
Abstract
Studies depict that patients often dread visits to the hospital because of an increased chance of spread of infections. Hence, this study investigated the design parameters that should be incorporated in the indoor public spaces in tertiary hospitals, as patients spend the most time here pre-diagnosis. The research focuses on reception, waiting areas, circulation areas and toilets as public areas in a tertiary hospital. The research utilized the salutogenic approach as it has been less adopted in past studies. Firstly, systematic reviews of the literature and design guidelines were conducted. Secondly, post-occupancy evaluation of tertiary hospitals in Delhi and Rotterdam were carried out. Finally, a focus group discussion was conducted with experienced healthcare architects to validate the framework of the design strategies. The main factors highlighted in the post-occupancy evaluations were parameters including ventilation, disinfection and layout. However, during the focus group discussion, digitalization, disinfection, daylight and ventilation were identified as key parameters. This study depicted that well-being should be incorporated into hospital design as a priority. Nevertheless, further research is required on the incorporation of digitalization in healthcare. This research will benefit architects in the design process while designing the public spaces of hospitals to improve the well-being.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has presented unprecedented challenges to healthcare systems worldwide, exposing critical vulnerabilities in hospital infrastructure and design. These challenges extend beyond mere technical considerations of infection control to encompass a range of issues including environmental contamination hazards, facility management and building layout adaptability. 1 Equally important, yet often overlooked, is the psychological dimension of healthcare environments. How patients emotionally and behaviourally respond to hospital spaces, particularly during public health emergencies. During such crises, patients tend to exhibit heightened sensitivity to their surroundings, often experiencing negative emotions that can compromise their healthcare-seeking behaviour. 2 As architect Llewelyn-Davies aptly noted, “For most individuals a visit to the hospital is a horrible experience and an absence of formality and an atmosphere of reassurance should be the aim." 3
The psychological impact of hospital environments became particularly evident during the COVID-19 pandemic, as many patients postponed essential hospital visits due to fear of infection. 4 This phenomenon was especially pronounced in developing countries like India, which recorded nearly 45 million confirmed cases and over 532,000 deaths by September 2023. 5 Even developed nations with robust healthcare systems, such as the Netherlands, experienced significant impacts with over 8.6 million confirmed cases and nearly 23,000 deaths during the same period. 6 These statistics underscore the urgency of reconsidering hospital design approaches to address both infection prevention and control (IPC) requirements and the psychological needs of users, promoting overall health and well-being. 7
Within hospital settings, indoor public spaces including waiting areas, entrance zones, triage assessment areas, cafeterias and circulation routes, warrant particular attention. These spaces serve as critical points of first contact and prolonged interaction for patients and visitors before they transition to treatment areas. 8 Studies have identified hospital waiting areas as high-risk zones for disease transmission, as patients spend significant time there interacting with others prior to diagnosis.9–11 The design of these spaces must therefore carefully balance infection control measures with considerations for user comfort, navigation and psychological well-being. While there is relevant literature available looking at outdoor public spaces, and these are included in the discussion section below, this paper particularly focuses on indoor public spaces in relation to infection control and well-being.
Traditionally, hospital design has been dominated by the pathogenic approach, which conceptualizes health primarily as the absence of disease, focusing on preventing illness, disability and premature death. 12 While this approach has undoubtedly yielded important advances in infection control and patient safety, it often neglects the psychological and social dimensions of health. In contrast, the salutogenic approach, which we adopt in this study, views health as a positive state encompassing human abilities and functionality across behavioural and cognitive domains. This perspective examines not only physical health but also mental and social well-being, offering a more comprehensive framework for healthcare environment design. 13
The World Health Organization (WHO) has advocated for this reorientation toward salutogenic healthcare models for decades, as articulated in the Ottawa Charter. 14 This shift is particularly relevant in light of growing evidence that conventional pathogenic approaches are less effective for managing chronic conditions such as obesity, cardiovascular diseases and diabetes. 14 Furthermore, the business-oriented healthcare model that often accompanies the pathogenic approach, with its emphasis on cost and time efficiency, may inadvertently compromise patient experience. 15 In contrast, substantial evidence supports the positive impact of salutogenic approaches on quality of life, mental health, physical well-being and overall patient satisfaction. 16
Despite these advantages, few studies have examined the environmental aspects of hospital public spaces through a salutogenic lens that promotes patients’ sense of coherence. 17 Our research therefore has adopted this underutilized approach, which has established psychological connections between users and their physical environment 18 that can better addressing occupants’ emotions and experiences.19,20 Such an approach can transform patients’ perception of hospitals from intimidating medical facilities to healing environments that support their pursuit of health and well-being.21,22
IPC, while grounded in biomedical science, is fundamentally a behavioural science. 23 IPC practices can be enhanced through education, system changes and motivation. All are influenced by cultural factors and environmental design. This behavioural dimension of IPC calls for a holistic approach that integrates pathogenic strategies (e.g., air filtration systems) with salutogenic elements that could positively influence human psychology and behaviour. While acknowledging the importance of pathogenic measures, our research focused primarily on salutogenic strategies due to their relative underrepresentation in existing literature.
The relevance of such an approach was focused on patient behaviour that has been recognized in some COVID-19 literature, even when not explicitly framed in terms of salutogenic principles. Studies have demonstrated that controlling disease spread requires understanding cultural and social determinants specific to each community. 24 For instance, community-based interventions that account for social, individual and cultural characteristics have proven effective in minimizing infection transmission and mortality rates.
Given the importance of patients’ emotional and behavioural responses to healthcare environments, this study focused on the aspects of ‘well-being’ that emerge from a salutogenic perspective that are more regularly considered in design of tertiary hospitals.20,25,26 Well-being, defined as a state of positive perception that can be assessed both subjectively and objectively, provides a valuable framework for evaluating healthcare environments. 27 While a pathogenic approach focuses on understanding how etiological factors lead to illness 19 a salutogenic approach emphasizes maintaining physical and mental well-being based on a concept of positive health. 28
Although salutogenic and pathogenic approaches may initially appear disconnected, particularly regarding infection control, significant overlaps exist. As previously highlighted, patients’ engagement with hospital environments is influenced by their emotional responses, and many aspects of infection prevention rely on patient behaviour. In the context of IPC, salutogenic design could encourage practices such as hand hygiene, proper distancing and adherence to safety protocols by creating environments that naturally guide appropriate behaviour rather than enforcing compliance through restrictive measures. By framing IPC measures positively, highlighting the benefits of handwashing or the importance of clean environments, we can more effectively motivate individuals to adopt and maintain these practices. 29
This paper aims to fulfil four key objectives:
To identify well-being and IPC design parameters for indoor public spaces in tertiary hospitals that have been proposed following the COVID-19 pandemic To develop an evaluation framework for tertiary hospitals with particular focus on well-being and infection prevention To test the efficacy of design strategies for well-being and IPC through post-occupancy evaluation (POE) of selected hospitals To understand the application of identified design parameters across various countries and define potential further developments.
To achieve these objectives, we analysed post-COVID-19 guidelines issued by major organizations including the WHO, UK National Health Service (NHS), Netherland Board for Hospital Facilities (NBHF), and Indian Public Health Standards (IPHS). We examined their alignment with salutogenic principles and identified potential contradictions. Additionally, we conducted case studies of tertiary hospitals in Delhi, India and Rotterdam, Netherlands, applying our evaluation framework to assess their design effectiveness for promoting well-being while maintaining infection control. Our analysis further distinguished between design elements and operational factors, and accounts for practical considerations of implementation cost and timing, to provide actionable recommendations.
The outcome of this research has provided a practical evaluation tool and design recommendations that healthcare architects, design researchers, hospital administrators and facility managers can use to prioritize features that promote both well-being and infection control in indoor public spaces of tertiary hospitals. By integrating salutogenic principles with established infection control measures, we aimed to contribute to the development of hospital environments that not only prevent disease but actively promote health and healing.
Methods
This study employed a qualitative research methodology, integrating a systematic literature review, case studies and focus group discussions 30 to investigate design strategies for enhancing well-being and IPC in indoor public spaces of tertiary hospitals following the COVID-19 pandemic. This multi-faceted approach was chosen to comprehensively address the research aim, which was further delineated into four specific objectives.
Objective 1: Identification of design parameters
The first objective aimed to identify design parameters for well-being and IPC in tertiary hospital public spaces, as proposed in the post-pandemic literature. A systematic literature review, adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework, was conducted. Open access, English-language journals indexed in Google Scholar, published from 2020 onwards, were included. Initial screening of 62 retrieved publications eliminated 10 duplicates or overlapping studies. Subsequent screening based on abstract review and relevance to indoor public space design in tertiary hospitals resulted in the exclusion of 11 more publications. Finally, full-text review, focusing on the development of a salutogenic approach, led to the exclusion of an additional 9 publications, yielding 32 articles for inclusion. This review was supplemented by an analysis of hospital design guidelines and standards from the WHO, NHS, UK, NBHF and IPHS, with a specific focus on post-COVID-19 updates. This comprehensive review provided a foundation for identifying key design parameters and the PRISMA framework has been shown in Figure 1.
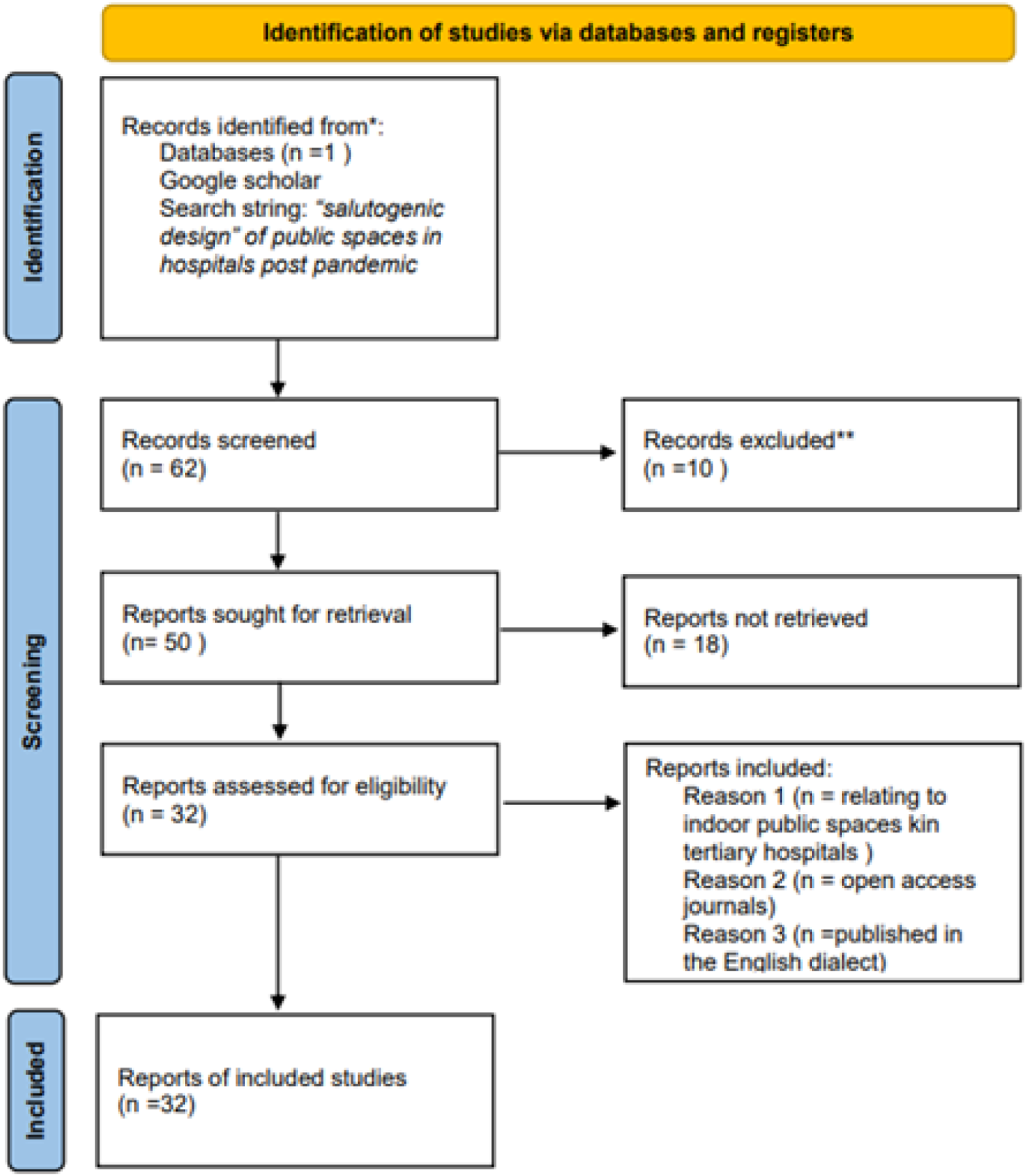
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework for literature review.
Objective 2: Development of an evaluation framework
The second objective focused on creating an evaluation framework for assessing well-being and IPC in tertiary hospital public spaces. Thematic analysis of the reviewed literature facilitated the categorization of design parameters into three domains: Space planning, environmental factors and human design factors. These parameters were then integrated with IPC requirements to develop a quantitative evaluation framework. A scaled point system was assigned to each design criterion, enabling a comprehensive assessment of public space effectiveness in promoting both well-being and IPC. This resulted in a practical checklist for evaluating tertiary hospital spaces.
Objective 3: Post-occupancy evaluation of case studies
To evaluate the efficacy of the identified design strategies, a POE was conducted in three government tertiary hospitals in Delhi, India and Rotterdam, Netherlands that treated COVID-19 patients. These super-specialty hospitals were selected due to their role in managing severe COVID-19 cases, particularly in India. Ethical approvals were obtained prior to data collection. The developed evaluation checklist, employing a 3-point scale, was used to assess each hospital. A score of 3 indicated full implementation of a design parameter, 1.5 indicated partial implementation and 0 indicated absence. The relative importance of each parameter was determined from the literature review, reflecting its contribution to physical and mental well-being and IPC. The scoring system was inspired by the Clinic Design POE Toolkit developed by the Centre for Health Design (2015). Hospital names have been anonymized to ensure ethical compliance. The discussion provides an analysis of the results of the POE focusing on design or operational challenges, while further considering implementation costs and occupancy constraints to provide actionable recommendations for healthcare facilities.
Objective 4: Consolidation and future directions
The final objective aimed to consolidate the perceived importance amongst the identified design parameters, and to explore their application across different countries. A focus group discussion was conducted with seven experienced architects and researchers from the US, Spain and India, all with expertise in hospital and healthcare building design. The discussion, held on 30th November 2022, was facilitated by the host university, and participants provided informed consent for recording. Thematic analysis of the discussion data was used to highlight the perceived importance of design parameters and identify future research directions for developing pandemic-resilient hospitals.
Results
The results of the research are presented in four sub-sections correlating to the literature review, the evaluation framework, the post occupancy evaluation and the group discussion phases of the study.
Literature review
Tertiary hospitals, characterized by their specialized care and high patient throughput, present unique challenges for IPC in public spaces. 31 These areas facilitate frequent interactions, potentially increasing the risk of pathogen transmission. 32 While open public building designs may enhance accessibility, they can compromise IPC efforts. 33 This review of 32 publications and hospital design guidelines from the WHO, UK NHS, NBHF, and IPHS identified key design considerations, categorized into space planning, environmental and human design factors, to optimize both well-being and IPC in these critical spaces.
Space planning factors
Effective circulation is paramount in tertiary hospitals to minimize waiting times and reduce exposure to pathogens. 34 However, this must be balanced with the need for isolation of infected patients to prevent cross-contamination. 1 Clear separation of routes and avoidance of shared vertical and horizontal connections are essential. Flexible functional spaces, readily convertible to treatment areas during surges, are also critical. 35
Wayfinding is increasingly recognized as a crucial aspect of space planning. Legible signage and visible landmarks facilitate navigation, reducing patient anxiety and stress.32,36 During pandemics, efficient triage is essential. Temporary pavilion triage areas and dedicated access routes for infectious disease management have proven effective. 32 Hospitals should consider incorporating large, adaptable open spaces for rapid triage area deployment.37,38 At entrances and registration zones, physical separation of staff and patients, particularly those undergoing triage, is crucial.33,39 Colour-coded zoning, such as green (clean), blue (COVID-19) and amber (undifferentiated), can further enhance IPC. 40
Beyond entrances, hospital layout influences both patient flow and environmental factors. Crossing-type layouts promote daylight and reduce cross-contamination, while alternating layouts enhance connectivity and outdoor access. 41 Decentralized waiting areas, integrated with digital triage and food delivery systems, can minimize overcrowding and pathogen transmission. 42 Open layouts for waiting areas and lobbies enhance natural ventilation, further reducing airborne pathogen transmission. 43 Social distancing measures, such as 1.5-m spacing between seating, are also essential. 38
Environmental factors
Environmental design plays a critical role in mitigating pathogen transmission and promoting well-being. Ventilation, lighting, acoustics and access to greenery are key considerations. Increased air exchange rates and humidity control (40–60%) are effective strategies for reducing airborne pathogen transmission.37,44 Seating arrangements should prioritize proximity to ventilation openings and views of gardens.35,42 In eating areas, enhanced ventilation is crucial to minimize transmission during mask removal. 45 Natural ventilation and lighting can minimize errors and pathogen load, and operable windows are recommended.46–51 Ultraviolet radiation can further reduce surface pathogen load. 43 Acoustic measures, maintaining sound levels below 45 decibels during the day and 35 decibels at night, are essential for patient comfort. 52 While access to greenery is beneficial, water features should be avoided due to the risk of Legionnaires’ disease. 53
Human design factors
Human design factors focus on creating comfortable, safe and accessible spaces. Adequate seating capacity with waiting areas of 37 m2 minimum and appropriate spacing (1500 mm between seats) are essential.33,54 Furniture and fittings should be constructed of non-porous, antimicrobial materials, such as copper-based alloys, to facilitate cleaning and reduce pathogen survival.4,7,33
Sufficient electrical and telecommunication infrastructure is needed to support patient surges and emergency medical equipment. 55 Ample hand hygiene facilities, including washing stations and sanitizers are crucial. 40 Touch-free technologies, such as soap dispensers and taps, reduce surface transmission. 43 Extractor fans and disposable towels in bathrooms are preferable to hand dryers. 45 Telehealth consultations can reduce in-person interactions and minimize pathogen spread.1,35
From a salutogenic perspective, patient well-being is paramount. Ergonomic furniture, access to greenery and sensory-rich materials contribute to a positive experience.36,42 Tranquillity rooms with nature-based elements can reduce staff stress. 56 Innovative approaches, such as outdoor waiting areas and drone-based temperature monitoring, can further enhance patient and staff well-being and IPC.33,57
To further illustrate the variations in design recommendations, Table 1 shows a comparative table giving contrasting guidelines of the the WHO,1,37,39 the IPHS, 54 UK NHS 58 and the NBHF 59 .The 2022 revision of the IPHS, reflecting post-pandemic adaptations, provides a valuable point of comparison. As the NHS and NBHF have not yet issued updated standards, this table serves as a practical tool for understanding the divergence in current design approaches.
A comparison of standards for NHS, WHO, Netherlands standards and IPHS
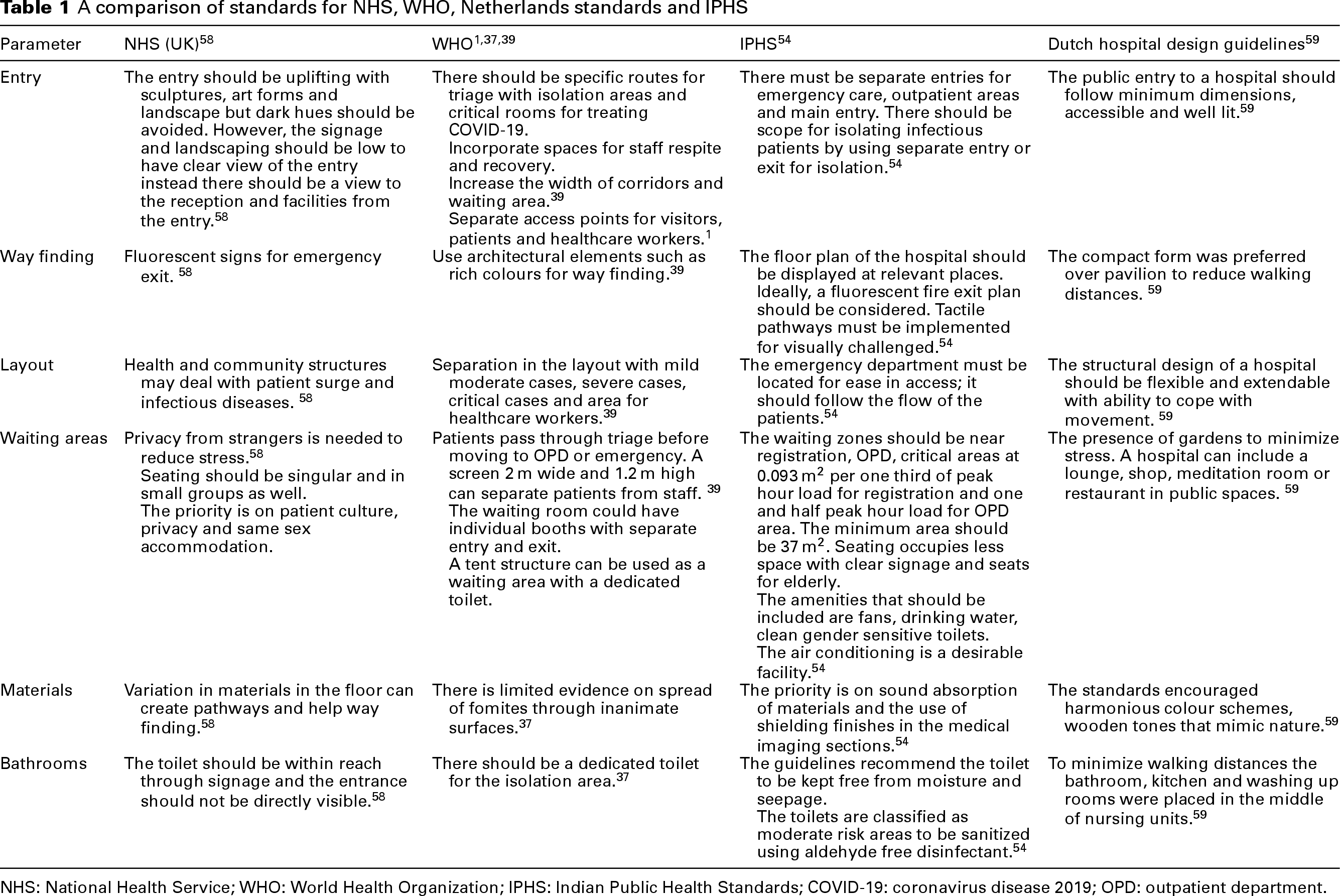
NHS: National Health Service; WHO: World Health Organization; IPHS: Indian Public Health Standards; COVID-19: coronavirus disease 2019; OPD: outpatient department.
A thematic analysis of these four sources, presented below, highlights the relative importance of design parameters as prioritized by each authority. This analysis could inform the development of the evaluation framework in the subsequent section. Table 2 provides the list of themes from thematic analysis from hospital standards in descending order of importance.
List of themes from thematic analysis from hospital standards in descending order of importance
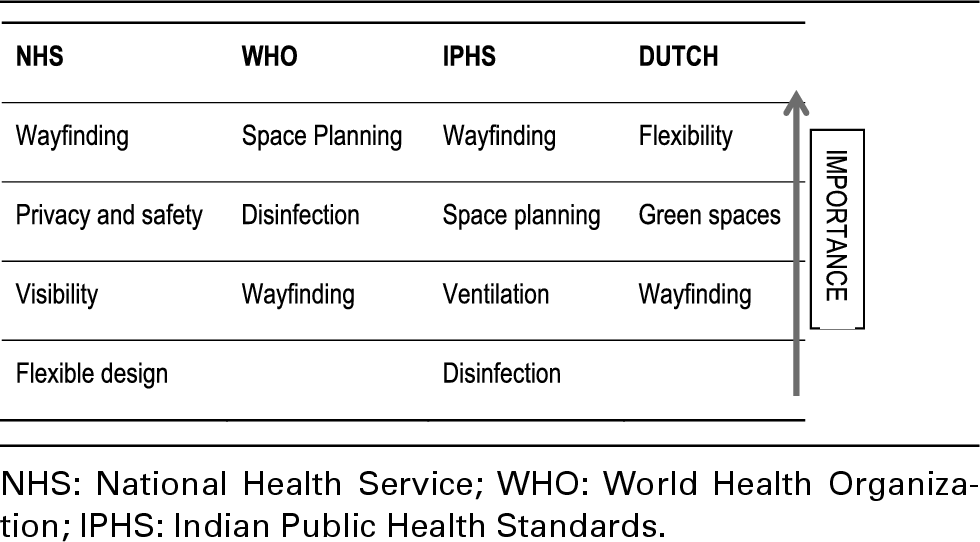
The comparative table illustrates that modifications to space planning were the most prevalent design changes implemented in public hospital spaces following the pandemic. While the WHO guidelines1,37,39 provide overarching emergency protocols for global infection control, regional standards exhibited specific areas of focus. The UK NHS guidelines 58 prioritize wayfinding, patient privacy and safety, visibility and flexible design, whereas the Indian standards 54 emphasize wayfinding, space planning, ventilation and disinfection. The WHO guidelines31,9,37 predominantly addresses space planning, disinfection and wayfinding.
Evaluation framework
Drawing upon the design parameters identified in the literature review and the guidelines provided by international authorities, an evaluation checklist was developed to facilitate POEs of tertiary hospitals, specifically focusing on IPC and well-being. Each parameter within the checklist was assigned a weighted score, reflecting its significance in mitigating pathogen transmission and promoting a salutogenic environment. The list of design parameters that must change post-pandemic in hospital have been shown in Table 3 below.
List of design parameters that have to change post pandemic in hospital
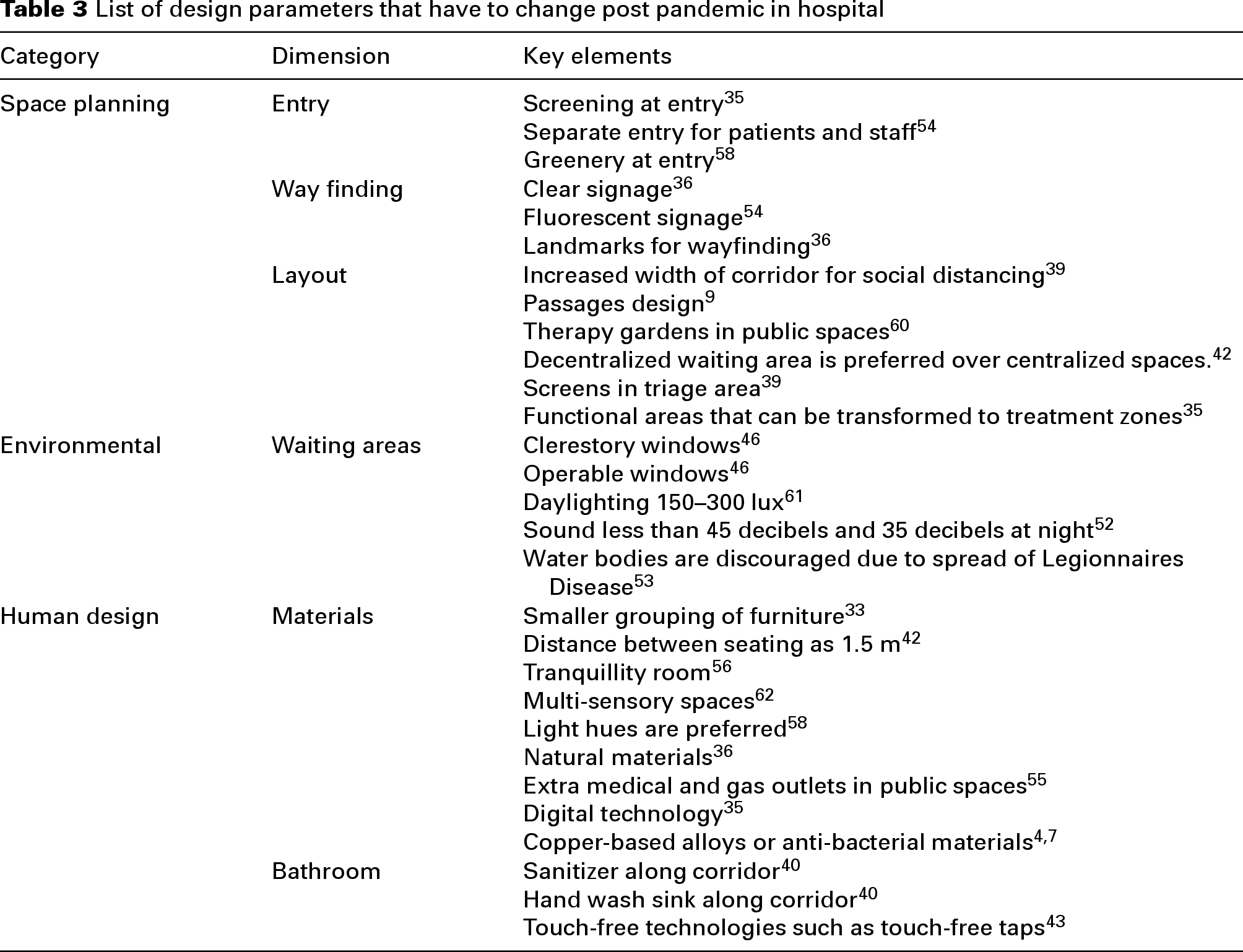
The evaluation framework utilized the design parameters outlined in Table 3, assigning scores ranging from 1 to 3 based on their criticality for IPC. A score of 1 indicated ‘important’, 2 indicated ‘very important’ and 3 indicated ‘extremely important’. During evaluation, a score of 0 signified that the parameter was not met, and a score of 1.5 indicated partial compliance. The cumulative score for a hospital, derived from this system, provides a quantitative measure of its design efficacy in promoting both well-being and IPC.
The weighting of parameters was determined based on the WHO guidelines and established modes of pathogen transmission. As per WHO, 39 pathogen transmission occurs through close-range respiratory droplet exposure, inadequate ventilation and contact transmission via contaminated surfaces. Consequently, disinfection and ventilation were designated as parameters of highest importance, reflecting their critical role in post-pandemic public space design. This scoring system was based on the Clinic Design POE Toolkit developed by the Centre for Health Design (2015). 63
For instance, screening at entry and segregated staff/patient entry points were assigned a score of 3, aligning with WHO space planning recommendations and their direct impact on minimizing close-proximity transmission. Similarly, a flexible design with readily available medical gas and electrical outlets received a score of 3, recognizing its importance in preventing overcrowding and subsequent transmission during patient surges. Wayfinding strategies, such as signage and colour-coded floor markings, were assigned a score of 2, acknowledging their role in optimizing patient flow and reducing close-proximity interactions, as highlighted in multiple standards.
Post-occupancy evaluation
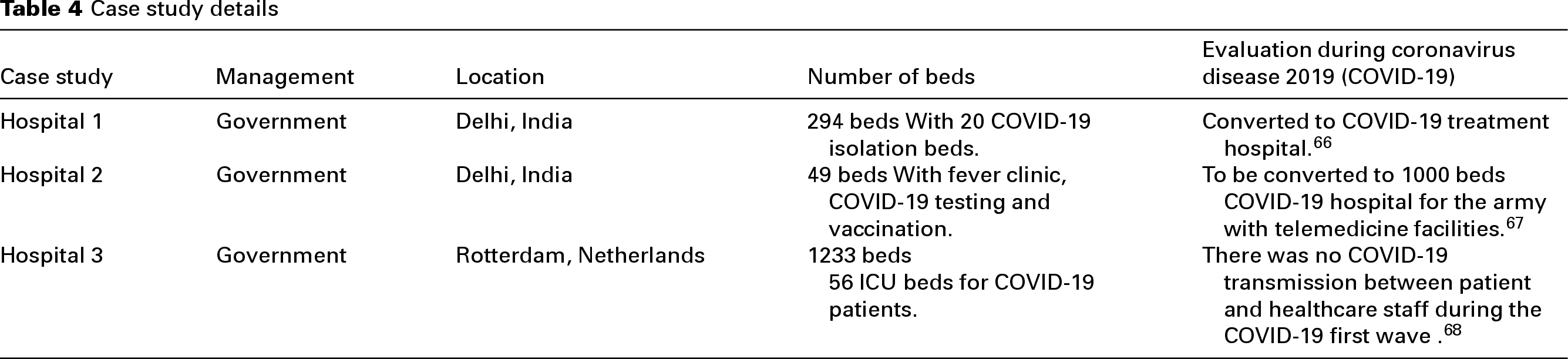
To evaluate the effectiveness of the developed evaluation checklist, a POE was conducted across three tertiary hospitals. The case studies were selected based on the presence of COVID-19 testing or isolation wards, a minimum of one year of operational history, and their status as super-specialty institutions. Two hospitals were located in Delhi, India, representing a developing country facing significant COVID-19 challenges. The third hospital was located in Rotterdam, Netherlands, representing a developed European nation. It is pertinent to note the distinct healthcare systems: the Dutch system emphasizes long-term care for chronic ailments, basic and essential medical care from visits to general practitioner and supplementary care, 64 while the Indian system employs a three-tiered structure of primary, secondary and tertiary care adopted to provide preventive and curative healthcare. 65 Table 4 below provides the details of the case studies used in the research.
Case study details
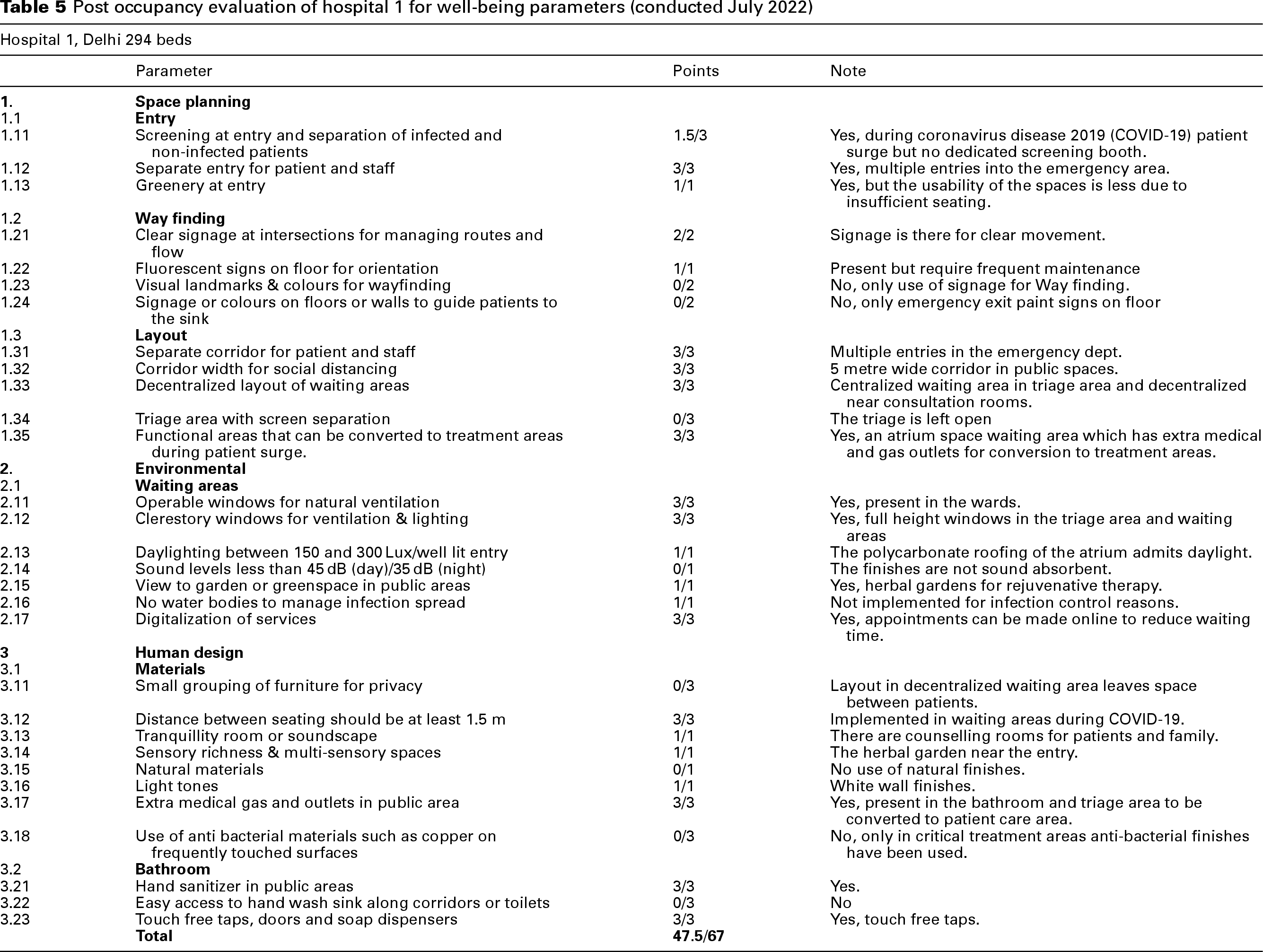
Tables 5–7 show the post occupancy of hospitals 1, 2 and 3, respectively.
Post occupancy evaluation of hospital 1 for well-being parameters (conducted July 2022)
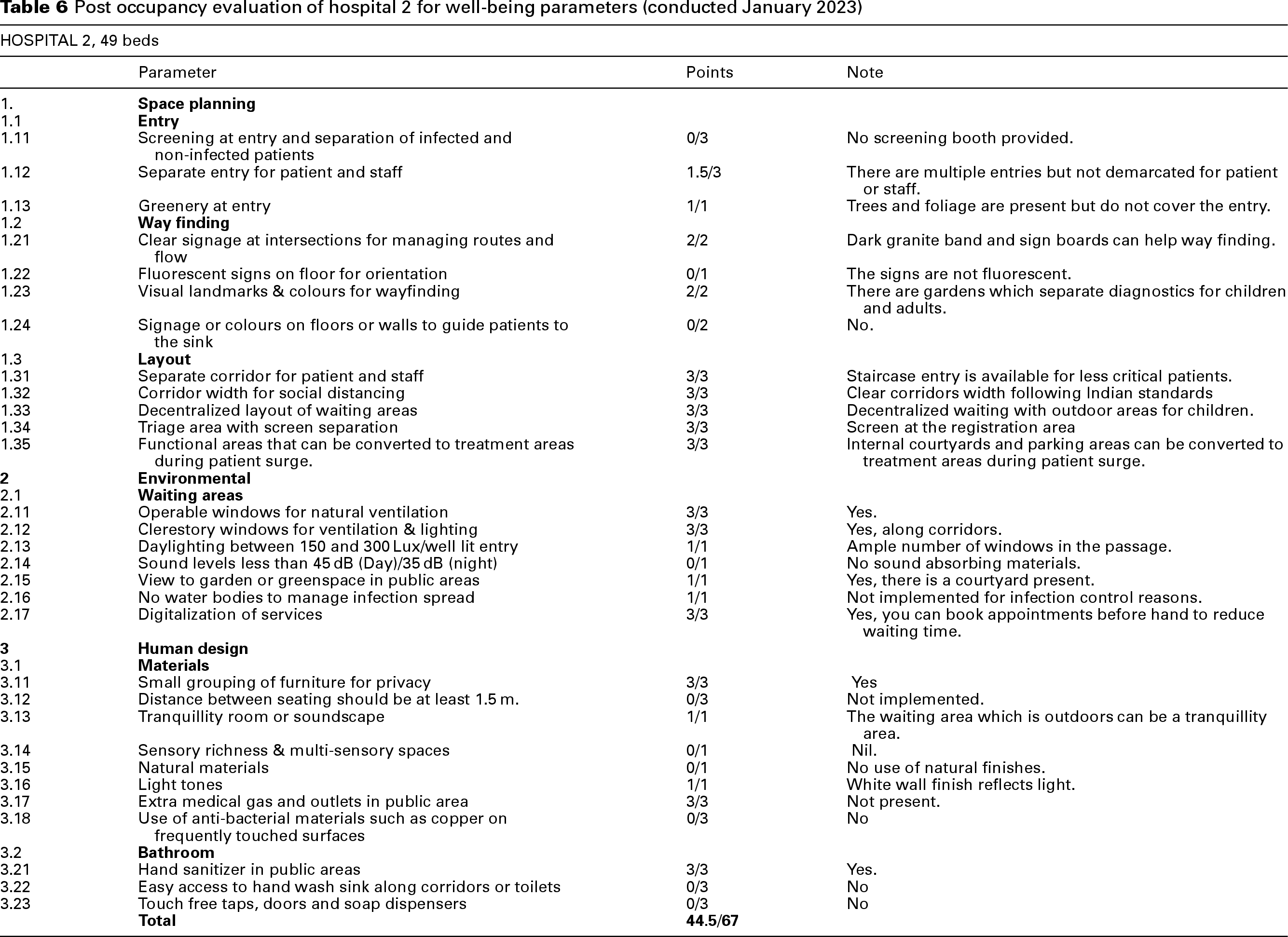
Post occupancy evaluation of hospital 2 for well-being parameters (conducted January 2023)
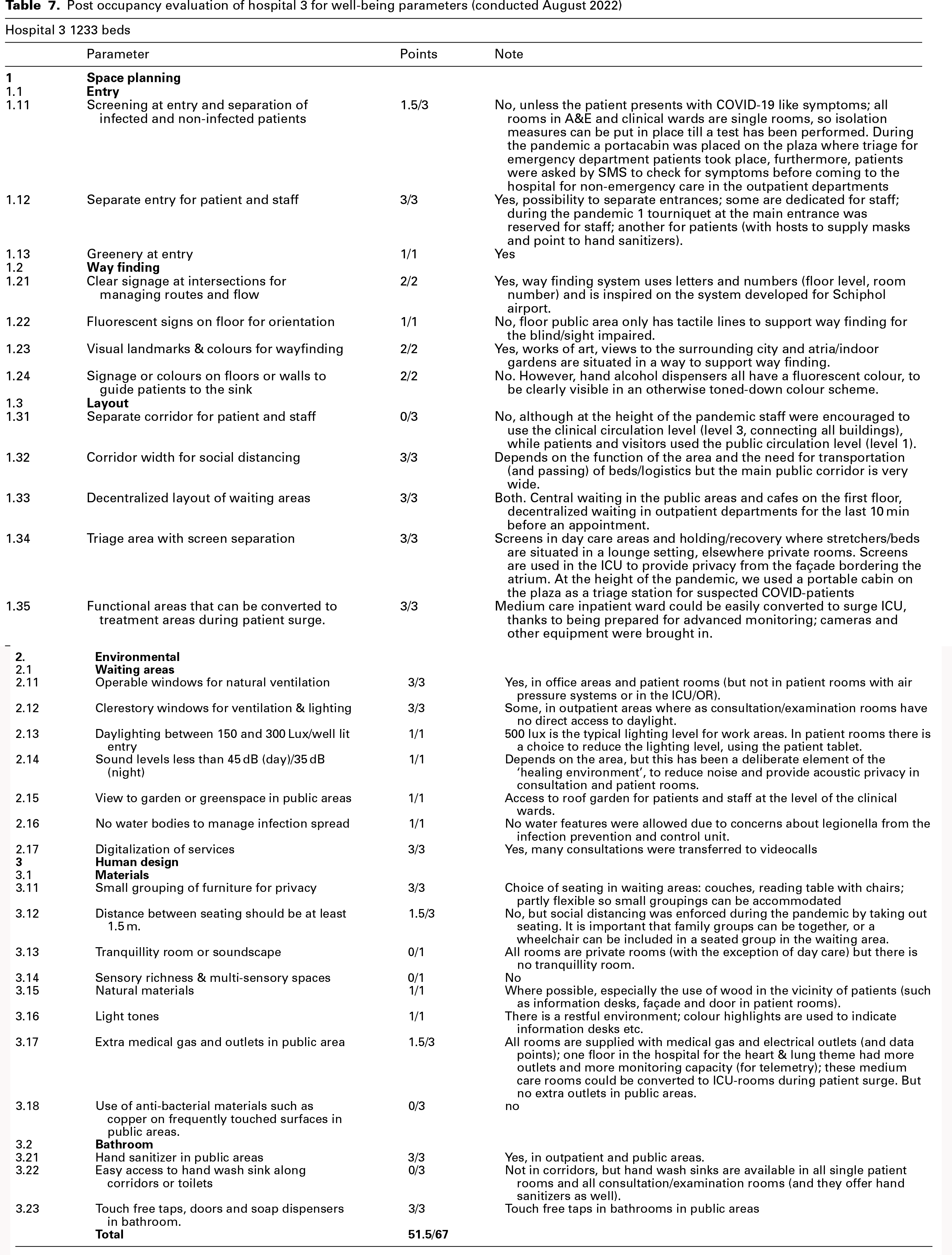
Post occupancy evaluation of hospital 3 for well-being parameters (conducted August 2022)
The facilities were analysed using the evaluation checklist, and the following results were obtained:
Hospital 1 evaluation (Score: 47.5/67)
During the peak COVID-19 period, Hospital 1 implemented a dedicated screening booth and separate entry points for COVID-19 patients. However, these measures were discontinued post-pandemic. Wayfinding was facilitated by fluorescent floor and hanging signage but lacked the landmark-based approach recommended by NHS guidelines. While hand sanitizer dispensers were available, the absence of strategically placed handwashing sinks along corridors represents a potential gap in contact transmission prevention. The 5 m wide corridors align with WHO guidelines, facilitating patient flow and emergency egress. The incorporation of herbal gardens at the entrance promotes well-being, consistent with the UK NHS recommendations. The hospital features a multifunctional hall with a polycarbonate roof, allowing for natural light and surge capacity. The absence of water features minimizes the risk of waterborne infections. The provision of extra medical gas and electrical outlets supports the rapid conversion of triage areas to treatment areas during patient surges. The use of fluorescent floor signs enhances emergency evacuation safety.
Table 6 provides the post occupancy evaluation of Hospital 2 for well-being parameters.
Hospital 2 evaluation (Score: 44.5/67)
Hospital 2 utilized a dark grey granite floor band for wayfinding. However, tactile pathways for visually impaired individuals, as specified in Indian hospital design guidelines, were absent. Gardens served as effective landmarks for interdepartmental navigation. Open-to-air staircases and single-loaded corridors with natural light and ventilation met WHO guidelines. Decentralized waiting areas provided adequate seating and minimized crowding. Artwork in the children's department enhanced the environment, and the double-height, glazed-roof registration area promoted natural light and ventilation. Segregation of staff and patients via screens in the registration area contributed to IPC. Hospital 2 demonstrated compliance with many UK NHS design standards outlined in Table 1.
Table 7 provides the post occupancy evaluation of Hospital 3 for well-being parameters.
Hospital 3 evaluation (Score: 51.5/67)
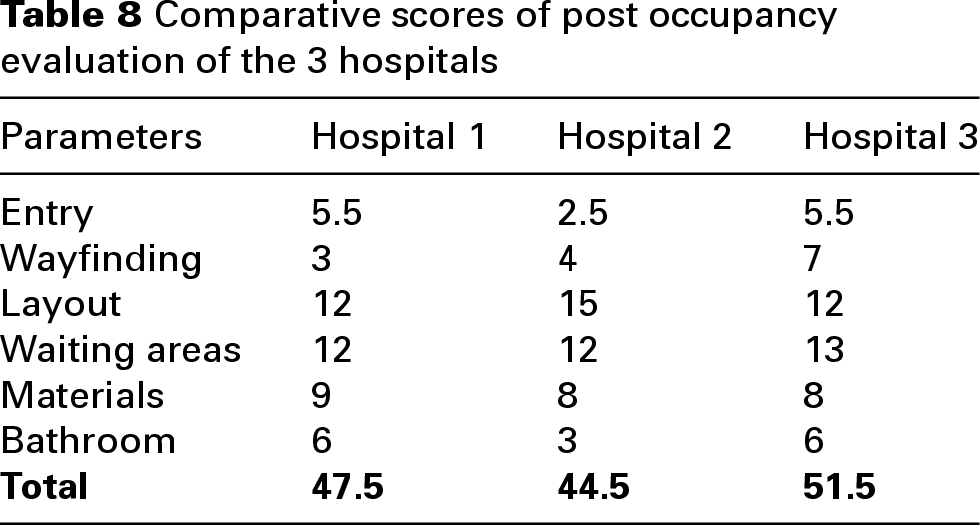
Hospital 3's wayfinding system, inspired by airport design, incorporated tactile lines for visually impaired individuals. Artwork, atria and indoor gardens further aided navigation. Operable windows were present in-patient rooms and office areas, except in air-pressurized rooms and ICUs/OTs. Indoor plants were present in public areas, minimizing pollen-related concerns. Daylight levels in work areas met recommended standards, and patient room lighting was adjustable via tablets. The hospital's use of wood finishes, resistant to disinfectants, aligned with Dutch guidelines. Screens in daycare and holding/recovery areas enhanced patient privacy and IPC. A dedicated floor with increased medical gas, electrical outlets and monitoring capacity supported surge capacity. However, Hospital 3 lacked separate patient and staff routes, as recommended by WHO, potentially increasing transmission risk during surges. Furniture spacing did not consistently meet WHO guidelines. The absence of tranquillity rooms or multi-sensory spaces represents a missed opportunity for enhancing staff and patient well-being. Table 8 provides the comparative scores of post occupancy evaluation of the 3 hospitals.
Comparative scores of post occupancy evaluation of the 3 hospitals
Group discussion
The focus group discussion served as a critical analytical tool to explore the complex relationship between salutogenic design principles and the exigencies of IPC in post-pandemic hospital environments. By engaging experienced architects and researchers from diverse geographical contexts, the discussion aimed to validate and expand upon the findings of the literature review and POEs.
The focus group, held on 30 November 2022, was organized by the University following a webinar on “Healthy Spaces: The Responsibility of Architects.” The 40-min session convened seven experienced architects and researchers, each with over five years of experience in hospital design, representing India, Spain and the United States. The discussion was facilitated by three faculty members.
Participants were prompted with the central question: “What are the key post-pandemic design strategies for hospitals across diverse geographical contexts?” While many themes corroborated findings from the literature review and evaluation checklist development, the focus group also introduced novel insights which are discussed below. The primary themes emerging from the discussion are visualized in the word frequency chart presented in Figure 2.
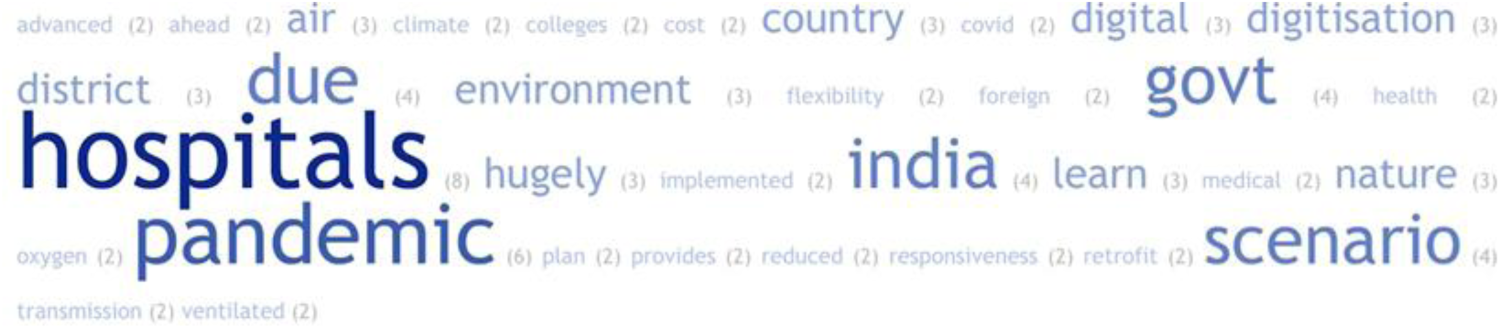
Frequency of terms from focus group discussion.
Digital Technology as a Salutogenic and IPC Strategy: The discussion underscored the potential of digital technologies to enhance both salutogenic approach and IPC. Telemedicine, pre-scheduled appointments, and digital health records were recognized as tools that could reduce crowding, thereby minimizing transmission risk, and also improve patient accessibility and reduce anxiety associated with hospital visits. This resonates with the salutogenic principle of creating environments that foster a sense of control and empowerment.
Natural Ventilation and Environmental Quality: The emphasis on natural ventilation and environmental quality highlighted the inherent tension between salutogenic principles and IPC requirements. While natural ventilation promotes well-being by providing access to fresh air and daylight, it also presents challenges in controlling airborne pathogen transmission. Participants recognized the need for innovative design solutions that balance these competing demands, such as hybrid ventilation systems and advanced air filtration technologies.
Space Planning and Pandemic Preparedness: The discussion on space planning revealed the necessity of integrating flexibility and containment strategies to create pandemic-resilient hospitals. The adoption of dedicated COVID-19 blocks, as mandated by the Indian government's Ayushman Bharat Scheme, exemplifies a proactive approach to isolating infectious patients. However, participants also stressed the importance of flexible spaces that can be rapidly adapted to accommodate patient surges, highlighting the need for designs that anticipate future health crises.
Sustainability, Flexibility and Well-being: The focus group discussion emphasized the importance of a holistic approach that integrates sustainability, flexibility and well-being. Retrofitting hospitals, as suggested by Panellist 3, aligns with both environmental sustainability and resource efficiency, while flexible designs, as advocated by Panellist 2, ensure adaptability to evolving healthcare needs. The recognition of healthcare worker well-being, as highlighted by Panellist 2, underscores the importance of creating supportive environments that mitigate the psychological impact of pandemics.
The emergent themes from the discussion are shown in Figure 3 below.
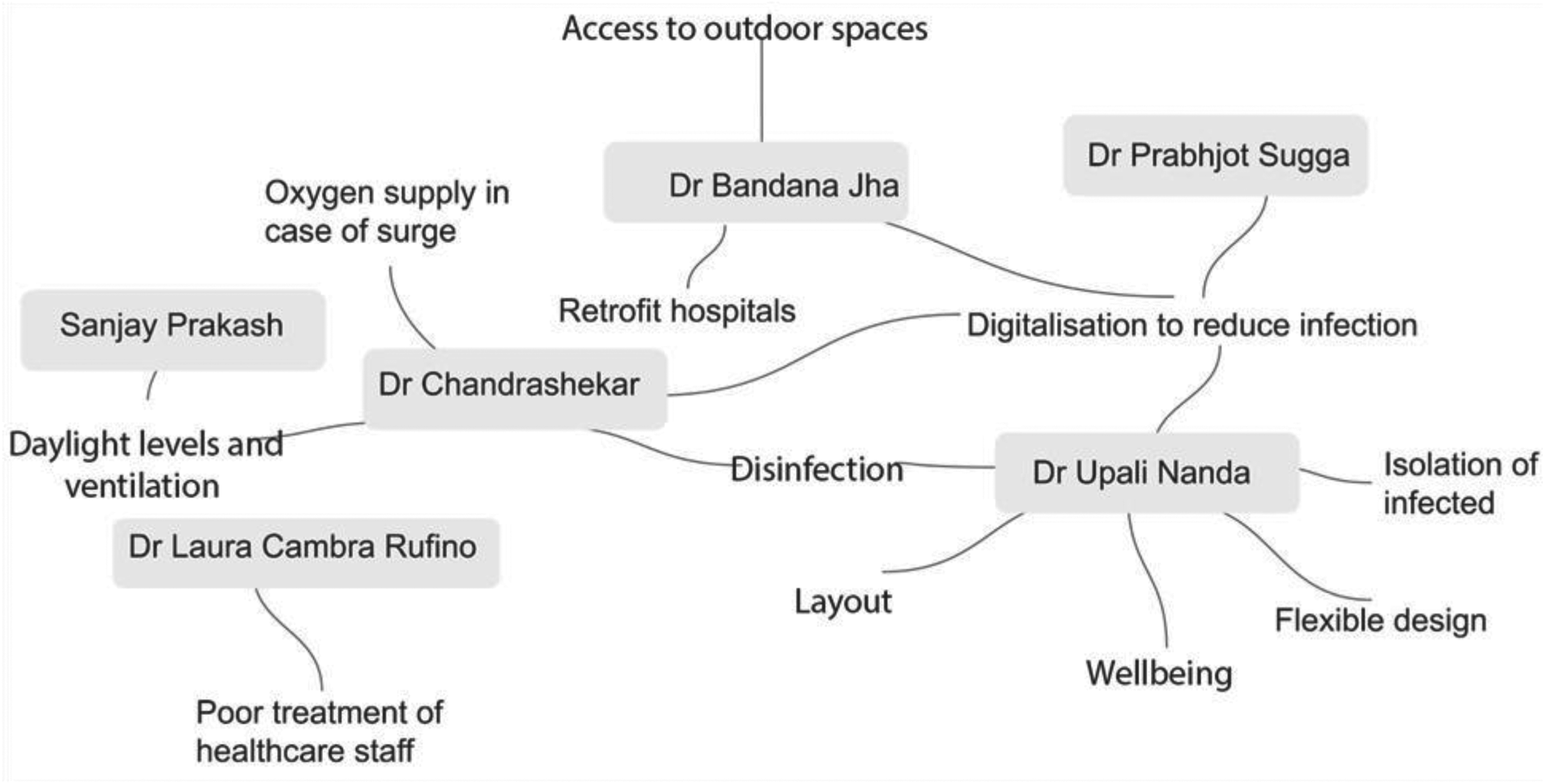
The connection of themes from focus group discussions
The focus group discussion reinforced the need for a design framework that integrates salutogenic principles and IPC requirements. As depicted in Figure 3, disinfection, natural light and ventilation emerged as key design priorities. However, the discussion also highlighted the importance of considering the broader context, including digital technologies, flexible spaces and healthcare worker well-being. By adopting a holistic approach that balances these competing demands, designers can create hospital environments that promote both well-being and resilience in the face of future health challenges. The continued importance of design strategies such as furniture grouping, decentralized waiting areas, and effective wayfinding, even beyond strict social distancing mandates, reflects the ongoing need to mitigate infection spread while enhancing occupant well-being. 35
Discussion and conclusion
This study sought to bridge the gap between salutogenic design principles and the stringent requirements of IPC in tertiary hospital public spaces, particularly in the context of post-pandemic healthcare. Through a systematic literature review, the development of a novel evaluation checklist, and a focus group discussion with expert practitioners, this research has demonstrated the feasibility and necessity of integrating well-being considerations into IPC strategies.
The initial phase of this study involved a comprehensive literature review, comparing international design guidelines from organizations like the WHO, UK NHS, NBHF and IPHS, alongside relevant journal publications released post-2020. This review served to identify key design parameters that demonstrably influence both patient well-being and pathogen transmission within tertiary hospital public spaces. These parameters were then systematically translated into a practical evaluation checklist, designed to provide a standardized tool for assessing the effectiveness of existing hospital designs in promoting both salutogenic principles and IPC.
Subsequently, a rigorous POE was conducted, utilizing the developed checklist to assess three diverse tertiary hospitals located in Delhi, India and Rotterdam, Netherlands. The POE revealed a clear correlation between higher evaluation scores and the consistent prioritization of specific design elements. Notably, Hospital 3 in Rotterdam, which achieved the highest score, demonstrated a strong emphasis on wayfinding, flexible design and environmental quality. These design priorities directly align with both salutogenic principles, which aim to create health-promoting environments and IPC best practices, which focus on minimizing pathogen transmission. This finding highlights the practical applicability of the developed checklist and reinforces the importance of integrating these design considerations into hospital planning.
The following discussion examines the results of the POE through two primary lenses: Design elements (physical infrastructure, spatial configuration and material choices) and operational practices (policies, staffing and resource management). We also considered implementation cost and feasibility based on occupancy as a framework to prioritize interventions and modifications that could be carried out without major disruption to existing operations.
Hospital 1 demonstrated strengths in materials selection and entry design due to effective management decisions and design choices. However, several design-related issues were identified in wayfinding, including insufficient visual landmarks, colour-coding, and floor/wall signage to guide patients to handwashing facilities. These represent low-cost, post-occupancy modifications that could significantly improve infection control. The absence of privacy screens in the triage area is an operational issue that can also be readily addressed. While Hospital 1 meets most environmental parameters, sound level requirements remain unmet and could be resolved by adding acoustic panels. Additional design improvements requiring moderate investment include implementing small furniture groupings for privacy, increasing natural finishes, incorporating antibacterial materials such as copper and installing additional handwashing sinks in corridors.
Hospital 2 excelled in layout design, implementing effective spatial strategies for infection control. However, it received the lowest overall assessment. The absence of an entry screening booth represents both a design and operational challenge but could be resolved at low cost in a post-occupancy context. Bathroom design issues, including limited handwashing access along corridors and lack of touch-free fixtures, are design flaws requiring moderate investment. Additional design improvements needed include ensuring 1.5 m minimum seating distance, enhancing sensory richness through multi-sensory spaces, incorporating natural and antibacterial materials, and improving wayfinding with floor-based orientation guides. Some of these like seating distance and signage can be achieved at lower costs, but others including change of materials might have higher costs associated with them. Despite these limitations, Hospital 2 meets most environmental criteria (except sound levels) and all layout requirements.
Hospital 3 successfully implemented all the wayfinding and waiting area criteria. Its primary operational challenge is the lack of separate corridors for patients and staff during non-pandemic periods, a low-cost operational adjustment is needed. Several design enhancements requiring larger investment would benefit both staff and patients, including tranquillity rooms, sensory-rich spaces and antibacterial materials. The facility needs improved access to handwashing facilities along corridors and in toilets which could be implemented at a moderate cost post occupancy. While 1.5 m distancing between seating was implemented during the pandemic, maintaining this standard is an ongoing operational issue that can be simply addressed through revised protocols.
This discussion reinforces the connection between behavioural aspects of the salutogenic approach to the pathogenic focus in terms of infection transmission. According to WHO guidelines 39 pathogen transmission primarily occurs through respiratory droplets, inadequate ventilation and contaminated surfaces. Accordingly, our evaluation framework assigns highest priority (3 points) to features directly impacting these transmission routes. In our proposal contact transmission is reduced through antibacterial materials, publicly accessible hand sanitizers and touch-free fixtures. The respiratory transmission is mitigated through natural ventilation systems and appropriate spatial distancing. Critical spatial configurations include entry screening, separation of patient populations, staff/patient pathway segregation, adequate corridor width, decentralized waiting areas, screened triage spaces, digital service options and appropriate furniture spacing (minimum 1.5 m) further support behaviour that mitigates infection transmission and have thus been highlighted in our evaluation and discussion. The study of literature depicted that functional areas that can be converted to treatment areas during patients surge and extra medical gas and outlets in public spaces are pandemic resilient strategies that should be incorporated to deal with patient surges during a pandemic.
The focus group discussion further validated these findings, emphasizing the importance of digitalization, natural ventilation and access to nature in creating pandemic-resilient hospitals. Notably, the discussion highlighted the inherent synergy between design strategies that promote well-being and those that mitigate infection risk. For instance, strategically placed seating near ventilation openings and decentralized waiting areas not only reduce pathogen transmission through enhanced air circulation and reduced crowding but also contribute to patient comfort and privacy. Similarly, effective wayfinding systems minimize patient stress and anxiety while optimizing patient flow, thereby reducing close-proximity interactions that facilitate pathogen spread.
While our research focused on indoor public spaces, we must acknowledge an emerging body of evidence highlighting the complementary role of outdoor environments in both patient well-being and infection control. Hospital gardens incorporating natural elements such as plants, fresh air, birdsong, sunlight and water features have been shown to promote healing and reduce stress.69,70 From an infection control perspective, studies from Wuhan hospitals demonstrated significantly lower COVID-19 concentrations in outdoor areas, 71 suggesting important design implications. Outdoor spaces offer additional pandemic resilience through flexible design elements that can be repurposed for health screening, medical storage and quarantine functions. Moreover, thoughtfully designed exterior environments can function as “buffer zones” between healthcare facilities and surrounding communities, potentially reducing community transmission. 72 This represents an important area for future research that integrates both infection control and holistic well-being considerations. 35 While our present evaluation framework has remained focused on indoor public spaces, where pre-diagnosis patients spend considerable time near others creating heightened transmission risk, future extensions of this framework might productively incorporate outdoor space assessment alongside the indoor criteria presented here.
Future research could also expand our evaluation framework to address the diverse demographic needs and behavioural patterns that impact infection control efficacy. Different patient populations require tailored design and operational approaches. For children, effective infection control necessitates regular disinfection protocols for play areas, shared spaces and toys. 73 Elderly patients present unique challenges due to compromised immune systems, placing them at heightened infection risk and warranting enhanced protective measures. 74 People with disabilities, who experience disproportionately higher infection and mortality rates, require thoughtful inclusion in pandemic planning through accessible communication methods such as sign language and simplified materials. 75 While our research has not yet been extended to fully account for these population-specific requirements across the design-operational spectrum, future extensions of this framework could incorporate demographic-specific criteria that evaluate how both physical infrastructure and management protocols can be optimized for vulnerable populations. This would create a more comprehensive evaluation tool that recognizes the heterogeneity of healthcare facility users and their distinct infection control needs.
The current research, however, underscores the potential for a paradigm shift in hospital design, moving beyond a purely pathogenic approach to embrace a holistic framework that integrates salutogenic principles and IPC. By creating environments that encourage healthy behaviours and promote psychological well-being, we can enhance patient compliance with IPC measures and foster a culture of proactive health maintenance. This research provides a systematic approach to incorporating recent literature into actionable guidelines and evaluation tools, serving as a valuable resource for architects, hospital administrators and healthcare professionals seeking to optimize the design of tertiary hospital public spaces.
Ultimately, this study advocates for a design philosophy that recognizes the interconnectedness of physical and psychological health. By prioritizing both well-being and IPC, we can create hospital environments that not only effectively manage infectious diseases but also contribute to the overall health and resilience of our communities. This is not simply a matter of architectural aesthetics, but a crucial component of building a robust and responsive global health infrastructure.
Footnotes
Acknowledgments
The authors would like to acknowledge Professor Manoj Mathur, Professor Dr Bandhana Jha, Professor Dr Chandrashekar, Dr Upali Nanda and Dr Laura Cambria Rufino for being part of the focus group discussion. The authors would like to acknowledge Mrs Soumya Uttam for helping record the minutes of the focus group discussion.
Author's contribution
The corresponding author's (Priya Boby) contribution was writing the research, conducting case studies and chairing the group discussion, Anil Dewan and Prabhjot helped with the case studies, supervized the focus group discussion and proofread the paper. Amit Srivastava proofread the paper, helped write the paper and improved the structure of the paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.