
Abstract
Aims:
Outcomes in opioid use disorder (OUD) in Nordic countries have improved with integrated treatment and harm-reduction programmes. Approaches and the standard of care are different across the region. Evidence of treatment needs and current approaches are defined from evidence to inform development of a common standard.
Method:
Evidence of population sizes and treatment approach collected. Common standards for care (harm reduction, pharmacotherapy, psychology/social therapy) defined for each country.
Results:
Evidence defines number in treatment; potential population needing treatment not defined for all countries. Populations sizes, treatment access (ratio in treatment programme compared to total country population) defined: Sweden 4,000 in OUD care (access ratio 40); Finland 3,000 (55); Norway 8,000 (154); Denmark 7,500 (132). Approach to treatment similar: integrated treatment programmes standard. Care provided by specialists in outpatient clinics/primary care; secondary care/inpatient services are available. Harm reduction is limited in Sweden but available and more accessible elsewhere. Treatment entry criteria: access relatively unlimited in Norway and Denmark, more limited in Finland and Sweden. Standards of care defined: easy access to high-quality services, individual planning, care not limited by time, management of relapse, education for patients, continuous engagement, holistic approach including management of comorbidities, needle equipment programmes without limit, treatment in prisons as community.
Conclusion:
There are opportunities to improve OUD care in the Nordics. Policy makers and clinicians can advance OUD care and share common success factors. Collaborative work across the Nordic countries is valuable. Further research in clinical practice development can yield important results for the benefit of patients with OUD.
Opioid use disorder (OUD) is associated with risk of mortality and morbidity (Dematteis et al., 2017) including adverse mental and somatic health outcomes, poor perceived quality of life, unemployment (Callahan et al., 2015), homelessness (National Alliance to End Homelessness, 2016), family disruption, social instability, criminal activities (Daley, 2013) as well as loss of economic productivity (Jiang, Lee, Lee, & Pickard, 2017). Pharmacotherapy with opioid agonist therapy (OAT) in an integrated programme with psychosocial care is proven to improve outcomes and can address the health and social consequences of OUD (Nielsen et al., 2016). Needle equipment programmes are effective in limiting harms from blood-borne viruses. Other approaches such as mutual help and Narcotics Anonymous are also important treatment options.
Sweden, Denmark, Finland, Norway, and Iceland have similar welfare and national healthcare system approaches with open access to healthcare in general. There are similarities in substance-use culture across these countries (Selin et al., 2015) and guidance for treatment of people with OUD is available in Sweden (Socialstyrelsen, 2015), Denmark (Sundhedsstyrelsen, 2017), Finland (Alho et al., 2012), Norway (Helsedirektoratet, 2016), and Iceland (SAA National Center of Addiction Medicine, 2016).
Pharmacotherapy is an established part of treatment systems in these countries (Skretting & Rosenqvist, 2010); although approaches to OUD care differ in each country. This work compares population needs and approaches to OUD care across the region to define standards for practice.
Materials and methods
A comparison of approaches to OUD care was completed; care was described by collecting evidence of relevant populations, service type and access. Evidence describing the size, access, and approach for OUD care was collected from publications of national agencies concerned with substance-use disorders and peer-reviewed publications recommended by experts in the therapy area. Evidence sources were selected in a standard manner retrieving the most recent official government data describing OUD populations. Two reviewers familiar with the field assessed the evidence sources independently and extracted relevant data. Results of the evidence collection and analysis were reviewed by experts in the field (more than 10 years’ experience in OUD care in the relevant countries). A recommendation for a standard of care was developed based on a comparison of current observed approaches across countries.
Results
Assessment was completed for Sweden, Denmark, Finland, Norway, and Iceland (Table 1).
Key studies defining opioid-use disorder (OUD) population in Nordic countries.
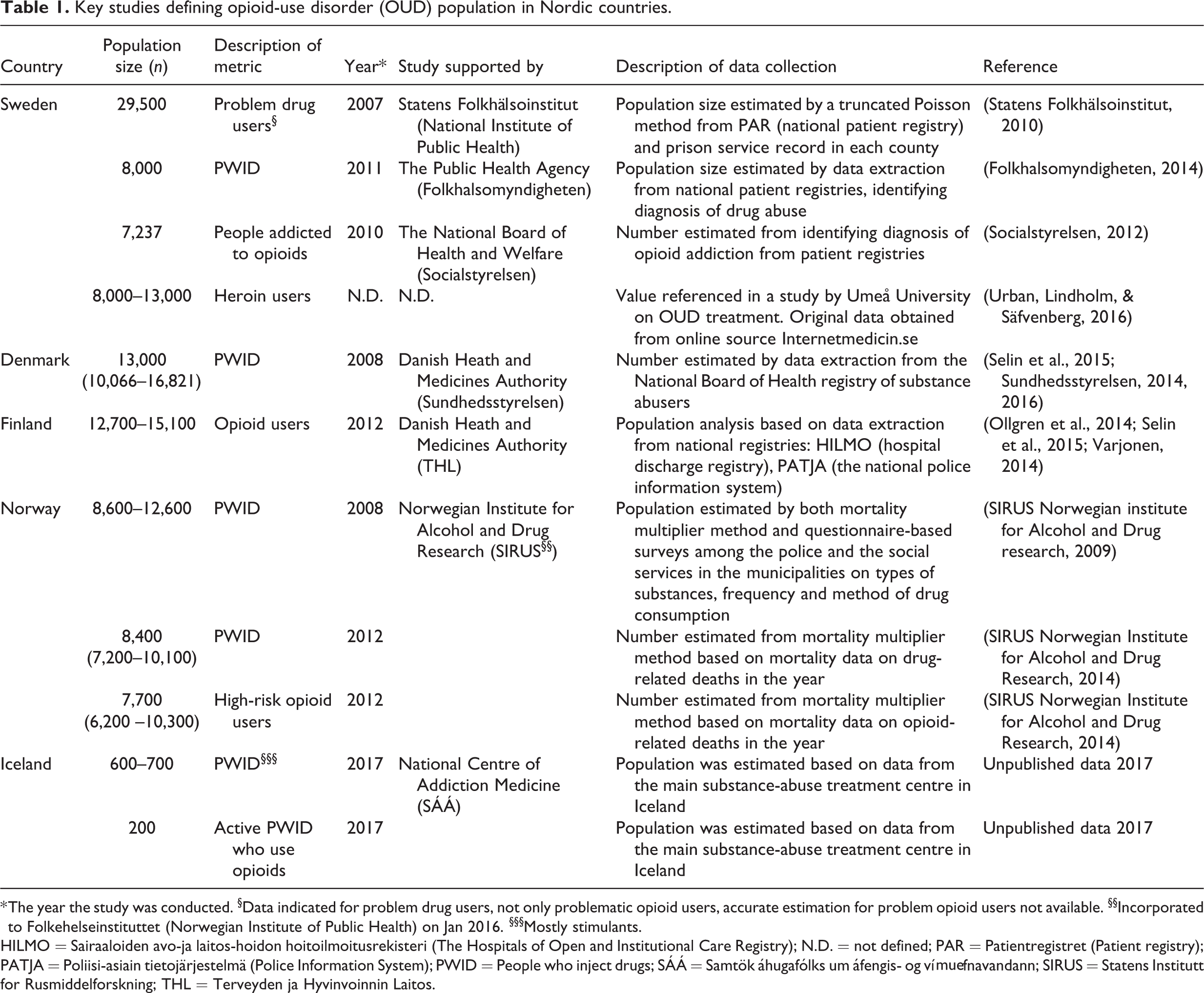
* The year the study was conducted. §Data indicated for problem drug users, not only problematic opioid users, accurate estimation for problem opioid users not available. §§Incorporated to Folkehelseinstituttet (Norwegian Institute of Public Health) on Jan 2016. §§§Mostly stimulants.
HILMO = Sairaaloiden avo-ja laitos-hoidon hoitoilmoitusrekisteri (The Hospitals of Open and Institutional Care Registry); N.D. = not defined; PAR = Patientregistret (Patient registry); PATJA = Poliisi-asiain tietojärjestelmä (Police Information System); PWID = People who inject drugs; SÁÁ = Samtök áhugafólks um áfengis- og vímuefnavandann; SIRUS = Statens Institutt for Rusmiddelforskning; THL = Terveyden ja Hyvinvoinnin Laitos.
Population treatment needs and access
In Sweden, the population with potential need for OUD care is likely 29,500, as based on national patient and prison registries (Statens Folkhälsoinstitut, 2010); other sources describe different groups within this population including point prevalence estimates of persons involved in injecting drugs and those involved in heroin use (8,000–13,000) (Folkhalsomyndigheten, 2014; Urban, Lindholm, & Säfvenberg, 2016). In Denmark, the population with potential need for OUD care is 13,000 based on the national health registry data (Selin et al., 2015; Skretting & Rosenqvist, 2010; Sundhedsstyrelsen, 2014). In Finland, the number of problem opioid users is estimated to be 15,000 based on national hospital discharge registries and the police information system (Ollgren et al., 2014; Selin et al., 2015; Varjonen, 2014). In Norway, the population of high-risk opioid users or number of injecting drug users is 7,700–12,600 (SIRUS Norwegian Institute for Alcohol and Drug Research, 2014; Skretting & Rosenqvist, 2010) based on mortality data on drug-related deaths and questionnaire-based surveys among policy and social services. In Iceland, the population of active opioid users is 200 from the main substance misuse treatment centre (unpublished data, 2017). Opioid use profiles among people with OUD differ: injected heroin use is common in Denmark (Skretting & Rosenqvist, 2010), Norway (Helsedirektoratet, 2010; Bretteville-Jensen & Amundsen, 2006), and Sweden (Skretting & Rosenqvist, 2010); illicit use of diverted buprenorphine is predominant in Finland (Selin et al., 2015); in Iceland almost all patients attending OUD treatment reported predominantly injected morphine use (Rúnarsdóttir, 2014). Relative levels of treatment engagement for the countries assessed are different. Estimated numbers engaged with treatment programmes are Norway (8,000) (Granerud & Toft, 2015), Denmark (7,500) (Sundhedsstyrelsen, 2014), Sweden (4,000) (Most recent estimate, likely an underestimated figure) (Socialstyrelsen, 2017), Finland (3,000) (National Institute for Health and Welfare Finland, 2017) and Iceland (130) (unpublished data, 2017). The index of treatment access (based on the number of patients in OUD care, annual estimate, as a ratio of the total national population, all citizens) indicates higher access to OUD care in Norway (ratio 154) and Denmark (132); access to care is more limited in Finland (55) and Sweden (40). (Iceland was not assessed due to small national population.)
Approach to treatment
The approach to OUD management is defined for each country (Table 2). The approach to OUD care is similar across the Nordic countries; treatment is based on integrated programmes of OAT medication and psychosocial therapy in the context of similar welfare and national state-provided healthcare systems. Housing and social benefits, such as long-term disability pension, may be provided when appropriate from the municipality.
Opioid-use disorder (OUD) population and treatment system in the Nordic countries.
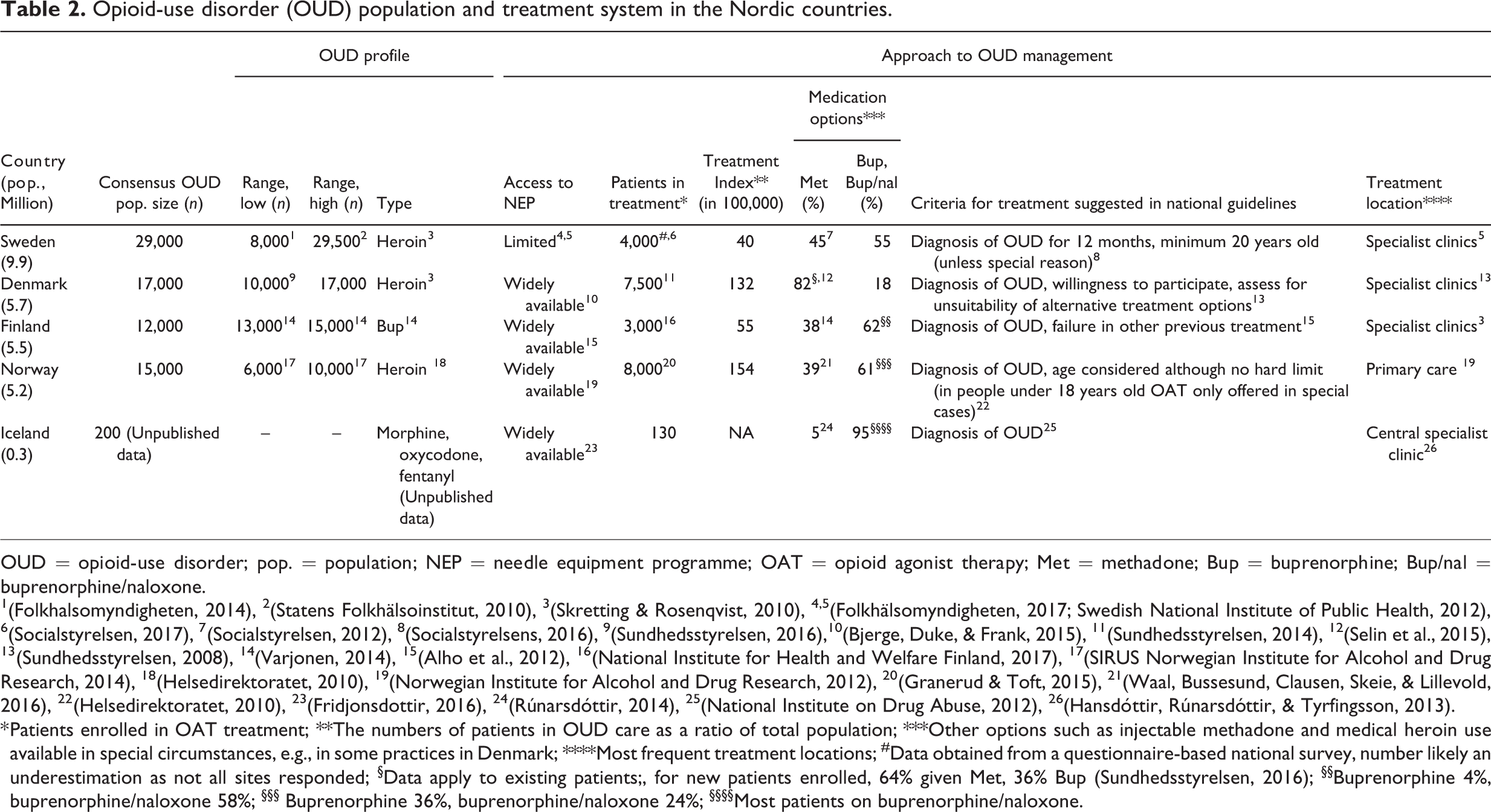
OUD = opioid-use disorder; pop. = population; NEP = needle equipment programme; OAT = opioid agonist therapy; Met = methadone; Bup = buprenorphine; Bup/nal = buprenorphine/naloxone.
1(Folkhalsomyndigheten, 2014), 2(Statens Folkhälsoinstitut, 2010), 3(Skretting & Rosenqvist, 2010), 4,5(Folkhälsomyndigheten, 2017; Swedish National Institute of Public Health, 2012), 6(Socialstyrelsen, 2017), 7(Socialstyrelsen, 2012), 8(Socialstyrelsens, 2016), 9(Sundhedsstyrelsen, 2016),10(Bjerge, Duke, & Frank, 2015), 11(Sundhedsstyrelsen, 2014), 12(Selin et al., 2015), 13(Sundhedsstyrelsen, 2008), 14(Varjonen, 2014), 15(Alho et al., 2012), 16(National Institute for Health and Welfare Finland, 2017), 17(SIRUS Norwegian Institute for Alcohol and Drug Research, 2014), 18(Helsedirektoratet, 2010), 19(Norwegian Institute for Alcohol and Drug Research, 2012), 20(Granerud & Toft, 2015), 21(Waal, Bussesund, Clausen, Skeie, & Lillevold, 2016), 22(Helsedirektoratet, 2010), 23(Fridjonsdottir, 2016), 24(Rúnarsdóttir, 2014), 25(National Institute on Drug Abuse, 2012), 26(Hansdóttir, Rúnarsdóttir, & Tyrfingsson, 2013).
* Patients enrolled in OAT treatment; **The numbers of patients in OUD care as a ratio of total population; ***Other options such as injectable methadone and medical heroin use available in special circumstances, e.g., in some practices in Denmark; ****Most frequent treatment locations; #Data obtained from a questionnaire-based national survey, number likely an underestimation as not all sites responded; §Data apply to existing patients;, for new patients enrolled, 64% given Met, 36% Bup (Sundhedsstyrelsen, 2016); §§Buprenorphine 4%, buprenorphine/naloxone 58%; §§§ Buprenorphine 36%, buprenorphine/naloxone 24%; §§§§Most patients on buprenorphine/naloxone.
Outpatient care based on similar integrated programmes of medical and psychosocial therapy is the common model for treatment of OUD in all countries (Skretting & Rosenqvist, 2010). In Sweden and Iceland, patients may be advised or required to start with inpatient care under intensive monitoring (Hansdóttir, Rúnarsdóttir, & Tyrfingsson, 2013). Criteria to enter treatment programmes described in national guidelines differ across countries. In Denmark, Finland, Iceland and Norway criteria for access to services are minimal. In Sweden, a diagnosis of OUD for at least 12 months is required for treatment entry and the minimum age for receiving OAT is 20 years old with exceptions for special reasons (Socialstyrelsens, 2016).
Choice of medication options for OUD management varies. Common choices for OAT include methadone, buprenorphine/naloxone fixed-dose combination product, and single agent monotherapy with buprenorphine. Methadone is the most common choice in Denmark (Selin, 2013; Selin et al., 2015); buprenorphine and fixed-dose combination product of buprenorphine/naloxone are widely used in Sweden (Selin et al., 2015; Socialstyrelsen, 2012) and Norway (Ding, Mosdøl, Hov, & Staumann, 2016; Selin et al., 2015). In Finland, buprenorphine/naloxone is most common: there is very limited prescribing of buprenorphine as a result of the common practice of buprenorphine misuse and diversion (Selin et al., 2015; Varjonen, 2014). In Iceland most patients are treated with buprenorphine/naloxone (Hansdóttir et al., 2013; Selin et al., 2015).
All countries operate some form of integrated needle equipment programme (NEP) for harm reduction; accessibility is high in Denmark (Bjerge, Duke, & Frank, 2015), Finland (National Institute of Health and Social Welfare, 2016), Iceland (Fridjonsdottir, 2016), and Norway (Norwegian Institute for Alcohol and Drug Research, 2012). In Sweden, access to NEP was restricted until 2017; progress has been made but access is still difficult or limited for many people (Folkhälsomyndigheten, 2017; Swedish National Institute of Public Health, 2012).
Discussion
Effective OUD treatment improves outcomes: it reduces illicit drug use and demand on the illicit drug market at individual and community levels (Dematteis et al., 2017; Sumnall, Bates, & Jones, 2017; Wodak, 2011), potentially limiting future opioid use (The National Center on Addiction and Substance Abuse, 2017). Access to long-term and sustained coverage of harm reduction interventions is associated with lower levels of risky behaviour and lower prevalence of infectious diseases (Martin et al., 2012; Strang et al., 2012; Vickerman, Martin, Turner, & Hickman, 2012).
In theory, OUD treatment is available for all citizens at no or insignificant cost in the countries assessed, all of which have similar healthcare systems. Despite this similar foundation, this work shows important differences in OUD care for Nordic countries. Access to care is different with higher levels of engagement in Norway and Denmark, and lower levels in Sweden and Finland. Entry criteria are an important determinant of this difference. Access to services to reduce harm, such as needle equipment programmes, is limited in Sweden and reduces the ability of citizens to avoid preventable risk behaviour. This access level has changed in Sweden but remains distinctly different from other countries.
This summary of the differences and similarities in OUD care across this region is the basis for a definition of a set of simple standards which should apply generally. These are described in groups considering a journey a patient might take from initial engagement to assessment and treatment: During “Engagement, diagnosis and treatment assessment”, making decisions openly and in collaboration with patients, including confirmation of the OUD diagnosis, recording all drug use, assessing somatic and psychiatric co-morbidities, and discussing treatment options are important.
Developing a treatment or management plan centred around relevant goals, tailored to individual needs, is important. This includes assessment of different starting points, risks, treatment goals, potential outcomes, with patients being well-informed on the scope of long-term care and the standards for the expected level of conduct and compliance. For treatment choice, ongoing therapy and completion, it is important to adopt an integrated approach considering elements of pharmacotherapy, psychiatric and social interventions, which is holistic and includes the management of other frequent somatic co-morbidities such as hepatitis C virus (HCV), HIV, and other mental health problems for successful outcomes. Important outcomes include control of craving, ongoing opioid and other drugs consumption, and management of somatic and psychiatric comorbidities, as well as subjective improvement of overall quality of life. Buprenorphine/naloxone, buprenorphine and methadone are common choices in pharmacotherapy: decision making should be based on a careful consideration of efficacy, safety, comorbidities, any preceding treatments, guidelines and patients’ preference and individual needs (Dematteis et al., 2017). Buprenorphine/naloxone fixed-dose combination product is recommended in national treatment guidelines as a key choice (Alho et al., 2012; Helsedirektoratet, 2010; Socialstyrelsen, 2017; Sundhedsstyrelsen, 2008). The choice of medical product should not preclude focus on planning other forms of social support such as stable housing, employment, and other meaningful daily activities that are important in promoting wider improvement in all aspects of life. At the beginning of the treatment programme, more intensive input is recommended to allow close monitoring and careful titration to ensure patients receive an appropriate OAT dose, and to minimise risks of overdose and likelihood of problems with “on top” opioid use. As treatment progresses and patients stabilise, regimens may evolve from intensive daily visits towards self-management of picking up doses from a pharmacy. An assessment for suitability of take-home medication should be implemented across all treatment services. For patients using take-home medication, it is important to ensure continuous contact with clinical professionals to help predict problems, avoid risk and relapse, minimise risk of diversion, and provide assistance if necessary. A flexible treatment plan with scope for changes, based on patients’ preferences and ongoing assessment, improves outcomes; an inflexible plan may be counterproductive. Treatment duration should not be limited based on arbitrary grounds – treatment can continue for as long as needed, with continuous support from an integrated team of stakeholders according to patients’ perceived needs for counselling and assistance. Developing a working approach with patients’ input, with regular reviews of goals and progress, offers the opportunity to educate patients to conduct self-evaluation to catch early signs of relapse and actively ask for help. Relapse is common and should be considered as part of the recovery process. Relapse can be addressed with increased intensity of planned intervention, for example more regular visits to clinics, more input from psychosocial support such as counselling and peer support. The choice of medication and dosage should be reconsidered; dose might need to be increased if there are signs of “on top” opioid use. Concomitant health problems such as psychiatric co-morbidities may need to be reassessed and treated. Some patients may complete therapy with significant support by a carefully programmed approach; careful planning of timing and assessment of patients’ motivation and decisions are important. Achieving abstinence should be planned carefully and agreed with the patient, with a thorough discussion on whether he or she is sufficiently motivated and has the personal and social stability to cope and solve problems. A pragmatic approach for both the delivery of evidence-based treatment, i.e., OAT and harm reduction, is important. Wide access to harm reduction will potentially serve as an entry point to services for those underserved for healthcare and hard to reach, and it may be a first step towards more formal care. On a practical level, access to NEP and other harm-reduction interventions should be offered without restriction. Increase in differentiated treatment options tailored to individualised needs should be considered in countries with lower participation in therapy. Examples such as primary care and NEP centres as key points of treatment entry and evaluation can be considered. Treatment should be widely available including in prisons. Prison OUD care should be the same high quality as community care. Treatment for comorbidities including mental health and HCV infection should be easily available.
This work defines the needs of populations based on available evidence describing OUD groups. It is difficult to estimate the size of populations with OUD because of the criminal nature of illicit drug use. Evidence collected here represents the best available profile of populations with OUD; population estimates and related needs for treatment can be improved with further work. An index of persons recorded in treatment compared to national country population is used. This is not ideal, and it would be more conventional to compare to total population potentially requiring treatment. The total value is not available for Sweden and introducing this figure as an estimate is problematic and likely would remove the focus from the insights to be drawn from the metric used. Research – including collaborative regional programmes with common approaches to measurement – to identify the size and types of the population needs and reasons for non-participation should be supported. Evidence on the impact of the continuing observed levels of access to treatment in OUD can be used to support future policy decisions that promote continuing access to integrated treatment with OAT. This can include comparative analysis leveraging existing similar population attributes and approaches to healthcare in general with the opportunity presented by existing pan-Nordic healthcare registries of activity and outcomes healthcare data. Insights from this research are key to making decisions about the future of OUD care aiming to achieve increased engagement to address dependence, improve overall health with management of comorbidities, quality of life and citizen participation leading to better social and family outcomes matched with reduced criminal activity and wider benefits to society.
Conclusion
Progress in OUD care and improvement in outcomes has been significant since the introduction of integrated treatment and harm-reduction programmes. National policy and practice must be optimal to ensure equity of access to services providing easy access to high-quality treatment programmes with OAT and NEP. Decision makers including policy makers, providers of services, researchers and clinicians can improve outcomes by adopting and extending observed best practice across the region.
Footnotes
Acknowledgements
The authors are grateful for the contributions of Dr Li Li and Tara Lumley in preparing analysis and editorial works.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Expert meeting attendance and support services for this work were supported by a grant from Indivior. Indivior did not influence the meeting discussion, nor the content of this review.