
Abstract
Background:
Treatment for substance use disorder (SUD), results, in general, in improvements in terms of both drug use and social functioning. However, there are clients who are in need of repeated treatment. The aim of this retrospective study was to identify, for adults in compulsory care for severe SUD, the association between reporting having experienced a risky psychosocial childhood and repeated entries into the Swedish compulsory care system for SUD.
Method:
Hierarchical logistic regression and mediation analysis methods were used to analyse data from the Swedish National Board of Institutional Care (SiS) database. The sample included 2719 adults assessed at their compulsory care intake. The study examined the association between history of institutional care, family with SUD or psychiatric problem and repeated compulsory care entries as an adult controlling for main drug, age and gender.
Results:
In the regression model the factor with the strongest association with repeated compulsory care intakes for SUD, was as a child having been in mandated institutional care (OR = 2.0 (1.60–2.51)). The proportion of the total effect that is mediated through LVU (law (1990:52) the care of young persons (special provisions) act) was 33% for SUD problems in family during childhood, 44% for psychiatric problems in family during childhood, and 38% for having been in foster care.
Conclusion:
Having been in mandated institutional care as a youth was strongly associated with repeated compulsory care for SUD as an adult. This is concerning since receipt of services as a child is supposed to mediate against the consequences of risky childhood conditions. These adults, as a group, are in need of a well-coordinated and integrated system of extensive aftercare services to reduce the likelihood of re-entry into compulsory care for an SUD.
Introduction
Whereas there is a significant amount of research on the effectiveness of treatment for substance use disorder (SUD), there are much fewer studies on the group of clients for whom treatment is less successful, those who return repeatedly, i.e., treatment repeaters. In a review of the literature it is shown that treatment for SUD, in general, results in improvements for the clients, in terms of drug use and social functioning (McNeese-Smith, Faivre, Grauvogi, Warda, & Kurzbard, 2014; Perreaulte et al., 2010). Other studies (Stenius, Ullman, Storbjörk, & Nyberg, 2011) also indicate that treatment use for SUD results in reductions in substance use and criminal activities, as well as improvements in psychosocial functioning. However, there are clients who need to use SUD treatment more than just for one time period and instead use treatment in a repeated pattern.
In a Swedish study by Grahn, Chassler, and Lundgren (2014) the authors identified that among clients in the Swedish voluntary treatment system for SUD, individuals with higher substance use severity and higher service needs were more likely to be treatment repeaters. Grahn and colleagues (Grahn et al., 2014; Grahn, Lundgren, Chassler, & Padyab, 2015) also found that individuals with SUD who were treatment repeaters had more severe levels of substance use and criminality than clients with only one admission. In a second study (Grahn et al., 2015) they identified that a key factor associated with repeated entries to compulsory care for SUD as an adult was having been mandated to compulsory care as a youth. 1 However, this study did not explore any family and childhood conditions factors.
An important continuation of the research on repeated compulsory care for SUD is to now examine the association between having had a riskier psychosocial childhood history, not only having been institutionalised as a child, and having a history of repeated compulsory care episodes for SUD as an adult. The current study’s aim was to investigate the association between (1) having resided with parents with SUD problems; (2) having resided with parents with psychiatric problems; (3) having been in foster care; (4) having ever been in compulsory institutional care for youth and having more than one entry to compulsory care for SUD as an adult.
The Swedish compulsory care system for individuals afflicted by SUD
Individuals who suffer from SUD so severely that they constitute a danger to themselves or others, can in Sweden be mandated to compulsory care by the Swedish court system. The law “Care of Abusers (Special Provisions) Act (1988:870)” is founded on the framework of civil (non-criminal justice) rehabilitating compulsory care. In comparison to other countries, for example the United States, where it is common that compulsory care for SUD is part of the criminal justice system or part of psychiatric care (Israelsson & Gerdner, 2010) this is not the case in Sweden, where there is a unique government authority for compulsory care due to SUD for adults.
It is the Social Services Board in a person’s home municipality that applies for care through LVM (Care of Abusers (Special Provisions) Act (1988:870)) to the administrative court. The legislation is mandatory for the municipality in the sense that if it is likely that a person needs to be given care by LVM, the social welfare board is obliged to apply the law to provide the necessary care. 2 In Sweden, compulsory care for SUD can be up to six months.
Although compulsory care is an established part of the addiction treatment system in Sweden (Gerdner & Berglund, 2011; Runquist, 2012) it has been subject to recurrent political and professional debate. Central issues in the discussion includes security of person in compulsory care, ethical aspects of providing care for an SUD without the person’s consent, content and quality of the provided care (Storbjörk, 2010).
A previous study by Storbjörk (2010) indicated that clients in compulsory care in Sweden, in comparison to clients in voluntary treatment, tend to use higher levels of alcohol and drugs, to be younger, and live in more marginalised social situations with respect to both housing and livelihood. An earlier study by Grahn et al. (2015) showed that clients who were repeatedly mandated to compulsory care for SUD experienced greater needs and problems and were in a more vulnerable social situation than those who experienced compulsory care for an SUD only once. From this we can assume that those who are mandated to compulsory care for SUD in Sweden are individuals who experience high risk and high vulnerability with respect to a range of biopsychosocial needs and problems.
Family related vulnerability and risky substance use as adult
Residing in institutions or in foster care during childhood
Our prior research study indicated that compulsory institutional care for youth increased the likelihood of repeated institutionalisation for SUD as an adult (Grahn et al., 2015). However, the literature on the consequences of youth institutionalisation is conflicting (Preyde et al., 2011; Souverein, Van der Helm, & Stams, 2013). There are studies that show that adolescents with social problems who live close together may influence each other in negative ways (Aguilar-Vafaie, Roshani, Hassanabadi, Masoudian, & Afruz, 2011; Whitehead, Keshet, Lombrowski, Domenico, & Green, 2007). Positive attitudes toward, for example, crime and substance use were more likely to be reinforced. These adolescents tend to learn to know others with similar problems to their own, which has a negative impact on their own behaviour (Andrews & Dowden, 2006; Dodge, Dishion, & Lansford, 2006). On the other hand, there are two meta-analysis studies which both found positive effects of institutionalisation. In a meta-analysis of research from 1990 to 2005, regarding children and adolescents with behavioural problems conducted by Knorth, Harder, Zandberg, and Kendrick (2008), the results indicated that adolescents treated in an institution for their behavioural problems experienced an improvement of their problems to a moderate or large extent, compared with control groups that had not been institutionalised. Another meta-analysis by De Swart et al. (2012) included studies on adolescents from the US and Europe between the years 1980 and 2011. Their analysis showed that institutional care for adolescents overall can lead to positive effects.
There is, however, research that indicates that there are not similar effects of institutionalisation compared to foster care on outcomes (Strijbosch et al., 2015). One study by Laukkanen, Hakko, Riala, and Räsänen (2008) showed that boys who were placed in institutions were more likely to abuse drugs than boys who grew up in foster care, or with their parents. These findings indicate a need to separately explore the relationship between having a history of foster care and a history of institutionalisation on repeated LVM care as an adult.
Residing in a family where substance abuse was a pattern during childhood
Previous research has shown that risky substance use and SUD within the family has a strong association with future substance use and SUD for adolescents (Andreas & O’Farrell, 2017; Clark, 2004; Park & Schepp, 2015; Stone, Becker, Huber, & Catalano, 2012). Parents with SUD may serve as role models whom youngsters follow. The use of substances may also lead to conflict and violence in families, which may increase the risk of abuse (Hjern, Arat, & Vinnerljung, 2014). In families where narcotics are used this vulnerability increases further, given that it is illegal and less socially accepted (Järkestig Berggren, Magnusson, & Hanson, 2015).
A meta-study by Clark (2004) regarding risk factors for substance use among adolescents found that children of parents with SUD ran an increased risk of developing substance abuse themselves; further risk factors were low socioeconomic status and male gender. Other studies have shown that alcohol addiction in the family is related to occurrence of own alcohol use by adolescents (Gruber, Celan, Golik-Gruber, Agius, & Murphy, 2007; Milne et al., 2009), recurring problems with alcohol abuse, as well as more serious substance use problems (Milne et al., 2009). Narcotic use in the family was associated with emergence of own narcotic use and recurring problems with use of narcotics (Milne et al., 2009). One study (von Sydow, Lieb, Pfister, Höfler, & Wittchen, 2002) showed contradictory results concerning the relationships between different family members’ substance use and a future problematic substance use for children and adolescents. A Swedish report by Hjern et al. (2014) showed that children with parents with SUD who had not been in contact with social services as children or adolescents were at increased risk of addiction, psychiatric problems and criminality as adults. These studies suggest the importance of examining whether there is an association between residing with parents with substance use problems as children and later patterns of repeated court-ordered compulsory care for SUD as adults.
Residing in family with significant mental health problems during childhood
Psychiatric problems within the family have, in research studies, been found to be linked to individuals developing SUD as adults (Alati et al., 2005; Lovejoy, Graczyk, O’Hare, & Neuman, 2000). In a meta-study conducted by Mowbray & Oyserman (2003) regarding SUD for individuals born to parents with mental disorders, they found that having parents with mental disorders as a child was associated with a moderate increase in risk for developing both SUD and a mental disorder as adults. Adolescents with parents with mental health problems also showed increased risk for substance use, even though the results were mixed.
Other studies (Cortes, Fleming, Mason, & Catalano, 2009; Lamis, Malone, Lansford, & Lochman, 2012) identified a strong association between maternal depression and both earlier onset of use of alcohol for adolescents and higher level of alcohol use. The results from another study showed that the risk of developing SUD was approximately three times higher with a mother who was suffering from depressive symptoms, compared those with a mother who was not depressed (Weissman et al., 2006). These studies suggest that it is important to explore whether having resided with parents with mental health problems is associated with later risks of receiving court-ordered compulsory care for SUD.
Theoretical framework
As the theoretical foundation for this study we have used the behavioural model for vulnerable populations (Gelberg, Andersen, & Leake, 2000). This is a modification and development of the original model that was created during the late 1960s in order to define and measure equitable access to healthcare and to reveal which factors predict healthcare use (Andersen, 1968). The behavioural model of health services use is based on the idea that use of health services is a function of predisposing, enabling, and need factors (Andersen, 1995). The modified version, the behavioural model for vulnerable populations (Gelberg et al., 2000), adds further dimensions to the model to consider when studying the use of health services among vulnerable populations. When using the revisited model, some of the categories can and need to be adapted based on the group it is intended to be applied with.
In this article, we adapted and used the behavioural model for vulnerable populations as a theory to identify whether specific risky childhood factors (predisposing) is associated with repeatedly needing compulsory care for SUD as an adult through the Swedish addiction treatment system. The association between the following risky childhood factors will be examined: having resided with parents who had SUD or psychiatric problems. We also examine two enabling factors: having been in foster care or residing in an institution through LVU setting as a child. The following literature review reports on additional predisposing, enabling, and needs factors that need to be taken to account when examining factors associated with repeated compulsory care for SUD.
Predisposing factors
Age
Research has shown that treatment utilisation for SUD is highly associated with age (Saum, Hiller, Leigey, Inciardi, & Surratt, 2007). One study from the US showed that clients with experience from prior treatment episodes are older than first-time clients (Cacciola, Dugosh, Foltz, Leahy, & Stevens, 2005). Other studies highlight that clients who use treatment repeatedly are at a younger age when they begin with problematic use of a substance compared to clients who have had only one episode in treatment (Dennis, Scott, Funk, & Foss, 2005; Scott, Foss, & Dennis, 2005). Swedish studies (Grahn et al., 2014; Grahn et al., 2015) show similar results, that higher age is associated with both more voluntary treatment episodes and repeated entries to compulsory care for SUD.
Gender
Studies on SUD and treatment by gender show differences between men and women regarding how and when they begin their addiction career and the subsequent treatment for SUD (Dennis et al., 2005; Grella, Hser, & Hsieh, 2003; Grella, Scott, & Foss, 2005; Östlund, Spak, & Sundh, 2004). Studies (Grella et al., 2003; Grella et al., 2005) show that women often begin with substance use through personal relationships and at a later age, but enter treatment for SUD after a shorter period of misuse compared to men. The SUD career among women was considerably shorter compared to among men (Dennis et al., 2005). In a study by Grella et al. (2003) the authors showed that women were more likely to have a history of repeated treatment use, which can be understood as women being in generally more likely to participate in treatment than men (Kang, Deren, & Colóne, 2009). Regarding psychosocial vulnerability, research by Östlund et al. (2004) shows that early experiences of insecurity, stress and trauma are factors that are much more prevalent among women with SUD compared to their counterparts.
Family
In this study, having resided in a family with SUD or psychiatric problems as a child are classified as predisposing factors, due to these riskier family and childhood conditions being immutable and not something welfare policies can change at the point of adulthood. Previous research regarding family related factors such as SUD or psychiatric problems has shown a significant association with developing risky substance use as an adult (Alati et al., 2005; Andreas & O’Farrell, 2017; Clark, 2004; Lovejoy et al., 2000; Park & Schepp, 2015; Stone et al., 2012).
Enabling factors
This study defined having resided in foster care and/or LVU (law (1990:52) the care of young persons (special provisions) act) as possible enabling factors in that these societal interventions were provided in order to promote well-being of the children and if successful should reduce the likelihood of repeated compulsory care. Studies on consequences of youth institutionalisation and foster care are conflicting (Preyde et al., 2011; Souverein et al., 2013). Some studies show negative outcomes of institutionalisation (Andrews & Dowden, 2006; Dodge, et al., 2006; Grahn et al., 2015), while other studies show positive effects of institutionalisation and foster care (De Swart et al., 2012; Knorth et al., 2008; Laukkanen et al., 2008).
Need factors
Substance use
Since individuals who are placed in court-ordered compulsory care, LVM (Care of Abusers (Special Provisions) Act (1988:870)), due to their SUD, all have high levels of current substance use severity, we used no variable to specifically measure substance use severity. Instead, we used one variable to measure primary type of substance used. Specifically, a question asked to the client was “What is the primary drug you have problems with?” The answers were either alcohol or narcotics. This is of interest since alcohol is a culturally accepted and legal drug in Sweden, while all narcotic use is prohibited, unless it is on prescription by a physician.
Methods
Register databases
In Sweden, the National Board of Institutional Care (SiS, in Swedish, Statens institutionsstyrelse) at the request by the government uses DOK (documentation systems in addiction treatment) as an instrument for baseline assessments and documentation, and KIA (client administrative database) as a register database for adults mandated to compulsory care for SUD. SiS has responsibility for the data from these assessments that are entered into a database (DOK and KIA). The DOK and KIA data (2001–2009) have been merged with data from the Swedish National Death Registry (2001–2011) at an individual level using a de-identified person identification number. The researchers do not have access to any identifiable information regarding any individual in the study.
Population
The population in the study was individuals who had been mandated to enter compulsory care for SUD between 2001 and 2009 and who had, during their assessment interview at the intake, given their consent to SiS that their interview could be used for research. A total number of 4515 individuals were included in the database, representing approximately 90% of the 5007 clients who received compulsory care for SUD between 2001 and 2009. Given that 90% of the national LVM treatment population was included in the study we felt it was more appropriate to talk about our study population as a “population” rather than as a “sample”. Among the 4515 individuals included in the database, 1061 died during the course of the study and an additional 735 were missing baseline data (i.e., did not complete the baseline interview), resulting in 2719 cases for analysis. We have included a missing data section below.
Statistical methods
Univariate descriptive statistics were used to describe the population. Second, bi-variate analyses were conducted using chi-square tests to examine the statistical association between ordinal independent variables and compulsory care repeaters compared to non-repeaters and an independent samples t-test was used to examine the statistical association between the continuous level variable (age) and compulsory care repeaters compared to non-repeaters. Odds ratios and their 95% confidence intervals for compulsory care repeaters were calculated by means of a multivariable hierarchic logistic regression model. This model was used to assess the predictive value of socio-demographic variables and type of main drug (first block), childhood variables (second block) and compulsory institutional care for youth (third block). This method was used to assess the relative importance of demographic, type of main drug, family and childhood risk factors including history of prior of institutional care during childhood and adolescence. Finally, in order to test for the hypothesis that the effect of gender, having resided with parents who had SUD or psychiatric problems and having been in foster care on repeated compulsory care for SUD as an adult may be mediated by compulsory institutional care as a youth (LVU), a mediation analysis was performed. Mediation analysis was undertaken using the user-written command binary_mediation in Stata version 13.1 (StataCorp, College Station, TX, USA) to estimate the direct and indirect effects using the product of coefficients approach which was made popular by Baron and Kenny (1986). This approach is based on two regressions: (1) regress the outcome on the exposure, the mediator, and the covariates; (2) regress the mediator itself on the exposure and the covariates. The direct effect is the exposure coefficient in the outcome regression model that includes the mediator. The indirect effect, however, is taken as the product of the exposure coefficient in the mediator model times the mediator coefficient in the outcome model. This product taken as a measure of the indirect effect, thus has a seemingly intuitive interpretation as the effect of the exposure on the mediator times the effect of the mediator on the outcome. The binary mediation program is based on the methods described by MacKinnon and Dwyer (1993) and computes indirect effects for models with multiple mediator variables (binary or continuous) along with either a binary or continuous response variable using standardised coefficients. We used the bootstrap command to obtain standard errors for the direct and indirect effects along with 95% confidence intervals.
Missing data analysis
A detailed analysis of missing data was conducted. For each variable that was missing data, the dependent variable was compared for the missing data cases and the complete data cases. To evaluate the impact of missing data on the final results, all bi-variate analyses were repeated and compared to bi-variate results based on complete cases. Results for each of these analyses showed that the results were highly comparable to the analysis based on complete cases.
A comparison between age, gender and repeated entries between those who died during the time span of the study and those who were available until the end of the follow up were also included in the analyses. There were more men represented between deceased compared to non-deceased (76% and 61%, respectively, p < 0.01) and those who died also showed higher age vs. non-deceased (47 ± 14 vs. 37 ± 13 years, p < 0.01). The proportions between deceased (44%) and non-deceased (40%) individuals (p-value was not significant) regarding repeated use of compulsory care were similar.
Ethics and limitations
The register data and the baseline interview data used in this study are from clients who gave permission for the use of their data for research purposes. These databases do not contain information that could lead to identification of individuals. The Swedish National Ethics Board have reviewed and approved the study.
When interpreting the study’s results, it is important to consider its limitations. One of the limitations is that we only had access to limited registry data. The database from SiS, based on the DOK interview, does not contain registry/baseline data on an individual level regarding clients’ living conditions during their childhoods. The data are self-reported. We are using data that describe the clients’ own perceptions of whether, in their childhood, their parents had SUD and or mental health problems. This is combined with registry data on institutionalisation as a child and shows a strong correlation.
Registry data are best used to identify relationships between independent variables and the dependent variable, not to test the total effect of an entire model. The important issue here is to take note of the direction of how various independent factors were associated with the dependent variable, whether they increase or decrease the risk for repeated compulsory care for SUD.
We do not have access to a large range of variables measuring risky psychosocial childhood history. Our study focuses on three factors, identified in literature as measures of risky psychosocial childhood history.
A further limitation of our study is that we do not have any biological or genetic data to use in the analysis which limits the results of the study regarding the heritability of addiction and repeated needs of treatment.
Results
Population description
Descriptive statistics are based on 2719 subjects (see Table 1), including 1658 men (61%) and 1061 women (39%). Mean (SD) age was 36 (14) years ranging from 18 to 76 years. Non-repeaters were relatively younger compared with repeaters (36 ± 14 vs. 38 ± 13 respectively, p < 0.001). The percentage of those who had more than one LVM compulsory care episode for SUD was 38% of all clients.
Description of the population (N = 2719).
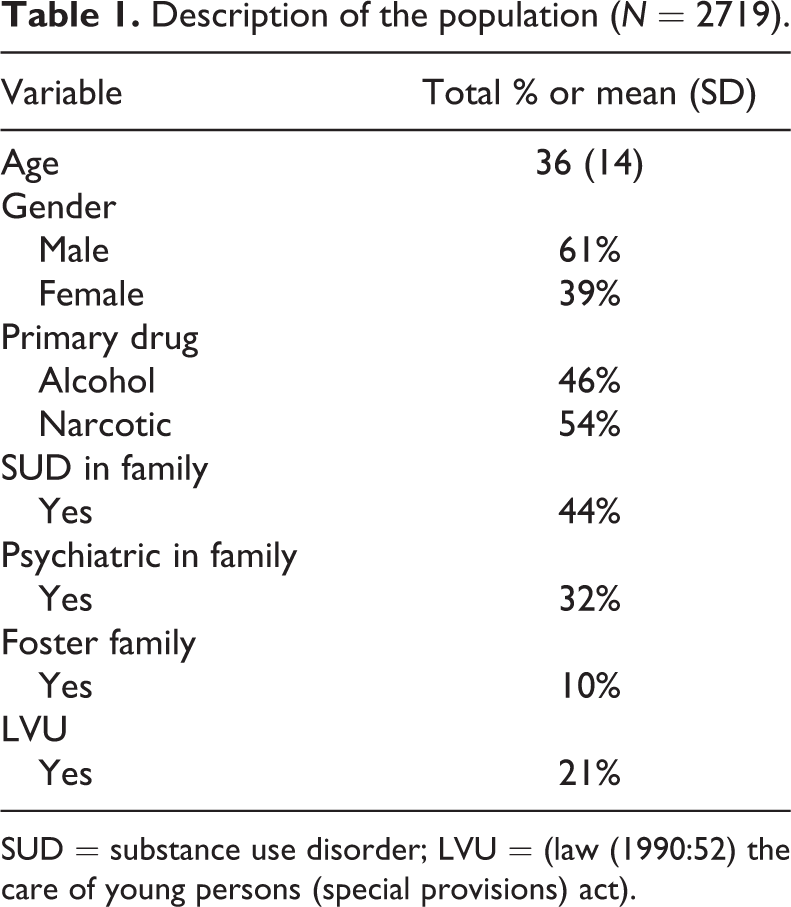
SUD = substance use disorder; LVU = (law (1990:52) the care of young persons (special provisions) act).
Predisposing factors
The clients in this study were on average 36 years old and 61% were men. Forty-four per cent of clients reported having a family with SUD, and 32% stated that there was a history of psychiatric problems in their family.
Enabling factors
Twenty-one per cent had been in compulsory institutional care for youth and 11% had been placed in foster care during their childhood and youth.
Need factors
Forty-six per cent of the clients in this study reported alcohol as the primary drug and 54% reported a narcotic as their primary drug.
Bi-variate results
The bi-variate analysis shows that a number of variables were significantly associated with repeated compulsory care for SUD (see Table 2). Specifically, it shows that clients who were older, clients whose main drug consisted of alcohol, those who grew up in a family with SUD, those who had been in foster care and those who had been in compulsory institutional care for youth were more likely to have been repeatedly in compulsory care for SUD as adults. On the bi-variate level neither gender nor psychiatric problems in the family during childhood showed a significant relationship with repeated compulsory care for SUD.
Distribution (%) of baseline characteristics by compulsory care repeaters (N = 2719).
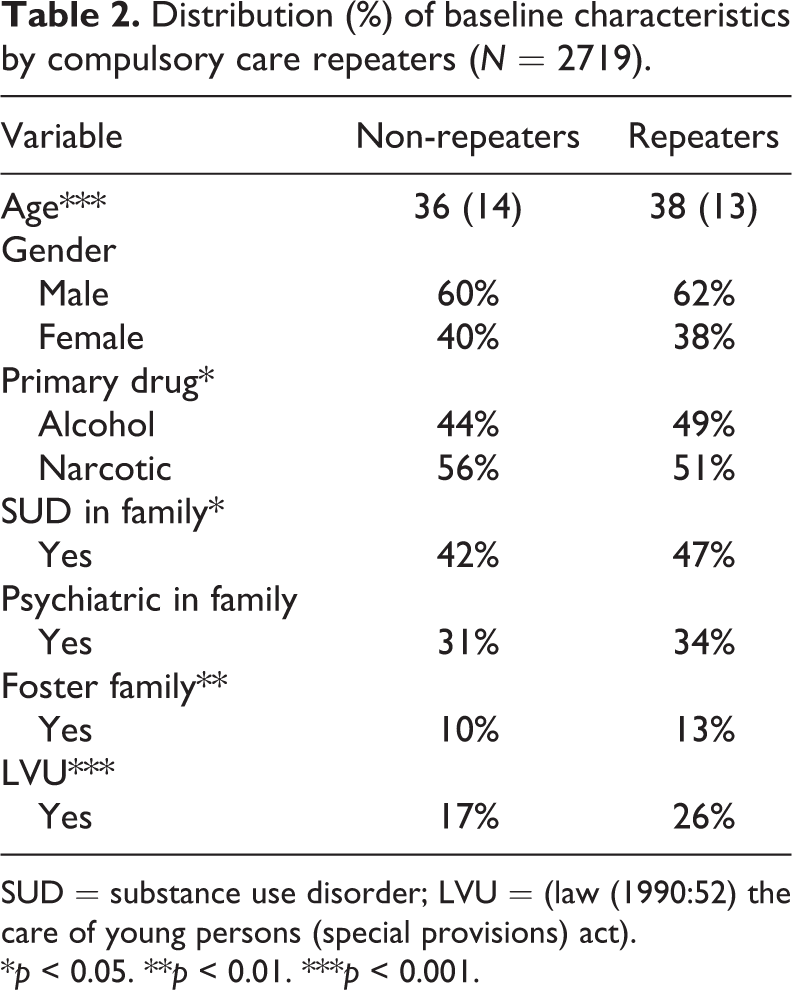
SUD = substance use disorder; LVU = (law (1990:52) the care of young persons (special provisions) act).
*p < 0.05. **p < 0.01. ***p < 0.001.
To clarify the relationship between the independent variables and the dependent variable, repeated compulsory care entries, a hierarchical logistic regression model was developed where independent variables were entered into the regression model separately in three different blocks. Specifically, age, gender and primary drug were included in Block 1 in the hierarchical logistic regression. As second step, the variables SUD in family, mental health disorder in family and having resided in foster family were included. As a third step, having been in institutional care as a child was added to the model. Specifically, we compared the relative importance of demographic and drug use factors, history of family SUD, mental health disorder and foster care, and having been placed in court-ordered compulsory care as a youth. The reason we created these three blocks was that we wanted to examine family factors separately.
Hierarchical logistic regression results
As Table 3 shows, seven variables in three blocks were used in the hierarchic logistic regression model. The first block included three variables, age, gender and main drug. Of these, only age showed increased probability for repeated compulsory care for SUD. The second block of the regression model adds the variables family with SUD during childhood, psychiatric problems in family during childhood and experience of foster care. When these six variables were included in the regression it showed that age was still a significant variable, but also to have experienced SUD within the family during childhood and having experience of foster care showed a significant relation to repeated compulsory care for SUD. In the third block of the hierarchic logistic regression model we added compulsory institutional care for youth. Two variables that showed significant association and increased the likelihood of being mandated to compulsory care for SUD repeatedly were age and having been in compulsory institutional care for youth. Note that the factor that was most strongly associated with repeated compulsory care for SUD was having been in compulsory institutional care for youth as a child or adolescent (see Table 3), which in the regression model showed the highest OR = 2.0 (1.60–2.51) to predict the likelihood of entering addiction compulsory care for SUD as an adult repeatedly (Table 3). Those who had been in compulsory institutionalised care as a youth were two times more likely to be in repeated compulsory care as adults.
Odds ratios (95% CI) from hierarchical multiple logistic regression for repeated compulsory care (N = 2719).
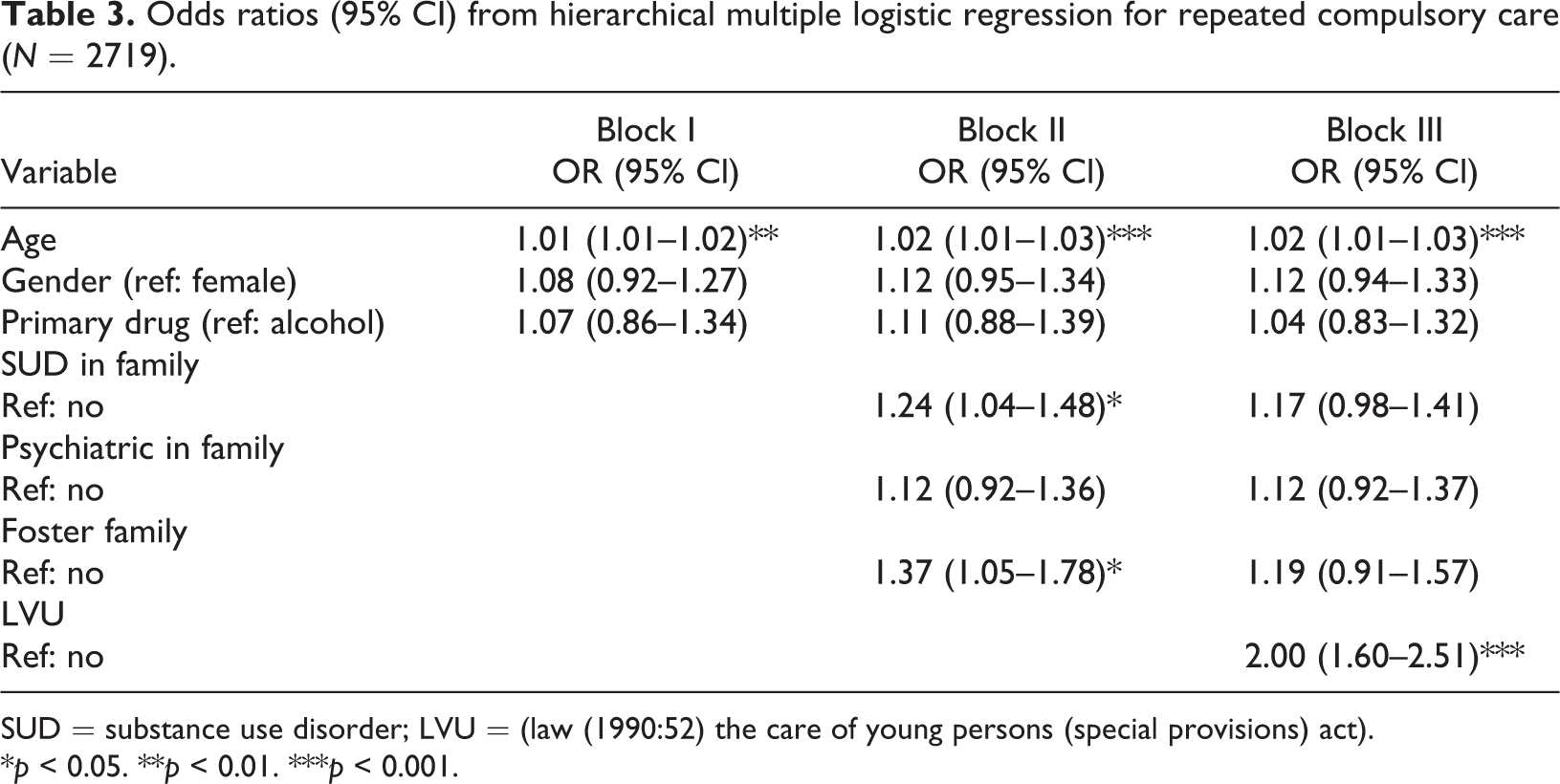
SUD = substance use disorder; LVU = (law (1990:52) the care of young persons (special provisions) act).
*p < 0.05. **p < 0.01. ***p < 0.001.
We analysed the predictor for compulsory institutionalised care as a youth (Table 4) and significant predictors were having been placed in foster care (OR = 3.95) which had the highest likelihood of being in compulsory institutional care for youth, followed by SUD in family (OR = 1.64), i.e., there were significant indirect effects of foster care and SUD in family on compulsory institutional care as a youth.
The odds ratios (95% CI) of LVU for childhood variables.
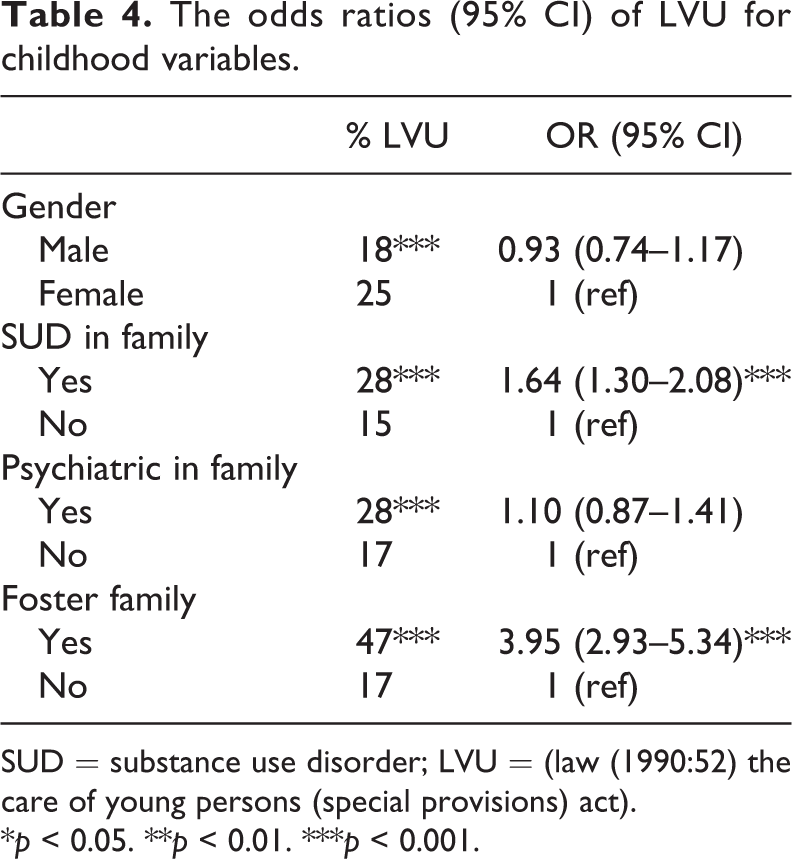
SUD = substance use disorder; LVU = (law (1990:52) the care of young persons (special provisions) act).
*p < 0.05. **p < 0.01. ***p < 0.001.
A mediation analysis (Table 5) showed that there were significant (confidence intervals do not contain zero) indirect effects of having resided in a family with SUD problems in childhood (coefficient = 0.015, 95% CI: 0.007, 0.024), having resided in a family with psychiatric problems in childhood (coefficient = 0.008, 95% CI: 0.001, 0.017) and having been in foster care (coefficient = 0.021, 95% CI: 0.011, 0.032) on the likelihood of repeated compulsory care for SUD mediated through compulsory institutional care for youth. The proportion of the total effect that is mediated through compulsory institutional care for youth was 33% for SUD problems in family during childhood, 44% for psychiatric problems in family during childhood, and 38% for having been in foster care (Table 5). In contrast, neither the direct nor the indirect effect of gender was statistically significant for the likelihood of repeated compulsory care for SUD. The direct effect of psychiatric and addiction in childhood as well as being in foster care, however, was not statistically significant (Table 5).
LVU as a mediator between independent variables and repeated compulsory care (N = 2719).
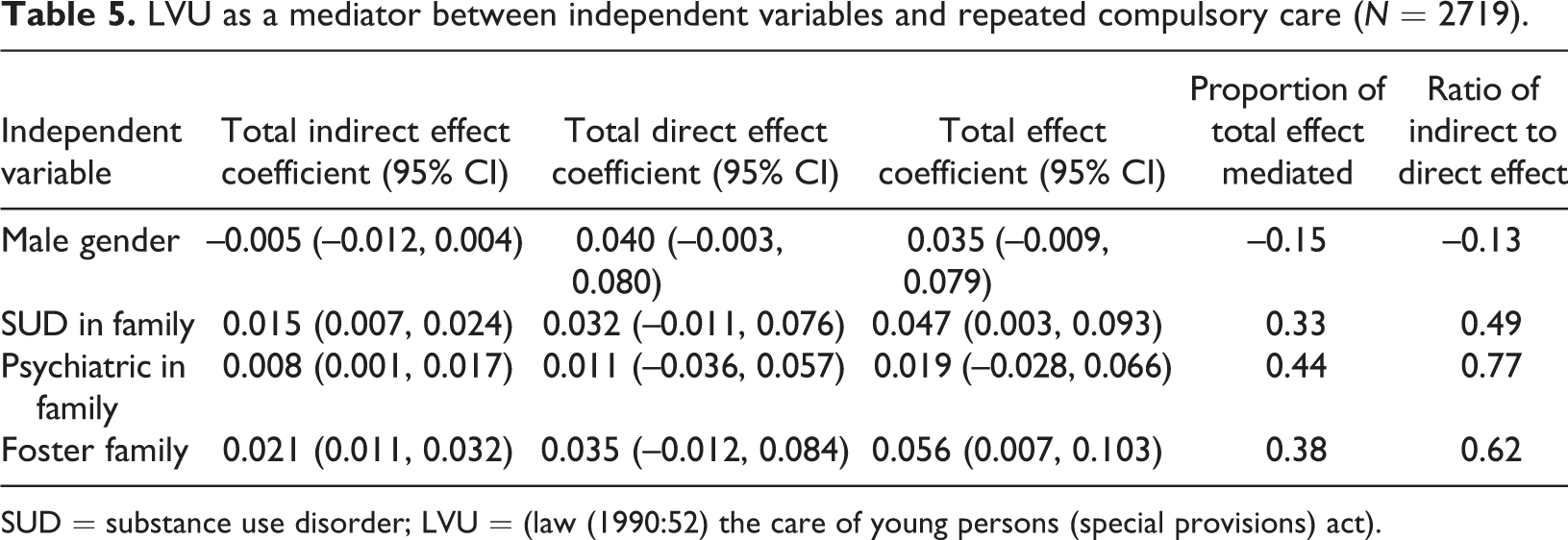
SUD = substance use disorder; LVU = (law (1990:52) the care of young persons (special provisions) act).
Discussion
This is one of few studies that identifies the statistical association between risky childhood factors (reported having a family with SUD, psychiatric problems in family, experience of foster care, and having experienced compulsory institutional care for youth) and repeated compulsory care for SUD as an adult.
Previous studies has shown that family related problems such as SUD and psychiatric problems (Alati et al., 2005; Andreas & O’Farrell, 2017; Clark, 2004; Lovejoy et al., 2000; Park & Schepp, 2015; Stone et al., 2012), and experience of institutional care and foster care (Andrews & Dowden, 2006; Dodge et al., 2006; Grahn et al., 2015) as a youth increased the risk of developing a risky substance use or substance use disorder as an adult. In the study by Grahn et al. (2015) the variable with the strongest association with repeated compulsory care episodes due to SUD was having been placed in court-ordered compulsory care as a child. These prior studies provided the argument for the need to investigate how risky childhood factors such as residing with parents with SUD and residing with parents with psychiatric problems were associated with repeated need of compulsory care for SUD.
In the study presented here, two psychosocial childhood factors, residing with parents with SUD and residing with parents with psychiatric problems, were not significantly associated with having more than one compulsory care episode for SUD. However, having parents with substance use problems, having parents with psychiatric problems and having experience of foster care, all showed significant association with been mandated to institutional care as a child/adolescent. As we can see in the mediation analysis (Table 5) we note a relationship between reporting a risky childhood psychosocial environment and a history of being placed in court-ordered compulsory institutional care for youth, which in turn is associated with repeated compulsory care for substance use disorder as an adult. This is a concerning finding in that it seems like compulsory institutional care does not mediate for childhood psychosocial risks but actually increases risk of SUD so severe that an adult is in need of repeated compulsory care for the SUD.
The results from this study can be interpreted in different ways. First, one can interpret that children of parents with SUD or a psychiatric problem were also those who had need of and were given access to care through social services and court-ordered mandatory care for youth. That is, the results suggest that the Swedish social welfare system targets the correct population in need of services. On the other hand, the results can be interpreted that the care given to these children has been insufficient to improve their situation, when there is such strong relationship between having been in court-ordered compulsory institutional care for youth, and having a need of repeated compulsory care for SUD as an adult. Finally, the results can be interpreted as the care the clients received as children was not only insufficient, it has been harmful and resulted in negative effects in the long term, such as severe SUD. Which of these three interpretations is the most likely cannot be determined based on the design of the study. However, it can be stated that the efforts made by society on behalf of the clients through court-ordered compulsory care system for youth were insufficient to create conditions for adulthood without further mandated efforts from society.
Implications for SUD treatment practice
Previous research (Dozier et al., 2014; Hansson, Hedenbro, & Centrum för utvärdering av socialt arbete unspecified Contributor, 2001; Sexton & Alexander, 2002; Weisz et al., 2013) recommends that intervention for individuals with risky substance use, delinquency or other psychosocial problems, should involve the family. Our study suggests that this recommendation may be problematic in that it is not unusual that these clients have been institutionalised as children on the basis that they were in a risky family situation, which was deemed to be unfavourable and/or insufficient for their personal development. In order to promote the client’s well-being and create opportunity for positive personal development, society has been forced to use one of the most powerful interventions there is, i.e., in the form of mandated care and removal of the child from their family. In such cases trying to use psychosocial support from family and relatives in treatment, which may be non-existent, may be insufficient and not a particularly favourable component in the design of treatment interventions for this vulnerable target group.
This study shows a population of individuals living in a highly vulnerable life situation with high levels of SUD resulting in repeated compulsory care, and after the completion of the addiction compulsory care episode probably many will continue to live with a lack of functioning social support from their families. This is important knowledge that the Swedish social services should be aware of and should take into consideration in the design of the intervention that follows after completion of a compulsory care episode for SUD. These clients are in need of interventions that take into account clients’ lack of social support and therefore interventions should include continuing care that offers expanded levels of social support from other sources. This should be given continuously during an extended time period, i.e., a treatment given over a prolonged time and addiction treatment with related psychosocial interventions and social support.
Based on our knowledge there exists a limited number of quantitative studies on the association between childhood risk factors and repeated compulsory care for SUD as an adult. Our study is one of few that identify the relationship between social background variables from the childhood and their relation to repeated compulsory care for SUD within one country, Sweden. One of the main conclusions of this study is that service factors that we defined as enabling, i.e., that were supposed to mediate against risky childhood conditions, instead may be risk factors themselves. Specifically, our mediation analysis identified that reporting having grown up with parents with SUD problems and/or psychiatric problems in themselves are not associated with repeated compulsory care as an adult. However, these factors are strongly associated with court-ordered mandated care as a youth that, in turn, is strongly associated with repeated compulsory care for SUD as an adult. The study will contribute to increased understanding for researchers, politicians and practitioners of SUD treatment through our research on a highly vulnerable population group at risk to be repeatedly mandated to compulsory care for SUD. These adults, as a group, are in need of a well-coordinated and integrated system of extensive aftercare services to reduce the likelihood of re-entry into compulsory care for SUD.
The focus of future studies may be studies based on qualitative open questions regarding clients’ attitudes about how they perceive their repeated treatment use and access to care.
Footnotes
Notes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was founded in part by the Swedish government: Statens Institutionsstyrelse (SiS Dnr 41-153-2011) and by the Umeå University Department of Social Work.