
Abstract
Keywords
Drug-related death (DRD) is a public health issue in Norway, as in many countries (Norwegian Institute of Public Health, 2021). In 2019, the European Union mortality number for reported drug-induced deaths was 5,769 (European Monitoring Centre for Drugs and Drug Addiction (EMCDDA), 2021), and the American equivalent, according to the Centers for Disease Control and Prevention (CDC), was 70,630. For the most part, drug-induced deaths/overdoses are sudden deaths from intoxication and can be classified as unnatural (CDC, 2021; EMCDDA, 2021). The overdose numbers are higher if DRD from other causes is included (Robertson et al., 2019). These causes of death may relate to behavioural disorders, mental illness and lifestyle-associated health risks, e.g., infections, accidents and violence (Amundsen, 2015). Subsequently, there is reason to believe that the number of bereaved following a DRD is significantly higher. The estimate that at least 10 persons are bereaved by each overdose fatality shows that a significant number of people are experiencing this type of loss (Dyregrov et al., 2000). In 2020, this figure was at least 706,300 persons in the United States, 57,690 in Europe and 3,240 in Norway. It has been documented that DRD may be a potentially traumatising experience with severe consequences for the bereaved, both socially and healthwise, ranging from reduced quality of life to early death, and leaving the bereaved at risk of prolonged grief, disabling grief reactions that do not diminish by time (Christiansen et al., 2020; De Leo et al., 2014; Dyregrov et al., 2003; Guy & Holloway, 2007; Li et al., 2005; Templeton, Valentine, et al., 2017; Titlestad & Dyregrov, 2022). Due to this severe risk, the health and welfare services must meet this group optimally.
Recent studies show that the bereaved encounter a complex and confusing service system and report not receiving assistance from the service system and experiencing associated stigmatisation due to the cause of death being illicit drug use (Cartwright, 2020, pp. 219–223; Dyregrov & Selseng, 2021; Feigelman et al., 2011; Templeton, Valentine, et al., 2017; Titlestad et al., 2019; Valentine et al., 2018; Walter et al., 2017). These findings, which correspond with the bereaved's own stories, can be elucidated in the light of associated stigma (Goffman, 2009; Mehta & Farina, 1988; Östman & Kjellin, 2002) and disenfranchised grief (Doka, 2002b). Discrimination in mental health care is widespread (Schulze, 2007; Thornicroft et al., 2007). McNeil (2021) outlined the stigmatisation of substance use from the perspectives of sociological, psychological, structural and social control processes. Stigma is shown in all of these areas, in line with Goffman's understanding, which implies discrediting, devaluating and stereotyping processes (Goffman, 2009; Link & Phelan, 2001, 2006). The associated stigma connected to drug death of bereaved persons may lead to disregard, according to research from the bereaved's perspective (McKell et al., 2018; Titlestad et al., 2019).
Disenfranchised grief is unacknowledged grief and has sociological, institutional, discursive and structural implications (Brabant, 2002). The loss is not recognised or acknowledged by others, and the one grieving is excluded from the regular social loss and bereavement processes in their communities. Some bereaved persons may also be self-disenfranchising because of the stigma attached to a next of kin with problems related to drugs, especially the use of illicit substances (da Silva et al., 2009; Kauffman, 2002; Titlestad et al., 2020).
A systematic review (Reime et al., 2022) found that there were no studies addressing the perspective of professional helpers on providing services to those bereaved as the result of a DRD. Given the number of those who are bereaved after drug death, who experience these losses as unnatural, and often had complicated and challenging relations with their next of kin when the latter was still alive, this gap in the research can be viewed as a missed recognition of persons who would benefit from psychosocial follow-up, as well as a shortfall in the knowledge of the health and welfare services (Lindeman et al., 2021; Orford et al., 2013; Templeton, McKell, et al., 2017; Valentine et al., 2016, 2018).
Norway has a service-intensive welfare state based on universal values and equal rights to health and social care for every citizen (Pasient- og brukerrettighetsloven [The Patient and User Rights Act], 2014; Vabo & Vabø, 2014, p. 11). Hasenfelt (cited in Vabo & Vabø, 2014, pp. 14–16) claims that “human service organisations”, such as public services, have people as their most important “raw material” because the services affect people directly. Public service logic and the public service ecosystem apply a framework for understanding public services and focus on value creation as the purpose of public services. Osborne et al. (2021, pp.668–670) address value creation processes as the purpose of public services and argues for an ecological approach to understanding complex organisational interactions and service delivery. The ecosystem offers concepts and an understanding of how public service delivery is integrated and interacts (Osborne et al., 2021). The service ecosystem comprises the organisational/institutional (macro-level), the service delivery system (meso-level) and the individual service user/stakeholder (micro-level).
In the Norwegian context, the emergency medical chain extends over three management levels: (1) pre-hospital services (including the medical emergency notification service, which communicates and coordinates resources); (2) the municipalities’ emergency room service; and (3) the specialist health service in hospitals, which includes emergency departments, and the ambulance service (Idland et al., 2019). The police, an independent authority under the Ministry of Justice and Public Security, is essential in unsettled medical emergencies and unnatural deaths. In emergencies, professionals on all levels are assumed to cooperate. The municipalities’ crisis teams are not a part of the emergency medical services. However, the national guidelines on psychosocial interventions in the event of crisis, accidents and disasters clearly state that “necessary psychosocial follow-up” must be included in these services to meet the justifiable requirement (Norwegian Directorate of Health, 2016, p. 20).
The municipalities are obligated to provide coordinated and comprehensive assistance to those bereaved after a sudden, unexpected death, which is primarily organised through multidisciplinary crisis response teams with specially trained professionals (Norwegian Directorate of Health, 2016).
The national policy document “The National guidelines of psychosocial interventions in the event of crisis, accidents and disasters” does not mention follow-up to bereavement from DRDs in particular. Still, follow-up after substance use deaths is perceived as this. Members of the crisis teams usually have their ordinary work elsewhere in the organisation, e.g., in mental health, child welfare or police services. A recent study has shown that first-responder professionals are essential in making referrals for further follow-up in the acute phase (1–4 weeks after death) in the municipalities (Løseth et al., 2022). In line with Kalkman (2020), the study also showed that establishing contact could be challenging because of the restricted timeframe and complex organisational premises, as in ordinary frontline work (Løseth et al., 2022). It is of vital importance to obtain more research-based knowledge from first-attending professional helpers in the acute phase in order to improve the services for psychosocial follow-up for those bereaved by a DRD.
This article examines what prevents and what facilitates the provision of professional assistance to persons bereaved after a DRD during the acute phase. Its aim is to broaden our knowledge, from the perspective of a municipality's first-responder services, of what prevents and what facilitates the provision of professional assistance to those bereaved as the result of DRD.
Method
Context of the study
This study is part of a larger project on drug death bereavement, the END project (Etterlatte ved Narkotikarelatert Død) initiated at Western Norway University of Applied Sciences in 2017. The primary purpose of the END project is to improve the life situation of persons bereaved following a DRD. This sub-study is based on the perspectives of first responder professionals.
Design
The article presents an analysis based on focus group interviews and demographic data collected in questionnaires. We have taken a flexible, inductive and empirically driven approach to researching the experience of the professional helpers who provide such assistance in the acute phase. We employed purposeful sampling and reflexive thematic analysis. Interaction among participants in focus groups can promote synergy and spontaneity, and participants can comment on, explain, share and discuss their opinions and experiences (Malterud, 2012, p. 18; Willig, 2013, pp. 30–31).
Context, recruitment and sample
In the spring of 2019, six target municipalities from the Norwegian Directorate of Health's nationwide pilot project to reduce overdose deaths were contacted orally and in writing. The leader of the END project informed the crisis team leaders and key personnel about the project and the selection criteria for the focus groups in terms of diversity in the number and demography of municipality citizens, including gender, professional education and occupational positions. They were asked to identify suitable candidates and form focus groups in collaboration with project interview teams. Suitable informants would occupy positions in the health and welfare services or non-governmental organisations (NGOs) through which they encountered persons bereaved by DRD. Potential participants were given an informed consent form stating that participation was entirely voluntary and consisted of one focus group interview of approximately 2.5 h and completing a questionnaire.
The main project recruited a total sample of 105 professional helpers and organised these into four groups of informants: (1) first responders and emergency personnel who were likely to be first on the scene; (2) professionals from the municipal services who generally met with bereaved persons; (3) representatives of various NGOs offering services to bereaved populations; and (4) the heads of various municipal services, such as emergency and outpatient rooms and mental health and addiction services. The informants represented municipal psychosocial crisis teams, the police, emergency medical services, NGOs, priests, undertakers, and health and welfare services. A total of 24 focus group interviews were conducted, i.e., one group for each of the four main groups in all six target municipalities.
The sample on which this article is based consisted of the 27 professional helpers from group one, i.e., the first-responder professional helpers in the acute phase. These 27 participants were organised into six groups: four groups of five participants, one group of six participants and one single interview because of drop-out (Table 1).
Characteristics of the interviewees in the focus groups (N = 27).
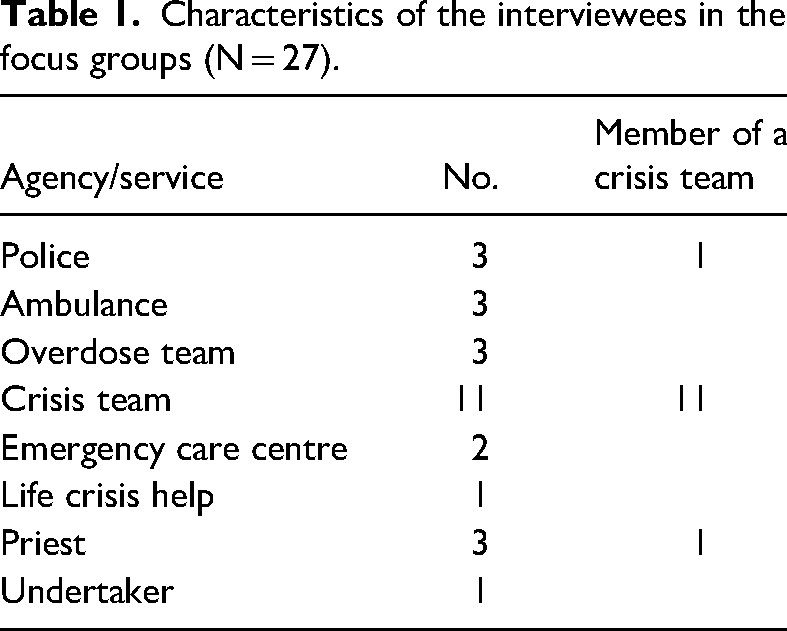
Eighteen of the participants were women (n = 18) and half as many were men (n = 9), which is a typical sex distribution among professional helpers. Four participants were aged 30–39 years, two were aged 40–49 years, eight were aged 50–59 years, and five were aged 60 years or older. Two-thirds of the participants had completed their education more than 15 years before the interview. In response to the question of how many bereaved persons they had met during the previous year (2018), seven participants replied either that they did not know or that they thought they had encountered none, 13 had met 1–5 bereaved persons, four had met 6–10 bereaved persons, and three had met 11–29 bereaved persons. One participant had lost one of their next of kin due to a DRD.
Data collection
The focus group interviews were conducted in person during the autumn of 2019 and spring of 2020 at or near the informant's workplace. Before the focus group interview, the informants completed a questionnaire on an e-pad or paper. These questions related to the participants’ background (e.g., age, education, time in position). Three teams conducted the interviews. Each team consisted of an experienced scientist as the focus group interviewer and an assistant as the co-moderator. The interview teams and the project leader prepared by discussing and reflecting on the interview method and how to secure the atmosphere and structure to co-create the best possible data collection. In order to feel confident in themselves, the team members practised their roles and how to use the technical equipment. A procedure guide ensured that the conduct of all interviews would be consistent with the information provided to the group – i.e., in terms of interview structure and management – and a theme guide ensured that the focus groups would focus on the same key themes. The teams conducted a pilot interview and modified the interview guide accordingly. The primary objective was to balance structure and openness so as to generate ideas and reflection, encourage insights, and manage the dynamics and interaction among group members (Tausch & Menold, 2016). The interview guide addressed the experience of community services in assisting the bereaved after a DRD, the barriers and critical conditions associated with helping these bereaved persons, the professional helpers’ thoughts regarding the assistance people needed after a bereavement due to a DRD, and their views on opportunities for cooperation with and help from the municipalities, social networks, NGOs and users, on forms of cooperation between public agencies, and on the use of key guides and management documents.
The suggested time frame for the focus group interviews was 1.5–2.5 h. A professional transcriber made audio tapes of the interviews and transcribed them verbatim. The quotations have been edited slightly to make the sentences complete and easier to read. After the interviews, the teams immediately summarised their impressions and reflected on them in writing. The first-responder/acute phase transcripts consisted of 174 pages of text. The first and third authors formed an interview team and conducted eight focus group interviews.
Analytical strategy
Because of the gap in what we know about professional follow-up on DRD (Reime et al., 2022), we used an inductive, empirically driven and flexible approach to explore the experience of first-responder personnel. We chose to apply a reflexive thematic approach to the analysis of the focus group interviews. This method emphasises the interaction among the purposefully sampled informants and provides favourable conditions for sharing, discussing and reflecting on opinions and experiences (Braun & Clarke, 2019b, pp. 4-16). Johnson and Christensen (2019, p. 299) define reflexivity as “continual self-awareness and critical self-reflection by the researcher on their assumptions, biases, predispositions, and actions, and their impact on the research situation and evolving interpretations”.
A bottom-up approach was used to search for themes throughout the whole of the dataset so as to identify repeated patterns of meaning by way of a coding process with a strong link to the data (Clarke et al., 2015). The first author reviewed the data several times to form an overall impression. The analysis and coding coincided in this iterative process. Initial thoughts about possible themes, coding schemes and meaning units for the dataset were noted and put into a table. Over the course of multiple re-readings, the authors began to develop an initial list of codes. The first author and third co-author read, discussed and re-read the table's content and the meaning units and began identifying possible themes based on the initial codes. The second co-author then read and discussed the coding units and main themes, and all of the authors discussed the findings and reached a consensus, generating the four main themes. Braun and Clarke (2019a) emphasise the researchers’ contribution to this reflective process. The authors’ backgrounds are significant in understanding the dynamics and utterances within the group interviews and their process of interpretation during the analysis, i.e., how their professional background and experience may have influenced their interpretative processes. We also discussed factors that may have influenced the interview process, such as differences between the interview teams. By occupation, the first author is a psychiatric nurse with an MA; the co-authors are a social worker with a PhD and a sociologist with a PhD. The researchers have long-term professional experience in health and welfare services and research into crisis and traumatic grief, addiction and mental health.
Ethical considerations
Before the sub-studies on the bereaved commenced, approvals were received from the Norwegian Regional Committees for Medical and Health Research Ethics (reference number 2017/2486) and the Norwegian Centre for Research Data (reference number 525501), which also approved the helper sub-study. Approval was also obtained from the Western Norway University of Applied Sciences.. All research and dissemination thereof comply with the Helsinki Declaration to ensure the highest ethical research standards, including participant anonymity and confidentiality. In accordance with the Norwegian Personal Data Act, the data have been managed in compliance with the General Data Protection Regulation, the Norwegian Regional Committees for Medical and Health Research Ethics instructions and Western Norway University of Applied Sciences regulations, and is securely stored.
Results
Our research identified three themes: (1) services are failing to initiate assistance; (2) bereaved persons who use drugs do not fit in; and (3) factors facilitating assistance. All themes and codes are interconnected and, to some degree, overlapping. We chose to code theme 2 as a separate category because bereaved persons who use illicit drugs were, to a large extent, perceived by our informants differently than other persons bereaved after a drug death. Some of the bereaved decline offers of psychosocial follow-up, or one bereaved person may decline on behalf of the whole family. As this is not a barrier within the services, it will be discussed under the heading of barriers relating to the informant's understanding of the phenomenon (Figure 1).
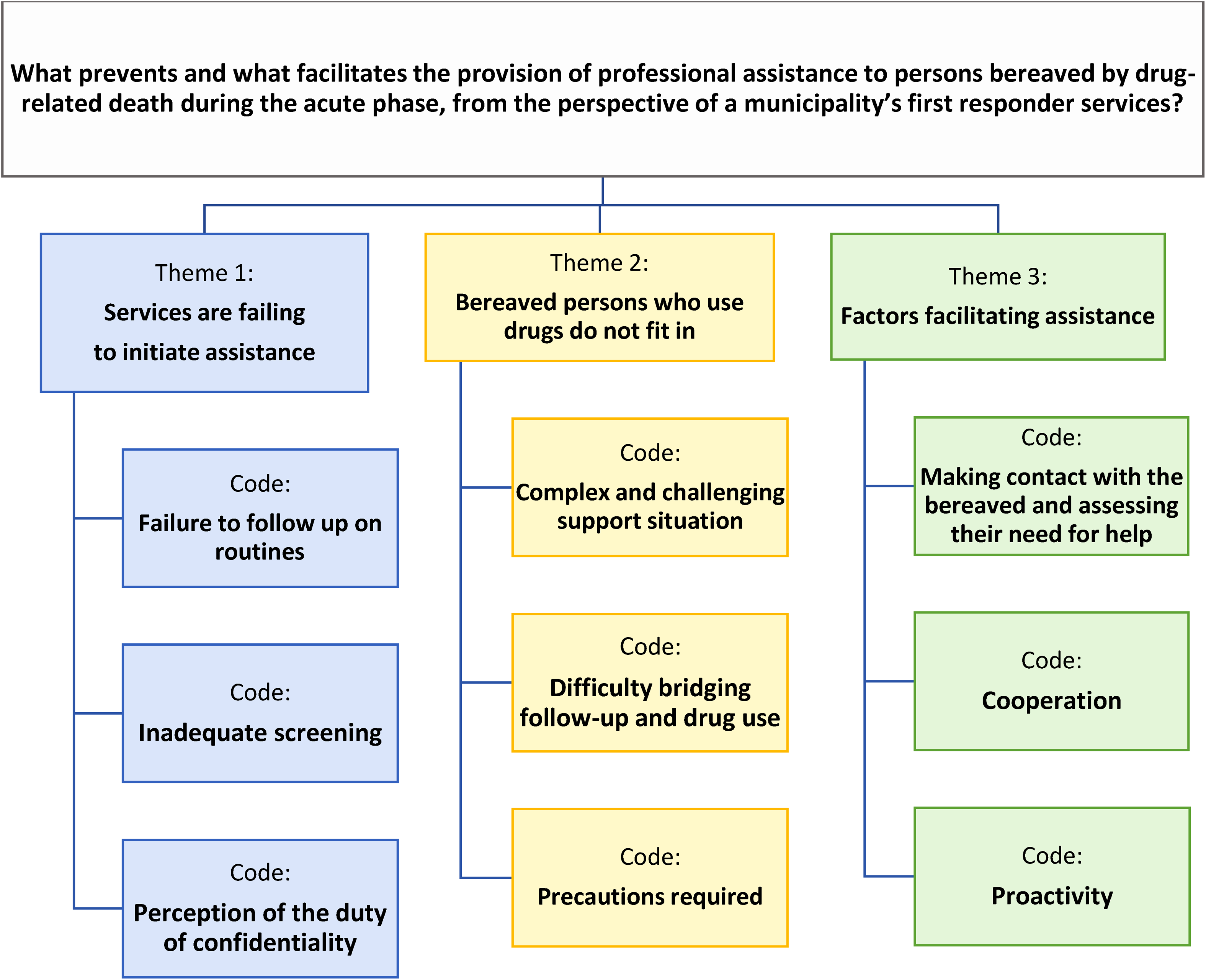
What prevents and what facilitates the provision of professional assistance to persons bereaved by drug-related death during the acute phase, from the perspective of a municipality's first responder services?
Services are failing to initiate help
A distinct pattern observed in the data material was the minimal psychosocial follow-up provided by the municipality services to the bereaved after a DRD. The bereaved were portrayed as a group that the municipality did not see and whose bereavement from sudden and unexpected death the municipality did not acknowledge. These findings can be sorted into three key categories: (1) failure to follow up on routines; (2) inadequate screening processes; and (3) first responders’ perceptions of the duty of confidentiality. These key categories are considered below.
Failure to follow up on routines
On an organisational level, most of our informants said that their municipality implemented the national guidelines in the event of a crisis, accident or disaster (Norwegian Directorate of Health, 2016). With regard to what prevents the provision of assistance, however, a central finding was that these guidelines may not be operationalised in DRD events. Regardless of organisational affiliation, most participants had not thought of the DRD-bereaved as suddenly bereaved. Even the three participants from the overdose teams who had the most experiences with DRD fatalities had not considered that these losses should be included in sudden death procedures for follow-up. Many were flustered and apologetic upon discovering the lack of reflection in their and their colleagues’ neglectful attitudes.
Very few of the first-responder professionals had routines for applying the national guidelines in DRD cases, despite the deaths being sudden, unnatural and unexpected by the bereaved. It was the experience of many of the participants that the appropriate services did not receive important information, and follow-up was hence not initiated. They shared and reflected upon possible reasons for this. For instance, one crisis team member noted the following: “We have routines that are very clear and simple, but which are not necessarily followed. And when they are not followed, it is often because they are not so practical and do not fit” (C1, ID1). In areas where the police delegate the duty of notification of death to a central security company, which passes the duty on to local services, such as members of the clergy or crisis teams, specific details of the death are often lacking. Informants from the police, who do not work within the health services, have assumed that when they alert the emergency centre, the municipality, as a single organisation, is informed and has internal routines for sharing information. Our findings suggest that this is not necessarily the case. In most of the focus groups, the informants shared their experiences and discussed how the municipality is a complex organisation with many divisions. When the focus group interviews were being conducted, it was not unusual for the informants to express surprise at the services that were available in their municipality. Information-sharing could be problematic between the various service divisions, a complexity that could lead to deaths not being included in the sudden and unnatural death category. In addition, the cause of death being drug-related is not always apparent for the helpers in the acute phase, and this kind of information may take some time before the bereaved individuals volunteer. The perception of a taboo around DRDs was perceived as further hindering the provision of an explanation for the cause of death, as well as playing a role in psychosocial follow-up not being initiated, as experienced by a member and leader of a crisis team in a larger city: What we experience in local crisis teamwork and emergency preparedness work … is difficult to ascertain whether it is drug-related death. We experience such a violent taboo on the subject … If you follow the bereaved over time in conversations, that story will often come out. (C6, ID24)
Inadequate screening
During the focus group interviews, most participants realised they had not been aware that this group should receive attention and be evaluated to determine whether there was a need for psychosocial follow-up. Except for those who worked in overdose teams, the informants had little previous understanding or knowledge of “the special death” and disenfranchisement of DRD-related bereavement (Doka, 2002b), and, thus, the DRD-bereaved had been overlooked with regard to referral for crisis services. This lack of competence led to an inadequate screening process because the emergency helpers (e.g., from police or ambulance workers) assessed an eventual need for psychosocial follow-up based on the immediate degree of the bereaved's acting out behaviour at the place of their loved one's death or when the bereaved was notified. This is illustrated by a quotation from a crisis team member: “What we experience is that the police or the emergency services contact us if they are with survivors with strong reactions, and if the survivors do not have strong reactions, then life goes on as usual” (C4, ID21). Our findings also showed that these first responders might evaluate the need to notify and offer psychosocial follow-up based on the perceived quality of the relationship between the deceased and the next of kin. Previous encounters and information on the family situation also affected the evaluation of needs problematised by this crisis team member: And then I called the police the next day to ask, are there no bereaved? The police said, no, we have checked it; she has a foster mother in another municipality, who is also her aunt, but they have not had contact in 10 years, but she has not received any message. Her mother is a drug addict and lives in another municipality, and she has been informed, but there is no need for a crisis team because none of them has contact with the deceased. I warned both crisis teams in those municipalities the next day again … Then, two days passed, and her mother was already hospitalised for an overdose. (C4, ID21)
Perception of the duty of confidentiality
Our material shows that local understandings, interpretations and practices relating to limitations of the duty of confidentiality often led to information being held back. This act of not sharing vital information was based upon different understandings of privacy protection and juridical issues of consent. It could be challenging merely to obtain the information required to assess the need for follow-up or to assess the situation, such as who is dead, what is the cause of the death and who was present at the place of death. This source of frustration was discussed in all of the focus groups and applied to both the divisions within the municipality and outsiders with other organisational affiliations. In our sample, clergy members and undertakers seem to play a particularly vague juridical role in sharing information with employees in municipal positions. What information an employee possessed as the result of a professional position that could legally be shared was also a consideration, as illustrated by this quotation from an undertaker: When the health service connects to us, it can often be a little difficult with confidentiality … you call the crisis team, but they do not even tell you who is dead or who is there. Then I did not go, because I do not go a place where I do not know … I have to know whom to meet. (C3, ID23)
Bereaved persons who use drugs do not fit in
A group of the bereaved who stood out in our data material were the bereaved in concurrent drug use. Several informants pointed out that when someone dies due to extensive drug use, they often have relationships with other illicit drug users. However, the helpers described this group of the bereaved as difficult to help. Regardless of whether they worked in the emergency services, drug-related services or crisis teams, most informants talked about the bereaved who used drugs as not fitting into the existing crisis services. They did not fit in because their needs and drug use were perceived as affecting the notification of the death and the further psychosocial follow-up. Organisational, relational and individual concerns were discussed in all focus groups, e.g., homelessness and challenges due to the rigidity of the service structures.
Complex and challenging support situation
The informants discussed what they thought of as a complex and demanding support situation, wherein the bereaved who use drugs often have an unstructured lifestyle that challenges the framework of the regular follow-up services for potentially traumatising deaths. Some families were described as dysfunctional and with less recourse than the average family with no family members in concurrent addiction. These bereaved were presented as being less capable of receiving ordinary crisis support or as having lived under stress for so long that the family system was affected negatively, as this crisis team member and child welfare social worker reflects on: I think that some of the families we follow up are a bit dysfunctional … it is not as easy to follow them up as it is in ordinary, sudden and unexpected deaths … It is not as easy to get the good conversations, or they do not manage well even with supporting each other, as a slightly more resourceful family might have done in a similar situation … So I think that it affects our work because there is something about the fact that if you are going to get good crisis help, then you have to want it yourself. Crisis help consists of a lot of giving, you cannot just sit … you must use yourself, you must take the help you get, because if you cannot do that, then you will not get good help either, I think. (C3, ID13)
Difficulty bridging psychosocial follow-up and drug use
Because the organisational structures of some municipalities mean that they differentiate between mental health services and addiction services, informants from the psychosocial follow-up services assumed that what the drug-related services could offer might be considered more appropriate than what the regular psychosocial follow-up could offer. They argued that those helpers had the necessary professional expertise and already had a professional relationship with the now bereaved and could better help them, and they stated that competence and experience were crucial when it came to working with bereaved persons in concurrent drug use. These bereaved individuals’ lifestyles were assumed to complicate and challenge the support structure of regular services. For instance, it could be particularly challenging to make contact with them, they had difficulties keeping appointments generally, and they were perceived as not benefitting from a support conversation when they were intoxicated, illustrated by this professional from ambulant emergency service and also a member of a crisis team: We usually follow up with a phone call and home visit the next day; it is difficult for homeless people who do not have a phone. And then, we transfer to crisis teams, and they follow up with telephone contact first and then home visits. You have to be able to answer a phone, be able to show up for an appointment, or get someone to come home and then be able to deal with appointments. I find this problematic. (C4, ID21)
Precautions required
In one of the focus groups, the helpers were particularly concerned about ensuring their security when they met with bereaved persons who were using drugs. The participants, who represented child welfare, ambulance, crisis teams and clergy, shared their experience of how the bereaved who were using drugs could react differently than other bereaved, e.g., acting out more dramatically or expressing themselves more angrily. These meetings were perceived as possibly hazardous situations, as one crisis team member elaborates: It can be different when you are under the influence of drugs … a grief reaction can then actually accommodate most things, but perhaps in a different way than many of us … they become more acting-out under the influence of drugs. (C3, ID13)
Factors facilitating assistance
A recurrent theme throughout our data material was that the barriers reported were surmounted and that the crisis team members said they had the resources, knowledge and systems to provide good quality services to the bereaved if they were notified. Nevertheless, they realised that the follow-up was not ideal and fell short of meeting the needs of the DRD-bereaved. Some informants talked about their wishes rather than the realities, while others shared their good experiences and reflected on what it would take to improve the services. The facilitating elements presented were a mixture of qualitative good professional judgement, functioning systems and good collaborative relationships between well-informed employees. The informants emphasised the significance of seamless transitions and automatic chain reactions in crossing over divisions to find the bereaved, which implies easy access to information by all helpers involved.
Making contact with the bereaved and assessing their need for help
The primary facilitative factor was the first-responder personnel at the place of death providing essential information about the death to the municipality's emergency communication centre, which would then contact the crisis team with expertise in assessing the need for psychosocial follow-up. This suggests that the first attending helpers, regardless of position, should not screen the bereaved's needs but gather crucial information about what happened, who was present, and other concrete details useful for crisis teams when the latter are contacting the bereaved, in line with regular procedures for unexpected, unnatural deaths.
Cooperation
All informants emphasised the importance of cooperation across all levels and organisational affiliations, which requires an overview of all the services involved and the accessibility of all involved services and contacts. It is also essential to understand the bereaved's possible needs. It is crucial to share factual information to permit a quick response in a time-sensitive situation within the services and to answer the questions of the bereaved, as illustrated from an ambulance worker's perspective below: I feel that we give good assistance when these transitions are seamless … from the ambulance and urgent care responders and the overdose team … the police have been there, the priest is on his way and the crisis team has been notified. When it becomes so seamless that it goes by itself without too many obstacles, I feel that we do a good job as a team. And then, when there are a lot of bumps in the road, the emergency room is busy, and we do not get to the priest, and the crisis team does not have resources, it lacks people, and the police are busy with something else … and when things do not go smoothly, we compensate and do a good job then, too. (C3, ID14)
Proactivity
All of the participants from crisis teams emphasised the need for outreach activity. Crisis team members search for the bereaved in whatever way is necessary, e.g., by crossing municipal borders and organisational divisions: It is often a bit like detective work, in the transition from the emergency situation … we have to investigate. (C1, ID1)
This crisis team member underlined that proactivity involves making repeated approaches, even if the service is initially rejected: But to somehow find them and follow up over time because it is not certain that the need will appear immediately, and there may be a completely different need long afterwards … we cannot give this to somebody else; if you say no after two days, then it is not enough; there may be a need later. (C1, ID1) We need to know who the clients are so that we know how to approach whom we approach. We have had some challenges internally with everyone acknowledging the necessity … some would call it luxury crisis work, but really it is not that. It is what is good crisis work. (C1, ID1)
This competence also involves understanding the complex family structures in modern society, which the legal system has not taken into account: We are not doing well enough now, but in the long run to achieve something so we will be able to assist those who need it, regardless of biological ties. Family structure is completely different now, right. The one case I work with, it's divorces, and there's new partners, and it's mine and yours and our children, and there are many, many lines … (C1, ID1)
Discussion
As set out in the results paragraph, our study found significant barriers and facilitative factors – related to organisational structures and cooperation, professional knowledge and understanding of tasks and legal matters, personal commitment and discretion – which either prevent bereaved persons from receiving, or help them to receive, psychosocial help. These findings are supported by international research on how the bereaved perceive support (Titlestad et al., 2019; Valentine et al., 2018; Van Boekel et al., 2013; Walter et al., 2017). The fact that most persons bereaved as the result of a drug death are not offered psychosocial follow-up (Titlestad et al., 2020) is in line with international findings (Cartwright, 2020; McKell et al., 2018; Titlestad et al., 2019; Valentine et al., 2018). However, despite evidence that most of the bereaved experience a lack of professional follow-up, some persons bereaved as the result of a DRD experience adequate and qualitatively good assistance (Titlestad et al., 2019; Valentine et al., 2018). In our study, crucial factors facilitating outreach to the bereaved, from the perspective of first-attending helpers, included seamless transitions across divisions and organisational affiliations, which requires a good overview and cooperation across all levels and accessibility for all professionals involved. A proactive approach to making contact with bereaved persons in need of psychosocial follow-up was also perceived as necessary. Furthermore, at an organisational level, ongoing personnel training was also considered to be necessary to keep all stakeholders informed of the relevant available services, as was easy access to information about these services.
The following discussion will look at the main barriers based on our analysis.
Barriers relating to complex service structures
Previous research shows that the bereaved experience complex help systems (Løseth et al., 2022; Templeton, Valentine, et al., 2017; Valentine et al., 2018). Attending to sudden and unnatural deaths requires the provision of services affiliated with various professions and institutional divisions, including medical first response, police investigation, care of the dead body and follow-up for the bereaved. This complexity also seems to apply to the service providers. The participants point to and illustrate the interconnections described in the ecosystem and clearly demonstrate a need for stronger cooperation between the various levels (Osborne et al., 2021). When helpers may mainly influence the mesosystem, they also must know the macrosystem (the solid framework of legislation and the subsequent follow-up guidelines that exist), whereas both helpers (and users) are essential actors on the microsystem to make the services work. Our findings show that the informants either did not know the legislation or the national crisis guidelines or that these also apply to DRDs. When the informants, to a large degree, had omitted the DRD-bereaved as potentially exposed to traumatic losses, this could be understood in light of a macro-level perspective. Pointing to the interconnection between the meso- and micro-levels, many participants were flustered and apologetic upon discovering the lack of reflection in their own and their colleagues’ neglectful attitudes when they realised this overlook. Although Norway has a welfare system based on equality and universal rights, this lack of attention could be related to the impact of societal norms connected to illicit drug use and associated stigma towards the bereaved (Guy & Holloway, 2007; McNeil, 2021; Reime et al., 2022; Walter et al., 2017). We found it very interesting that the helpers acknowledged their disregard and reflected on this possible connection in their practices. A deeper understanding could mean a significant difference and added value on the micro-level where the services are provided to the DRD bereaved in practice.
According to Osborne et al. (2021), the meso-level concerns the actors, service processes and improvements and represents the level the managers control the most. An example from the meso-level regarding the importance of functioning structures, clarity in delegation and assignment, and mutual understanding of the systems is illustrated by how the duty of confidentiality gave rise to various interpretations, creating a frustrating barrier to sharing information on the micro-level. The national guidelines state that there should be clear lines of responsibility to ensure that critical information reaches those with operational responsibility in the crisis team (Norwegian Directorate of Health, 2016). Our findings suggest that this is not always the case in DRD, at least not in many local practices. Procedures for reporting a possible crisis were not always followed. Thus, the managers should create practical systems, or they may not be in use because “they do not fit”, as the crisis team member quoted (C1ID1) on page 9 states, simultaneously illustrating the interconnection with the micro-level. Research confirms that the majority of DRD-bereaved miss psychosocial follow-up, implying that the resources from the meso-level do not reach the micro-level (Kalsås et al., 2022; Titlestad et al., 2019; Walter et al., 2017).
On the micro-level, the competence of the helpers is in play regarding the value creation for the bereaved from DRDs in public services, i.e., how competent, proactive psychosocial follow-up may prevent negative health consequences. The research on unnatural death shows that, given the magnitude of the incident, many of the bereaved may seem to be untouched or may dissociate or isolate themselves due to the shock or an existential crisis, or in other ways, they may not react as expected by employees who lack competence in sudden, unnatural death or crisis death (Brabant, 2002; Brataas, 2021, pp. 212–214; Doka, 2002a, pp. 323–336; Kauffman, 2011; Norwegian Directorate of Health, 2016, pp. 48–49; Rosenblatt, 2010, p. 1116; Thompson, 2017, pp. 7–18). The crisis teams have special competence in assessing situations and reactions in a more knowledge-based manner in such cases, but the police and ambulance services are usually the first-attending professional helpers and can act as gatekeepers to further help. Some first-responder professionals take a proactive approach when evaluating the need for psychosocial follow-up. Even when they have the bereaved's best interests in mind, this screening may act as a barrier. This may also serve as an example of the interconnection between the meso-level's service function in practice and the individual service provided on the micro-level. If the bereaved are perceived as “calm and collected”, they may not be assessed as needing psychosocial support and, thus, not reported to the municipality's crisis team. On the other hand, if the bereaved act out emotionally, police officers or ambulance workers, in some cases, report directly to a crisis team, with the risk that the emergency communication centre – whose procedures ensure that a crisis team is notified – is not informed of the referral.
Barriers relating to drug use and associated stigma
Most of our informants indicated that they had not thought of DRD as sudden, unnatural or unexpected and therefore did not follow the procedures for initiating psychosocial follow-up for the bereaved. Disenfranchisement is amplified when this co-occurs with an early evaluation and screening based on the grade of emotional expression at the initial meeting with a DRD-bereaved person who hid their reactions. This attitude may point to social stigmatisation, an “othering process” linked to illicit drug use and the presumed marginalised lifestyle of this group (Deacon, 2006; Van Boekel et al., 2013). Death is a sociocultural phenomenon. As are bereaved persons, first responders too are part of their respective cultures (Doka, 2002a, pp. 323–336). Goffman (2009) postulated that stigma influences social interaction by broadening the stigma associated with a societal group. Guy and Holloway (2007, p. 84) argue that deaths from illicit drug use are special because of their lack of social recognition and because the stigma towards this group may often be transferred to their families. The lack of support experienced by many of the DRD-bereaved may be related to associated stigma and disenfranchised death (Corrigan & Nieweglowski, 2019; Doka, 2002a; Goffman, 2009; Link & Phelan, 2001; McLaughlin et al., 2006; McNeil, 2021; Verhaeghe & Bracke, 2012; Walter et al., 2017). Furthermore, the connotations of illicit drug use may hinder the first-responder attendants’ initiation of follow-up. For example, our results showed that some of the first-responder police officers did not report to the emergency communication centre because they had perceived an estranged relationship between the deceased and their next of kin, i.e., the deceased had been in foster care for years as a result of the parent's drug use. Some family members clearly expressed their negativity to the representative of the services based on previous contact or were perceived as being overwhelmed by the loss. Such rejections could also be understood as self-stigmatisation or self-disenfranchisement when viewed from the perspective of stigma and power as processes that occur throughout society (Corrigan & Rao, 2012). This gatekeeping process could be lessened if there were greater competence in dealing with the multitude of shock and crisis reactions to disenfranchised grief. In our focus-group interviews, we did not perceive the individual informants as ill-willed or as intentionally discriminating against the DRD-bereaved, even if they had neglected to offer crisis help to this group. Walter et al. (2017) problematise the other possible reasons for perceived stigmas, such as lack of time or other pressing matters during the acute phase, which may correspond with some of our findings. In addition, some informants believed that the bereaved would receive better follow-up within the addiction services as the providers there were familiar with the next of kin. However, this could be understood as a form of “othering”, presuming that mourning and bereavement among those bereaved by DRD are experienced differently, with their need for psychosocial follow-up therefore being perceived as different than for other people who experience unnatural and sudden deaths.
Suggested actions for follow-up
The facilitative factors in our findings correspond with the main points in the national guidelines for psychosocial intervention in the event of crisis, accident or disaster (Norwegian Directorate of Health, 2016). The guidelines are based on research and the wishes of those bereaved by sudden death. Making contact with the bereaved and assessing their need for help are prerequisites to follow-up. In a crisis, only some of the bereaved can be expected to take the initiative to ask for the help they need. Therefore, proactivity on the part of the helpers is a prerequisite to reaching those who do not want to manage on their own or through their social network to receive the help they need from a preventative health perspective. Help must be offered, and if necessary, the offer must be repeated so that everyone is reached after an unnatural death (Norwegian Directorate of Health, 2016). Cooperation and competence are crucial in value creation in public services and getting the points across in a complex service apparatus with multiple providers. Expertise in unnatural death, DRD, acute grief, crisis and psychosocial follow-up from a prevention perspective is crucial to good cooperation in fulfilling the guidelines’ aims. In the focus group interviews, the moderators and co-moderators found our informants to have empathy and goodwill, which bodes well for professional development in practice.
Strengths and limitations
This study is part of a larger study that provides a source of extensive qualitative data material and ensures methodological stringency (Dyregrov, 2017). We chose focus groups and assembled informants from various positions who attended in the acute phase after medical emergencies and sudden deaths to enhance the reflective processes among the participant as they could relate to each other and make the most of the processes for reflexive thematic analysis (Braun & Clarke, 2019b). In many focus groups, the participants were surprised by their lack of an overview of existing services and said they would have acted differently in many situations had they known that certain services existed, which points to how the macro-, meso- and micro-levels are interconnected.
We have attempted to set out the recruitment procedure and made the analytical process explicit by describing the method and the findings. The numerous quotations have improved this study's validity and transparency. The members of the interview teams were paired so that an experienced senior researcher conducted the interviews and discussed and reflected on the process with the co-moderator, as described by the first author. Finally, the analytical trustworthiness of the study is considered good, as all of the authors discussed the data and findings thoroughly and repeatedly.
Weaknesses relate to the general challenges of focus group methodology, e.g., there was no guarantee that the participants were those with the richest experience in their respective municipalities. The data were derived from the participants’ experience or lack thereof and their assumptions, reflections and understandings. Some of them had met each other previously as colleagues, whereas others had not. At a minimum, previous encounters affected the start of the group discussions. Possible biases and confounders in our choice of municipalities concerning demographics, geography and exposure to those bereaved through DRD were discussed, i.e., how to group the various professionals and their dynamics and interaction flow and how best to facilitate their communication processes during the interviews.
Our cross-sectional grouping of first-responder participants enhanced their knowledge of related services and organisations. Consequently, new connections and relations were made, which is an example of how focus group methodology can create new knowledge as a result of sharing and reflecting processes (Malterud, 2012, pp. 15–17).
Conclusion
This study examines the perspectives of the municipal health and welfare service on what prevents and what facilitates the provision of assistance to persons bereaved as a consequence of DRD during the acute phase. The acute phase represents a challenging and complex support situation. Making contact with the bereaved and assessing their need for assistance are prerequisites to all types of assistance. First-responder professionals must understand DRD as a potentially traumatising event and initiate the procedures set out in the national guidelines. Upon losing a next of kin, a bereaved person cannot be expected to take the initiative to make contact and ask for help. Proactivity based on helpers’ knowledge of the situation is a prerequisite to reaching those who do not want to manage themselves. Help must be offered and, if necessary, repeatedly offered to reach everyone. Competence and cooperation are crucial and necessary within a complex support system, with many service providers acting within a limited timeframe. Expertise in unnatural death, DRD, acute grief, crisis, the prevention perspective and psychosocial follow-up is crucial for those bereaved as a result of DRD to experience being seen and met with the attention they need. For the first time, in 2019, the national strategy for reducing overdoses addresses drug death bereaved in the section for strengthening user participation and cooperation (NDH, 2019). It may seem that the political discourse has a raised awareness of this specific population of DRD, realising that they may represent a public health concern due to the increased risk of developing harmful health outcomes.
Further research is necessary to investigate how assistance in the acute phase can be optimised in cooperation with the bereaved, the municipal health and welfare services, and peer organisations.
Footnotes
Acknowledgements
We heartily thank all the bereaved and the service providers who have used their time and energy to participate in the END research project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Dam fundatio, Norway, funded the doctoral project.