
Abstract
Aims:
This study investigates demographic, personality, and psychological health correlates of different drinking patterns.
Design:
Students at the four largest institutions of higher education in Bergen municipality were invited via email to complete an internet-based questionnaire. The final sample size was 11,236 (39.4%), mean age 24.9 years (SD = 6.5), and 63.3% were women. The survey included the Alcohol Use Disorder Identification Test (AUDIT) and questions about demographics, personality traits, and symptoms of depression and anxiety. Binary logistic regressions were used to identify correlates of different drinking patterns.
Results:
A total of 53.0% of the students had an AUDIT score of or above 8 (i.e., hazardous drinking). Being native Norwegian, male, single, without children, non-religious, extroverted, unconscientious, and less open to experience were associated with higher AUDIT scores, drinking frequently, and binge drinking. Having parents with high alcohol or drug use increased the odds of engaging in binge drinking, but this factor was not associated with frequent drinking. Students scoring higher on neuroticism and openness were less likely to report problematic alcohol usage.
Conclusions:
A majority of the students reported alcohol habits that are associated with harm if they persist. This emphasises the need to examine the long-term consequences of students’ alcohol use.
The situation of college and university students has some unique characteristics. For instance, being a student tends to involve formation of new friendships and identities, and often fewer obligations to family and work life (Pittman & Richmond, 2008; Scanlon, Rowling, & Weber, 2007). Enrolment in higher education is typically associated with increased alcohol consumption (Bingham, Shope, & Tang, 2005; O’Malley & Johnston, 2002). A great proportion of students consume alcohol at a level classified as hazardous, with prevalence rates ranging from 21.1–82.0% across studies (Beenstock, Adams, & White, 2011; Heather et al., 2011; Nedregård & Olsen, 2014; Pengpid, Peltzer, van der Heever, & Skaal, 2013). Drinking more than five to six units on one occasion is often defined as binge drinking (Connor, Gray, & Kypri, 2010; Wechsler, Dowdall, Davenport, & Castillo, 1995). Compared to other consumers, students tend to engage in more frequent binge drinking (Slutske et al., 2004; Wechsler et al., 1995). Binge drinking among students has been associated with more dissolute and hazardous behaviour, such as missing classes, engaging in unprotected sex, and being involved in accidents (Connor et al., 2010; Perkins, 2002; Tefre, Amundsen, Nordlund, & Lund, 2007; Wechsler et al., 1995). Subsequently, binge drinking among students involves inconveniences to society at large through an increased burden on the healthcare system as well as the nuisance caused to sober neighbours and fellow students (Rehm et al., 2009; Wechsler, Dowdall, Maenner, Gledhill-Hoyt, & Lee, 1998). Alcohol use among students has also been associated with a range of serious injuries (Hingson, Heeren, Zakocs, Kopstein, & Wechsler, 2002). The possible adverse effects of alcohol use both on the individual student and on society warrant inquiries into the characteristics of the students at risk.
Several demographic factors have been associated with alcohol use among students. Age has been found to be inversely related to alcohol consumption. This relationship seems to be nullified when one controls for relationship status, job status, and child caring (Andersson, Johnsson, Berglund, & Ojehagen, 2007; Nedregård & Olsen, 2014). The number of years spent as a student might also affect alcohol use, as norms in the student setting can enhance certain drinking habits and condone others (Nedregård & Olsen, 2010). Some studies have suggested that certain aspects of alcohol use (such as hazardous alcohol use and frequency of drinking) increase with time spent as a student (Davoren, Shiely, Byrne, & Perry, 2015; Nedregård & Olsen, 2014), while others have argued that first-year students seem to be particularly vulnerable to high alcohol intake and binge drinking (Podstawski, Choszcz, Klimczak, Kolankowska, & Zurek, 2014; White, Kraus, & Swartzwelder, 2006). Because alcohol habits tend to vary significantly across cultures, country of birth may be associated with alcohol consumption (Pedersen, 2015; Skogen, Bøe, Sivertsen, & Hysing, 2016). Scandinavian alcohol culture is particularly known for encompassing frequent binge drinking, and recent studies also suggest an increase in the frequency of drinking among Scandinavians (Pedersen, 2015). The cultural differences in drinking may not be as prominent among students compared to other populations, as students seem to have similar drinking habits across cultures (at least in Western nations), and internationalisation may further increase this homogenisation (Andersson, Wiréhn, Ölvander, Ekman, & Bendtsen, 2009; Gill, 2002; Stock et al., 2009; Varela & Pritchard, 2011). Men tend to drink more alcohol than women (Andersson et al., 2007; Nedregård & Olsen, 2014; Nolen-Hoeksema, 2004; Wilsnack, Vogeltanz, Wilsnack, & Harris, 2000), but some studies indicate that gender differences in drinking are decreasing (Gill, 2002; Keyes, Grant, & Hasin, 2008). Besides sex and culture, parental alcohol use has been identified as a predictor of offspring’s alcohol consumption, and both environmental and heritability factors are believed to contribute to this relationship (Andersson et al., 2007; Ary, Tildesley, Hops, & Andrews, 1993; Froehlich, Zink, Li, & Christian, 2000; Haugland, Holmen, Ravndal, & Bratberg, 2013; Pedersen, 2015). Religious individuals tend to drink less than their non-religious counterparts (Engs, Diebold, & Hanson, 1996; Michalak, Trocki, & Bond, 2007). Singles and students without children have also been demonstrated to drink more than students in a relationship or students who are parents (Andersson et al., 2007; Nedregård & Olsen, 2010, 2014; Wechsler et al., 1995).
Personality factors such as psychopathy and sensation seeking have been found to predict alcohol consumption (Merenakk et al., 2003). The Five-Factor Model of Personality is a well-regarded and widely used taxonomy of personality traits, and includes the traits of extroversion (e.g., being talkative and outgoing), agreeableness (e.g., being sympathetic and warm), conscientiousness (e.g., being organised and prompt), neuroticism (e.g., being nervous and anxiety prone), and openness to experience (e.g., being imaginative and intellectually oriented) (McCrae & John, 1992). Extroversion (Merenakk et al., 2003; Raynor & Levine, 2009) and neuroticism (Malouff, Thorsteinsson, Rooke, & Schutte, 2007) have been found to be positively related to alcohol consumption, whereas agreeableness (Malouff et al., 2007) and conscientiousness (Malouff et al., 2007; Merenakk et al., 2003; Raynor & Levine, 2009) are inversely related to alcohol consumption.
Several studies indicate a positive relationship between psychological distress and alcohol consumption (Dixit & Crum, 2000; Grant et al., 2004; Kushner, Abrams, & Borchardt, 2000; Nedregård & Olsen, 2014). Symptoms of depression have been found to predict alcohol problems and binge drinking (Dixit & Crum, 2000; Grant et al., 2004). Anxiety has also been associated with increased alcohol consumption (Grant et al., 2004; Kushner et al., 2000).
Previous studies have investigated a range of correlates related to alcohol use, but few have investigated how different correlates relate to different drinking patterns. As alcohol use has a pivotal position in student life, correlates related to drinking in this population may differ from those linked to drinking in other populations. Against this backdrop, the current study aimed to identify demographical, personality, and psychological health correlates of different drinking patterns in a university college/university student population.
Methods
Procedures and sample
All students registered at the four largest institutions of higher education in Bergen municipality, Norway, were invited via email in autumn 2015 to participate in an online survey. The institutions on which our sample is based include a public university and a public college, which both offer a range of subjects. The other two institutions represent colleges that specialise in business subjects; one is private while the other is public. Most of the students who received an invitation were full-time students, but some part-time students from one of the institutions were included accidentally. The recipients who did not respond within two weeks were sent up to two email reminders. A total of 28,553 students received an invitation, and 11,236 (39.4%) agreed to participate. The project was approved by the Regional Committee for Medical and Health Related Ethics, Western Norway (no. 2015/1154). Those who responded took part in a lottery with two iPhone 6s and 50 gift cards (each with a value of 500 NOK = ∼ 50 EUR) as prizes.
Measurement
Alcohol use was assessed by the Alcohol Use Disorders Identification Test (AUDIT), comprising 10 items (Babor, Higgins-Biddle, Saunders, Monteiro, & WHO, 2001; Bohn, Babor, & Kranzler, 1995), Cronbach’s alpha: 0.78 (present study). The first three questions concern alcohol consumption (AUDIT-C): frequency of drinking, typical quantity consumed, and frequency of heavy drinking (i.e., large quantities consumed in a single session/episode). The AUDIT-C is a brief, well-validated measurement to detect alcohol misuse (Bradley et al., 2007; Bush et al., 1998). The following three questions in the AUDIT concern dependence symptoms – impaired control, increased salience, and morning drinking – whereas the four last questions ask about harmful alcohol use – guilt after drinking, blackouts, alcohol-related injuries, and others being concerned about the respondents’ drinking (Babor et al., 2001; Bohn et al., 1995). Total AUDIT scores range between 0 and 40; scores of or above 8, 16, or 20 indicate hazardous, harmful, or dependent alcohol use, respectively (Babor et al., 2001; Bohn et al., 1995).
Demographics were measured by closed questions about age, years studied, current religious identification, country of birth, gender, experience of parents’ alcohol and drug use negatively affecting childhood, relationship status, and parental status.
Personality was measured with the Mini-International Personality Item Pool (Mini-IPIP), a personality scale with 20 items. Cronbach’s alphas: 0.83 for extroversion, 0.77 for agreeableness, 0.69 for conscientiousness, 0.75 for neuroticism, and 0.74 for openness (present study). The Mini-IPIP is considered to be a reliable and valid measure of the five-factor personality dimensions (Donnellan, Oswald, Baird, & Lucas, 2006). The scale consists of several statements about typical behaviour (e.g., being compassionate, life of the party, tidy, having a rich imagination, and becoming easily upset), and the participants are asked to state to what degree the statements apply to them. There are four statements for each of the five personality traits, with total scores ranging from 5 to 20 for each trait.
Mental health was assessed using the Hopkins symptoms checklist (HSCL-25) (Derogatis, Lipman, Rickels, Uhlenhuth, & Covi, 1974). The HSCL-25 consists of 25 items measuring anxiety and depression symptoms. Cronbach’s alphas: 0.81 for anxiety and 0.89 for depression (present study). When answering the HSCL-25, the participants are asked to assess to what degree different symptoms of anxiety (e.g., heart palpitations) and depression (e.g., feeling of hopelessness) have bothered them during the past two weeks. Total scores range between 10 and 40 for anxiety, and between 15 and 60 for depression.
Analysis
All data analyses were conducted using IBM SPSS Statistics 23. Missing data were deleted listwise. We conducted six logistic regression analyses where the dependent variables entailed AUDIT scores of or above 8, 16, and 20 (i.e., hazardous, harmful, and dependent alcohol use), respectively, as well as scoring 2 or higher on the first three AUDIT questions. The cut-off of 2 was chosen, as lower scores indicate low or infrequent alcohol intake. The first three items on the AUDIT were chosen, as they address specific drinking patterns and constitute the items of the AUDIT-C (Bradley et al., 2007; Bush et al., 1998). The following independent variables were recoded into dichotomised variables before being entered to the regression models: country of birth (Norway vs. other), parental alcohol and drug use during childhood (affected childhood negatively vs. did not affect childhood negatively), religion (religious vs. non-religious), relationship status (single vs. in a relationship) and having child/ren (yes vs. no). To achieve a comparable metric, responses to the personality and psychological health symptoms were recalculated into z-scores before being entered to the regression models. A total of 1124 (10.0%) students were excluded from the sample before the regressions were conducted due to non-response to some of the questions included in analyses.
Results
The sample’s mean age was 24.9 years (range: 17–75 years, SD = 6.5); 63.3% (n = 7084) were women; and the majority were born in Norway (92.4%, n = 10,235). A total of 53.0% (95% CI: 52.1–54.0%) of the students had an AUDIT score of 8 or higher; 7.5% (95% CI: 7.0–8.1%) had an AUDIT score of 16 or higher; and 2.2% (95% CI: 1.9–2.4%) had an AUDIT score of 20 or higher. In all, 72.7% (95% CI: 71.8–73.5%) of the students reported to drinking 2–4 times a month or more often; 60.8% (95% CI: 59.9–61.8%) reported to drinking 5–6 units or more on a typical day of drinking; and 48.8% (95% CI: 47.9–49.8%) reported drinking 6 or more units monthly or more often. The sample’s characteristics in terms of demographics, personality, psychological health, and alcohol use are shown in Table 1.
Sample characteristics, N = 11,236.
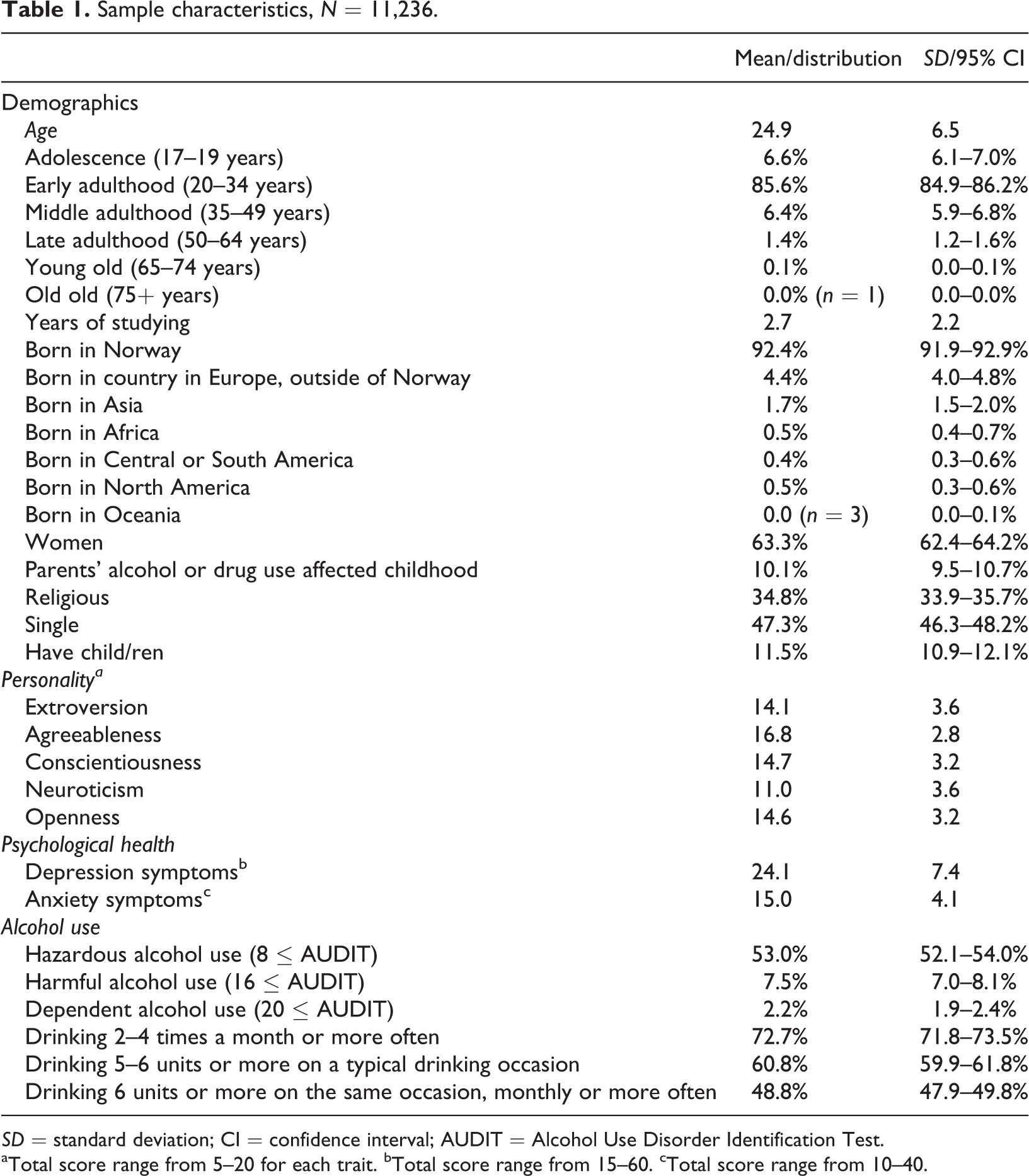
SD = standard deviation; CI = confidence interval; AUDIT = Alcohol Use Disorder Identification Test.
aTotal score range from 5–20 for each trait. bTotal score range from 15–60. cTotal score range from 10–40.
Correlates of different drinking patterns
The adjusted regression coefficients of the independent variables on the different dependent variables are shown in Table 2. The associations reported in the forthcoming sections were all statistically significant at p < .05. Age and years as a student showed an inconsistent relationship with the dependent variables. Age was negatively associated with hazardous alcohol consumption, positively associated with drinking 2–4 times a month or more often, and negatively associated with having a typical drinking quantity of 5–6 units or more, and drinking minimum 6 units on the same occasion monthly or more often. The number of years as a student was positively associated with drinking 2–4 times a month or more, but negatively associated with having a typical drinking quantity of 5–6 units or more and drinking minimum 6 units on one occasion monthly or more often. Being born in Norway increased the odds of hazardous alcohol consumption, drinking 2–4 times a month or more, typically drinking a quantity of 5–6 units or more, and drinking a minimum of 6 units monthly or more often. Men had increased odds compared to women of being in all problematic drinking pattern groups (i.e., having hazardous, harmful, and dependent alcohol use, and drinking a minimum of 2–4 times a month, having a typical drinking quantity of 5–6 units or more, and drinking a minimum of 6 units monthly or more often). The students who reported that their childhood had been negatively affected by parental alcohol or drug use were more likely to have hazardous, harmful or dependent alcohol use, and to have a typical drinking quantity of 5–6 units or more. These students were, however, not significantly more likely to drink often. Being religious decreased the odds of belonging to any problematic drinking pattern groups. Single students were more likely to belong to all the different problematic drinking groups. Having children decreased the odds of having hazardous or harmful alcohol use, and were negatively associated to drinking frequency, binge drinking, and frequent binge drinking.
Correlates of alcohol consumption, N = 10,112 (adjusted binary logistic regressions).
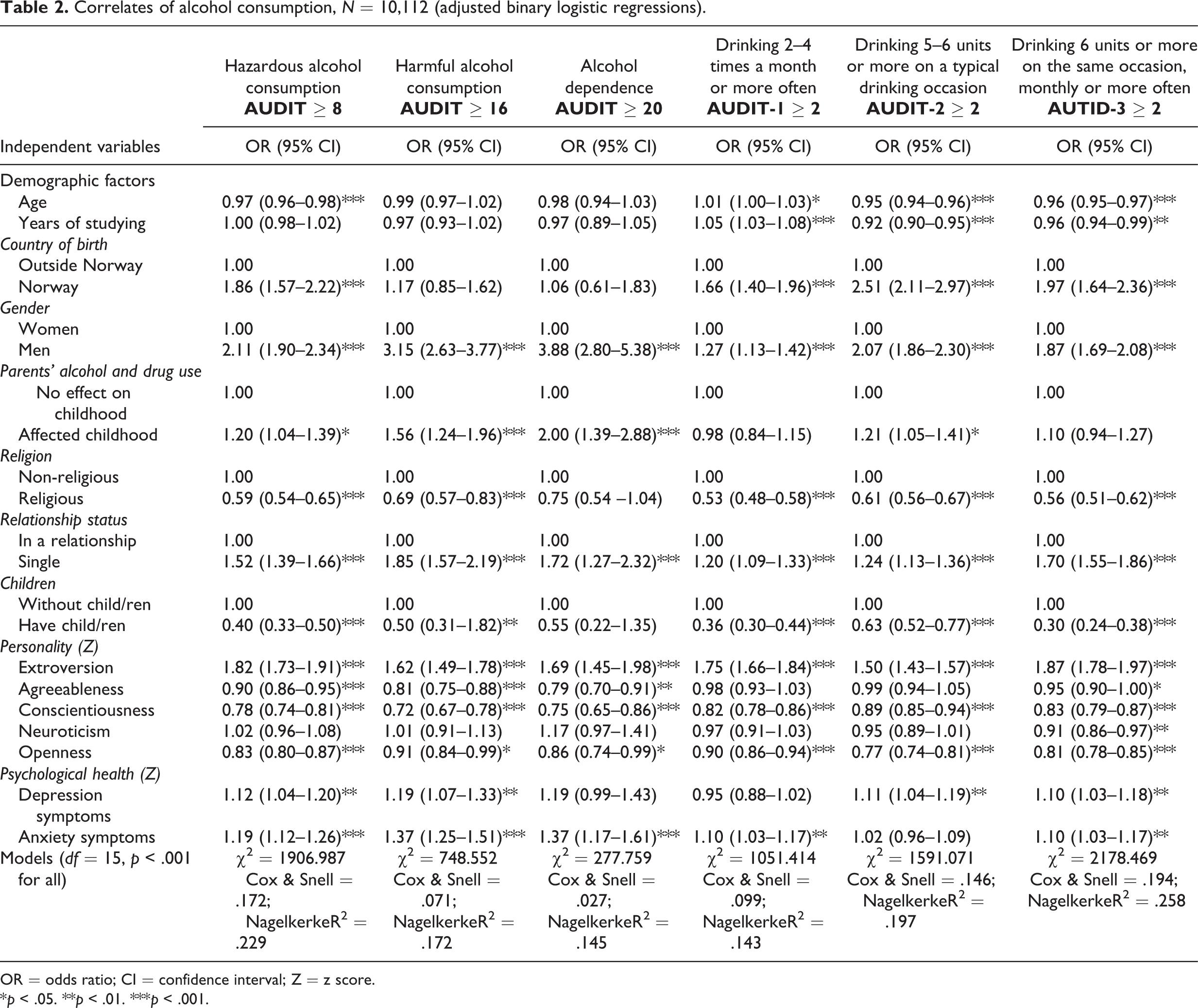
OR = odds ratio; CI = confidence interval; Z = z score.
*p < .05. **p < .01. ***p < .001.
In terms of personality, extroversion increased the odds of being in all problematic alcohol pattern groups. Agreeableness decreased the odds of having AUDIT scores of or above 8, 16, or 20, and of binge drinking frequently but was unrelated to the odds of drinking frequently and typically consuming large quantities. Conscientiousness decreased the odds of belonging to all problematic alcohol pattern groups. Neuroticism decreased the odds of engaging in binge drinking monthly or more often. Openness decreased the odds of being in all problematic alcohol pattern groups.
Both depression and anxiety symptoms were positively associated with alcohol consumption. Symptoms of depression increased the odds of having AUDIT scores of or above 8 and 16, and of having high typical quantity consumption and drinking 6 or more units monthly or more often. Symptoms of anxiety increased the odds of having an AUDIT score of or above 8, 16, or 20, drinking 2–4 times a month or more, and drinking a minimum of 6 units on one occasion monthly or more often.
Discussion
The number of students who reported hazardous alcohol consumption in this study seems worryingly high. This may pose a health threat, as hazardous alcohol consumption has been associated with an increased risk of harm for both the individual and others, and can lead to alcohol dependency (Babor et al., 2001). A recent Norwegian study indicated that hazardous drinking among students may also be associated with decreased academic achievement (Myrtveit, Askeland, Knudsen, Knapstad, & Skogen, 2016). Hazardous alcohol use is assumed to have adverse social consequences (Conigrave, Hall, & Saunders, 1995). The negative social effects associated with an AUDIT score of 8 or above may, however, not apply to student populations, as alcohol use seems to be an important component of relationship formation among students (Myrtveit, Askeland, Knapstad, Knudsen, & Skogen, 2016). Furthermore, the practical application of a cut-off value that puts the majority of students in an at-risk group may appear arbitrary, which emphasises the need for research on the development of students’ alcohol use (i.e., before and after studying) and potential long-term consequences of use. The findings from the current study indicate that binge drinking is the norm for the majority of these students. This finding is in accordance with previous research (Slutske et al., 2004; Wechsler et al., 1995). Binge drinking is related to several adverse effects (Connor et al., 2010; Tefre et al., 2007; Wechsler et al., 1995), and preventive initiatives among students seem warranted. With regard to binge drinking, it should also be recognised that research pertaining to suitable cut-offs is needed. In line with this it has been argued that the common cut-off of 5–6 units is rather arbitrary and may be too low to predict adverse consequences adequately (Jackson, 2008).
Several different demographic factors were associated with problematic alcohol consumption. The findings that students born in Norway, men, non-religious, singles, and students without children drink more than their counterparts have also been reported in previous research (Andersson et al., 2007; Engs et al., 1996; Nedregård & Olsen, 2014; Pedersen, 2015). Norwegian-born students were compared to students born in all other countries; the majority of the students born in other countries were born in other European countries. Males had a particularly increased likelihood of being in all the problematic drinking pattern groups. Several factors may explain this gender difference, among them gender roles and differences in risk aversion (Holmila & Raitasalo, 2005; Nolen-Hoeksema, 2004). It should, however, be noted that males may have a greater tolerance for alcohol compared to females (Mumenthaler, Taylor, O’Hara, & Yesavage, 1999). Some have therefore argued for gendered AUDIT cut-offs (Olthuis, Zamboanga, Ham, & Van Tyne, 2011; Reinert & Allen, 2007). Gender-specific cut-offs might have yielded different results. Increasing age and years as a student appear to be inversely proportionate to the amount of binge drinking, although, conversely, these factors are associated with increased drinking frequency. The current findings suggest that younger and less advanced students are more likely to engage in binge drinking, and this finding is supported by previous studies (Podstawski et al., 2014; White et al., 2006). The difference in drinking habits between younger/less advanced students and older/more advanced students may suggest that students are socialised into a more continental drinking pattern that is characterised by frequent consumption of low to moderate levels of alcohol. This alcohol pattern corresponds to the alcohol habits of others with high socioeconomic status (Pedersen, 2015). Low to moderate use of alcohol has fewer immediate adverse effects than does binge drinking, and has been suggested as a protective factor against some medical conditions (Rehm et al., 2003; Rimm, Williams, Fosher, Criqui, & Stampfer, 1999), although this has been debated and disputed (Pedersen, 2015). The total amount of alcohol consumed is nevertheless predictive of several other long-term illnesses, such as different forms of cancer (Rehm et al., 2003), and it seems therefore ill-advised to conclude that frequent alcohol consumption without binge drinking is without risk.
The students who reported that their childhood had been negatively affected by parents’ drug or alcohol use had greater odds of reporting hazardous, harmful, and dependent alcohol use, and to typically binge drink. These students were, however, not more prone to consume alcohol often or to binge drink often. This suggests that children of parents with high alcohol or drug consumption are more likely to drink large quantities when they drink and therefore experience more alcohol-related problems. Their tendency to binge drink may lead them to avoid frequent drinking. As far as we know, this finding represents a new specification of the relationship between parents’ drug and alcohol use and their offspring’s own alcohol use. The association between binge drinking and parental alcohol and drug use may be explained both by hereditary and environmental factors (Ary et al., 1993; Froehlich et al., 2000; Pedersen, 2015).
In the present study, extroversion was positively related, and conscientiousness negatively related, to alcohol consumption, which is in accordance with previous research (Merenakk et al., 2003; Raynor & Levine, 2009). Extroverts are known to be more sociable and to have a higher need for stimulation and excitement than their more introverted peers (McCrae & John, 1992). These needs may explain extroverts’ tendency to consume large amounts of alcohol. Their sociability typically puts them in situations where alcohol is consumed, and their need for stimulation may make them drink a larger amount of alcohol than introverts. The lowered alcohol use among individuals with high conscientiousness scores might be explained by several factors. Conscientious individuals are generally more organised and perform better academically than less conscientious individuals (Hair & Hampson, 2006; McCrae & John, 1992), and a certain level of abstinence from alcohol may be a prerequisite for this. Conscientious individuals also tend to score rather low on sensation-seeking and impulsivity, which are traits known to increase the odds of heightened alcohol consumption (Hair & Hampson, 2006). Agreeableness decreased the odds of having high AUDIT scores and engaging in frequent binge drinking. This factor did not, however, significantly decrease the odds of drinking frequently or having high typical quantity consumption. Alcohol-related problems have been argued to particularly affect others (Nutt, 2012), and agreeable individuals are known to be considerate of others (McCrae & John, 1992), which may make them less likely to drink in a manner associated with problems. In the present study, higher scores on neuroticism did not significantly increase the odds of high alcohol consumption; instead, higher scores on neuroticism appeared to decrease the odds of engaging in binge drinking frequently. This is a surprising finding, as it contradicts previous research (Malouff et al., 2007). Neuroticism is associated with anxiety (McCrae & John, 1992), a factor controlled for in the present study. It is possible that other traits associated with neuroticism, like being self-conscious and worry prone (McCrae & John, 1992), might explain the reduced odds of often engaging in binge drinking, as these traits may make individuals with high neuroticism scores more concerned about potential negative effects of binge drinking. Another surprising and novel finding from the present study was that individuals with high openness scores were less likely to report high alcohol consumption. To our knowledge, this association has not previously been reported. Individuals scoring high on openness are considered unconventional (McCrae & John, 1992) and interested in experiencing things beyond normative experiences. As our findings indicate that most students have high alcohol consumption, the lowered alcohol use among individuals with high openness scores may partly be explained by their unconventional nature.
The present findings supported the notion of a relationship between symptoms of depression and anxiety and problematic alcohol use. The relationship between symptoms of depression and anxiety and increased alcohol consumption can be explained by the assertion that alcohol relieves distress in the short run (Cowan, 1983), while increasing it in the long run, which may lead to a vicious circle. Our findings indicate some differences in drinking patterns predicted by the two constructs. Symptoms of depression increased the odds of typically drinking 5–6 units of alcohol or more on the same occasion and often engaging in binge drinking, but depressive symptoms did not significantly increase the odds of frequent drinking. Conversely, anxiety symptoms increased the odds of frequent drinking and frequent binge drinking, but did not significantly increase the odds of typically drinking 5–6 units of alcohol or more on the same occasion. These findings suggest that individuals with higher levels of anxiety symptoms are more likely to engage in both low to moderate alcohol consumption and binge drinking, while individuals with higher levels of depression symptoms are more likely to engage in binge drinking when they drink.
Limitations and strengths
The cross-sectional design of this study precludes conclusions about directionality and causality, although it should be noted that demographic and personality variables are considered stable traits that for the most part existed before the individual started to drink. Furthermore, answers to questions about alcohol consumption may be influenced by social desirability bias (Tourangeau & Yan, 2007), although this bias seems to be reduced in internet-based studies like the current one (Bowling, 2005; Gnambs & Kaspar, 2015).
To our knowledge, the current study represents the most comprehensive investigation of correlates related to different forms of problematic alcohol usage among students. Our findings contribute with new knowledge about the specific alcohol patterns associated with depression and parents’ alcohol and drug use. Our findings that neuroticism and openness are negatively associated with high alcohol consumption have not been reported before. The large sample size is another asset of the study. Based on the diverse sample frame (i.e., students from different institutions, study fields, and educational levels were invited to participate) and the relatively high response rate, the findings are likely to be generalisable to other similar populations.
Conclusion
A majority of the students reported hazardous alcohol consumption, and this may be a problem at the population level as well. There is a need for more research on the potential adverse effects of students’ alcohol consumption, and investigation is warranted concerning whether proposed AUDIT cut-offs are appropriate for this population. Parental alcohol and drug use were associated with increased odds of engaging in binge drinking and experiencing alcohol-related problems, but did not increase the odds of frequent drinking or frequent binge drinking. Agreeableness did not decrease the odds of drinking frequently or of typically drinking 5–6 units of alcohol or more on the same occasion, but agreeableness decreased the odds of reporting alcohol-related problems and frequent binge drinking. Neuroticism was associated with decreased odds of engaging in frequent binge drinking, while openness decreased the odds of reporting high alcohol consumption in general. The current findings suggest that preventive efforts toward reducing students’ alcohol use are warranted. Being male and extroverted were particularly associated with problematic drinking, which implies that male students and the organisation of social settings may deserve added attention in prevention efforts aimed at the student population. Future studies should investigate potential moderation effects between gender and the identified covariates of drinking.
Footnotes
Acknowledgements
The University of Bergen and Bergen municipality funded the research reported in this publication. We want to thank Trude Remme for her help in setting up the online survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors have declared receipt of funding from the following sources: The University of Bergen and Bergen municipality.