
Abstract
Aim:
To increase understanding of the consequences of growing up with substance-abusing parents, including how this can influence the experience of becoming a parent.
Methods:
In-depth interviews were conducted with 19 parents who had participated in an Infant and Toddler Psychiatry Unit intervention programme and who had experienced substance-abusing parents in their family of origin. Directed qualitative content analysis was used to analyse the data.
Results:
Analysis of the interview material revealed both a high incidence of parentification and a conspiracy of silence concerning the substance abuse that helped generate symptoms of cognitive dissonance in the children. As parents they experience a high degree of inadequacy, incompetence and stress.
Conclusion:
A majority of the children who had grown up with substance-abusing parents responded by taking a parenting role for themselves, their siblings and their parents. These children, often well-behaved and seemingly competent, need to be identified and offered support as they risk developing significant psychological and emotional difficulties that can extend into adulthood. They form an extra sensitive group who may need special support up to and including the time when they become parents themselves. This finding underlines the importance of further research on parenting among those who have grown up with abusive parents.
Alcohol and drug-abusing parents have shown to have clear deficiencies in their parenting role. They have difficulties in providing both functional parenting (Cronin, Murphy, & Elklit, 2016; Keller, Cummings, Davies, & Mitchell, 2008; Laslett, Dietze, & Room, 2013) and a sensitive and development-supporting relationship with their children (Suchman, DeCoste, Leigh, & Borelli, 2010). Research shows that children of substance-abusers run a high risk of developing mental health problems that negatively influence their physical, psychological and social maturation (Bakoyiannis et al., 2014; Dube et al., 2001; Edwards et al., 2017; Elkins, McGue, Malone, & Iacono, 2004; Hill et al., 2008; Kelley et al., 2005; Kelley, Pearson, Trinh, Klostermann, & Krakowski, 2011; Yule, Wilens, Martelon, Simon, & Biederman, 2013). However, there is limited research specifically concerning people who have grown up with substance-abusing parents when they become parents themselves (Wiig, Haugland, Halsa, & Myhra, 2017) and we have limited knowledge about the specific mechanisms of intergenerational transference of negative parenting style in families (Belsky, Conger, & Capaldi, 2009).
Children who have been the victims of abuse, neglect and psychological trauma reveal a higher risk of suicidal behaviour, having suicidal thoughts and/or making plans to commit suicide throughout their lives (Behr Gomes Jardim et al., 2018; Hardt et al., 2015; Park, Hong, Jeon, Seong, & Cho, 2015; Tunnard et al., 2014). Today there exists a convincing body of evidence that demonstrates the importance of the parent–child relationship for the child’s psychosocial development (Malone, Westen, & Levendosky, 2011; Sroufe, 2002; Toth, Rogosch, Manly, & Cicchetti, 2006). There is a general consensus that it is the parents’ sensitivity to their child, their ability to attune and their recognition and affirmation of the child’s communication that helps the child to develop adequate self-regulation, a sense of security and an organised attachment (Fearon & Roisman, 2017; Verhage et al., 2016).
Attachment theory and parentification
One premise in attachment theory is that the child is more likely to feel secure and to develop adequate and effective exploratory behaviour if her early experience of her parents is that they are both accessible and comforting when needed (Cassidy, 2008). When a child is raised in a home milieu where there is a high level of substance abuse, the resulting unpredictability of the parents’ behaviour means that it will be difficult to learn and develop effective strategies that reliably elicit consolation in stressful situations. Children who become stressed or anxious but who cannot turn to their parents to find the comfort needed to calm down run the risk of experiencing long periods of stress. If the parents themselves are the source of threat and danger, attempts to approach them, instead of providing comfort, may rather increase experienced levels of stress and anxiety (Bowlby, 1982; Solomon & George, 1999; Solomon & George, 2011). Such relationships may result in the child developing a chronic state of hyper-arousal containing a highly charged, negative emotional state which is difficult to manage (Howe, 2005). Over time and with increasing maturity, the child will develop her own strategies in an attempt to manage the relationship and minimalise stress. One such strategy involves the child taking responsibility in the relationship through a form of role reversal in which she herself behaves as if she was the parent, either through “compulsive self-reliance/controlling/punishing behaviour” or by “compulsive caregiving/caring and helpful behaviour” (Bowlby, 1988; Jacobvitz, Riggs, & Johnson, 1999; Solomon & George, 2011; Teti, 1999). Both sets of behaviour can be understood as a sign that the child cannot express her own helplessness and anxiety to her parents with any hope of receiving comfort and instead learns alternative ways to take care of her own needs (and/or even her siblings and parents) (Solomon & George, 2011).
Towards the end of the 1970s the term “parentification” began to be used, in the sense of “as if one’s child were one’s parent” (Boszormenyi-Nagy & Spark, 1973), and the concept has been refined and developed since then. One established definition is: …parentification in the family is a functional and/or emotional role reversal, in which a child in response to an adult’s abdication of parental responsibility, reacts by sacrificing his or her own needs for attention, comfort and guidance in order to care for the logistical, emotional and self-esteem needs of a parent. (Chase, Deming, & Wells, 1998)
Dysfunctional communication
One particular and common difficulty experienced by a child growing up in a substance-abusing family is a pattern of dysfunctional communication which takes the form of a “rule of silence” that denies the child the right to express and explore certain aspects of their cognitive and emotional experience. This rule of silence is built on the adult’s denial of the substance abuse, a denial that the whole family (and even the wider social network) complies with. This rule creates a dissonance for the child between two related elements of her experience and knowing (Dar, 2013): firstly, the actual experience of parents ingesting drugs and then being under their influence and secondly, the denial by their parents and their network that the abuse and its consequences exist (Kroll, 2004; Lorna, 2015). This silence is often part of a wider pattern of rejecting and sometimes humiliating communication from the parents towards their children which may become part of the child’s idea of self in which she becomes worthless, ugly, nasty and even stupid (Cicchetti, 2016). A child’s idea of self is primarily formed through interaction and communication with her attachment persons and a child who grows up with abuse and neglect will often experience that her parents do not like her when they refuse to affirm her – important relational messages that are easily internalised as being part of “that is who I am”. One way to lessen the despair produced by the parents’ lack of care is to create a sense of worth by taking care of others – deserving care through caring for others (Macfie, Brumariu, & Lyons-Ruth, 2015).
The child raised by substance-abusing parents becomes a parent herself
When children who have grown up under very insecure circumstances become adults and have their own children, they run a greater risk of experiencing insecurity and other difficulties in their role as parent (Byng-Hall, 2008; Haxe 2016). One of the most significant factors that correlates with the nature of an adult person’s parent role is the degree and nature of the care that they themselves received from their own parents (Anda et al., 2006; Conger, Belsky, & Capaldi, 2009; Main, Kaplan, & Cassidy, 1985; Meins, 1999; Slade, Grienenberger, Bernbach, Levy, & Locker, 2005). Another developmental difficulty commonly encountered by children raised by substance-abusing parents is that of trauma − an experience that creates difficulties for the child and eventually for the adult she becomes. Growing up in a substance-abusing family increases the risk of being exposed to traumatic experiences (Killén, 2009; Taplin, Saddichha, Li, & Krausz, 2014), and exposure to trauma is associated with problematic parenting, regardless of trauma-related psycho-pathology (Cohen, 2008). For the child, the emotional accessibility of her parents is important and studies find that it is a parent’s inability to recover from trauma, as measured by post-traumatic symptoms and inadequate caregiving behaviour, that affects the impact of that trauma on their children (Almqvist & Broberg, 2003; Lambert et al., 2014; Lehrner & Yehuda, 2018; van IJzendoorn & Sagi-Schwartz, 2008).
Studies carried out at the Department of Child and Youth Psychiatry in Malmö reveal that approximately 30% of the mothers who sought help at an Infant and Toddler Psychiatry Unit had been brought up in families with substance-abusing parents (Tedgård & Råstam, 2016), and many had been the victims of abuse and neglect (Tedgård, Råstam, & Wirtberg, 2018). An earlier clinical report from an Infant Mental Health Unit in Malmö, Sweden, describes how mothers who had grown up with substance-abusing parents experienced more difficulties in relation to their infants than mothers who had not grown up under such circumstances (Tedgård, 2008). The offspring of parents with serious substance-abuse problems face, as described above, an accumulation of risk factors because of biological, psychological, social and environmental vulnerability. However, remarkably little is known is about the challenges and perspectives experienced by children of substance abusers when they themselves become parents (Wiig et al., 2017). The present study contributes to this area by exploring the experience of men and women who grew up with one or both parents having an active substance-abuse problem and who then became parents themselves.
Aim of study
The aim of the present study is to gain a deeper understanding of and insight into the experience and consequences for children who grow up with substance-abusing parents, including how this can influence the process of them becoming parents. The research questions were focused on two themes: firstly, how they experienced their parents’ substance abuse and how it influenced them and secondly, how they experienced the psychosocial situation and their own parenting to small children, with their background of growing up with substance-abusive parents.
Materials and methods
Subjects
The sample consisted of 19 parents participating in an infant mental health intervention programme in a specialised outpatient infant and toddler psychiatric clinic. The programme had two basic components: the first focused on the interaction between parent and child during which the parents are encouraged to become attentive to the child’s emotions and contact initiatives, and the second was psychotherapy for the parent. From a total sample of 197 parents, screened at the beginning of the intervention through self-reports for sociodemographic and psychosocial data concerning physical and psychological health and substance abuse in the family of origin and traumatic life events (Tedgård & Råstam, 2016), a sub-sample of 53 reported that they had grown up in a family with substance-abusing parents. From the sample that reported growing up with substance abuse, 29 parents who had concluded treatment within a certain time frame were consecutively asked if they would consent to participate in the present study. Four parents declined due to lack of time and a desire not to revive painful memories and two were not reachable by telephone. Twenty-three people agreed to participate and of those, four did not show up for their interview without giving a reason. The final sample consisted of 19 informants (13 mothers and 6 fathers) whose children were between 1 and 5 years old at the time of the interview. None of the participants were partners with each other and none of the participants had received treatment from or had previous contact with the psychologist (ET) who carried out the interviews. Those interviewed had earlier participated in a larger study which included the total sample (Tedgård & Råstam, 2016): this study shows that rates of attention deficit and hyperactivity disorder, depression and own substance abuse are greater amongst mothers who had grown up in a home with substance-abusing parents and that they are also generally a more vulnerable patient group within infant and toddler psychiatry.
Methods
A qualitative approach was designed to explore the interviewees’ perceptions of their childhoods with substance-abusing parents. The participants were invited by letter that also contained information concerning the study. A week later they were contacted by telephone and asked if they would like to participate. All participants were informed that none of the information obtained would be identifiable as belonging to any specific individual and that the ethical rules that applied to the information gathered would be followed in accordance with the ethical approval that was obtained from the Regional Ethics Committee at Lund University, Sweden. All participants gave their written consent. In consideration of the possibility that some of the informants might experience problems after the interviews all were offered the opportunity to be referred for further counselling. One of the participants used that opportunity. The participants were compensated with two cinema tickets for study participation.
Measures
The methodological approach was qualitative – using in-depth interviews – and the focus was on describing and understanding the life stories told at the interviews (Hyden, 1997; Launer, 2002). A semi-structured interview guide was used in order to provide the freedom to access as many different areas as possible while at the same time ensuring that everyone was asked the same key questions. The guide contained retrospective questions about experiences from childhood that included family climate, relationship to parents, network and school. There were also questions concerning the present, and these included the experience of their own parenting. The informants were free to express themselves and to associate in different directions to the open-ended question and efforts were made to obtain small narrative examples that illustrated the answers in order to enhance understanding. The interviews lasted from 90 to 150 minutes. Each interview was tape-recorded after obtaining permission from the informant. Before beginning the data analysis, the interviews were transcribed verbatim.
Many of the questions concerned the subjects’ pasts. When asking people to recall their past there is usually no way of controlling “the facts”. The data collected are accepted as the memories and experiences these women and men have of their childhood and upbringing. It is further assumed that their recollections of historical events recalled in response to the retrospective questions of the interviewer are influenced in some ways by the narratives they have in the present (Kvale & Brinkmann, 2009).
Data collection
The in-depth interviews were conducted after the families had finished the treatment at the Infant and Toddler Psychiatry Unit from May 2012 to June 2013.
Data analysis
Directed qualitative content analysis (directed QCA) was used to identify, classify and code the themes and patterns of the interview data (Graneheim & Lundman, 2004; Hsieh & Shannon, 2005; Sandelowski, 2000). With Directed QCA, an analysis starts with a specific theory or with relevant research findings that are used as guidance for the initial codes that are selected (Graneheim, Lindgren, & Lundman, 2017). In this study the research findings presented in the introduction were used as a starting point. Directed QCA differs from more conventional qualitative methods (e.g., grounded theory) in that it is more structured and involves both inductive, deductive and adductive approaches (Krippendorff, 2013; Pisarik, Rowell, & Currie, 2013). Directed QCA does not prioritise a search for deep implications, but rather aims to present a thick description of the informants’ own stories (Graneheim & Lundman, 2004; Hsieh & Shannon, 2005). The inductive approach, also called data-driven (Schreier, 2012) or text-driven (Krippendorff, 2013), is characterised by a search for patterns. During the analysis, based on answers containing thoughts, feelings and memories as described in the texts, the researcher looks for similarities and differences in the data, which are described in categories and/or themes on various levels of abstraction and interpretation. Keeping as faithful as possible to the data is considered crucial, even if all analysis infers some degree of interpretation. The researcher moves from the data to a theoretical understanding – from the concrete and specific to the abstract and general (Graneheim et al., 2017). Using a deductive approach, also called concept-driven (Schreier, 2012), researchers test the implications of existing theories or explanatory models about the phenomenon under study against the collected data.
After careful reading of all the interviews several times, the text was − with an inductive starting point − divided into “meaning units”, which are those parts of the texts that relate to the aims of the study. All meaning units were then condensed, while care was taken to preserve the original content. The condensed meaning units were given codes. The codes were then grouped into sub-categories and thereafter to mutually exclusive categories, depending on similarities and differences in content. The emerging categories were then closely examined and discussed by the research team and reorganised until consensus was reached. Finally, we searched across categories to identify recurring regularities that could be expressed as themes. The first author (ET) performed the analysis throughout the whole analytical scheme, and the last author (IW) participated in all steps after the coding process. The analytical process had a continual back-and-forth movement between the emerging categories and the original parts of the text in order to secure trustworthiness and a comprehensive understanding of the material. In addition to the inductive analysis of the transcribed interviews, items from the “Parentification Questionnaire” (Jurkovic & Thirkield, 1998) were used to analyse the same interview material so that the theoretical method (directed QCA) was complemented by a more deductive approach in order to obtain a more complete understanding by analysing specific aspects of the material – for example their experience of role reversal regarding responsibilities in the family. Examples of the items that were applied to the interview material include: “In my family I often made sacrifices that went unnoticed”; “I often felt more like an adult than a child in my family” and “At times I felt I was the only one my mother or father could turn to”. This approach implies continually moving back and forth between inductive and deductive approaches − from theory to data and back again (Graneheim et al., 2017).
Results
Subjects
The informant’s social context
At the time of the interview and as parents to small children, most of the subjects had succeeded in creating a functional and organised lifestyle in which they followed daily routines and were able to earn their own living. At the time of the interview, all but two had steady jobs, all had their own home, just over half had finished secondary school and six had completed university studies. Thirteen lived with the other biological parent to their small child. For further sociodemografic and psychosocial data see Table 1.
Sociodemographic and psychosocial characteristics of the sample (n = 19).
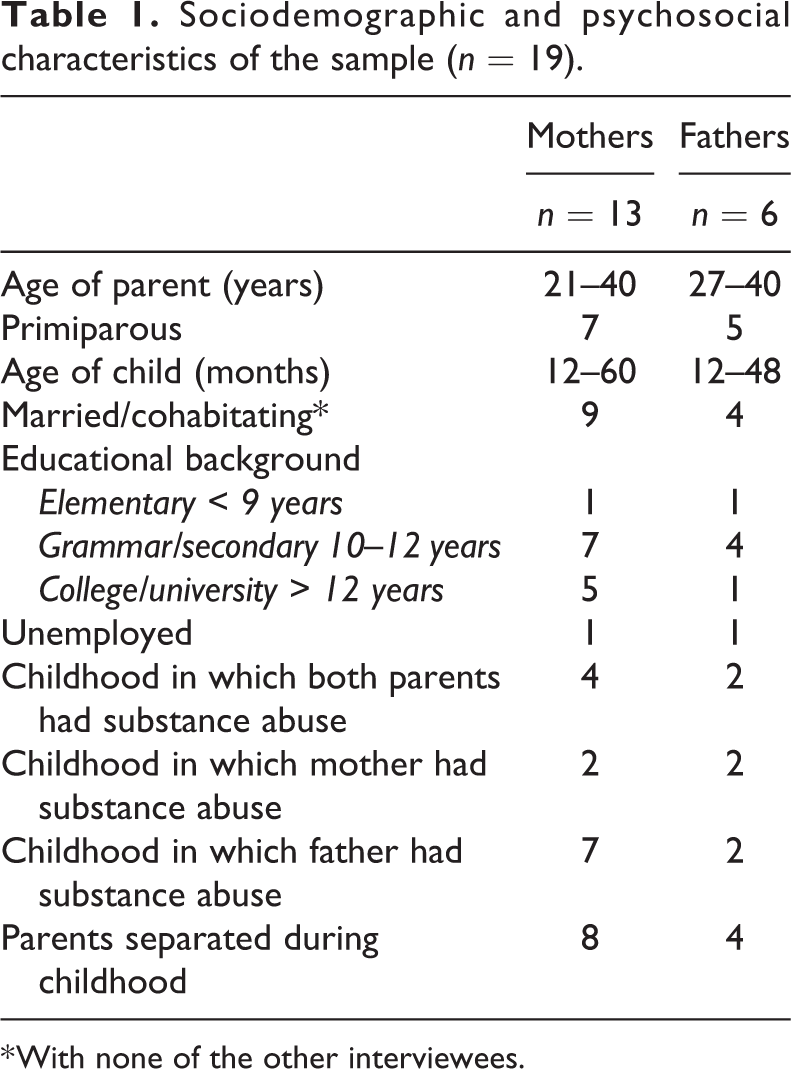
* With none of the other interviewees.
Our results describe data from the in-depth interviews. The material is organised into two major themes: the first is entitled “Descriptions of and reflections on my own upbringing” and the second “Reflections on my own parenting”. Without exception, those interviewed described how they were strongly influenced in their thoughts and their behaviour by their parents’ substance abuse, both when they were children and even now as parents. Their answers mixed together descriptions from the past and the present and it was often difficult for them to distinguish between their childhood experiences and their present experiences.
Theme 1: “Descriptions of and reflections on my own upbringing”
This major theme is sub-divided into 10 categories: (1) Fear; (2) Lack of love and affirmation; (3) Taking the role of a parent, (4) Inadequate self-preservation strategies; (5) Culture and conspiracy of silence; (6) The lack of support from the social network; (7) Difficulties with trust – difficulties asking for help; (8) Being drawn into drug abuse themselves; (9) Low self-esteem and denial of feelings; (10) Reflections on the possible cause of their parent’s abuse.
Fear
The most common descriptions provided by the interviewees told how parents often behaved in very hostile ways. Many described frightening and threatening situations in which for example some became physically paralysed, some cried, whilst others got stomach-ache. Yes, Dad was violent, mostly towards Mum, so one was scared that he would really hurt her, and he got really angry at me if I tried to rescue Mum, or protect her. (A mother) Sometimes they got really crazy when they fought a lot, honestly, for me it was like life and death at times. (A mother)
Several who had substance-abusing fathers, described how their father’s abuse seemed to paralyse their mother so that she was neither physically nor emotionally available to take care of them. A minority decribed that they were able to turn to one of their parents in order to gain some comfort.
Lack of love and affirmation
Most of those interviewed said that they did not believe that they were loved by either or both of their parents. They felt that they were neither understood as individuals nor affirmed for the responsibility that they often took in the family. A majority experienced this lack of understanding and affirmation from one parent, and almost half experienced it from both. I wasn’t at all close to either of my parents, if there was something that one wanted, one didn’t go to them. Instead one just kept silent about what one wanted and it disappeared after a while. (A father)
Taking the role of a parent
A large majority of the interview subjects described that during their childhood their role was to look after, care for and forgive their parents. They descibed a kind of role reversal in the family. They felt that they had to manage difficult situations when they happened and be a parent to themselves. I felt lots of times that I had to be my parent’s parent. Dad threatened to commit suicide, and I had to grab hold of him when I was five, and mum just stood there to one side. I had to stand between them when I was a kid and it isn’t a very pleasant memory. (A father) When I went to junior school, Dad started to talk with me more and more about my younger siblings, and about how to raise kids and other adult things. I was the one who tried to figure things out and be an adult, to be the one who could make everyone feel secure. (A mother) I had the role of taking care of Dad. I had to put him to bed and see that he slept with his head high when he was drunk so that he would not choke if he was sick. I was a very little girl when I had to start taking care of Dad, when really it should be the other way around. (A mother)
Inadequate self-preservation strategies
More than half of those interviewed had very poor self-preservation strategies and others described symptoms of dissociation as a means of escaping from their unmanageable life situations. They also described difficulties in understanding and managing their own feelings and most said that the dysfunctional family context made them feel very bad and that they suffered from different types of mental disturbances during their childhood. Several also described how they put themselves in dangerous situations during their childhood – for example by sitting in a dumpster and setting it on fire, jumping off a high bridge or by cutting themselves. Just over a third began to practice substance abuse in their early adolescence.
Half described strong feelings of anxiety and/or depression which in a few cases led to suicidal thoughts and even suicide attempts. I felt that I couldn’t talk with Mum, so I just sat and cried the whole night, like I couldn’t talk with my friends either because I was the big strong one, but when I needed help I didn’t dare ask. The first time I tried to take my life I was thirteen and on a school trip. Then we were sent to Child Psychiatry, but then I said I was never going back, and Mum couldn’t force me to. (A mother)
Culture and conspiracy of silence
Most of the interview subjects told about how difficult or even impossible it was to talk about their parents’ substance abuse. It was something that was always present, but which could not be put into words. Even if there was no official or explicit ban in the family about talking about the substance abuse (as it could not be talked about) the informants experienced strongly that it was a forbiddden subject. Dad knew about Mum’s substance abuse but despite that he denied it all the time, but he knew about it alright. But he just pretended that it didn’t exist, that was rule number one. We all pretended it didn’t exist, so it didn’t exist. (A mother)
Lack of support from the social network
A majority of those interviewed stated that they had not told anyone about their home situation during their childhood and that they had no-one at all with whom they could talk about their parents’ substance abuse. They felt there was a definite lack of support from their relations or their neighbours as few adults in their social network − apart from some school staff − reacted at all to their vulnerable situations. The subjects described how they had felt a desperate longing that someone would offer them support so that they could feel less abandoned. Only two subjects came to the attention of the the Social Work Services and received support from them. However, almost all enjoyed positive relationships with some peers during their childhood, even if there were also periods when they were isolated and became the victims of bullying. Engaged school staff members became significant and positive people for almost half of those interviewed, and in turn this meant that school became, in comparison to their home, something of a safe haven and that they were also able to finish their time at school and pass their final exams. These school staff members offered pedagogical support that made attending school easier − and in some cases even made it possible. On the other hand, however, no one offered any of the children the chance to talk about or get help for their parent’s substance abuse.
Nine of the informants described how organised leisure activities gave them positive experiences and valuable relationships outside of their home. This positive aspect was missing from the descriptions of those who experienced their school years only as a difficult and problematic period. Instead, they described how they were together with peers who exerted a negative influence, and were engaged in different destructive practices. When I was thirteen I had to have my stomach pumped, I had over 0.4 per cent alcohol. I was bathing in the park, I nearly drowned. (A mother)
Difficulties with trust – difficulties asking for help
When the interviewees reflected over their upbringings, several of them stated that they had difficulties in trusting people – a difficulty they saw as a consequence of their primary caregivers being so unreliable. All of the broken promises made by their parents as well as their obvious inability to change their lifestyle had left their mark on the informants. For some, lack of trust meant that as parents they could not rely on the abilities of either official childcare services or their friends to help them to take care of their children. For a large majority of the informants, a second set of reflections described how difficult it could be to ask for help, both when they were children and even now as adults and that this was connected to the fact that they had never talked with anyone about their home situations. They also described how difficult it was for them as children to understand just how dysfunctional their families were as they had nothing to compare them with. It was only later as adults that they could examine their childhoods at least in part from an outsider’s perspective and reacted with both anger and despair at what it had been like. Even though the very few supportive adults with whom they had had temporary relationships during their childhood had apparently no idea of the degree of the substance abuse in the family, they were still viewed as positive exceptions. Most of the informants decribed how, as children, they were exposed to dangerous situations without any kind of protection and had to take care of themselves and only now when they looked back could see that they had been forced to be parents to themselves. With a kind of shock, they could now as adults understand that they had never had the chance to be children. She left us, just wrote a note on the kitchen table, “I can’t manage any more, I have to get away”. Then we four kids woke up in the middle of Malmö without any mother, with just a note on the table. She is never going to be a part of my child’s life, she is not his grandmother. (A mother) I have watched my heavy substance-abusing parents and forgiven them everything…my biggest problem now is that I am the sort of person who cannot ask for help. (A mother)
Being drawn into drug abuse themselves
Just over one-third of the 19 people interviewed described that they themselves had had a serious substance abuse beginning in their early teenage years. When they reflected on this, they had difficulties in understanding and explaining for themselves how they were drawn into the world of drugs despite the fact that they did not want to be. Mother’s drug abuse influenced me so that I was unconsciously drawn into a hash-world that I didn’t really want to be in, but it was something new, something forbidden, something that one was curious about. It reminded one so very much of another person that one doesn’t want to be…(A mother) I was thirteen when I started to smoke hash. Yes, it was just before I got to know that Dad was on drugs. I used to wonder why he just disappeared, but I didn’t know why. Then I got the answer. (A father) Dad’s drug abuse made me miserable and angry, I got fed up with everything and couldn’t understand how he could carry on like he did. But then you sit there yourself in the same kind of situation, you get there yourself, but you didn’t realise it at the time. (A mother)
Low self-esteem and denial of feelings
Those interviewed described how they felt shame, denied their own feelings and had other great difficulties during childhood which they could still experience in varying degrees in the present. They also stated that their experience of substance-abusing parents made them feel “crushed”, “traumatised” and often left them “without feelings”. As adults they described a self-image marked by low self-esteem, and a sense of uncertainty and insecurity often coupled with a denial of feelings – all of which they attributed to their abusive upbringing. They also described ambivalent feelings of love and hate and felt that their parents had betrayed them. When asked how they were personally most affected by their parents’ abuse most of the subjects came back to the fact that the absence of supportive adults meant that they were forced into becoming premature adults very early and how they had tried to obtain the love of their parents by playing the role of a parent. I was loved if I made myself lovable – there was always the threat of being disowned. I forgave them every single time – there was no other choice. (A mother) I became really tough. I made everything impossible for Mum. When she was intoxicated I refused to lift a finger. When she was really drunk and collapsed in a heap outside she asked me for help. But I said no. I was thirteen and just stood and looked when she tried to crawl to a park bench to lift herself up. I was really tough. (A father) I wanted to kill myself very early. Now I didn’t do it as I had the feeling that there was no point. There wasn’t any reason for me being here. Now, as a mother, I know that I can do good things, but I can’t feel it. I can’t act on my feelings, only on what I know is right from using my common sense. (A mother)
Reflections on the possible cause of their parent’s abuse
Most of those who were interviewed had speculated as to why their parents abused drugs and a few of them stated that they had tried as adults to confront them, but the answers they had been given had not led to any real clarity. In one case this attempt had instead resulted in breaking off contact with the parents. Those interviewed explained their parents’substance abuse in different ways and the most common explanations were that their parents had experienced severe trauma and/or had lived in a cold emotional climate either as children or as young adults. From this perpective, the substance abuse was thought of as a way of “escaping” from difficult feelings – a means of “anaesthetising their pain”. One-third saw their parent’s substance abuse more as the result of an illness that was caused by physiological and genetic factors and as such was impossible to influence. For others, drug abuse was a consequence of the weak or reckless and uncaring personality that their parents possessed. A few lacked any kind of understanding or explanation as to why their parents had been active drug-abusers during their children’s uppbringing. Dad had a tough time in his family. He had it tough with his parents who also came from a tough background. My grandfather was an alcoholic, my Dad and all of his brothers are alcoholics. So there is something there. Something was crazy and completely wrong in his family, and I don’t really know what it was. (A mother) My parents didn’t know any better, my Mum lost her parents when she was a child and my Dad was physically abused at home. When I got my own child, I confronted my Dad and told him what was wrong and what he had to change, but he didn’t dare, so he stopped having contact with me. (A father)
Theme 2: “Reflections on my own parenting”
Under this theme, three categories are identified: (1) Experienced danger and traumatic events, (2) Motives for seeking treatment, (3) Difficulties with own parenting.
Experienced danger and traumatic events
All of the informants reported that they had experienced threatening or traumatic events both as children and as young adults and described how these events had influenced them in different ways as the parents of small children, even though they had happened a long time ago. Almost all of the the traumatic events that were described involved threats of violence and actual violence directed against them personally, in which they were physically beaten or were the victim of sexual abuse or rape. For half of the interviewees such traumatic events were carried out by their substance-abusing parents.
The interviewees described how the effects of traumatic events had been reinforced after they had become parents themselves and had responsibility for a defenceless child. The trauma that they had experienced meant that they were continually alert for possible danger, above all in relation to their child, which meant that they had difficulties in interpreting their child’s signals in a sensitive, nuanced way. It could also result in them acting in an over-protective manner towards the child and thus limiting the child’s world of possible experience.
Motives for seeking treatment
The interview subjects all experienced a high degree of stress and inadequacy in their role as parents and identified these feelings as being strong motives for seeking help from the Infant and Toddler Psychiatric Unit. The most common symptoms were feelings of incompetence, guilt and a sense of being socially isolated − by which they meant that they had no-one to whom they could turn for support and advice. They expressed the desire to be completely different as parents in comparison to how their own parents had been. When they began the family-therapy-based intervention at the unit, a majority described that they still suffered from the symptoms they had experienced when they were growing up (mostly anxiety, but also depression) and that those feelings negatively influenced their parenting. Four described how they had been in psychotherapy before they sought help in the programme offered by the Infant and Toddler Psychiatric Unit. I didn’t want to have a child at all, I absolutely didn’t want the baby when I was pregnant, had not intended to have a child ever. (A mother) There was a feeling of inadequacy in being a parent, that I could hurt my baby or even anyone, with my anxiety. (A mother) I got a post-partum deprssion and moved to a mother–child institution, then I came here and that was the start of my long journey to becoming a mother. It took two years. (A mother)
Difficulties with own parenting
The majority of the subjects said that they experienced being a parent as being very difficult. They described a high degree of stress, lived with strong feelings of anxiety and experienced perceived threats and dangers everywhere, which resulted in them being over-protective of their children (Tedgård et al., 2018). They also expressed the desire to have control as parents which meant that they wanted to be able to see in advance what would happen with their child, which was very problematic. They described that it was difficult to trust the people around them, whilst at the same time they were conscious of how important it was for their child’s sake to be able to display trust. A couple of the parents expressed the desire to prepare their children to be able to “cope with difficulties”. Several of the parents described a conflict they had between always wanting to be available for their child, whilst at the same time needing to be able to take care of their own needs. Such contradictory experiences created conflicts within the parents, resulting in emotional outbursts that were difficult to control, followed by paralysing feelings of guilt that were coupled with the fear that their child would not like them anymore. One parent told how her strong anxiety attacks could prevent her from being together with her child for long periods of time, despite her best attempts to be present and available. A couple of parents said that they deliberately waited a long time – until they were in their forties – to have chidren, as they did not feel mature enough earlier. The single, most important desire amongst all of those interviewed was to have the ability to give to their own children that which they themselves had not been given in their own childhood – and a little more if possible. When you have baggage with you from your childhood you always have to think and analyse just a bit extra as to why I do this and avoid other things. It’s a strong motivation to have her [n.b. daughter] and want to be able to protect her from the kind of things that you have been through yourself. (A father) I don’t hit my children, but I do shout at them. I don’t trust anyone to take care of my kids – everything is dangerous. I always want what’s best for the children. (A mother) I don’t want my son to be too namby-pamby. Then he will never be able to survive. I was a bit too sensitive myself when I was younger, got angry too easily. (A father) Feel like a bad mother – my kid won’t eat – I get really furious. Sometimes I just want her to disappear. (A mother)
Discussion
The goal of the present study was to explore what it was like for the subjects to grow up with substance-abusing parents and in what kind of ways that experience had influenced them. They were also asked to describe the psychosocial aspects of their own family situations at the time they applied for treatment. This was done by interviewing a group of patients who had participated in a family-therapy intervention at an Infant and Toddler Psychiatric Unit. The findings are discussed here, organised thematically.
Emotional parentification
The results confirmed those of earlier studies that being brought up by parents who are substance abusers is often connected with abuse and neglect (Jääskeläinen, Holmila, Notkola, & Raitasalo, 2016; Osborne & Berger, 2009; Raitasalo & Holmila, 2017). Almost all of those interviewed described how they had been the victims of emotional abuse with repeated threats, humiliating treatment, and the absence of love and affirmation. The subjects described how such a difficult family situation resulted in them feeling abandoned as their parents’ needs were always more important than their own. The absence of their parents’ emotional support contributed to their childhood experiences of insecurity, of difficulties in being able to trust their network and of poor self-confidence. They offered many examples describing the lack of space available for their own emotional needs and the majority developed emotional parentification strategies in their families which involved behaving in capable and competent ways and assuming responsibility for what were really adult tasks and responsibilities. For a child, emotional parentification is an especially difficult burden because she considers her parent’s emotional and physical wellbeing to be her responsibility – and this is a commission that is beyond her capabilities, but one that at the same time she cannot refuse (Haxhe, 2016). Most of those interviewed described how they had been the victims of neglect and dysfunctional parenting and how their social network offered no sign of being aware of what was happening. Possibly, their misery may have been masked by the children’s apparently capable and competent behaviour. Being aware of the compulsive caregiving strategy that children living in such families may assume means that it is important to be on the look-out for it. A child who takes on an emotionally parentified role wants and intends to be helpful and empathic – but at the cost of ignoring her own needs. In comparison to those children who assume a controlling/punishing strategy and who try to control their parents and their environment through the use of aggression, an emotionally parentified child does not act out and behave in a dramatic manner (Solomon & George, 2011). A number of studies have shown that parentified children run a risk of developing internalised problems both in preschool (Macfie, Houts, McElwain, & Cox, 2005; Sroufe, Egeland, Carlson, & Collins, 2005) and in their teenage years (Byng-Hall, 2008; Mayseless & Scharf, 2009; Shaffer & Egeland, 2011). The parentified role’s two contradictory sides were clearly expressed when the interview persons described how they paid a high price for their “competence” and were left with feelings of emptiness, despair and anxiety – which in some cases led to serious suicide attempts.
Another way of describing the situation of the interviewees arises from their reflections on why their parents were substance abusers. The majority of their explanations freed their parents from responsibility to a large degree, defining them instead as being victims of circumstance. As victims, they could not be held responsible for the personality changes that accompanied intoxification or for the frightening and unmanageable situations that were the result of substance abuse. To think of their parents as people who were not responsible for their actions may also be a part of the caretaking, parentified role which a majority of the interviewees had developed.
Cognitive dissonance: “The elephant in the room”
A child who grows up in a family where the parents are substance abusers runs the risk of not only being the victim of abuse and neglect but also of a dysfunctional form of communication which generates cognitive and emotional difficulties − typically in the form of a “culture and conspiracy of silence” in which the child is “gagged” so that she is rendered unable to talk about the difficulties in the family. The substance abuse itself may be likened to an important “family member” who casts a long shadow over the family and is exceedingly visible to the child, but whose existence is denied by the parents (Kroll, 2004; Lorna, 2015). Silence and denial may have a negative influence on the child’s internalised image both of her family and of herself. Many of those interviewed described how they were often afraid while growing up, a fear that could be generated for example by a threatening and drunken parent, or for the experience of being abandoned. Some, however, described that they did not feel fear − even when they knew that the situation they were in was in fact dangerous.
For the child, the ability to differentiate which of all of the perceived, potential threats are in fact dangerous has to be learned in the context of everyday life. This is done through social referencing (Klinnert, Emde, Butterfield, & Campos, 1986; Walle, Reschke, & Knothe, 2017) in which the parents’ response to the jointly perceived event signals the necessary information to the child to help her distinguish which potential threats are in fact perceived as dangerous even to her parents and which are not.
Parents who are substance abusers and who deny their addiction with a “culture and conspiracy of silence” that effectively gags anyone else’s attempts to talk about it and who also insist on ignoring catastrophic events, cannot be anything else than misleading teachers when it comes to explaining their own behaviour and the child’s experience of them. As a result, the communication pattern of denial will create distortions in the child’s cognitive maps of − and thereby their emotional response to − the world. The parent who denies or does not comment on dramatic events that occur in the family makes it difficult for her child to understand what has happened (Staf & Almqvist, 2015) and to be able to trust her own perception. If the parent says nothing, then the child is left to her own devices to make sense of and manage overwhelming and frightening experiences that may result in the child assuming responsibility for what has happened and even blaming herself. As a consequence, the child then might become alienated from herself or develop other types of dissociated states (Byun, Brumariu, & Lyons-Ruth, 2016; Dutra, Bureau, Holmes, Lyubchik, & Lyons-Ruth, 2009; Narang & Contreras, 2005; van IJzendoorn & Schuengel, 1996). There is an increased risk that existence will be thought of as being both uncertain and complicated and several of the interview subjects described how poor they were at protecting themselves, often placing themselves in situations of extreme danger as was noted earlier. It is noteworthy that all of those interviewed had been victims of traumatic events, often in the form of violence or sexual abuse. Their childhood experience − coupled with the conspiracy of silence − may have resulted in distortion of their perception of the world, for example that they became frightened of the wrong things, whilst being unable to identify and protect themselves from real dangers. It is known that children who do not receive adequate help to identify and prioritise their own needs run a greater risk of developing inadequate strategies to take both emotional and physical care of themselves and that children who have been the victims of emotional abuse run a higher chance generally of developing risk-filled behaviour (English, Thompson, White, & Wilson, 2015; Kendall-Tackett, 2002; Oshri, Sutton, Clay-Warner, & Miller, 2015).
Threats to the interviewees’ budding parenthood
One goal for this study was to obtain information about the interview subjects’ psychosocial situations as parents to small children. They lived as parents of small children in a lifestyle that functioned in many ways, with a home, work and relationships. However, they experienced the role of being a parent as an emotional burden with many difficulties. They wanted to be a totally different type of parent than their own parents had been for them, but at the same time they really had no idea of what that could be like in practice.
Several described how it was either too difficult for them to seek help when they were growing up, or that they did not in fact know that they needed help. But now, as parents for the first time, they felt it was possible to turn to The Infant Mental Health Unit for support as it was their children and not themselves who were the primary beneficiaries.
Their feelings of inadequacy were often reinforced by accompanying symptoms of anxiety and depression (Tedgård & Råstam, 2016) which are both known factors that influence parenthood in negative ways (Creswell, Cooper, & Murray, 2015; England & Sim, 2009; Murray et al., 2011). The unpredictable nature of bringing up a small child tended simultaneously to both stimulate anxiety and to increase the desire to have more control. This is in contradiction to a child’s need for parents who are flexible and are able to attune to and follow her initiatives. A child’s natural progression towards independence and autonomy can be very trying, and the inability to predict and control the child’s behaviour can re-awaken the parents’ own feelings of helplessness (Möhler, Resch, Cierpka, & Cierpka, 2001).
All of those interviewed had suffered trauma, as well as the experience of having a substance-abusing parent, either as children or as young adults and this is something else that can make the experience of parenting more difficult. Several studies show how traumatic events can influence parenthood (Appleyard & Osofsky, 2003; Bailey, DeOliveira, Wolfe, Evans, & Hartwick, 2012) by, for example, increasing parenting distress (Cross et al., 2017) and by influencing the affective communication between parent and child in a negative way (Lyons-Ruth, Yellin, Melnick, & Atwood, 2005; Thakar, Coffino, & Lieberman, 2013). Other studies have demonstrated a higher rate of both internalised and externalised symptoms for mothers who have been exposed to trauma (Babcock Fenerci, Chu, & DePrince, 2016) and an increased risk of child abuse (Kalebić Jakupčević & Ajduković, 2011). The subjects also described how they had difficulties in identifying and prioritising their own needs, yet another factor which can complicate parenting. A child needs a parent who can take care of herself and satisfy her own needs for, for example, sleep and food. Such an ability is important both from the perspective of being a secure attachment person and being a positive model for the child.
If one has grown up with an adopted parentified role, as most of those interviewed had, then this is also likely to influence becoming a parent in a negative manner. Studies show that mothers who have had a parentified role as a child may find it difficult to show warmth for and acceptance of their child’s emotional signals and have difficulties in accepting that their child is a unique individual who needs help and support from her in unique ways (Dearden & Aldridge, 2010; Nuttall, Valentino, & Borkowski, 2012).
Implications: The importance of detection and support
Growing up in a family in which one or both of the parents is a substance abuser is a reality for about 350,000 children in Sweden (Hjern & Mahnica, 2013). It is of great potential importance that the professional network (including primary care, psychiatric care, social services and school services) are able to detect and intervene in the difficult lives these children lead (Afzelius, Ostman, Rastam, & Priebe, 2018), and to understand more clearly the kind of emotional pressures a child experiences, it is necessary to explore what kind of responsibility she takes upon herself in the family, the nature of the expectations the parents have of her, and in what kinds of situation the child behaves in a more mature way than can normally be expected of a child of the same age (Haxhe, 2016).
There is a growing body of knowledge concerning the transgenerational transference of neglect and abuse (Berlin, Appleyard, & Dodge, 2011; Dixon, Browne, & Hamilton-Giachritsis, 2005; Smith, Cross, Winkler, Jovanovic, & Bradley, 2014), which suggests that it is important that primary care, social services and infant mental health are equipped to offer supportive interventions to parents who have themselves been the victims of abuse and neglect during their own childhoods.
In the treatment of parents who have grown up with substance-abusing parents, three goals are of considerable importance: the creation of a trustworthy alliance, to help the client to identify and accept her own needs and feelings, and to teach strategies for affect regulation. Treatment should also focus on reducing feelings of shame and creating an atmosphere in which it is possible to talk openly and freely about substance abuse and its effects so that it is possible to examine specifically how their parents’ abuse has influenced them (Kroll, 2004; Mackrill, Elklit, & Lindgaard, 2012). It is also important to assist them in developing a critical assessment of their parents’ way of being parents (Howe, 2005) and to help them to be able to grieve over their own lost childhoods. Another challenge is to help the new parents to find a balance between seeing and following their child’s initiatives and at the same time being able to handle their own loss of control. Treatment should also explore and strengthening their expectations about their ability to parent successfully (Jones & Prinz, 2005).
People who have grown up with substance-abusing parents often benefit from being encouraged to reflect over their childhood experience in order to understand it. Their experiences of different kinds of abuse, which perhaps never were talked about or recognised in the family, need to be understood and worked through. The ability to reflect is not necessarily a skill that we are born with and it has even been proposed by Peter Fonagy that it is a skill that we develop in interaction with our primary caregivers (Fonagy, 2003). Psychotherapy may also help an individual to develop the skill. This is important as studies show that the ability to reflect over one’s own childhood and make sense of one’s parents’ intentions greatly increases the possibility of helping one’s own child to achieve a secure attachment (Fonagy, Steele, Steele, Moran, & Higgitt, 1991; Steele & Steele, 2005).
Limitations
Qualitative research has its own built-in limitations, and it is not possible to draw any specific causal conclusions between difficulties experienced in the family of origin and an individual’s own difficulties. However, the stories told offer a nuanced picture of individual experience. When interviewing the people who participated in this study about their past, we obtain subjective narratives of a childhood as it is remembered after as many as ten or twenty years have passed. This introduces an uncertainty concerning the “objective” or “true” nature of the information received, but at the same time it is this very information that the informants themselves use to try and make sense of their present situation. As noted earlier, when asking people to recall the past there is usually no way of controlling “the facts”. The data collected are accepted as the memories and experiences these women and men have of their childhoods and upbringings. It is further assumed that their recollections of historical events, recalled in response to the retrospective questions of the interviewer, are influenced in some ways by the narratives they have in the present (Kvale & Brinkmann, 2009). There is an ongoing critique on how valid such data are (Widom, Raphael, & DuMont, 2004) whilst other studies support the use of retrospective data from childhood (Hardt, Vellaisamy, & Schoon, 2010).
Given the number of persons who were approached and the actual numbers who participated in the study there could be a selection bias. However, it might be considered reasonable to assume that at least some of the people who refused to participate did so because of difficult childhood experiences, and that their reason for not wanting to be interviewed was because they did not wish to reflect over painful childhood memories.
A further limitation concerns the bias of the interviewer, who has worked for many years as a psychologist and psychotherapist in the infant and toddler mental health intervention programme from which participants were selected. This means that, as a result of her experience, the interviewer had preconceptions concerning the nature and construction of the parenting role, something which may have influenced the choice and nature of follow-up questions in a context where treatment and research perspectives may influence each other.
Conclusions
Children who grow up with substance-abusing parents run the risk of being severely affected by a family life characterised by the absence of love, by a culture and conspiracy of silence and by serious breaches of care including psychological and physical violence and other forms of trauma. Children react differently in such contexts, and it is important to offer support to children who come from such backgrounds even if they do not offer any significant displays of externalising/internalising behaviour. The present study identifies that when the interviewees were children, support from the mental health services was inadequate and often non-existent. In reality, only a few were offered any form of support despite the fact that all of them were raised under difficult and inadequate conditions and several developed serious psychological symptoms. Recently published studies show that such problems tend to remain over time (Afzelius, Plantin, & Östman, 2017; Systembolaget, 2017), which suggests that it would be of value to discover these children early in order to offer the possibility of meaningful help, as this could lessen their suffering.
Children who appear on a cursory examination to function well because they behave in an apparently competent and capable manner may in fact have simply developed a strategy which is their best attempt to have some control in their extremely difficult situation – and to get some degree of closeness to their parents by taking care of their needs and feelings, rather than their own. These children run a high risk – both during childhood and later in life – of being affected with mental health problems, and when they themselves have children their own struggle to become parents may be severely complicated by high levels of parenting stress, anxiety and depression. The present study contributes to this area with valuable knowledge concerning this group of invisible children and underlines the importance of further research on parenting among those who have grown up with substance-abusive parents.
Footnotes
Acknowledgements
The authors gratefully acknowledge the parents who participated in the study. The authors thank Bill Petitt for excellent translating assistance and Professor Anders Möller for valuable and elucidative help concerning the methodology.
Ethics
All procedures performed in the present study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Skane Region County Council, Lindhaga Foundation and Johan Olsson Foundation.