iceland between 1995 and 2015 (Arnarsson et al., 2018). Change in risk perception may be partly influenced due to the positive and harmless image of cannabis provided by medical or recreational cannabis legalisation supporters via the media (Hall & Morley, 2015; Lewis & Sznitman, 2019). In addition, adolescents may overperceive their peers’ approval towards cannabis and therefore lower their own negative perceptions (Vallentin-Holbech et al., 2017). This indicates a need for prevention efforts that aim to educate adolescents about the harmful nature of cannabis and to correct any misperceptions. In 2019, the prevalence of the perceived risk from cannabis use once or twice a month was 27% in Estonia, which was comparable with Finland and Latvia, but was higher than in Sweden and Lithuania (ESPAD Group, 2020a).
Factors associated with monthly cannabis use
Based on the adjusted logistic regression analysis, cannabis use among adolescents in Estonia was significantly associated with perceived easiness of getting cannabis, perceived low health risks from cannabis use, lack of parental rules, smoking and alcohol use.
The relationship between monthly cannabis use and perceived easiness of getting cannabis was strong and remained unchanged over time among adolescents in Estonia. The same relationship was found among adolescents in other European countries (Agaku et al., 2015). A similar relationship was found between a decline in alcohol use, as well as heavy episodic drinking, and alcohol availability, when it became more difficult to access for adolescents in Finland (Raitasalo et al., 2021; Raitasalo et al., 2018).
Perceiving low health risk from cannabis use once or twice a month was associated with a higher probability of monthly cannabis use throughout the study period among Estonian adolescents, which supports previous research findings in Norway and Sweden (Burdzovic Andreas, 2019; Burdzovic Andreas & Bretteville-Jensen, 2017; Karlsson et al., 2018). This shows that, despite different prevalence estimates, the factors associated with cannabis use can be similar across countries.
The results of this research are in line with previous findings that adolescents with more unsupervised time are more likely to use cannabis (Borawski et al., 2003). However, other research has found that a consciously permissive parenting style could have a protective effect on adolescents’ cannabis use (Calafat et al., 2014).
According to a survey among the Estonian adult population in 2018, the prevalence of lifetime cannabis use was 24% and past year cannabis use 3% (Reile et al., 2019). This is important, as with frequent cannabis use among adults it is likely that a higher number of parents with cannabis use experience, and their positive attitude towards cannabis, may encourage their offspring’s cannabis use (Kosty et al., 2015; O’Loughlin et al., 2019). On the other hand, parents who know their children well might recognise potential risk factors associated with cannabis or other substance use earlier. As parents play an important role in influencing their child’s substance use behaviour, it is vital to consider which factors should be addressed and how they can be implemented for parents (Miller et al., 2017).
Monthly cannabis use was significantly associated with other substance use in Estonia, which concurs with the findings in Norway and Canada (Burdzovic Andreas & Bretteville-Jensen, 2017; Sampasa-Kanyinga et al., 2018). With this in mind, providing guidance and recommendations for parents may contribute to the prevention of complex substance use by adolescents.
Monthly cannabis use was strongly associated with daily smoking over the study period. This relationship is in line with previous studies (Lemyre et al., 2019; Raitasalo et al., 2020). While the association between monthly cannabis use and smoking remained unchanged over time in Estonia, it was found that the relationship between experimentation with cannabis and smoking became weaker over time in Finland; the explanation being that experimentation with cannabis has increased among non-smokers recently (Raitasalo et al., 2020).
The relationship between monthly cannabis use and alcohol consumption was significant over the study years and the association became stronger over the years. Thus, in addition to other risk factors associated with monthly cannabis use, it is likely that alcohol is one of the main factors that may lead to an increase in cannabis use. There has been a public discourse about whether the decline in alcohol use by adolescents can be explained by the substitution of other substances, such as cannabis (Raitasalo et al., 2020), but Estonian data showed that the association between cannabis and alcohol use became stronger over time and it was not possible to distinguish a subgroup using only cannabis but not alcohol.
In the context of leisure time activities, no significant association was found between adolescents’ monthly cannabis use and their engagement in sports or hobbies. This finding contradicts the research results from a study in Iceland (Kristjansson et al., 2010) as well as one in Norway (Burdzovic Andreas & Bretteville-Jensen, 2017), where regular sports activities among adolescents, together with their families or in their communities, lowered adolescents’ cannabis use.
Limitations and strengths of the study
This survey has several limitations that could be considered. First, the ESPAD is a cross-sectional survey, therefore it was not possible to establish the causality of the associations between cannabis use and explanatory factors. Second, as data were collected by self-completed questionnaires, the prevalence of cannabis use may have been underestimated due to reporting bias related to the desire to conceal risk behaviour.
The strength of the ESPAD survey was that similar methodologies were used across the survey years and in different countries which allows for a long-term investigation of the trends within a country and comparisons between the participating countries. The large sample size and high response rate make the data representative of 15–16-year-old adolescents in Estonia.
Conclusions
Monthly cannabis use increased significantly from 2003 to 2015 and thereafter slightly decreased among adolescents in Estonia. Monthly cannabis use was associated with a number of factors including perceived easiness of getting cannabis, perceived low health risk from cannabis use, smoking and alcohol use throughout the study period and with low parental control in the later study years, only. The relationship between monthly cannabis use and alcohol use became significantly stronger over time.
The upward trend of monthly cannabis use among adolescents in Estonia highlights the need for expanding the pre-existing and ongoing substance use prevention programmes, and for the development of new programmes that take into consideration the factors associated with cannabis use. In this way, the programmes can aim to prevent or delay the start of cannabis use. Due to there being evidence that alcohol consumption may play a key role in the increase of cannabis use, it is recommended that prevention programmes take a multi-faceted and universal approach, in order to achieve the goals of reducing cannabis use among adolescents in Estonia.
Footnotes
Ethics approval
All ESPAD surveys in Estonia were administered in accordance with national ethical standards and with the Declaration of Helsinki. The ESPAD 2015 and 2019 surveys were confirmed with passive parental consent and approved by the Tallinn Medical Research Ethics Committee (decision no. 791, no 2525).
Acknowledgements
The authors thank the National Institute for Health Development for permission to use the data from the ESPAD survey in Estonia.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Estonian Research Council (grant number IUT34–17).