
Abstract
Aims:
Combined use of alcohol with drugs elevates risk for problems including injury and driving while intoxicated. We assessed contributions of heavy drinking (5+ drinks for men/4+ for women), drug use (cannabis and other drugs) and simultaneous co-use to DSM-5 alcohol use disorder (AUD) and drug abuse (DA). We expected co-use to increase risk for AUD and DA.
Methods:
Using population-weighted data from adults in the 2014–2015 National Alcohol Survey who had never been to treatment (N = 3386 drinkers, 50% male, 13% Hispanic, 11% Black, mean age 45 years; N = 439 drug users, 56% male, 20% Hispanic, 15% Black, mean age 36), we tested hypotheses using logistic regression adjusting for demographics, family history of alcohol problems and impulsivity.
Results:
Ten percent of drinkers and 26% of drug users met criteria for mild AUD; <1% of drinkers and 4% of drug users met criteria for DA. Heavy drinking significantly increased risk for AUD, as did monthly or weekly use of cannabis. When simultaneous co-use was added, increased risk associated with cannabis use was reduced to non-significance. Weekly cannabis use, weekly use of other drugs and simultaneous drug and alcohol co-use were associated with significantly elevated risk of DA. In bivariate analyses, simultaneous co-use was associated with significantly greater endorsement of each of the separate AUD and DA symptom domains, including alcohol craving, tolerance and withdrawal, as well as drug and alcohol social and physical health problems.
Conclusion:
Healthcare providers should screen for simultaneous co-use of alcohol and drugs to help identify patients who may benefit from substance abuse treatment.
The developmental literature shows that alcohol and drug use trajectories are related (Pape, Rossow, & Storvoll, 2009; Schulenberg & Maggs, 2002; Wiesner & Windle, 2004). Combined use of alcohol with drugs elevates risk for problems including injury and for other high-risk behaviours such as driving while intoxicated (Cherpitel, 1999; Subbaraman & Kerr, 2015). Whether these substance use behaviours are primarily related through a unifying externalising tendency or whether they are indicative of a high-risk “deviance proneness” pathway eventually leading to development of alcohol use disorder (AUD, Chassin, Sher, Hussong, & Curran, 2013) is not always readily apparent. For example, driving under the influence of alcohol or drugs is strongly associated with impulsivity and sensation-seeking (Luk et al., 2017), and this behaviour also fits the criterion of “hazardous use” (getting into situations during or after drinking that increase risk of injury) under the American Psychiatric Association’s diagnostic criteria for AUD (American Psychiatric Association, 2013).
Externalising behaviours have long been linked together in problem behaviour clusters, particularly among youth (Buu, Dabrowska, Heinze, Hsieh, & Zimmerman, 2015; Donovan, Jessor, & Costa, 1988; Donovan, Jessor, & Jessor, 1983). Problem behaviour theory (Jessor, 1991; Jessor & Jessor, 1977) emphasises those behaviours that are socially constructed as problematic or undesirable, and which typically are socially controlled or discouraged by conventional norms. This theory acknowledges that only part of a behavioural tendency is due to personality; interactions with the social environment, including peers and parents, also are of paramount importance. The use of multiple substances might be due to common psychosocial risk factors, as well as more biological factors, such as the chemical nature of the substances or neurological changes causing use of one substance to lead to use of another (Jackson, Sher, & Schulenberg, 2008; Ozburn, Janowsky, & Crabbe, 2015).
Clustering of externalising behaviours has been widely studied among adolescents and young adults, and some work has emphasised the interrelationships of behaviours such as heavy alcohol use and drug use into adulthood. Lifecourse models underscore key developmental transitions such as achieving higher education, marriage and childrearing (Mortimer & Shanahan, 2003) that often signal change from youthful behaviours (such as binge drinking or petty crime) to more adult behavioural patterns. These adult behaviours often still include alcohol use, although typically at lower levels than earlier in the lifecourse (Mulia et al., 2017; Mulia, Tam, Bond, Zemore, & Li, 2018; Muthén & Muthén, 2000; Williams, Mulia, Karriker-Jaffe, & Lui, 2018). Use of cannabis or other drugs remains more stigmatised and socially controlled in adulthood (Falk, Yi, & Hiller-Sturmhöfel, 2008), but this may be changing in countries like the US that have moved toward legalisation of recreational use (Han et al., 2017; Kerr, Lui, & Ye, 2018).
Unifying theories of addiction emphasise the commonalities in the sensation-seeking behaviours and pathophysiologies associated with alcohol and other substance use disorders (Ozburn et al., 2015). There are a wide variety of diagnostic criteria for these disorders, which range from indicators such as hazardous use or social problems due to use to physiological symptoms of dependence such as increased tolerance, inability to stop using and withdrawal upon cessation of use (American Psychiatric Association, 2013). If there are certain levels and patterns of substance use that are not strongly associated with criteria for substance use disorders (SUD), then those alcohol and drug co-use behaviours indeed may be indicative of a more benign externalising tendency. However, if there is a strong association of particular alcohol and drug co-use patterns with indicators of SUD, then the behaviours may be important warning signs that merit clinical attention. Using US data from a national sample of adults who have never been to alcohol treatment, we examine relationships between heavy drinking, drug use, and co-use with symptoms of SUD, specifically those for alcohol use disorder and drug abuse.
Problematic patterns of use
Not everyone who drinks alcohol also uses cannabis or other drugs, and there also are people who use cannabis or other drugs without using alcohol. Despite a growing acceptability of cannabis use by some demographic sub-groups, particularly youth and young adults (Keyes et al., 2011), some still consider any use of substances such as cannabis during adulthood to be indicative of problems that merit attention. These views are due, in large part, to the associated health consequences of cannabis use and potential for addiction (American Society of Addiction Medicine, 2012), as well as evidence of an increased risk of development of other types of substance use disorders, including AUD, associated with cannabis use (Blanco et al., 2016).
Among people who use multiple substances, certain patterns of use appear to be more problematic. Prior work has documented relationships of simultaneous (at the same time) and concurrent (use of both substances during a given time period, such as a year, but not at the same time) use of alcohol and cannabis with drunk driving, social consequences and alcohol-related harms in US general population samples of adults (Midanik, Tam, & Weisner, 2007; Subbaraman & Kerr, 2015). In the 2000 National Alcohol Survey (NAS, N = 7612), simultaneous use of alcohol and cannabis was related to increased social consequences, depression and alcohol dependence compared to outcomes among drinkers who did not use cannabis (Midanik et al., 2007). People who simultaneously used alcohol and cannabis were younger, less well educated, less likely to have a partner, and had heavier drinking patterns (Midanik et al., 2007). A more recent analysis of the 2005 and 2010 NAS (combined N = 8626) showed that simultaneous use was the most detrimental use pattern: compared to alcohol only, simultaneous use approximately doubled the odds of drunk driving, social consequences, and harms to self (Subbaraman & Kerr, 2015). The magnitudes of differences in problems remained when comparing drunk driving among people who simultaneously use alcohol and cannabis to people who only use concurrently (Subbaraman & Kerr, 2015). People who are under the combined influence of alcohol and cannabis may be more likely to make decisions leading to intoxicated driving than people who are only under the influence of either alcohol or cannabis (Claus et al., 2018). Importantly, among individuals who used both cannabis and alcohol, simultaneous use was almost twice as prevalent as concurrent use, suggesting that this may be an important issue for further study.
Study aims
To build on prior work on co-use of alcohol and cannabis, our primary aim in this study was to assess contributions of heavy drinking, drug use and simultaneous co-use of alcohol with one or more drugs to DSM-5 alcohol use disorder (AUD) and drug abuse (DA). Our primary hypothesis was that, controlling for level of use of the primary substance and other known risk factors, including family history of alcohol problems (Salom, Williams, Najman, & Alati, 2015) and impulsivity/sensation-seeking (Hittner & Swickert, 2006), co-use of alcohol and drugs would be associated with increased risk for both AUD and DA in a sample of adults who had never been to drug or alcohol treatment. Limitation to people without a history of treatment was important because co-morbid substance use problems are highly prevalent in treatment samples (Gossop, Marsden, & Stewart, 2002; Ogborne, Kapur, & Newton-Taylor, 1992); this sub-group also has higher levels of clinical SUD severity than would be expected in a general population sample. A secondary aim was to assess associations of simultaneous co-use of alcohol and drugs with different diagnostic criteria for AUD and DA. Limited associations of co-use with indicators of hazardous use or social problems due to use would suggest this behaviour may be primarily an indicator of a more general externalising tendency, but robust associations of co-use with different criteria indicating physiological dependence would suggest this behaviour may be an important indicator of clinical risk.
Methods
Data
Data were from adults in the cross-sectional 2015 US National Alcohol Survey (NAS). In brief, the NAS is a nationally representative survey of the non-institutionalised adult (aged 18 years and older) population. The survey includes targeted oversamples of African Americans and Hispanics, the country’s two largest racial/ethnic minority groups. Interviews were conducted in 2014 and 2015 with landline and cellular telephone respondents selected through random digit dialling. The Institutional Review Boards of the Public Health Institute, Oakland, CA and ICF, Inc., Fairfax, VA (the fieldwork agency) approved all data collection protocols. The cooperation rate (proportion of confirmed eligible people who participated in the survey, N = 7071) was 59.8%. Survey methods are described in detail elsewhere (Karriker-Jaffe, Greenfield, & Kaplan, 2017). Datasets and codebooks from the US National Alcohol Survey Series can be requested here: http://arg.org/nas-datasets/.
For this secondary analysis, the key inclusion criterion was past-year substance use. Among those respondents with data on both alcohol consumption and drug use (N = 6469; 91.5%), past-year drinkers were those who had at least one whole alcoholic beverage in the prior 12 months (N = 3840; 59.4%), and past-year drug users included people who reported using marijuana or another recreational drug (including heroin, amphetamines/methamphetamines, prescription drugs such as opioid painkillers not used as prescribed, or any other drug) at least once in the prior 12 months (N = 626; 9.7%). The analytic sample was restricted to respondents who had never been to treatment (no history of either formal help-seeking nor informal aid such as mutual help groups) for an alcohol or drug problem. Two sub-samples were included: 3386 people who reported drinking in the past year and who had never been to treatment and 439 people who reported past-year drug use and who had never been to treatment (454 past-year drinkers, 11.8%, and 187 past-year drug users, 29.9%, were excluded due to a history of treatment/help-seeking). The two samples were not mutually exclusive, and respondents who indicated use of both alcohol and another drug in the past year were included in both sub-samples.
Measures
Among drinkers, the primary outcome was past-year alcohol use disorder, AUD, based on criteria in the 5th edition of the American Psychiatric Association’s Diagnostic and Statistical Manual (American Psychiatric Association, 2013). There are 11 symptom domains: failure to fulfil role obligations; drinking despite social or interpersonal problems; drinking when physically hazardous; giving up important activities; spending a lot of time getting alcohol, using or recovering from use; tolerance; using more than or for longer than intended; persistent desire to cut down/control use; drinking despite physical or psychological problems; withdrawal; and craving. Varying levels of severity are defined for mild (symptoms in 2–3 domains), moderate (4–5 domains) and severe AUD (6 or more domains). We used an indicator of symptoms in two or more domains (versus one or none), indicating at least mild AUD in the past 12 months.
Among people who used drugs, the primary outcome was past-year drug abuse, DA. This was indicated by at least one of three work, social or health problems due to drug use: lost time from work due to drug use, got in a heated argument while using drugs, and felt drug use was becoming a serious threat to physical health. This definition is more consistent with the prior edition of the American Psychiatric Association’s Diagnostic and Statistical Manual (American Psychiatric Association, 2000), which emphasised use despite social or interpersonal problems as a key indicator of drug abuse.
Measures of past-year substance use included alcohol, cannabis and other drug use. Alcohol use was indicated by the frequency of heavy drinking and, in the AUD models only, the maximum number of drinks consumed on a single day in the past 12 months. Heavy drinking was defined based on the number of days drinking five or more drinks for men and four or more drinks for women in the past 12 months, consistent with the guidelines issued by the US National Institute on Alcohol Abuse and Alcoholism (National Institute on Alcohol Abuse and Alcoholism, 2005). The frequency was derived from graduated quantity–frequency questions about how often specific quantities of alcohol were consumed on a single day, starting with “12 or more drinks”, then specifying “at least 8 but less than 12 drinks”, “5, 6 or 7 drinks”, and so forth down to one drink (Greenfield, 2000). This approach is highly effective for capturing occasional heavy drinking (Rehm et al., 1999). Frequency of heavy drinking ranged from 0–365 days (M = 16.8, SD = 51.6 in the sample of drinkers and M = 35.6, SD = 66.7 in the sample of people who used drugs). The maximum number of drinks was coded into categories ranging from none (in the sample of people who used drugs) to eight or more drinks on a single day. Frequency of cannabis use and frequency of other drug use were categorical variables with response options coded as never (referent), less often than every month or two, every month or two, or at least weekly in the past 12 months. Other drug use included “prescription drugs not taken as prescribed, recreational drugs or illegal drugs”, with separate questions assessing any (vs. no) use of heroin, prescription painkillers, and uppers/amphetamines/methamphetamines. Simultaneous co-use was assessed separately for cannabis, heroin, painkillers, and uppers (including amphetamines and methamphetamines), but small sample sizes precluded analyses of simultaneous co-use with alcohol by type of drug. Thus, simultaneous co-use of alcohol and drugs was included as a dichotomous indicator (no simultaneous use vs. simultaneous co-use of alcohol with at least one other drug at least once in the past 12 months).
Demographic control variables included age (continuous) and gender (female as referent). Race/ethnicity was coded using non-exclusive indicators for Hispanic/Latino ethnicity, Black/African American race, and Other race (in AUD models only), with “only White/Caucasian” as the effective referent for the AUD models and “not Hispanic or African American” as the effective referent for the DA models. Education was coded using indicators to compare those with a degree from a four-year college or university (referent) with those who had a high school diploma or less and with those who attended some college or technical school; due to small sub-sample sizes, these lower levels of education were combined into a single indicator of “less than a college degree” in the DA models. Income was coded using indicators for having a household income in the prior year at or below $50,000 and for missing income data, compared to having an income above $50,000 (referent). Family history of alcohol problems was coded using non-exclusive indicator variables for having a biological parent and/or other biological relative who is/was a problem drinker or alcoholic. We also included a score on a four-item scale of impulsivity/sensation-seeking (Cherpitel, 1999), with higher scores indicating greater impulsivity (range: 1–4; M(SD) = 0.92(0.72) for current drinkers and 1.25(0.71) for people who used drugs).
Analyses
We used adjusted logistic regression models to examine associations of alcohol use, cannabis use, other drug use and simultaneous co-use with past-year AUD and DA, controlling for demographic characteristics of respondents. Analytic samples were limited to those not missing data on the covariates (N = 2857 current drinkers (84.4%) and N = 388 drug users (88.4%)). Analyses incorporated sampling and non-response weights, so that the results were representative of the US adult population at the time of data collection. Additional analyses used design-based F-tests to assess bivariate associations of simultaneous co-use of alcohol and drugs with the specific symptoms of AUD and DA. All analyses were conducted in Stata (StataCorp., 2015).
Results
Descriptive statistics
Demographic characteristics, including weighted percentages, of the two sub-samples are shown in Table 1. Among the past-year drinkers, 36.4% engaged in heavy drinking in the past year and the average past-year maximum number of drinks on a single occasion was 5.7 (SD = 1.8). A minority (13.4%) had used cannabis or another drug in the past year. Among the people who used drugs in the past year, most (87.8%) had used alcohol in the past year and more than half (52.7%) had engaged in heavy drinking in the past year, with the average past-year maximum number of drinks on a single occasion being 5.1 (SD = 2.0). Simultaneous co-use of alcohol with at least one other drug was less common in the sample of drinkers (7.6%) than in the sample of people who used drugs (49.9%).
Descriptives for weighted sub-samples1 of past-year drinkers and past-year drug users who have never been to treatment, 2014–2015 National Alcohol Survey.
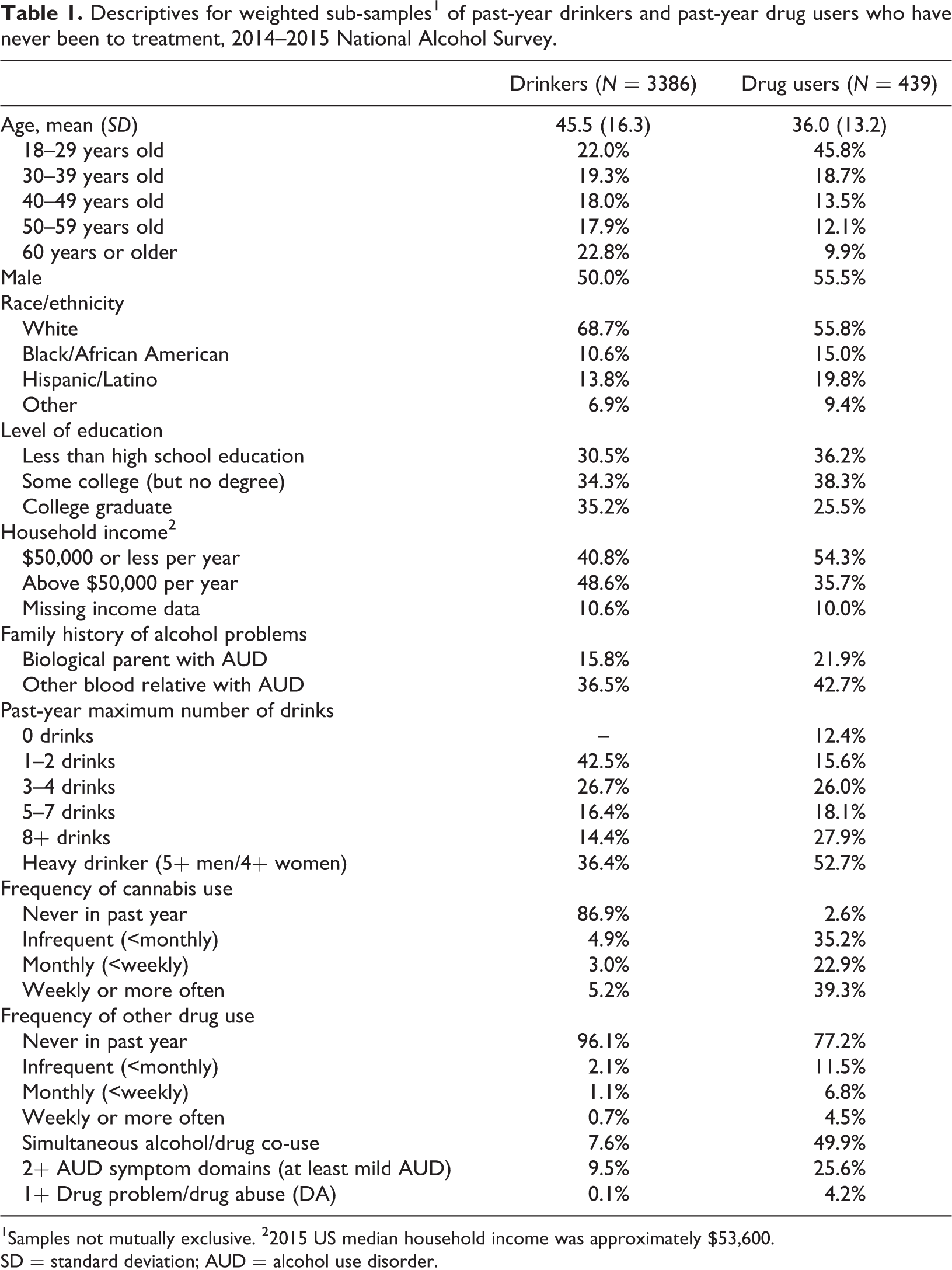
1Samples not mutually exclusive. 22015 US median household income was approximately $53,600.
SD = standard deviation; AUD = alcohol use disorder.
In this treatment-naïve sample, 9.5% of drinkers and 25.6% of people who used drugs met criteria for mild AUD, and 2.6% of drinkers and 8.8% of people who used drugs met criteria for moderate or severe AUD (symptoms in 4+ domains in the past year). Less than 1% of drinkers and 4.2% of people who used drugs met criteria for DA.
Regression models
Results from the adjusted models in the sample of past-year drinkers are shown in Table 2. Heavy drinking was associated with significantly increased risk for AUD, as was monthly (odds ratio, OR = 2.39, p < .05) or weekly (OR = 2.72, p < .05) use of cannabis. The associations between infrequent (less than monthly) cannabis use (OR = 1.51, p > .10) or use of other drugs (less than monthly: OR = 1.47, p > .10; monthly use: OR = 3.06, p = .10) with AUD were not statistically significant. With simultaneous co-use in the model, risks associated with monthly or weekly cannabis use (OR = 1.34 and 1.25, respectively, both p > .10) were reduced to non-significance; simultaneous co-use (OR = 2.35, p < .10) was not statistically significant either. In sensitivity analyses omitting the frequencies of cannabis and other drug use, the association between simultaneous co-use and past-year AUD was statistically significant, however (OR = 3.18, 95% CI = 1.83, 5.54, p < .001; model results available upon request).
Associations of past-year alcohol use disorder (AUD) with alcohol and drug use in a US general population sample of past-year drinkers who have never been to treatment (N = 2857).
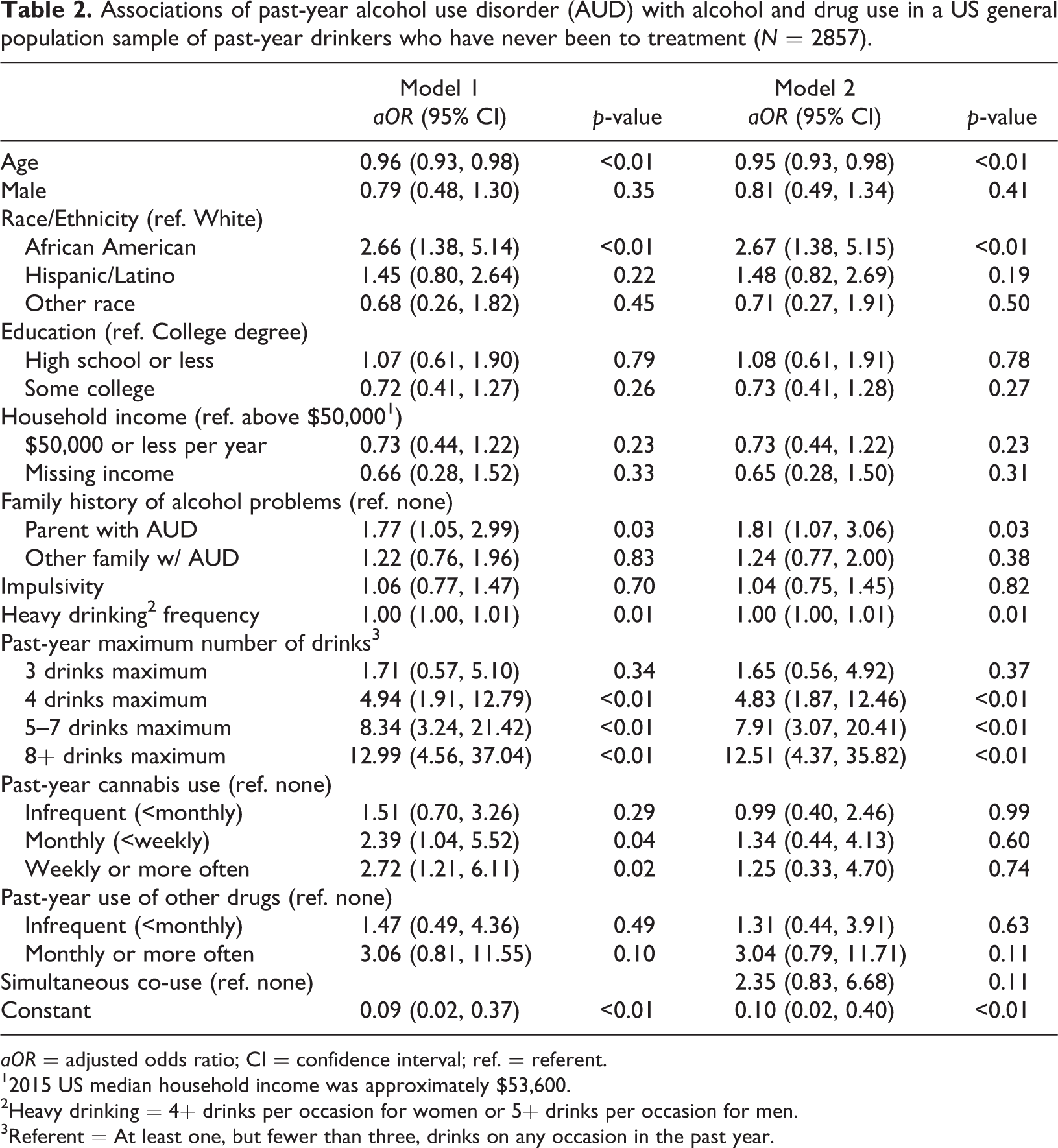
aOR = adjusted odds ratio; CI = confidence interval; ref. = referent.
12015 US median household income was approximately $53,600.
2Heavy drinking = 4+ drinks per occasion for women or 5+ drinks per occasion for men.
3Referent = At least one, but fewer than three, drinks on any occasion in the past year.
Results from the adjusted models in the sample of people who used drugs in the past year are shown in Table 3. Heavy drinking was not associated with past-year DA, but weekly cannabis use (OR = 4.20, p < .05) and weekly other drug use (OR = 7.20, p < .05) were associated with greater odds of DA. Simultaneous co-use was strongly associated with DA (OR = 16.01, p < .01), and the risk associated with weekly other drug use (OR = 6.79, p < .05) remained elevated but the risk associated with weekly cannabis use (OR = 2.92, p < .10) was reduced to non-significance after accounting for co-use. In both models, confidence intervals were wide for use of other drugs, suggesting substantial variability in DA among weekly users of drugs other than cannabis.
Associations of past-year drug abuse with alcohol and drug use in a US general population sample of past-year drug users who have never been to treatment (N = 388).
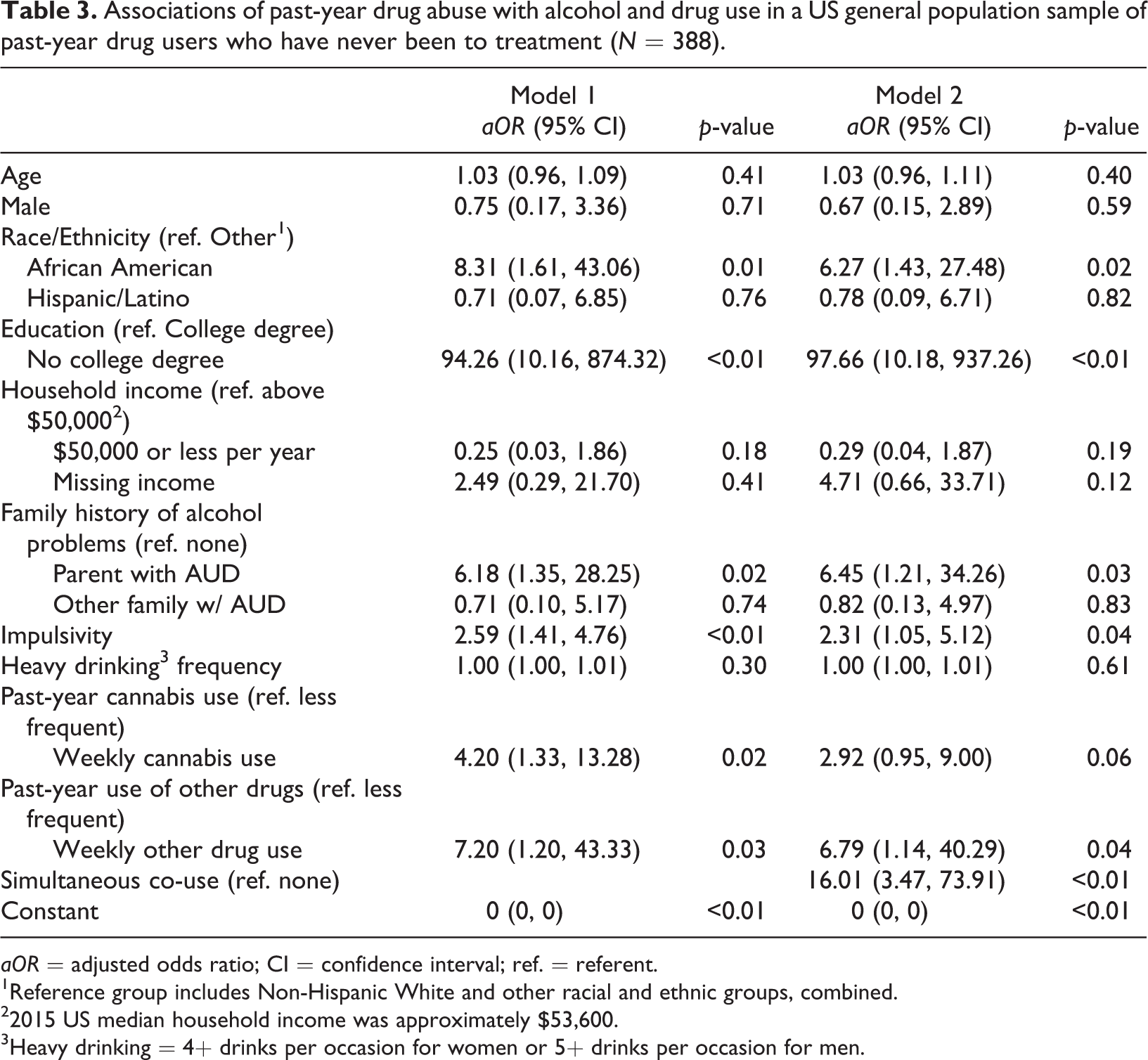
aOR = adjusted odds ratio; CI = confidence interval; ref. = referent.
1Reference group includes Non-Hispanic White and other racial and ethnic groups, combined.
22015 US median household income was approximately $53,600.
3Heavy drinking = 4+ drinks per occasion for women or 5+ drinks per occasion for men.
In the models accounting for simultaneous co-use of alcohol and drugs, having a parent with a history of alcohol problems (OR = 1.81, p < .05 for AUD; OR = 6.45, p < .05 for DA) and being African American (OR = 2.67, p < .01 for AUD; OR = 6.27, p < .05 for DA) were correlated with both AUD and DA. Impulsivity and low levels of education were significantly correlated with DA (OR = 2.32, p < .05 and OR = 97.66, p < .01, respectively) but not AUD.
Examining specific symptom domains
To examine whether elevated risk of AUD might be primarily attributable to symptom domains associated with externalising behaviours (such as use in hazardous situations), rather than biological manifestations of addiction (such as withdrawal and craving), we conducted exploratory bivariate analyses. These showed that simultaneous co-use of alcohol and drugs (compared to no simultaneous use, collapsing across all types and frequencies of cannabis and other drug use) was associated with significantly greater endorsement of each of the separate AUD and DA symptom domains, including alcohol craving, tolerance and withdrawal, as well as social and health problems (see Figure 1). For example, 12.8% of respondents who reported simultaneous use of alcohol and at least one other drug reported using alcohol in hazardous situations, compared to 3.7% of respondents without simultaneous co-use (including people who did not use drugs); design-based F-statistic (df = 1, 3382) = 21.74, p < .001. Results for physiological alcohol dependence symptoms were even more pronounced: 44.5% of respondents who reported simultaneous use of alcohol and at least one other drug reported withdrawal symptoms, compared to 9.0% of respondents without simultaneous co-use; design-based F-statistic (df = 1, 3382) = 115.08, p < .001. Similarly, 23.5% of respondents who reported simultaneous use of alcohol and at least one other drug reported cravings for alcohol, compared to 5.0% of respondents without simultaneous co-use; design-based F-statistic (df = 1, 3382) = 54.68, p < .001. (Other results available upon request.)
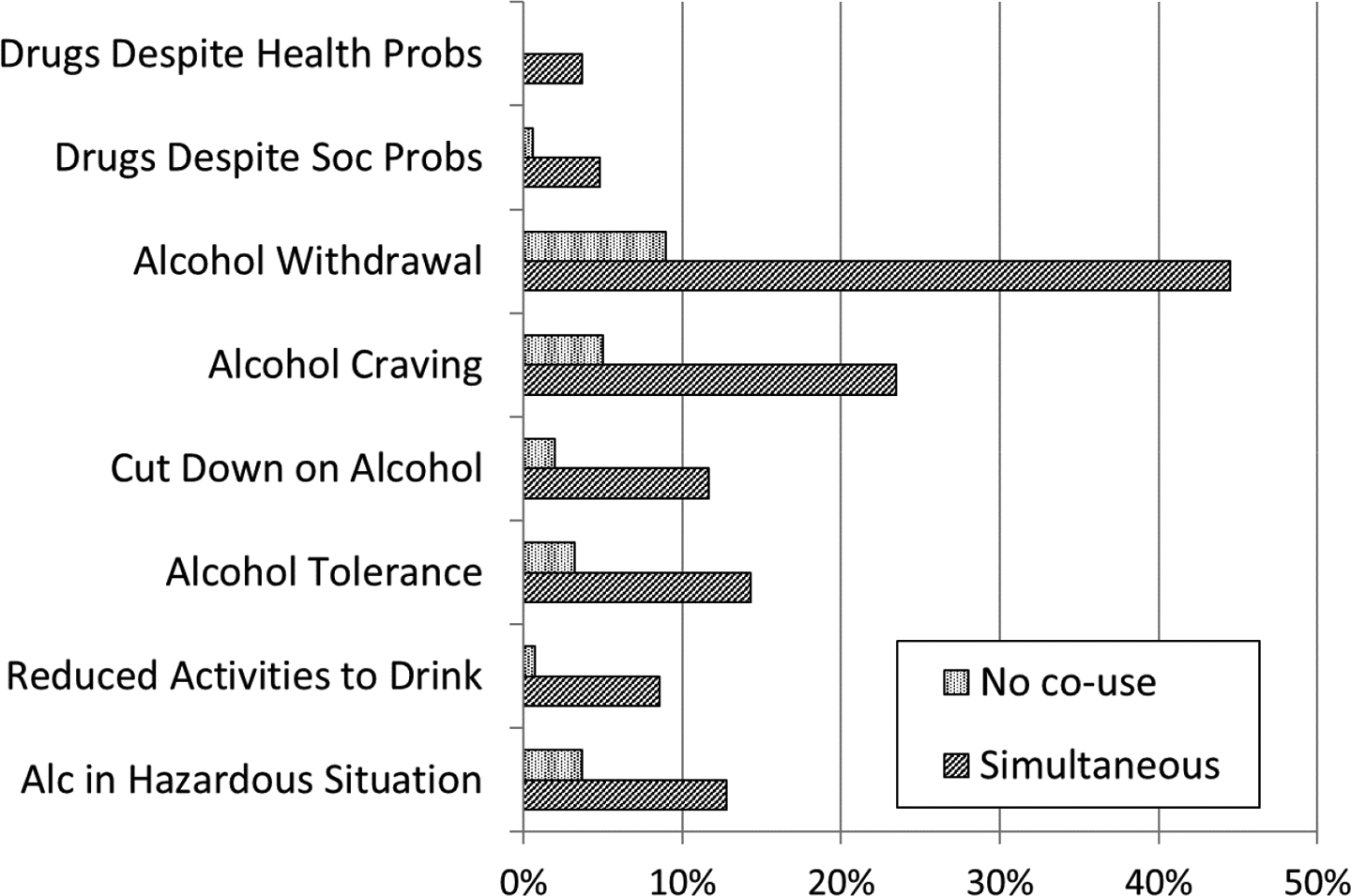
Prevalence of specific symptoms of alcohol use disorder (AUD) and drug abuse (DA) for groups of treatment-naïve adults defined by co-use of alcohol, cannabis and other drugs.
Discussion
In a general population, treatment-naïve sample, we found that the strongest and most robust correlate of AUD was heavy drinking. Monthly or weekly cannabis use also was significantly associated with AUD, but less frequent use of cannabis was not. In addition, in a trimmed model, simultaneous co-use of alcohol and drugs was associated with three times the odds of meeting criteria for AUD. Weekly cannabis use and weekly use of other drugs were also significantly associated with DA, with the strongest correlate of DA being simultaneous alcohol and drug co-use. Heavy drinking was not related to DA.
Other correlates of both AUD and DA included having a family history of AUD and being African American, with the latter relationship also being highlighted in another recent study of concurrent alcohol and cannabis use (Saha et al., 2018). Additionally, impulsivity and low levels of education were significantly correlated with DA but not AUD. Future research is needed to identify barriers to care that may disproportionately impact African Americans and people with low levels of education who are in need of treatment for SUD, including studies of appropriate screening and intervention strategies to reach people who are not presenting for care for substance use problems (Zemore et al., 2018).
Building on prior work in the US National Epidemiologic Survey of Alcoholism and Related Conditions suggesting cannabis use is a risk factor for development of AUD (Blanco et al., 2016; Weinberger, Platt, & Goodwin, 2016) and showing the odds of AUD are significantly elevated among cannabis-dependent individuals (Saha et al., 2018; Stinson et al., 2005), we found frequent cannabis use – at least monthly or weekly – was an important correlate of AUD. However, frequency of cannabis use was no longer related to AUD once accounting for simultaneous co-use of alcohol and drugs. These findings are in line with prior studies showing simultaneous co-use is one of the most salient predictors of adverse alcohol outcomes the general population (Subbaraman & Kerr, 2015). Furthermore, the current study extends previous results by examining clinically important outcomes, as well as including use of drugs other than cannabis.
Findings suggest that co-use of alcohol and drugs may be an important risk factor for substance use disorder, rather than a low-risk behavioural pattern driven by impulsivity. Specifically, we found in bivariate analyses that simultaneous co-use was significantly associated with endorsement of each of the separate AUD and DA symptom domains, including alcohol craving, tolerance and withdrawal, as well as social and health problems due to use. In fact, differences between people who did and did not report simultaneous co-use of alcohol and drugs were most pronounced for cravings and withdrawal, which would not be classified as externalising symptoms. Additional studies with large samples of people who use both alcohol and drugs would help to verify and extend these preliminary results.
It is not clear whether physicians ask about co-use of alcohol with other drugs during routine screening for alcohol or other substance-use disorders, although co-use has long been considered a consequence of SUD. For example, the Drinker Inventory of Consequences (DrInC), an instrument commonly used in clinical and research settings, includes an item on drug use (“My drinking has caused me to use other drugs more”) as part of its Physical Consequences sub-scale (Miller, Tonigan, & Longabaugh, 1995). Our results suggest that co-use might be a precursor of alcohol-related problems, as well as a consequence. In this sample of treatment-naïve adults, screening only for heavy alcohol use would rule out a sizable proportion of respondents who reported simultaneous co-use of alcohol and drugs. In fact, 31.3% of simultaneous users reported a past-year maximum number of drinks on any one occasion as less than five, which is a threshold typically identified as high-risk (National Institute on Alcohol Abuse and Alcoholism, 2005). If the co-use of alcohol with cannabis and/or other drugs is a risk factor for alcohol use disorders, then physicians screening for alcohol problems should also ask about other drug use.
Screening and brief intervention (SBI) for problematic drinking in primary care is among the most effective and cost-effective of preventive services (Saitz, 2014). Evidence is more equivocal for universal drug-use screening (US Preventive Services Task Force, 2011), although some successful studies have been conducted (see, for example, Smith, Schmidt, Allensworth-Davies, & Saitz, 2010). A review of primary care approaches to addressing substance misuse recommends that physicians use the Drug Abuse Screening Test-10 (DAST; Skinner, 1982) for identifying patients with substance use disorders (Shapiro, Coffa, & McCance-Katz, 2013). However, while the DAST includes a question asking about use of more than one drug at a time, it does not address alcohol explicitly. Similarly, the most common diagnostic criteria for SUD appear to pertain to one substance at a time. Some have recommended that new SBI approaches address multiple risk behaviours (e.g., co-use) and prioritise these for intervention, emphasising that primary care physicians should ask patients about drug use just as they would ask about other symptoms, drinking behaviours, or diet (Saitz, 2014). Intervention studies are needed to increase the prevalence of screening for drug use and associated problems in primary care; perhaps a targeted focus on simultaneous co-use would be an efficient method for identifying patients in need of targeted care while also appealing to practitioners with limited time available to devote to screening.
Study limitations
Because our study is cross-sectional, causality cannot be established. It is possible that symptoms of AUD or DA developed prior to the onset of co-use of alcohol and drugs in these samples. Another limitation is that, even with a large, representative sample, there remains somewhat limited statistical power for assessing these relatively rare outcomes, particularly in the smaller sample of people who used drugs in the past year, which should be taken provisionally. We used analytic weights to represent the US adult population at the time of data collection, but our findings may not be representative of certain population sub-groups such as college students who may be at elevated risk of co-use of alcohol and drugs. Reporting bias is a possible limitation, as some behaviours are likely to be under-reported due to social desirability concerns. There also may be biases associated with missing data. Although telephone interviews afford more privacy than face-to-face, in-person interviews, in general, self-administered questionnaires are preferred for reporting of sensitive information such as illicit behaviours and substance use. A distinct strength of this study is the assessment of simultaneous co-use of alcohol with other drugs; other major epidemiological studies from the US are only able to examine concurrent use of alcohol and drugs or co-morbidity of AUD with another form of SUD in the same 12-month period (see, for example, Saha et al., 2018). In addition to addressing the limitations of our study, future research should include more detailed measures of co-use, and analyses should identify potential differences between medical and recreational cannabis users.
Conclusions
At a minimum, healthcare providers should assess the maximum number of drinks their patients have consumed on a single occasion in the past year, and they also should screen for simultaneous co-use of alcohol and drugs to help identify patients who may benefit from substance abuse treatment
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding provided by the US National Institutes of Health’s National Institute on Alcohol Abuse and Alcoholism grants P50AA005595 (W. Kerr, PI) and R21AA23039 (M.S. Subbaraman, PI). Opinions expressed are those of the authors and do not necessarily reflect those of the sponsoring institutions, which had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the manuscript for publication.