
Abstract
In the Swedish population, prevalence of alcohol use disorders (AUDs), including harmful use during the past year, has been estimated at 8.9% (men: 12.6%; women: 5.3%), while regarding alcohol dependence the estimate was 4.7% (men: 6.7%; women: 2.8%) (WHO, 2010). Alcohol use disorders give rise to considerable psychosocial impairment and suffering for the affected as well as for friends, families and co-workers (Gowing et al., 2015). More than half of adolescents in the US (aged 13–18 years) report alcohol use, and the lifetime prevalence of alcohol abuse and alcohol dependence was reported to be 5.2% and 1.3%, respectively (Merikangas & McClair, 2012). Regarding the influence of genetic factors, the heritability estimates of AUDs vary substantially across twin studies (i.e., 30–78%; Slane et al., 2012; Walters, 2002). Since AUDs encompass both excessive alcohol consumption and alcohol abuse/dependence, the heritability estimates for alcohol consumption vary between 20–60% (see Edwards & Kendler, 2013), while heritability estimates for alcohol abuse/dependence vary between 30–78% (Agrawal et al., 2012; de Moor et al., 2011; Walters, 2002). In one recent meta-analysis of twin and adoption studies, the heritability of AUD was estimated more precisely to be about 50% and there was no difference between men and women (Verhulst et al., 2015). These reported heritability estimates are specific to the studied population, gender and ages. In addition, the variation in heritability estimates may also be an effect of the different instruments used, since the tests operationalise different thresholds for measuring AUDs.
The Alcohol Use Disorder Identification Test (AUDIT) is probably the most commonly used instrument when screening for alcohol-related problems. Developed by the World Health Organization (WHO), the AUDIT has been well established within clinical practice as well as in research settings (Reinert & Allen, 2007). To our knowledge, four studies have previously used this instrument to estimate prevalence and heritability of AUDs among twins (de Moor et al., 2011; Slane et al., 2012; Sung, Lee, & Song, 2011; Sung, Lee, Song, & Kim, 2011). These studies show that heritability estimates for AUDs using the total AUDIT scores vary from 0.35 to 0.78. The observed discrepancies in results might be an effect of the studies’ different age and sex cohorts. The studied populations in all four studies have a wide age range: 18–89 years (de Moor et al., 2011), 30–79 years (Sung, Lee, & Song, 2011; Sung, Lee, Song, & Kim, 2011) and 18–29 years (Slane et al., 2012). Furthermore, the discrepancies in heritability estimates might reflect the studies’ use of different cut-off levels within the AUDIT form related to alcohol consumption, alcohol abuse or alcohol dependence.
To our knowledge, no previous study has investigated the prevalence and heritability estimate of AUDs in an age-homogenous population by using validated scales of the AUDIT. Therefore, the aim of the present study was to investigate this, using a nation-wide sample of male and female twins in late adolescence (18 years old). Assessment of AUDs was performed by using different cut-off levels within the AUDIT, generating different measures of alcohol problems.
Material and methods
Participants
Subjects were included from the on-going Child and Adolescent Twin Study in Sweden (CATSS), which has been described in detail in earlier studies (see Anckarsäter et al., 2011). The participants were recruited from a follow-up assessment at age 18 years, where twins were asked to respond to a web-based questionnaire that included measures of substance and alcohol abuse. The twins were born in Sweden between 1 July 1992 and 31 December 1999. Data were available for 8,972 twins out of whom 642 were excluded due to lack of complete data, i.e., missing items in the AUDIT. Thus, the final study group comprised 8,330 twins. Of these, 58% were female; 29% were monozygotic twins (MZ), 32% dizygotic same sex (DZ-ss), 34% dizygotic opposite sex (DZ-os), and for 5% the zygosity could not be determined. Zygosity is determined by a validated algorithm with a > 95% predictive value compared to DNA testing (Lichtenstein et al., 2010).
AUDIT
The Alcohol Use Disorder Identification Test (AUDIT) was developed by the WHO (Saunders & Aasland, 1987; Saunders et al., 1993) and is a self-report of alcohol-related behaviour during the last 12 months. The AUDIT consists of 10 questions assessing amount and frequency of alcohol consumption (subscale 1, questions 1–3), alcohol dependence symptoms (subscale 2, questions 4–6) and alcohol-related problems (subscale 3, questions 7–10). All 10 questions in the AUDIT could be assigned a score between 0 and 4, thus the total AUDIT score can range from 0 to 40. The validity and reliability of the AUDIT have been extensively investigated. Depending on the cut-offs used, specificities between 78% and 96% and sensitivities between 51% and 91% have been reported for at-risk, hazardous, or harmful drinking (for reviews see Fiellin et al., 2000; Reinert & Allen, 2007). The Swedish version of the AUDIT and its subscales has shown acceptable reliability (Selin, 2003). The AUDIT measures excessive alcohol consumption as well as alcohol-related problems and consequences thereof, such as “signs” of alcohol dependence and alcohol-related harmful effects (Babor et al., 2001; Reinert & Allen, 2007). By using different cut-off levels when using the AUDIT, one can derive several measurements from the AUDIT total score (see below descriptions of AUDIT-10, AUDIT-C and risk groups).
AUDIT-10
This measure is based on the total score and measures excessive alcohol consumption as well as alcohol-related problems and consequences thereof such as “signs” of alcohol dependence and alcohol-related harmful effects (Babor et al., 2001; Reinert & Allen, 2007). From the AUDIT total score, two aspects of clinically relevant alcohol consumption can be derived:
The measurement hazardous/harmful alcohol use, which by using a cut-off of 8 or higher for men and 6 or higher for women, based on research findings in the study by Reinert and Allen (2007) and thus based on findings in adults, indicates the presence of AUDs in general (i.e., hazardous alcohol consumption and alcohol-related problems and consequences thereof). Henceforth, this measurement will be referred to as potentially harmful alcohol use. The measurement alcohol dependence, which, by using a cut-off of 20 or higher for men and 18 or higher for women, indicates presence of potential alcohol dependence specifically. Henceforth, this measurement will be referred to as most likely alcohol dependent.
AUDIT-C
The Alcohol Use Disorders Identification Test-Concise (AUDIT-C) is a brief alcohol screening instrument. The AUDIT-C identifies individuals who are potentially hazardous drinkers or potentially have active alcohol use disorders (including alcohol abuse or dependence) but do not experience the harmful social and physical consequences of alcohol dependence. Henceforth, this measurement will be referred to as potential hazardous alcohol consumption/active alcohol use disorders. The measure is derived from the person's summed score of the first three questions in AUDIT, questions that assess alcohol consumption amount and frequency. The AUDIT-C is a validated screening measure to identify hazardous alcohol use. The summed total score on these three questions in the AUDIT can range from 0–12 and the cut-off for hazardous alcohol consumption is 4 or more points for men and 3 or more points for women (Gual et al., 2002; Reinert & Allen, 2007).
Risk groups for alcohol dependence
This classification is based on an estimate of the person's risk for alcohol dependence. Men and women were classified into four risk groups based on their AUDIT total scores: a low-risk group (0–7 points; 0–5 points), a risky group (8–15 points; 6–13 points), a high-risk group (16–19 points; 14–17 points) and a group needing referral (referred to as most likely alcohol dependent; ≥ 20 points; ≥ 18 points) (Babor et al., 2001).
Statistical analyses
All analyses were performed in both a collapsed fashion and a gender-specific fashion. The Cronbach's α coefficient of internal consistency was calculated for the whole AUDIT scale. Distributions and descriptive statistics were performed for the total AUDIT scale, and for all the cut-offs described above on all 8,330 individuals.
Twin methodology is based on the difference in genetic relatedness in MZ and DZ twins. MZ twins share 100% of their genes while DZ-twins on average share 50% of their segregating alleles. This renders it possible to describe the present genetic and environmental contribution to a trait. The first step of quantitative genetics is intra-class correlations where the score of twin 1 is correlated to the score of twin 2, which is done separately for MZ and DZ twins. If the correlation is larger for MZ twins this implies that genetic factors are involved. By using structural equation modelling it is possible to partition the aetiological factors into (A) the amount of variance due to genetic factors, (C) the amount of variance due to shared environmental factors (i.e., environment that makes the twins similar), and (E) the amount of variance due to non-shared environment (i.e., environment that makes the twins dissimilar). Intra-class correlations were calculated on the total AUDIT scale, and tetrachoric correlations on cut-off measures. Genetic and environmental influences on the total AUDIT scale and cut-offs measures were estimated using univariate sex-limitation twin models (Neale & Cardon, 1992). Sex-limitation analysis assesses quantitative and qualitative sex differences for the genetic and environmental effects on a phenotype. Quantitative sex differences refer to factors that influence both males and females, but their effect on the phenotype is greater for one sex than the other. Quantitative sex differences are implied when the magnitude of the (ACE) variance components is different in males and females. Qualitative sex differences refer to factors that affect phenotypic variation in one sex but not the other. Qualitative sex differences are implied when the genetic correlation among opposite-sex twin pairs is less than 1. For the total AUDIT score and the three different AUDIT cut-offs, we fitted three univariate sex-limitation models. The first model was the full sex-limitation model, allowing for both quantitative and qualitative sex differences. The second model allowed for quantitative sex differences but not qualitative sex differences. The third model allowed for neither quantitative nor qualitative sex differences. For the total AUDIT scale (continuous), we additionally allowed for sex differences in phenotypic variances in models two and three. Models were compared using Akaike information criterium (AIC) to determine the best fitting model. None of the variance components (A, C and E) could be dropped without a deterioration in the fit of the model. All analyses were performed in R Version 4.1.1 (R Core Team, 2021), using the package OpenMx (Neale et al., 2016). OpenMx enables models to be estimated with missing data, i.e., missing completely at random and missing at random. Therefore, both complete and incomplete twin pairs were included in all analyses, resulting in a total of 1,374 MZ twin pairs, 1,604 DZ same-sex (DZ-ss) twin pairs, and 1,807 DZ opposite-sex (DZ-os) twin pairs.
Ethical considerations
The present study was approved by the Research Ethics Committee at Karolinska Institute, Sweden and was in compliance with the 1975 Helsinki Declaration (World medical association, 2001).
Results
Descriptive data
The Cronbach’s alpha for the total AUDIT was 0.80, and for the total AUDIT-C 0.81. The mean total AUDIT score (AUDIT-10/AUDIT-C) for the entire group was 4.3/3.3 (SD 3.6/2.4), and for males and females the corresponding figures were 4.5/3.6 (SD 3.8/2.7) and 4.1/3.1 (SD 3.4/2.2). There were no statistical differences between genders in the AUDIT scores.
Total sample: prevalence of potential hazardous alcohol consumption/active alcohol use disorder (AUDIT-C), potentially harmful alcohol use (AUDIT-10) and most likely alcohol dependent (AUDIT-10)
Regarding the measure “potential hazardous alcohol consumption/active alcohol use”, 57.1% of the entire group reported hazardous alcohol use. When comparing genders, 54.4% of the men and 59.0% (p < .0001) of the women reported potential hazardous alcohol use (Table 1). Regarding the measure “potentially harmful alcohol use”, 26.5% of the entire group reported potentially harmful alcohol use, which included an excessive alcohol consumption, alcohol-related problems and consequences thereof. Comparing gender, 20.0% of the males and 31.1% of the women (p < .0001) reported potentially harmful alcohol use (Table 1). Regarding the measure “most likely alcohol dependent”, females were significantly overrepresented in risk groups 1 and 2 (p < .0001, respectively), while no differences could be discerned between the sexes in risk group 3 (p = .355) and risk group 4 (p = .500) as shown in Table 2. Of the entire sample, 0.3% were most likely alcohol dependent; 0.2% of the males and 0.3% of the females (p = .500; Table 1).
Prevalences (n) and percentages within brackets of twins in respect to hazardous/harmful alcohol use (AUDIT-10), hazardous alcohol use (AUDIT-C) and most likely alcohol dependent (AUDIT-10).
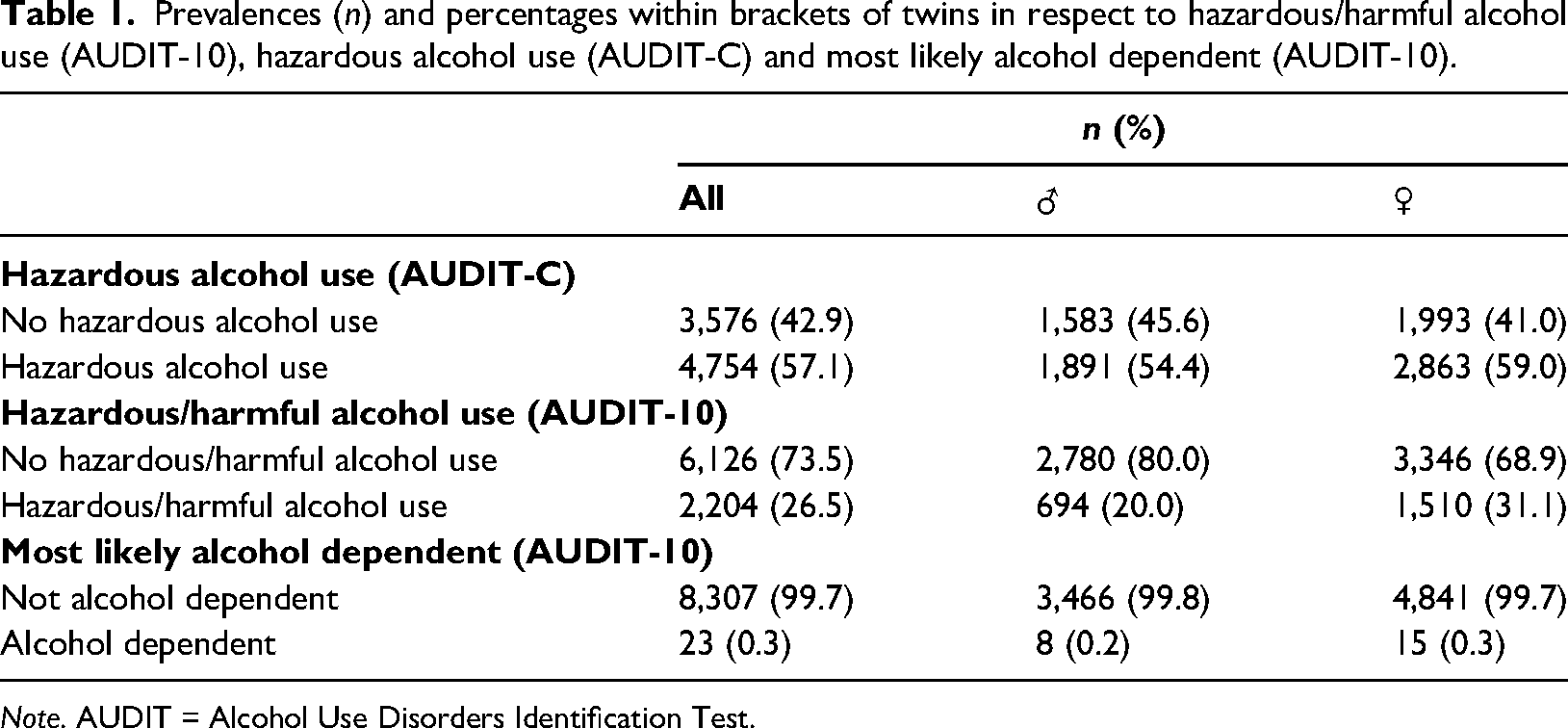
Note. AUDIT = Alcohol Use Disorders Identification Test.
Prevalences (n) and percentages within brackets of twins in respect to 4 risk groups for alcohol dependence for men and women based on the AUDIT total score (AUDIT-10).
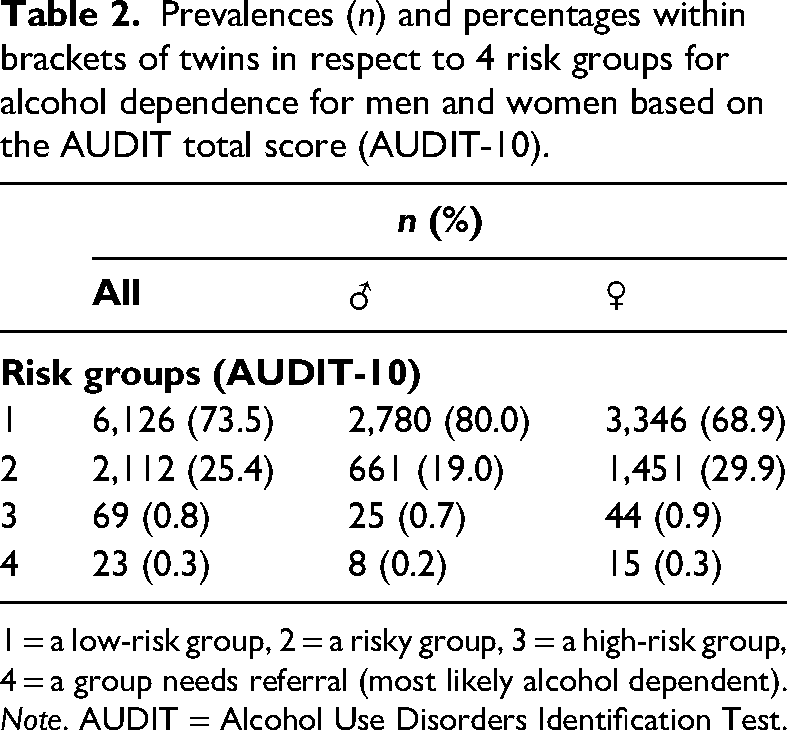
1 = a low-risk group, 2 = a risky group, 3 = a high-risk group, 4 = a group needs referral (most likely alcohol dependent).
Note. AUDIT = Alcohol Use Disorders Identification Test.
Heritability: Twin type comparisons
Total AUDIT score
Intra-class correlations based on the total AUDIT score can be found in Table 3 and were higher for MZ twins than for DZ twins, suggesting genetic influences. DZ-os intra-class correlations were smaller than those of DZ-ss twins, suggesting qualitative sex differences. Results from the univariate sex-limitation model fitting for the total score of the AUDIT and the two cut-offs on all individuals can be found in Table 4. For the total AUDIT score, the best fitting model was the qualitative model, suggesting sex differences in genetic and environmental influences on the total AUDIT score. The heritability was 0.40 (95% CI 0.30–0.51).
Intra-class correlations and heritability estimates for AUDIT total (AUDIT-10).
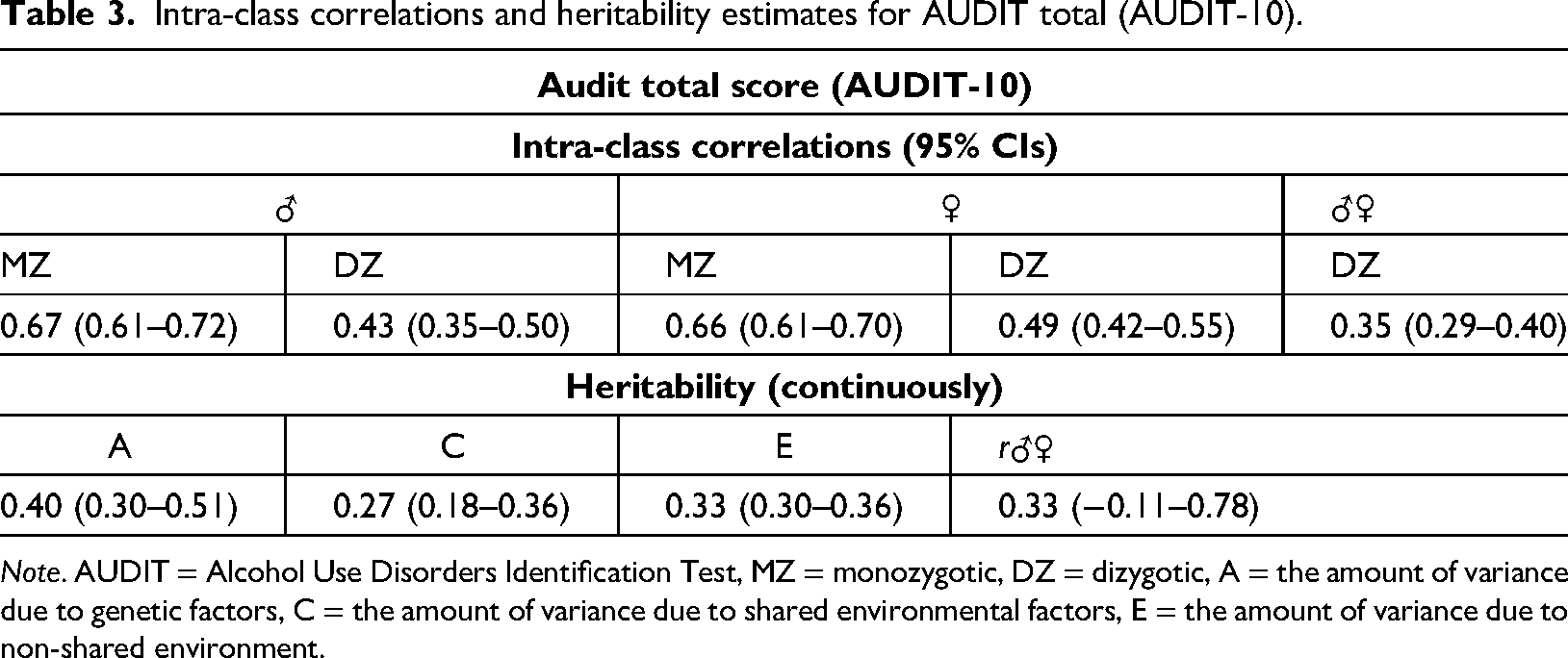
Note. AUDIT = Alcohol Use Disorders Identification Test, MZ = monozygotic, DZ = dizygotic, A = the amount of variance due to genetic factors, C = the amount of variance due to shared environmental factors, E = the amount of variance due to non-shared environment.
Results of fitting univariate models for the different AUDIT scores and cut-offs on all individuals.
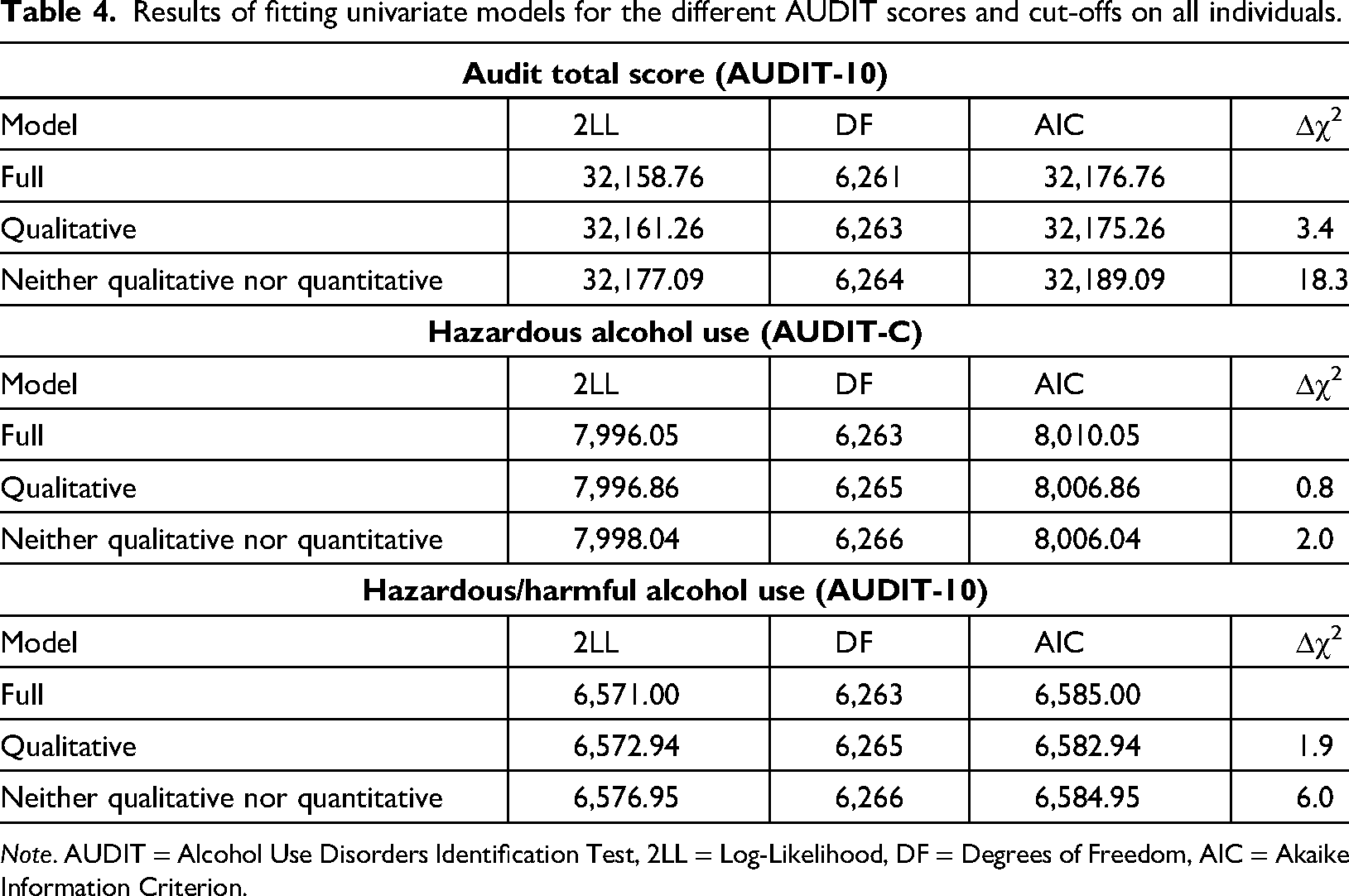
Note. AUDIT = Alcohol Use Disorders Identification Test, 2LL = Log-Likelihood, DF = Degrees of Freedom, AIC = Akaike Information Criterion.
Potential hazardous alcohol consumption/active alcohol use (AUDIT-C)
Tetrachoric correlations based on the AUDIT-C and potentially harmful alcohol use (AUDIT-10) cut-off can be found in Table 5. Overall, correlations were higher for MZ than for DZ twins, implying genetic influence. DZ-os intra-class correlations were smaller than those of DZ-ss twins, suggesting qualitative sex differences. The best fitting model was the qualitative model, suggesting sex differences in genetic and environmental influences on the AUDIT-C cut-off. The estimated heritability was 0.37 (95% CI 0.19–0.54).
Tetrachoric correlations and liability threshold models for hazardous/harmful alcohol use (AUDIT-10) and hazardous alcohol use (AUDIT-C) and most likely alcohol dependent (AUDIT-10).
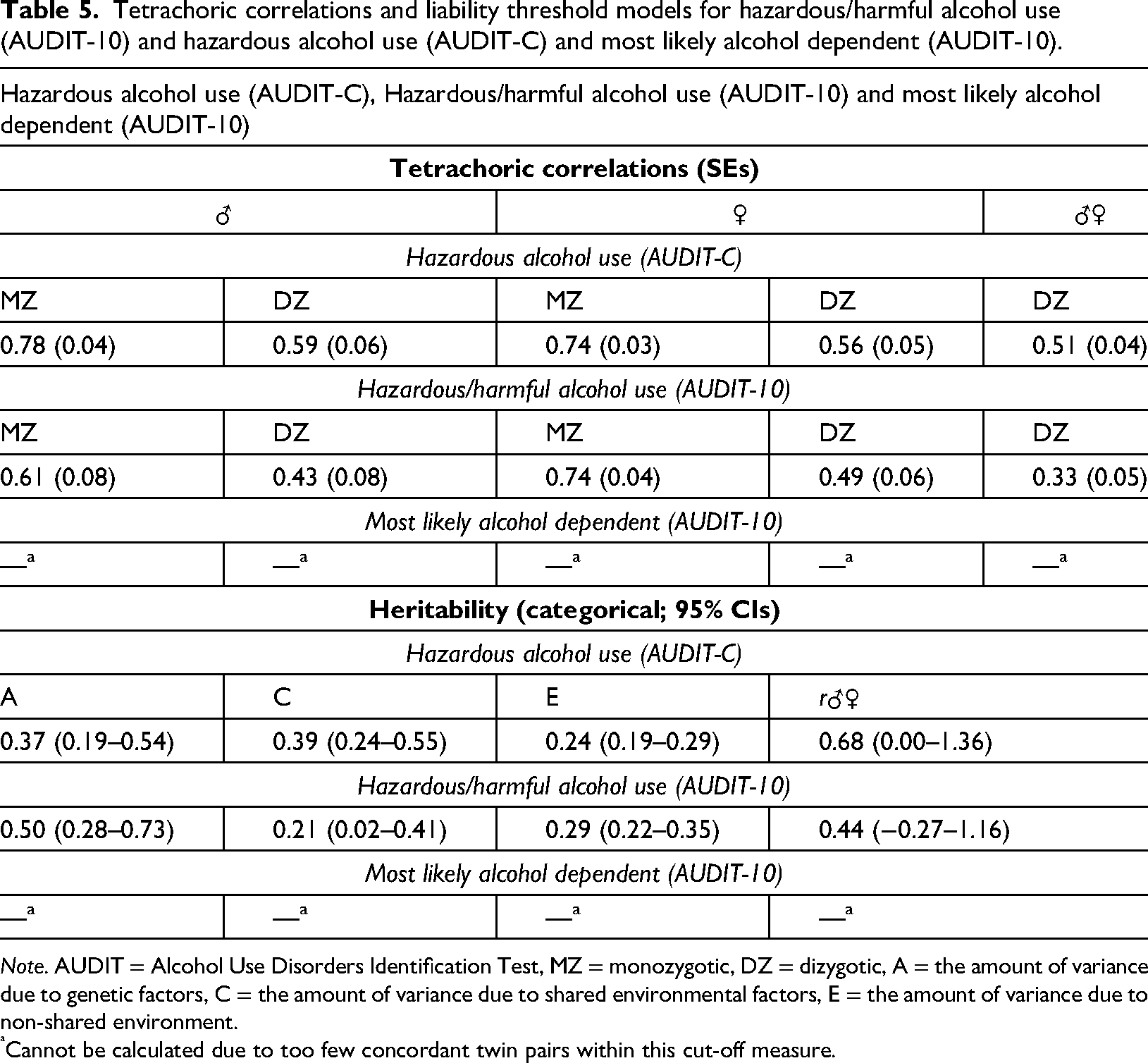
Note. AUDIT = Alcohol Use Disorders Identification Test, MZ = monozygotic, DZ = dizygotic, A = the amount of variance due to genetic factors, C = the amount of variance due to shared environmental factors, E = the amount of variance due to non-shared environment.
Cannot be calculated due to too few concordant twin pairs within this cut-off measure.
Potentially harmful alcohol use
Results from the model fittings revealed the qualitative model to be the best fitting model for potentially harmful alcohol use, with a heritability estimate of 0.50 (95% CI 0.28–0.73; see Table 5).
Most likely alcohol dependent
Tetrachoric correlations and univariate twin analyses could not be calculated due to lack of concordant twin pairs within this cut-off measure.
Discussion
The aim of this study was to describe the prevalence and investigate the heritability of AUDs in a nation-wide sample of male and female twins in late adolescence (aged 18 years). Assessment of AUDs (here: incl. hazardous alcohol consumption) was done by using AUDIT.
Regarding prevalence, risky alcohol consumption was, as expected, more common than alcohol dependence. However, the females in this sample had a risky alcohol consumption to a larger extent than the males did, i.e., were comparatively overrepresented in risk group 2, while men were overrepresented in risk group 1 (i.e., “low risk”). This result is interesting since earlier studies have found that men have a riskier alcohol consumption than women. Second, univariate sex-limitation analyses revealed qualitative sex differences in the genetic and environmental influences for all measures and cut-offs. Heritability estimates were found to be moderate throughout, with overall equally high contributions from shared and non-shared environment.
Prevalence
The prevalence figures indicate that 57.1% of 18-year-old Swedish twins participating in this study reported potential hazardous alcohol consumption /active alcohol use disorder (AUDIT-C) and 26.5% reported potentially harmful alcohol use. Comparing the present prevalence data to the four aforementioned twin studies using AUDIT to investigate AUDs, two studies reported prevalence data of 19.5% of the men and 8.9% of the women (de Moor et al., 2011), and of 70% of the men and 38% of women (Sung, Lee, & Song, 2011). However, these two studied cohorts had quite a wide age span: 18–89 years (de Moor et al., 2011) and 30–79 years (Sung, Lee, & Song, 2011). This wide age span makes it difficult to fully compare them to the prevalence data in the present study, which is based on a homogenous age cohort (18 years). The literature, though, indicate that the prevalence of AUDs is age-related, and that a higher prevalence is found in younger cohorts compared to older cohorts (Hasin et al., 2007). Nevertheless, it should be noted that the absolute majority of the present sample of Swedish 18-year-olds still live at home and attend school, which increases the degree of external social control in this sample compared to, for example, Swedish 25-year-olds who, to a greater extent, will have left both home and school. To develop tolerance and biologically based craving also requires time.
The gender pattern of potentially harmful alcohol use (AUDIT-10) found in the present study deserves some comments. The results show that 31.1% of 18-year-old females twins had a potentially harmful alcohol use, compared to 20.0% among 18-year-old male twins. Concerning AUDIT-C, significantly more females (59.0%) than males (54.4%) had a potential hazardous alcohol consumption/active alcohol use disorder. Nevertheless, the present results regarding “risk groups” (i.e., risk for alcohol dependence) showed more males than females in group 1 (“low risk”) and more females than males in group 2 (“risk group”). However, no gender difference was found regarding group 3 and 4 (“high risk” and “most likely alcohol dependent”). It should, however, be noted that there was no difference in mean total AUDIT score (AUDIT-10/AUDIT-C) between the genders. It therefore appears that the aforementioned difference in genders may be due to some extent to a difference in cut-off levels, being lower in females than males, which in turn could result in higher proportions of hazardous/harmful alcohol use in females. This brings forward the important question of whether one should use different cut-off levels in AUDIT scores between genders. Taken together, assuming that the use of different cut-off values for AUDIT scores between females and males is appropriate, and despite the gender similarities in higher risk groups, these results concerning gender-related alcohol consumption are interesting since they may reflect a development in Swedish society that young females begin to develop alcohol drinking patterns similar to, or even exceeding, those of males at this age. If the alcohol drinking pattern in young females is not only similar to but exceeds that of young males it would be unusual from a global point of view. Other studies have concluded that although males consume more alcohol than females in all regions worldwide, females in high-income countries consume more alcohol than those in low-income countries (Rehm et al., 2009). For example, Keyes et al. (2011) have reported that in younger birth cohorts in North America and Europe the gender gap in alcohol consumption is narrowing in many countries. In fact, during the last 20 years, the gender gap in drinking has successively narrowed among emerging adults, and for adults, a similar pattern, as well as a narrowing of the gender gap regarding alcohol-related health problems, has been observed (White, 2020). For adolescents and emerging adults, this seems to be primarily due to alcohol use among males having declined more than among females, while among adults, alcohol use is increasing for women but not for men (White, 2020). Such a convergence in the rates of alcohol use and alcohol-related problems between men and women in young cohorts has been consistently observed in different countries across the world, and has been suggested to reflect changes in the socio-psycho-cultural environments that affect drinking habits (Erola & Karpyaka, 2015). That it was more common to find gender difference among lower-risk groups but not higher, could indicate a more similar drinking pattern between genders, while the cut-off for potentially harmful alcohol use (AUDIT-10) is still lower for women due to gender differences in biological sensitivity to the harmful effects of alcohol. Based on this, women at this age should then be at greater risk of biological adaptation and therefore greater risk of developing alcohol dependence compared to men.
Clinical relevance and implications for practice regarding prevalence
Taken together, the results from the present study, in combination with previous research, emphasise that the need to focus on AUD interventions is more urgent than previously known. Notably, Roerecke and Rehm (2013) state, first, that mortality in individuals with AUDs is higher than stated in previous research; second, that females generally have higher mortality risks compared to males; and third, that younger age groups display substantially higher mortality risks than older age groups. The present results are alarming, both relating to AUD as a more comprehensive threat to general public health, and to the more hazardous/harmful drinking pattern among females than anticipated. Although women often still tend to drink less than men, the risk–severity paradox (wherein women suffer greater harms than men at lower levels of alcohol exposure, see Foster et al., 2018), also needs to be considered. Since females in general develop more harmful consequences from alcohol intake compared to males, this would merit a more comprehensive focus on preventative work with young persons and females in particular. The present results regarding gender pattern concerning AUDs support the need to develop more targeted prevention towards women, to address both the alcohol use and the related harms among women (see White, 2020), which may require a national intervention from Swedish society.
Heritability
Heritability estimates for the different AUDIT measures and cut-offs were overall found to be moderate. For the AUDIT total and the AUDIT-C (potential hazardous alcohol consumption/active alcohol use disorder) cut-off, heritability estimates were fairly similar with largely overlapping confidence intervals, 0.40 (95% CI 0.30–0.51), and 0.37 (95% CI 0.19–0.54), respectively. For potentially harmful alcohol use (AUDIT-10), heritability was estimated to be 0.50 (95% CI 0.28–0.73), albeit with confidence intervals considerably wider than for the other two measures. Estimates for shared and non-shared environment ranged between 0.21 and 0.39, implying overall moderate influences on AUDs.
Univariate sex-limitation models revealed qualitative sex differences for AUDs, suggesting that different genetic and/or environmental factors influence AUD variation in males and females. Regarding the influence of sex, the present results were in line with those of previous studies, indicating no quantitative sex difference regarding heritability of alcohol dependence (e.g., Knopik et al., 2004). There are highly limited data on adolescent AUDs but some studies do suggest small and non-significant genetic effects (e.g., Knopik et al., 2009; Rose & Dick, 2004).
To our knowledge, the present study is the only study that has used the AUDIT to investigate the heritability estimates of AUDs in the transition into adulthood (18 years of age). This study design is important since the heritability estimates of AUD might be age dependent (i.e., the influence of genetic factors predisposing for AUDs may vary with age). In this study, it was found that by 18 years of age, heritability for potentially harmful alcohol use (AUDIT-10) was in line with other studies using adult twin studies (i.e., approx. 30-year-olds) on various drinking-related outcomes, where genetic effects accounts for 40–60% of the variance (Dick et al., 2009; Hicks et al., 2014). Heritability seems to be “building up” towards more influence in adult age, since studies have found that while heritability among young persons (in adolescence) is relatively low and studies on adults have found that heritability is higher – the age of 18 years is a point in time where estimates of heritability are in line with those obtained in adult samples, but less so compared to adolescents. Unfortunately, heritability estimates were not possible to calculate for alcohol dependence, since too few twin pairs were concordant. Previous twin and adoption studies have shown that heritability measures estimates between 50–60% for alcohol abuse/dependence (Dick & Bierut, 2006). However, there are indications that problem drinking might have lower heritability estimates (upper limits 30–35%) (Walters, 2002), and that heritability estimates are higher when employing more severe definitions of AUDs (Walters, 2002).
Hence, that the influence of genetic factors predisposing for AUDs varies with age is one explanation behind the divergent results in heritability estimates for AUDs. The present heritability estimates converge with the findings of de Moor et al. (2011) and Sung et al. (Sung, Lee, & Song, 2011; Sung, Lee, Song, & Kim, 2011: range 35–40%), but they are lower than those found by Slane et al. (2012), who reported an estimate of 78% in 20-year-old twins. These divergent heritability estimates could thus be explained by the different ages of the studied cohorts. Twins in the present study and in that of Slane et al. (2012) were younger (present study: 18 years; Slane et al., 2012: mean age = 21 years), compared to the twins studied by de Moor et al. (2011) and Sung et al. (Sung, Lee, & Song, 2011; Sung, Lee, Song, & Kim, 2011) (mean sample ages = 40 years). Though the literature is relatively scarce concerning knowledge about the genetic influence on AUDs in various ages, van Beek et al. (2012) studied the heritability of AUDs, as assessed by the CAGE inventory, in various age groups (age span 15–32 years) of male and female twins. Their results indicate an increase of additive genetic influence on AUDs from 28% at ages 18–21 years to 58% at ages 21–23 years, which remained high thereafter up to ages 30–32 years. On the other hand, Long et al. (2017) found that the total heritability for AUD in males was stable across the three age periods 18–25 years, 26–33 years and 33–41 years. Long et al. (2017) also found that two sets of genetic factors contributed to the risk of AUD, one originating during the age period 18–25 years and the other during the age period 26–33 years. It is, however, not known whether the additive genetic influence on AUDs decreases at or after age 40. In this context it should be noted that sustained epigenetic differences arise from early adulthood to old age and contribute to an increasing discordance among MZ twins during aging (Talens et al., 2012). Regarding the influence of heritability and environmental factors on alcohol consumption, Edwards and Kendler (2013) investigated the influence of total heritability and shared environmental factors on alcohol consumption in various age groups (total age range of 12–33 years) of male twins and found that total heritability increased from 0 at ages 12–14 years to 40% by ages 18–21 years. Therefore, it seems that in the present study, the 18-year-old twins are at a time-point when heritability for alcohol consumption begins to rise rather dramatically. Edwards and Kendler (2013) also found that the influence of shared environmental factors on alcohol consumption declined over time. In the age group 18–21 years they found an influence of shared environmental factors of 17%, compared to the corresponding value of 39% in our study of 18-year-old twins. However, as previously discussed regarding the impact of shared environmental influence, it is possible that the decline in influence of shared environmental factors could be more apparent somewhat later in life, after 18 years of age, since leaving home after 20 years of age effectively decreases the level of external social control and increases individual responsibilities. This could, especially for vulnerable persons, result in a considerable degree of increased stress. Nevertheless, taken together, the results from the present study suggest that, at the age of 18 years (or thereabouts), a moderate influence on alcohol consumption by additive genetic factors (i.e., heritability) has been established.
Clinical relevance and implications for practice regarding heritability
In our data, genetic, shared and unique environment account for an approximate equal variance; in fact, shared environment accounted for slightly more of the variance. From a clinical standpoint, this is an important finding. It indicates that while genetic influences increase steeply with age (as discussed above), moderate influences of shared and non-shared environment actualise the importance of initiating early interventions around this age. By focusing on early interventions to decrease alcohol use among 18-year-olds, for example through information of the consequences of alcohol consumption on the developing brain and increasing the possibilities of establishing alternative ways of life, the alcohol debut and development of problematic drinking patterns may be at least postponed. This should result in better ways of coping with stress and more awareness of the negative consequences of an increased alcohol use. However, the generalisability of the results is limited, as the answering frequency was 55% of those who participated at age 9, and since non-responders are more likely to experience/exhibit mental health issues as well as adverse outcomes. Thus, our estimates should be interpreted with caution regarding uncritical extrapolation to the general population.
Strengths and limitations
The CATSS-18 study is a prospective and nation-wide study that adds to the validity of the obtained results. However, the results must be interpreted in the light of some limitations. First, this was a cross-sectional study and the results are derived from self-reported data. This might imply that the results concerning alcohol consumption and the perceived effects thereof might be influenced by subjective distortions, as well as being confined to the cohort in question. However, the AUDIT has been validated for self-report. Second, the study's response rate of the twins who completed the questionnaire at 18 years was 55% of those who participated at age 9. Thus, if included, the remaining 45% of the twins who chose not to complete the questionnaire might have influenced the present results concerning heritability and prevalence of AUDs in an uncertain fashion (also, non-responders are more likely to experience/exhibit mental health issues as well as other adverse outcomes). Most likely the prevalence would then have risen since non-responders may be more prone to problems, which limits the generalisability of the study and the obtained estimates should be interpreted with caution regarding uncritical extrapolating to the general population. If the non-responders had been included, this might hypothetically have resulted in altered prevalence rates, possibly more similar to the ones presented by Edwards and Kendler (2013). Finally, confidence intervals in the potentially harmful alcohol use (AUDIT-10) group were quite wide, therefore these findings should be interpreted with caution.
Conclusions
The present results emphasise the issue of using an age-homogenous sample in this type of research. For this sample of Swedish 18-year-olds, it was more common for females than for males to have a potential hazardous/harmful drinking pattern rather than a low-risk drinking pattern (where instead males were overrepresented). Since previous studies have found that men in general engage in more hazardous drinking than women, the cause of the present result merits further investigation. It can be discussed whether this finding in 18-year-old twins is representative of the whole population of 18-year-old individuals in Sweden. Nevertheless, this finding merits further study, investigating whether earlier public health-oriented interventions should be more directed towards young women. In addition, whether it is appropriate or not to use different cut-off values for AUDIT scores for males and females needs to be further investigated. Heritability estimates for potential hazardous/harmful drinking patterns were moderate, with shared and unique environmental effects contributing to the association to an equally large extent. This also merits future investigation of differences in the impact of heritability and shared and unique environment on the person to better understand the mechanisms behind the development of alcohol dependence.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.