
Abstract
Objective:
This paper evaluates the implementation fidelity of Family Partner, a home-visiting intervention from the child welfare service that aims to reduce child maltreatment in families with complex support needs.
Method:
To assess implementation fidelity, we utilized self-reported routine data from practitioners delivering the intervention, comprising 1657 reports concerning 19 enrolled families. Furthermore, five in-depth qualitative interviews and two focus groups were conducted with practitioners. Descriptive analyses were conducted on quantitative data, and thematic analysis on the qualitative data.
Result:
The critical components for the implementation of the Family Partner intervention were generally met, with the exception of the requirement to conduct three home visits within the first 10 days of the intervention. Additionally, the quality and structure of the practitioner-reported routine data presented challenges in accurately assessing fidelity.
Conclusions:
Keywords
Background
The consequences of child maltreatment can be severe, including increased risks of adult mortality [1], mental health problems [2], and a higher likelihood of perpetrating violence [3]. Home-visitation programs have shown significant effectiveness in reducing maltreatment [4]. For instance, early prevention home-visiting programs have effectively reduced maltreatment by improving child and parent functioning, as well as strengthening parent–child interaction [5,6]. Despite home visitation programs being the most common referred services for children and families in child welfare services (CWSs) internationally [7], Norway has implemented few large-scale home visitation programs in CWSs [8]. Given the severe and long-term health consequences of child maltreatment, effective prevention through early home-visiting interventions represents a critical public health strategy. In response to the Norwegian CWSs’ need for home-visiting interventions, the Family Partner program was developed in conjunction with the practice field and evaluated through a pilot randomized trial [9]. A crucial component of evaluating the intervention’s effectiveness involved assessing its implementation fidelity.
The expanding field of implementation science in home-visiting programs has shown that fidelity, the degree to which an intervention is delivered as designed, is essential to treatment effectiveness [10 –12]. Evaluating implementation fidelity serves several essential purposes. First, it ensures that practitioners deliver the intervention in alignment with its original design [13,14]. It also provides valuable insights into how the intervention is used in practice [15], and identifies both barriers and facilitators to successful implementation [15,16]. Moreover, fidelity data inform modifications to improve the intervention and reveal whether additional practitioner training is required [17]. Understanding fidelity helps explain why an intervention might or might not yield the expected outcomes [15] and identifies practice changes that might influence its effectiveness [10]. Without measuring fidelity, we cannot determine whether null effects reflect an inadequate program model or poor implementation. Implementation science highlights fidelity as a critical determinant of program effectiveness [10,12]. However, interventions delivered in child welfare are embedded in complex, often crisis-driven service contexts, where strict adherence to manuals can be challenging and where adaptations might be necessary to remain feasible and acceptable. Recent research therefore argues for a balance between fidelity and contextual adaptation, sometimes described as “flexible fidelity,” to preserve core mechanisms while allowing tailoring to local realities [18,19]. This makes fidelity assessment particularly important in child welfare, both to document adherence and to distinguish between productive adaptations and deviations that might undermine effectiveness.
Several barriers have been identified in the implementation of early intervention programs. Banda et al. [20] found that barriers include limited trust in the child welfare system to provide or facilitate access to appropriate services, weak communication between workers and families, and systemic issues such as unclear joint child welfare and domestic violence policies, missing guidelines for cross system collaboration, and high staff turnover. These challenges are further compounded by the difficulty of balancing program objectives with the immediate needs of families, highlighting a persistent gap between the intended goals of early intervention programs and the realities of implementing them in practice.
Frontline workers highlight training and organizational support as a contributing factor to implementing Evidence-based intervention [21], as well as the suitability of the intervention to the family’s needs and acceptability of evidence-based practice [22,23]. A systematic review on factors for evidence-based implementation in CWSs found that successful implementation is often dependent on a multitude of additional factors, namely funding, collaboration with external stakeholders, the agency culture, staff culture, and client resistance to the intervention and leadership support [24,25].
Aim of the study
Using quantitative and qualitative process data, we assess fidelity to the core components of the Family Partner intervention: (a) meeting frequency during the first 10 days, (b) intervention duration across phases, (c) meeting frequency across phases, and (d) pre-defined meeting topics per phase. This leads to our research questions: to what extent is the intervention delivered as intended within CWSs?
Data and methods
This is a mixed methods process evaluation examining implementation fidelity combining descriptive quantitative analysis of routine practitioner reports with qualitative interviews and focus groups interviews analyzed thematically.
The Family Partner intervention
Family Partner is an intensive and flexible home-visiting intervention aimed at reducing child maltreatment in families with complex support needs, namely difficulties across multiple life domains, including mental health problems, substance use, poor physical health, limited emotional coping, high conflict, unstable relationships or recent break-ups, and economic hardship.
The intervention seeks to strengthen parenting skills, parental self-efficacy, trust in welfare services, and overall child well-being. A Family Partner is a practitioner employed within CWSs, responsible for providing tailored and supportive assistance to each family. The target group consists of families with at least one child aged 0 to 12 years who might be exposed to harmful caregiving conditions, which include physical and psychological violence, sexual and emotional abuse, and neglect. Families are included in the intervention based on the discretion of child welfare workers. Although their needs are heterogeneous, the Family Partner intervention is designed to tailor support to the specific circumstances of each family.
Participating parents often face challenges related to both emotional and practical aspects of parenting. The intervention includes parent training, regular home visits, practical assistance, and monthly scoring forms completed by both parents and children on topics such as housing, finances, daily routines, and relationships. It also places strong emphasis on building a trusting relationship between practitioner and parent, and on coordinating services across the welfare system. Each CWS office provides two Family Partners. Although a bachelor’s degree in social work or child protection is preferred, it is not a formal requirement. The intervention is designed to last nine months, with the option of extending to 12 when needed. Families typically receive between 50 and 100 sessions of direct contact, corresponding to around 6 h of weekly support, which may include home visits, interdisciplinary meetings, and other forms of contact such as phone calls or text messages.
The intervention is structured into three phases—start-up, working, and ending—each lasting about three months. In the start-up phase (months 1–3), the focus is on building a trusting relationship, with the Family Partner working to understand the family’s needs and identify available resources. At least three home visits are required within the first 10 days.
Early scheduling reduces the risk that parents postpone sessions or that practitioners become occupied with other urgent cases, which enables a faster and more efficient start for all involved.
In the working phase (months 3–6), the emphasis shifts from practical support and relationship-building to more active and intensive guidance. The Family Partner helps the family tackle specific challenges and develop sustainable strategies for daily life. In the final phase (months 6–9), support is gradually reduced to encourage independent management, while ensuring a clear and well-communicated transition. Home visits become less frequent and are supplemented with phone-based support. See Figure 1 for the theory of change, which outlines how the inputs and activities described above are expected to influence short-term and long-term outcomes and the overall impact of the intervention. The model specifies the proposed causal pathways linking each phase of work to intended changes and identifies key factors that might moderate these processes. The core of the theory lies in the relationship between the families, the Family Partner and expected outcome, reflecting previous literature on home visitation [26,27].

Theory of change.
Recruitment of the families to the intervention
Participants were identified and recruited by CWS caseworkers at the three participating offices. Eligibility was assessed by caseworkers based on level of concern and perceived fit with the Family Partner intervention, using clinical judgment rather than a standardized screening tool. When a family was referred to the office, caseworkers evaluated whether they met the inclusion criteria and, if eligible, invited them to participate in the study. Families who consented completed a baseline questionnaire before being randomized in a 1:1 ratio to the intervention or control condition. Allocation was concealed from both participants and staff at the point of randomization. After randomization, researchers received the allocation information and informed the relevant CWS staff.
Data collection procedure
The data presented in this study were collected as part of a pilot random controlled trial of the Family Partner intervention [9]. The fidelity data consist of entries registered on online registration forms by Family Partners during or following each meeting or contact with all the 19 families in the intervention group. To supplement this data, five in-depth interviews and two focus group interviews were conducted with Family Partners. The focus group interviews covered experiences related to delivering the program, while the individual interviews focused on experiences with recruitment, randomization, and screening.
Participants were informed about the research project prior to the interviews and provided informed consent. The semi-structured interviews, each lasting between 50 and 75 min, were audio recorded and transcribed verbatim using Whisper by OpenAI (on a computer for increased confidentiality). Transcripts were reviewed and corrected by a research assistant. The study received ethical approved from The Norwegian Agency for Shared Services in Education and Research (reference number: 804402).
Measures
Fidelity data in this study were collected through digital registration forms developed jointly by the research team and Family Partner practitioners. After each contact with a family, practitioners completed a checkbox-based form documenting the meeting’s location, main focus, topics discussed, and duration. The form included predefined categories (see Figure 4) to standardize reporting on the main topic of each session. Its purpose was to provide a structured overview of each meeting and inform the research team about the activities conducted across services.
The registry forms did not indicate which intervention phase the Family Partners were operating in. Phase classification was therefore derived analytically by combining the date of the meeting or contact with the recorded enrollment date and the date of the final registration. The intervention consists of three sequential phases of approximately three months each, and some families received an extension during the middle phase (the working phase), resulting in a total duration of approximately 12 months for those cases. Because exact enrollment and completion dates were available for each family, all observations could be assigned to the appropriate phase.
The fidelity criteria applied in this study are based on the delivery standards specified in the intervention description. For four indicators, the manual provides explicit cutoffs, and fidelity was coded as met or not met according to whether practitioner reports matched these thresholds. These cutoffs are completion of three home visits within the first 10 days, an intervention length not exceeding nine months (or 12 months with an approved extension), a total of 50 to 100 meetings delivered, and at least three home visits within the first 10 days.
For the phase-specific indicators, the manual defines expected thematic phases rather than quantitative thresholds. Fidelity was therefore assessed by examining whether the content of meetings reflected the prescribed topics for each phase. This included a focus on relationship building and practical support in the starting phase, intensive guidance in the working phase, and coordination with other services in the ending phase. The final criterion, a gradual reduction in meeting frequency toward the end of the intervention, is also not tied to a fixed numerical cutoff. Fidelity was assessed by identifying whether a clear pattern of reduced contact could be observed in the data.
Data analysis
Means, medians, and standard deviations were computed by R Studio to examine the number of sessions in each phase of the intervention. Sessions included all registrations done by the Family Partners (i.e. meeting places). The number of visits within the first 10 days, meeting location and topics for each session were analyzed by examining frequencies by phase. Observations containing missing values were excluded from the analysis, and as a result, the sample size (N) might vary across samples.
Qualitative interviews were used to supplement the quantitative data. The qualitative material included in this paper is drawn from a thematic analysis originally published in Finne et al. [28]. The study identified the following themes: acceptability of the Family Partner intervention, practical challenges in conducting the study, CWS as a barrier to the intervention’s reach, practical challenges in conducting the study. For the present study, we used quantitative material as an analytical framework together with previously unused qualitative data as an analytical resource. We selected excerpts that illustrate key implementation challenges.
Results
The findings are presented across four thematic areas based on interviews and registration forms: the intervention’s duration and delivery context, the thematic distribution of Family Partner topics across phases, and benchmarks for fidelity. Qualitative interviews provide insight into Family Partners’ firsthand experiences and help contextualize and interpret gaps in the quantitative data.
The duration and delivery context of the Family Partner intervention
The fidelity data comprises 1657 registries from the Family Partners throughout the intervention period. The duration of the Family Partner intervention among the 19 participating families ranged from 16 to 77 weeks (approximately 4–18 months; M = 55.8 weeks (≈ 13 months), SD = 13.9), with 14–184 sessions per family and an average of 87 (median = 95.0, SD = 46.6). The intervention followed a three-phase structure—start-up, working, and ending—each designed to last about three months, though the working phase could be extended based on family needs. Eleven families (58%) received such an extension. These families averaged 109 sessions, compared with 58 for those without an extension, aligning with the program’s intended intensity of 50–100 sessions per family (Figure 2).
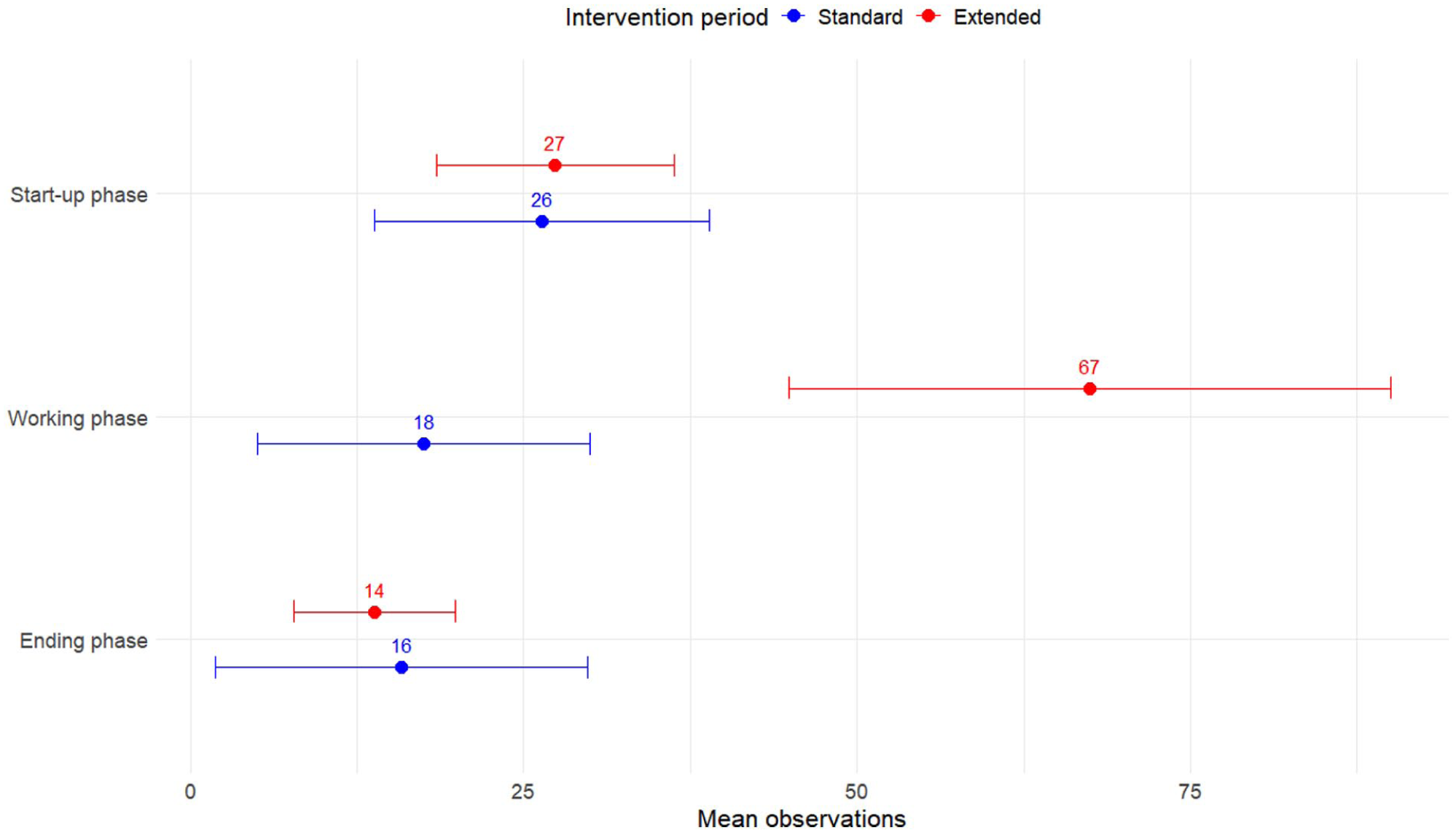
Average number of sessions in each phase of the intervention.
As expected, the ending phase showed a gradual reduction in session frequency, reflecting the program’s aim to promote family autonomy and prepare for closure. The main difference between families with and families without an extended intervention period appeared in the working phase: those without an extension averaged 18 sessions, while those with an extension averaged 67, reflecting the more intensive support provided during this phase.
In addition to home visits, Family Partners also recorded a range of contact types, such as participation in collaborative meetings and communication via text messages, phone calls, and video calls (Figure 3).

Distribution of meeting locations by intervention phase.
Of all registered meetings, 28% took place at the CWS, 25% were via phone or video, 24% were home visits, and 23% occurred elsewhere. The distribution varied by phase: in the start-up phase, 37% of sessions were home visits, reflecting the focus on building trust. Although a key implementation criterion specifies at least three home visits within the first 10 days, this was inconsistently followed. Only eight of the 19 families (42%) received the required number of home visits, while 11 had at least three contacts of any kind with their Family Partner during this period.
During the working phase, home visit frequency declined as other meeting formats increased. Sessions at the CWS accounted for 28%, and phone or video contacts for 29%, while home visits dropped to 19%. This trend continued in the ending phase, with 35% of sessions at the CWS and only 13% as home visits.
Qualitative data confirmed that meetings often take place outside both the CWS and the family’s home. Although home visits are a core element of the intervention, the flexibility of the Family Partner role allows sessions to be adapted to family needs and practitioner preferences. These include joint meetings with other services, such as schools, health or social services, or informal encounters during daily activities, like conversations in the car, during a walk, or at children’s extracurricular events. One Family Partner explained: . . . the flexibility we have allows me to maintain that relationship. She works full-time and is quite frustrated with everything that happens during the day while she’s at work. There are children’s groups, driving back and forth, information here and there, and then she has to take time off, but her employer doesn’t accommodate that. So, the fact that I can meet her in the evening, like, we can meet while her son is at football practice, and we can go for a walk and talk, that, she has said, has been very important.
Thematic distribution of Family Partner topics according to phases
In the registration forms, Family Partners recorded the main topic of each session. As shown in Figure 4, the most frequently addressed topics across all phases were conflict management, collaboration and service coordination, and emotional parenting skills. Conflict management, in particular, showed a notable increase during the ending phase. Practical parenting skills was also a frequent topic, appearing most often in the start-up phase and declining thereafter. Mental health was likewise an important topic, especially during the start-up and ending phases. Family and child observation occurred most frequently in the start-up phase, as expected. Other more practically oriented topics, such as housing and financial support, practical assistance, and work-oriented follow-up were particularly common early in the process, with some showing an increase again in the ending phase.

Topics for the meetings, by phase.
Although relationship-building with parents underlies all other topics, it is also a separate category on the registration form. Relationship-building with parents was most frequent early on, whereas relationship-building with children appeared more often during the working and ending phases. Sensitive issues, such as intimate partner violence and child maltreatment, substance use, and sexual behavior, were less frequent (the latter two topics appearing in 3% or fewer meetings/contacts and not shown in the figure), but they were nevertheless addressed in several sessions.
Although relationship-building with parents is a core component of the intervention, it was recorded relatively infrequently on the registration forms. This may reflect limitations of the registration system rather than low emphasis in practice, as the category appeared last in the list and overlapped conceptually with other categories that might have captured relational work.
In interviews, however, Family Partners strongly emphasized its importance, describing it as a continual effort across all phases. As one Family Partner put it: I believe that building relationships is something we work on continuously, throughout all three phases. It’s not like you establish a relationship in three months and then you’re done with it. No, I see it as an ongoing process. And that relationship can go up and down, it can improve, it can deteriorate over time.
When reflecting on the final phase of the intervention, Family Partners described a growing sense of empowerment and autonomy among families. Trust was highlighted as a key component in this process: But the ending phase has allowed them to gradually take on more responsibility themselves, while we have been there to support them closely and say, “Look, you’re managing! You can do this.” I think the trust they have developed in us, the fact that we have shown them they can rely on us, has, in turn, helped them gain confidence in their own lives. It has shifted their mindset to, “People actually mean well. The world isn’t against us.”
Benchmarks of fidelity measures
The benchmark of fidelity outcomes specifies how practitioners are expected to deliver the Family Partner intervention. Fidelity is assessed against eight criteria. These include completing three home visits within the first 10 days, keeping the intervention within the standard nine months or the extended 12-month limit, and delivering a total of 50–100 meetings. Fidelity also requires that at least three of the meetings in the first 10 days are home visits, that phase 1 focuses on relationship building and practical support, that phase 2 focuses on intensive guidance, and that phase 3 addresses coordination with other services. Finally, practitioners must demonstrate a graduated reduction in meeting frequency in the final phase. Most benchmarks were met (see Table I). The intended duration (nine months, with an optional three-month extension), the target frequency of 50–100 sessions, and the gradual reduction of meetings in the ending phase were all achieved. The thematic focus across phases also aligned with the intervention manual: relationship-building and practical support in phase 1, intensive guidance in phase 2, and service coordination in phase 3. However, the requirement of at least three home visits within the first 10 days was not met.
Benchmarks of fidelity measures.

Discussion
This study examined the degree to which the Family Partner intervention was delivered as intended within CWSs and identified barriers to assessing its fidelity. Overall, the findings indicate that the intervention was implemented with a high degree of adherence to most core components, the total number of meetings, and the thematic structure of the three phases. However, one key benchmark, the requirement for three home visits within the first 10 days, was not achieved, and this deviation raises important questions about the balance between fidelity and necessary adaptation when implementing complex interventions in child welfare settings.
As outlined in the introduction, fidelity is widely recognized as a key determinant of intervention effectiveness [10,12]. At the same time, recent work on complex interventions and implementation argues that fidelity must often be balanced with contextual adaptation in systems such as child welfare, where practice is shaped by crises, organizational constraints, and heterogeneous family needs [18,19]. This tension between adherence and flexibility is central for understanding the deviations observed in the Family Partner intervention. Home visits are typically considered a core mechanism of change in home-visiting models, yet practitioners in this study often adapted contact formats to accommodate families’ schedules, acute stressors, or work obligations. We cannot determine, based on our data, whether these deviations represented necessary and appropriate adaptations or whether they reflected missed opportunities to build the early relational foundation envisioned in the model. The literature suggests that early and intensive contact might be important for establishing momentum in change processes [29], but the empirical significance of early meeting frequency and intensity in this particular intervention remains to be scrutinized. Thus, while some of the observed deviations might align with what Albers et al. [18] describe as “flexible fidelity,” we cannot conclude this with confidence. Instead, the findings underscore the need for fidelity tools capable of distinguishing productive, context-sensitive adaptations from deviations that might undermine the intervention’s mechanisms of change.
Aside from the shortfall in early home visits, the majority of fidelity benchmarks were achieved, which provided preliminary support for moving toward a more rigorous evaluation of the intervention. The findings suggest that the core components of the Family Partner model are implementable within the organizational and practical realities of Norwegian child welfare services. If future impact evaluations of this implementation or of later implementations with comparable fidelity fail to detect effects, these findings suggest that the absence of impact should not primarily be attributed to shortcomings in structural fidelity (e.g. dosage, duration, or thematic sequencing). Instead, attention might need to shift toward the intervention’s theory of change, practitioner competence, or family engagement mechanisms. Based on our observations, the strong qualitative emphasis on flexibility, relationship-building, and trust-building suggests that the relational processes might function as primary mechanisms of change. This aligns with research showing that trust between families and practitioners is central in home-visiting interventions [26] and in child welfare practice more broadly [22].
Although trust emerged repeatedly as a central theme in the qualitative material, it was not systematically measured in the fidelity data. Prior studies conceptualize trust in parent–provider relationships as rooted in reliability, consistency, emotional safety, and partnership [26,30]. In the Family Partner model, trust appears to underpin both engagement and uptake of guidance, two known mediators of intervention outcomes in home visiting interventions. The absence of a structured measure of trust therefore represents a gap in the current fidelity assessment. Future studies should incorporate validated relational measures to better understand how trust develops and contributes to outcomes.
Limitations
One limitation of this study concerns the measurement of fidelity. The registry forms were not designed as fidelity assessment tools, but rather to support the work of Family Partners. Consequently, their design and content present certain limitations when used for fidelity evaluation. Furthermore, the flexible nature of the Family Partner intervention complicates the process of defining and measuring fidelity. While this flexibility is integral to tailoring the intervention to diverse family needs it also complicates efforts to develop standardized benchmarks. In addition, a key limitation is that fidelity was assessed solely through practitioner-reported data, without observational assessments or feedback from service users. Implementation research stresses the importance of multi-informant fidelity measurement [16,17]. Practitioner self-report tends to inflate fidelity estimates and might obscure deviations or adaptations not recognized by the practitioners themselves. Similarly, the lack of user perspectives limits insight into whether families experienced the intervention as intended, particularly regarding the relational components that practitioners emphasized as central. There was a lack of qualitative data to explain why benchmark criteria were met in some cases and not in others, which further limits our ability to interpret fidelity.
Conclusion
In sum, this study provides preliminary evidence that the Family Partner intervention can be implemented with high structural fidelity in Norwegian child welfare services, while identifying key uncertainties related to adaptation, relational processes, and measurement. Overall, family partners largely adhered to the intervention manual, with one notable exception: the requirement to conduct at least three home visits within the first 10 days of the intervention. The present data do not explain non-adherence to this criterion. Future research should therefore assess both the feasibility and the added value of delivering these early visits, particularly during the initial days of the intervention. More rigorous fidelity measurement in a full-scale randomized controlled trial or other robust effect evaluation is necessary to determine whether and how the Family Partner model benefits families with complex needs.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This work was supported by the Research Council of Norway under project no. 320080, Family Partner – Co-development, Implementation and Evaluation of a Child Maltreatment Prevention Intervention.