
Abstract
Aims:
Overdose deaths have been increasing in parts of Europe, including Norway, where opioid analgesics have been the leading cause since 2016. This study quantifies the risk of overdose death following exposure to dispensed opioid analgesics, stratified by sex and age, and examines associated causes of death.
Methods:
Nationwide data from 2010 to 2018 on overdose deaths were obtained from the Norwegian Cause of Death Registry and linked with the Norwegian Prescription Database to identify prior opioid analgesic dispensations. Aggregated prescription data and population figures from Statistics Norway were also used.
Results:
From 2010 to 2018, 42% of individuals who died from an overdose had been dispensed opioid analgesics in the previous year. Among those dispensed strong opioid analgesics, the overdose death rate was low but exceeded the population death rate among men aged 20–49 and women aged 20–39 years. The rate was higher in men and remained stable over time. Opioids other than heroin or methadone were listed as the cause of death in 62% of cases with prior dispensed opioid analgesics, compared with 24% among those without.
Conclusions:
Background
Over the past two decades, several European countries have experienced rising prescription opioid consumption [1]. Despite this increase, opioid-related problems remain relatively limited in most of Europe [2]. However, overdose continues to be a significant contributor to mortality and morbidity among individuals who use drugs, with Estonia, Lithuania, Sweden, Finland and Norway reporting some of the highest overdose fatality rates [3].
In Norway, the underlying causes of overdose deaths have changed notably over the past 15 years. By 2016, opioid analgesics – a class of medicines with opioids that are used to treat moderate to severe pain – had become the leading cause of opioid-related overdose deaths [4,5]. The number of individuals dispensed strong opioid analgesics at least once per year nearly doubled from 46,500 in 2010 to 84,500 in 2018, while the number dispensed only weak opioid analgesics remained stable at 441,000–485,000 [6]. Estimating the risk of overdose death following exposure to opioid analgesic is therefore essential for targeting prevention strategies.
A systematic review and meta-analysis based of six US studies estimated a pooled overdose crude death rate of 1.1 per 1000 person-years among people prescribed opioids [7]. In a Norwegian study of individuals with dispensed analgesics (opioids or non-opioids) reimbursed for chronic, non-cancer-related pain, the age-standardized overdose death rate was 20.8 per 100,000 person-years [8]. Most studies, however, report population-based rates rather than rates among those dispensed opioid analgesics [9], underscoring the need for further research in this area.
A meta-analysis identified substance use disorder as the strongest risk marker for fatal prescription drug overdose, with psychiatric disorders, white race, male sex and age 35–44 years also associated with higher risk. Additional markers – including opioid type, dose, potency, polysubstance use, frequent emergency department utilizations, doctor shopping and illicit obtained opioids (fentanyl) – were also listed as risk markers [10]. Outside the US, ethnicity may in some countries substitute for race as a relevant marker.
Three Norwegian studies have investigated related aspects of sex and age. A 2016 Norwegian Global Burden of Disease (GBD) study identified alcohol and illegal drug use as leading risk markers of death among individuals aged 15–49, with death rates for men roughly four times higher than for women [11]. Another study found a higher proportion of women among overdose deaths caused by opioid analgesics than caused by heroin [4]. A third reported that opioid analgesic-related overdose deaths more often involved older women with chronic pain and opioid analgesic prescriptions, compared with those who died from other causes of overdose [12]. Together, these findings indicate a need for more knowledge of overdose death risk across age and sex following dispensed opioid analgesics.
Exposure to dispensed opioid analgesic prior to overdose death does not necessarily imply that dispensed opioid analgesic caused the death. Although opioid analgesics listed as the cause of overdose death strengthen the likelihood of a causal link, Norwegian Cause of Death Registry classifications do not specify individual substances. Moreover, it remains unclear whether the opioids involved as cause of death were prescribed or illicitly obtained. Understanding the contribution of dispensed opioid analgesics to overdose death is complex and involves multiple aspects of both individual and public health.
Aims
This study quantifies the risk of overdose death in Norway following exposure to dispensed opioid analgesics within the preceding 12 months. It examines changes in this risk from 2010 to 2018, differences across sex and age, comparisons with population death rates, and the role of opioid analgesics as the recorded cause of death.
Methods
This study used two nationwide data sources to estimate overdose death rates among individuals dispensed opioid analgesics:
Linked individual-level data from the Norwegian Cause of Death Registry (NCDR) [5] and the Norwegian Prescription Database (NorPD);
Aggregated anonymized data from the NorPD and Statistics Norway [6].
The first dataset is part of a linked register study, Drug-Induced Deaths 2003–2018, approved by the Regional Committee for Medical and Health Research Ethics (REK South-East approvals 2019/543 and 2020/10154). It includes overdose deaths in the NCDR from 2010 to 2018.
Deaths in the NCDR were coded according to the 10th revision of the International Classification of Diseases (ICD-10) [13]. Inclusion criteria of overdose death followed the European Union Drugs Agency’s (EUDA’s) definition of drug induced death [14], which includes:
Mental and behavioural disorders due to psychoactive substance use: opioids (F11), cannabinoids (F12), cocaine (F14), other stimulants (F15), hallucinogens (F16) or multiple drug use (F19));
Poisonings (accidental: X42, X44; intentional: X62, X64; or undetermined intent: Y12, Y14) involving narcotics (T40.x) or psychostimulants (T43.6).
Before 2003 – and still in some European countries – Cause of Death Registries used F-codes instead of X/Y poisoning codes for overdose deaths. In Norway, F-codes account for about 10% of overdose deaths, typically when the deceased was a known drug user and the cause of death was clearly a drug overdose, without forensic autopsy. Thus, in Norway, the EUDA definition of drug-induced death corresponds closely to overdose death.
Table I lists examples of substances underlying overdose deaths based on ICD-10 codes. Opioid analgesics appear under ‘Other opioids’ and ‘Other synthetic opioids’. Throughout this paper, the term ‘opioid analgesic related cause of overdose death’ refers to these categories. Table I is a revised version of a table published by the Norwegian Institute of Public Health [15].
Substances and ICD-10 codes that form the basis of statistics on overdose (drug-induced) deaths.
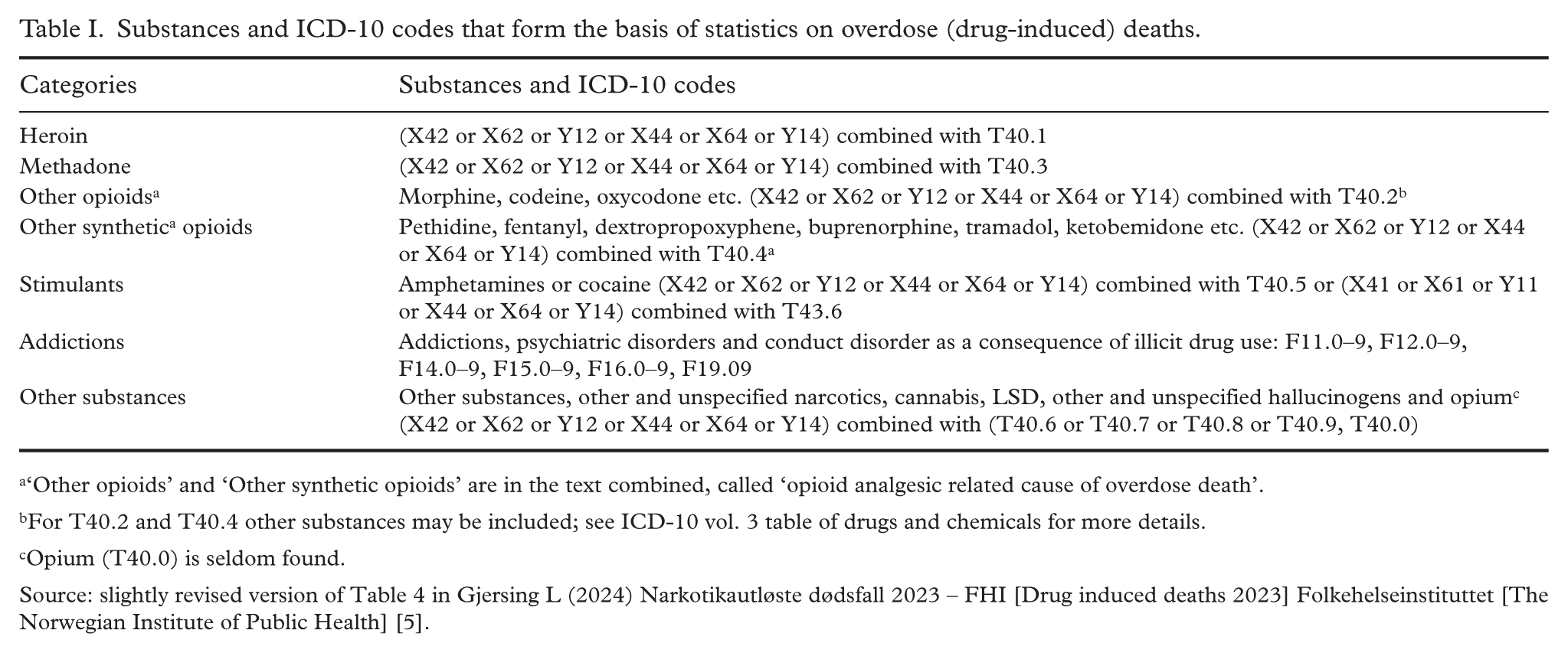
‘Other opioids’ and ‘Other synthetic opioids’ are in the text combined, called ‘opioid analgesic related cause of overdose death’.
For T40.2 and T40.4 other substances may be included; see ICD-10 vol. 3 table of drugs and chemicals for more details.
Opium (T40.0) is seldom found.
NCDR records were linked to data from NorPD on dispensed opioid analgesics within the 12 months prior to death. Details of the linkage and additional findings are reported elsewhere [16].
The second dataset consists of aggregated NorPD data on all individuals dispensed at least one opioid analgesic per calendar year from 2009 to 2018 (2009 included for a 12-month look-back). Data for 2013 were further stratified by sex and age. The NorPD excludes drugs administered in hospitals and nursing homes.
Individuals were categorized by opioid analgesic type dispensed before death. One group included individuals dispensed only weak opioid analgesics: Anatomical Therapeutic Chemical (ATC) codes N02AJ06 (codeine and paracetamol), N02AJ07 (codeine and acetylsalicylic acid), N02AJ13 (tramadol and paracetamol) and N02AX02 (tramadol). The second group included those dispensed strong opioid analgesics. Strong opioid analgesics were defined by the ATC group N02A, excluding the weak opioids mentioned above [17]. Individuals dispensed both weak and strong opioid analgesics were included in the second group.
Methadone tablets can be prescribed for chronic pain in Norway. This form of methadone is classified in ATC group N07BC and is thus not included in the study.
The numerator in the estimator for overdose death risk was the number of overdose death per year in which the deceased had been dispensed opioid analgesics within the previous 12 months. The denominator was the total number of individuals dispensed opioid analgesics each year minus half the overdose deaths that year, approximating person-years at risk. Separate estimates were calculated for weak and strong opioid analgesics and by calendar year.
Sex- and age-stratified data for the total number of individuals dispensed opioid analgesics were available only for 2013. To estimate denominators in overdose death rates across age and sex groups 2010–2018, the 2013 figures were adjusted using the average annual numbers for that period: equal for weak opioid analgesics and 14% higher for strong opioid analgesics. Based on a linear trend for strong opioid analgesics dispensing, these averages were assumed valid for age groups and sex as well, multiplied by 9 to approximate total exposure for 2010–2018.
To contextualize overdose death rates by sex and age, they were compared with average population death rates 2010–2018. Person-years were estimated as the population on 1 January minus half of the deaths during the year. MedCalc was applied to compare death rates and rate ratios and to calculate confidence intervals (CIs) [18]. CIs were reported for males and females aged 20–49 years, the group theoretically at higher risk. Sex was determined using registry data.
The NCDR’s ICD-10 categories do not specify the exact opioid analgesic involved or whether it was legally prescribed or illicitly obtained. Thus, it is not possible to determine causality between dispensed opioid analgesics and overdose deaths. A high proportion of opioid analgesic-related deaths among those with recent opioid analgesic prescriptions suggests a possible link to dispensed opioids, whereas opioid analgesic-related deaths among individuals without prescriptions likely reflect use of illicitly obtained opioids.
Results
Between 2010 and 2018, 42% of individuals who died from overdose had been dispensed opioid analgesics in the preceding 12 months. Among these individuals, 62% had been dispensed only weak opioid analgesics, and 38% strong opioid analgesics.
Among individuals dispensed opioid analgesics, the annual overdose death rate was 21 per 100,000 person-years, comprising 15 per 100,000 for weak opioid analgesics, and 68 per 100,000 for strong opioid analgesics (p<0.0001). For both sexes, the overdose death rate decreased with increasing age among those dispensed strong opioid analgesics (Table II).
Population death rates and overdose death rates for individuals dispensed opioid analgesics in the 12 months period prior to death, by sex and age groups, per 100,000. Rate ratios.
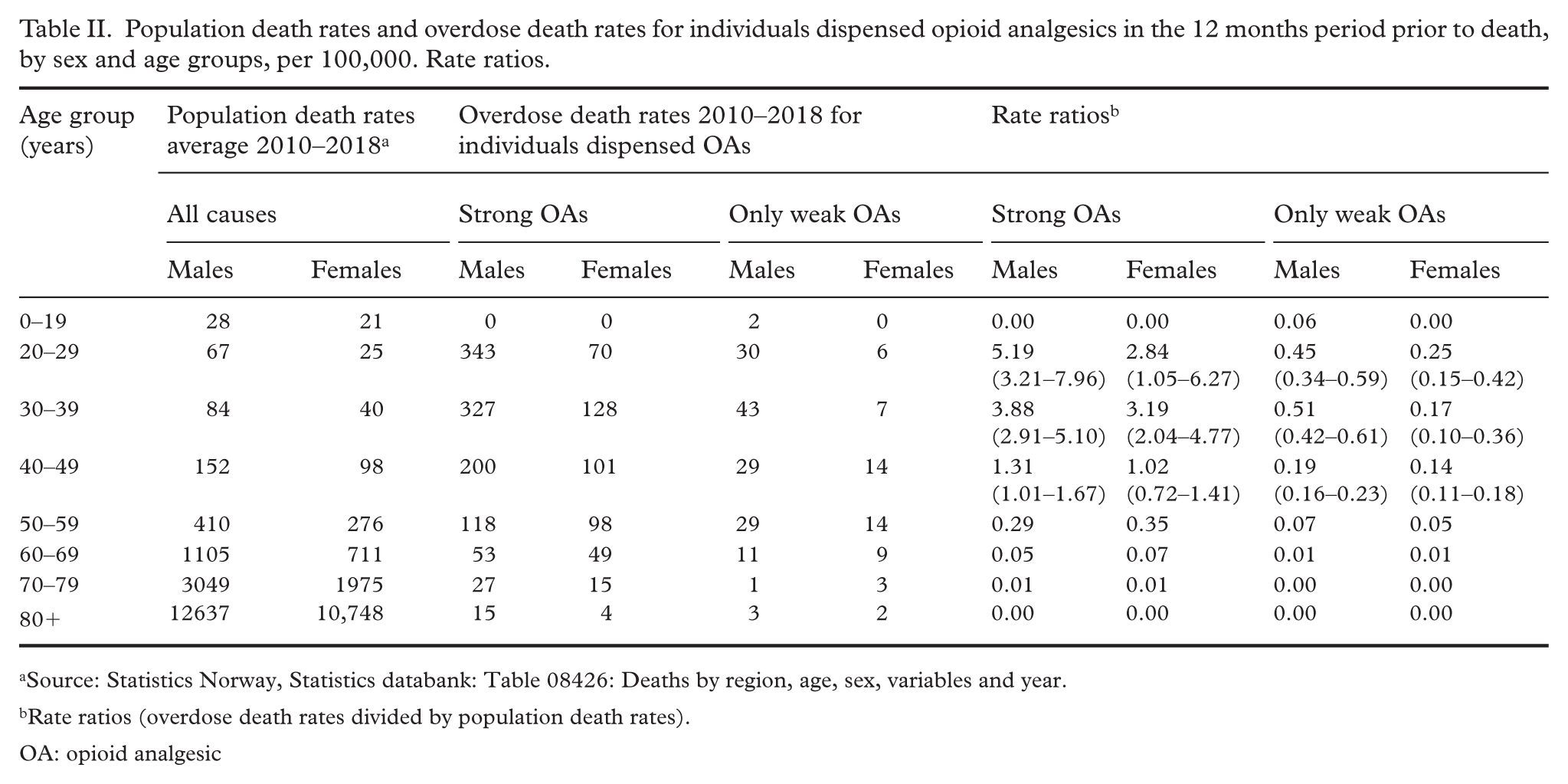
Source: Statistics Norway, Statistics databank: Table 08426: Deaths by region, age, sex, variables and year.
Rate ratios (overdose death rates divided by population death rates).
OA: opioid analgesic
When stratified by sex, the overdose death rate for those dispensed weak opioid analgesics was 23 per 100,000 per person-year for men and 9 per 100,000 for women (p<0.001). Among those dispensed strong opioid analgesics, the corresponding rates were 115 per 100,000 per person-year for men and 52 per 100,000 for women (p<0.0001). The risk of overdose death among those dispensed opioid analgesics remained stable from 2010 to 2018 (test for trend: p= 0.61 for weak opioid analgesics, p= 0.34 for strong opioid analgesics).
The ratio of overdose to population death rates differed significantly from 1 (p < 0.05) for males aged 20–49 years dispensed strong opioid analgesics, indicating elevated risk of overdose death. A similar pattern was observed for females aged 20–39 years (Table II).
Significant differences were found in cause of overdose death according to exposure to dispensed opioid analgesics (see Figure 1). Among individuals without exposure to dispensed opioid analgesics, 23.9% of overdose deaths had an opioid analgesic-related cause, compared with 45.3% among those dispensed weak opioid analgesics and 62.0% among those dispensed strong opioid analgesics. This gradient was consistent across sex and age groups (Table III).
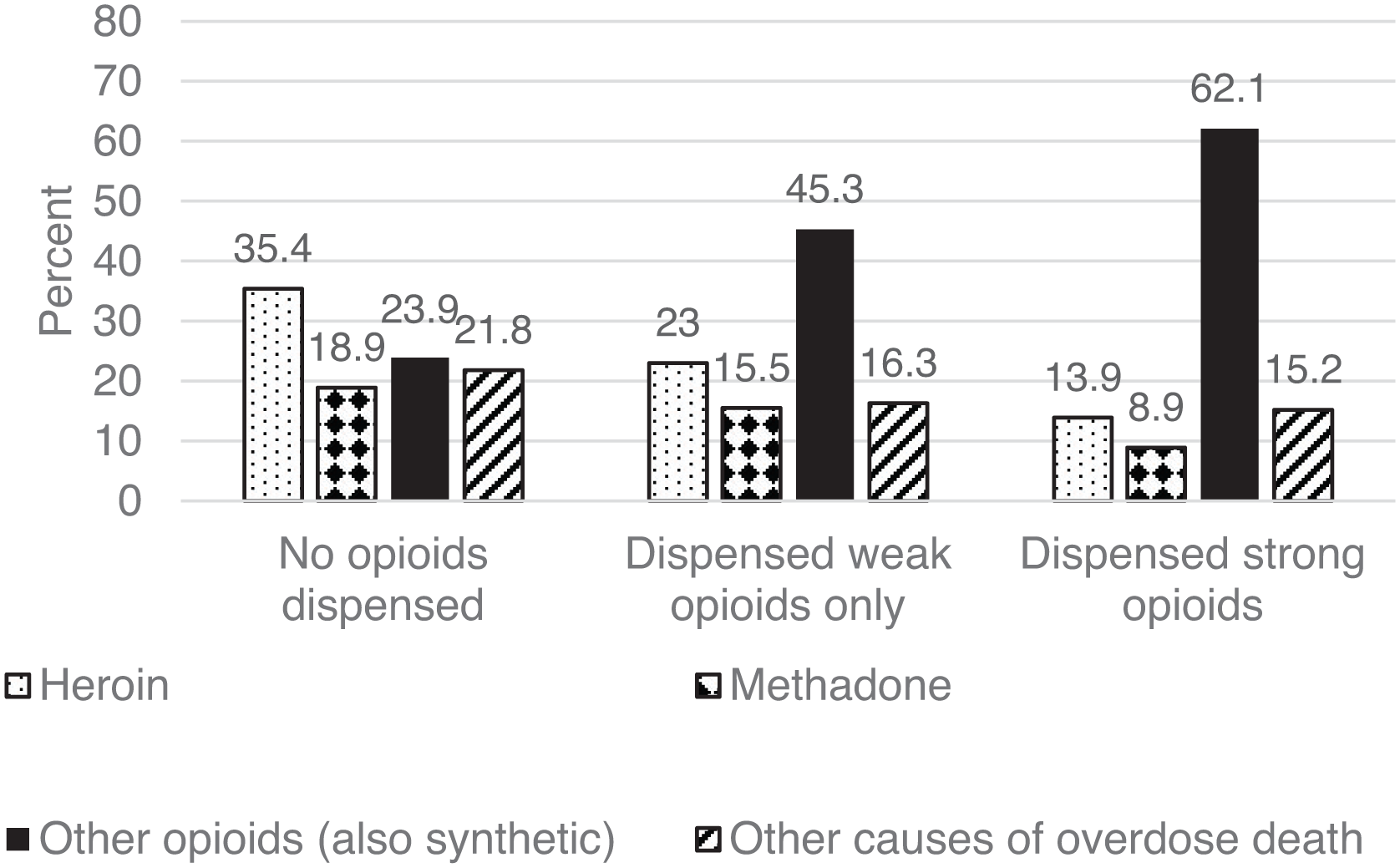
Cause of death for overdose death grouped by exposure to dispensed opioid analgesics in the 12 months period prior to death, 2010–2018.
Underlying cause of overdose death grouped by exposure to dispensed opioid analgesics 12 months prior to death. Sex and age. 2010–2018. Per cent.
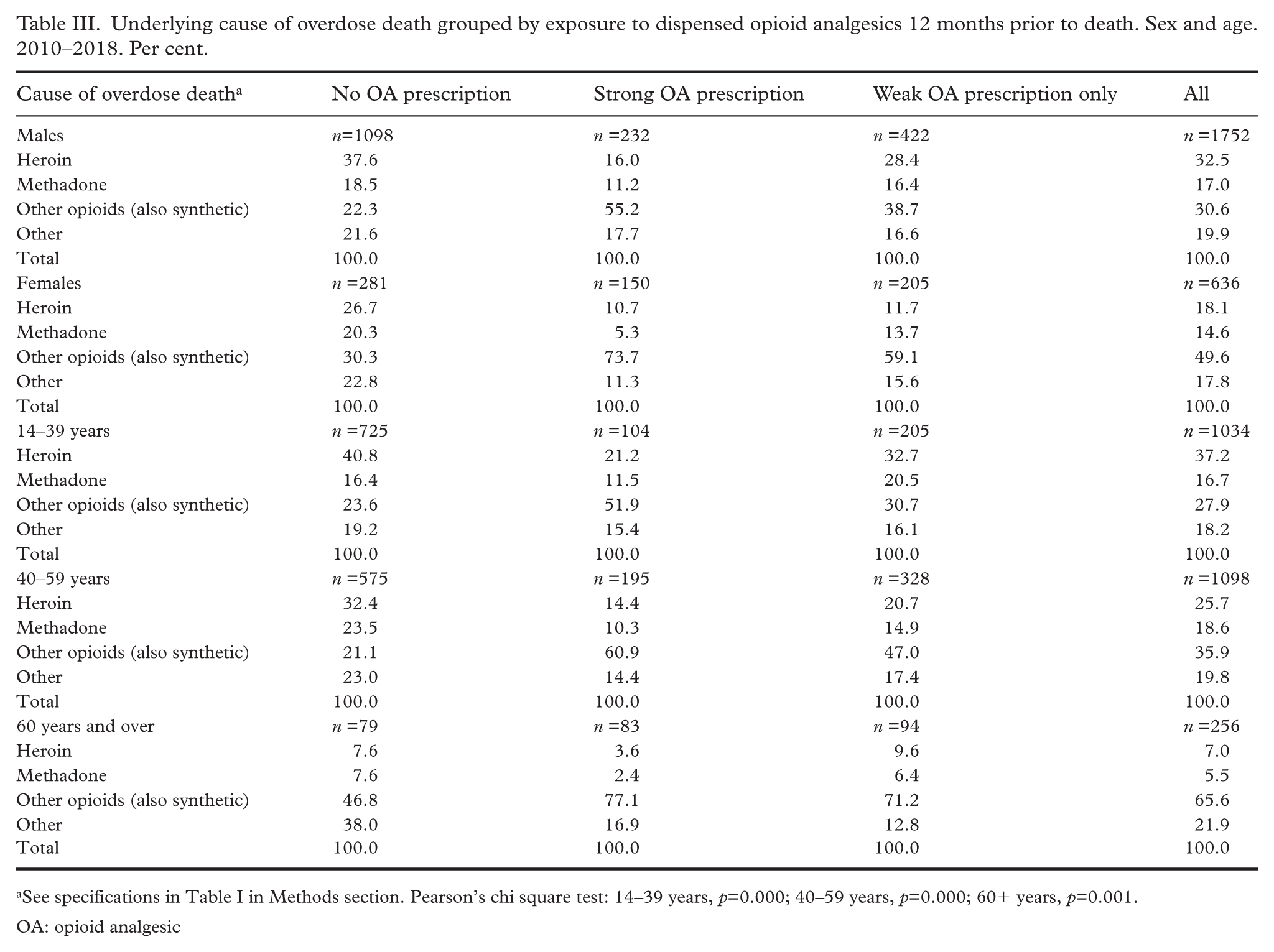
See specifications in Table I in Methods section. Pearson’s chi square test: 14–39 years, p=0.000; 40–59 years, p=0.000; 60+ years, p=0.001.
OA: opioid analgesic
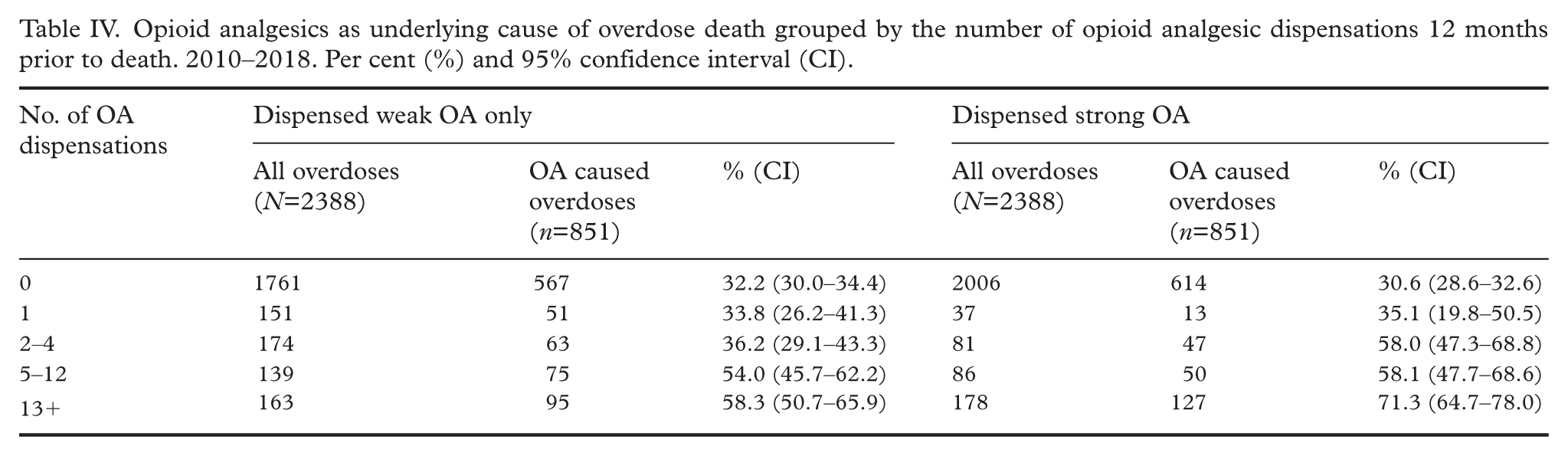
The proportion of overdose deaths with an opioid analgesic-related cause also increased with the number of opioid analgesic dispensations: individuals with more dispensations had a higher likelihood of an opioid analgesic-related cause of death (see Table IV). However, the wide CIs indicate that some between-group differences were not statistically significant.
Opioid analgesics as underlying cause of overdose death grouped by the number of opioid analgesic dispensations 12 months prior to death. 2010–2018. Per cent (%) and 95% confidence interval (CI).
Among individuals exposed to dispensed opioid analgesics, the distribution of opioid analgesic-related overdose deaths by sex and age differed slightly from that observed for all overdose deaths (Table V). Among those exposed to weak opioids, there was no difference in death rates between men and women 60 years and over, with both sexes showing the lowest death rate in this age group. For strong opioid analgesics, opioid analgesic-related overdose death rates were higher for males than females in all three age groups.
Estimated person-years for individuals dispensed OAs, overdose deaths among individuals dispensed OAs with OAs as cause of overdose death. Average 2010–2018. Death rate of OAs per 100,000 person-years dispensed OAs across age and gender (95% confidence interval).
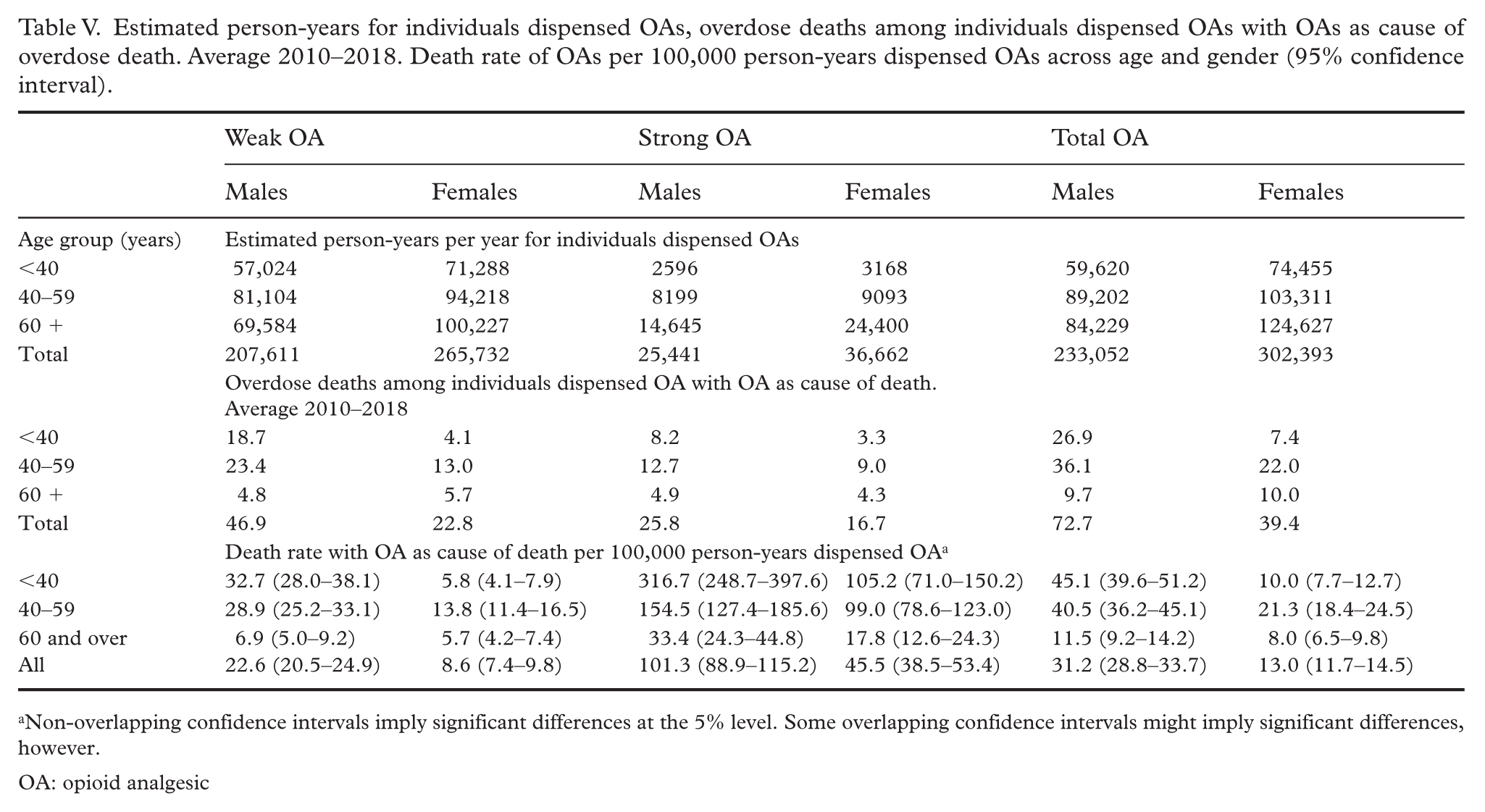
Non-overlapping confidence intervals imply significant differences at the 5% level. Some overlapping confidence intervals might imply significant differences, however.
OA: opioid analgesic
Discussion
Less than half of individuals who died from overdose death had been dispensed opioid analgesic in the 12 months preceding death. The overall risk of overdose death following opioid analgesic exposure was low, remained stable from 2010 to 2018, was higher for men than women and decreased with age. However, overdose death rates among men aged 20–49 and women aged 20–39 exposed to dispensed strong opioid analgesic exceeded the general population death rate. The proportion with opioid analgesic attributed to overdose death was lowest among individuals without recent 12 months opioid analgesic exposure, higher for those dispensed weak opioid analgesics only and highest for those dispensed strong opioid analgesics.
Our finding of 21 overdose deaths per 100,000 person-years among individuals dispensed opioid analgesics aligns with a previous Norwegian study of analgesics users (opioids or non-opioids) reimbursed for chronic, non-cancer-related pain between 2010 and 2019 [8]. In contrast, a meta-analysis of US data reported a rate of 1.1 per 1000 [7]. This large discrepancy likely reflects study population differences and the far greater scale of the US opioid epidemic [2]. There are several studies of overdose deaths per capita, which cannot be adjusted to death rates among persons exposed to opioids [9].
The elevated risk of overdose death among men aged 20–49 years and women aged 20–39 years exposed to dispensed strong opioid analgesic compared with population death risk is consistent with findings from the Norwegian GBD study and meta-analysis [7,11]. Clinicians should carefully balance the benefits and risks of prescribing strong opioid analgesics in these groups, without withholding needed pain treatment [19].
The stability in overdose risk despite increasing strong opioid analgesic dispensing suggests that greater prescribing did not translate into a higher fatality rate. This might relate to declining morphine milligram equivalents per user for several strong opioid analgesics dispensed from 2010 to 2018 [20].
Even though this study cannot reveal whether a dispensed opioid analgesic was the direct cause of an opioid analgesic-related overdose death, a likely contribution from dispensed opioid analgesics is suggested – lowest among those unexposed to opioid analgesic and highest among those exposed to strong opioid analgesic.
Opioid analgesic-related overdose deaths may be caused by either dispensed or illegally obtained opioids. Estimating separate death rates for these sources requires knowledge of the populations at risk as well as the corresponding classification of cause of death. Although some studies have examined overdose deaths attributed to prescribed versus illegally obtained opioid analgesics [9,21], none have had access to risk populations. Consequently, separate overdose death rates for dispensed and illicit opioid analgesics could not be calculated.
In our study, the risk population for dispensed opioid analgesics is known; however, the opioid analgesic-related cause of death includes deaths caused by both dispensed and illegally obtained opioids. In a Norwegian study covering overdose deaths from 2005 to 2021, 60% of individuals with detected codeine, oxycodone or tramadol at autopsy had been dispensed these medications; the corresponding figure was 29% for buprenorphine, methadone and fentanyl [21]. This indicates the size of proportion of illegally obtained opioid analgesic also in the present dataset, and that the estimated overdose death rates of dispensed opioid analgesic might be too high.
Earlier Norwegian studies of opioid analgesic-related overdose deaths have found higher proportions of women than men, and higher proportions of older adults than younger individuals, among those who died [12,22]. These findings supported prevention efforts aimed at older women. In contrast, our study examined the risk of overdose death among individuals exposed to opioid analgesics and found higher death rates among those younger than 50 years, particularly men. This suggests that prevention efforts should also target these groups. Thus, incorporating the population at risk when calculating overdose death rates can lead to different conclusions about which groups should be prioritized for prevention compared with studies that examine the characteristics of only those who died.
Numerous factors – including age, sex, urban/rural setting, substance use disorders, psychiatric disorders, race, type of opioid, dose, potency, polysubstance use, frequent emergency department utilizations, doctor shopping, legally versus illegally produced opioids (fentanyl) – are known risk markers for fatal drug overdose after exposure to opioids [10]. As this study focused primarily on age, sex and strength of opioid analgesic dispensed, unmeasured confounders such as substance misuse might partly explain the observed patterns.
Type, dose and potency of opioids are established risk markers for overdose death [10]. In this study, in addition to distinguishing between weak and strong opioid analgesic, Table IV presents the proportion of overdose deaths attributed to opioid analgesics across the number of opioid analgesic dispensations in the 12 months before death. The high proportion of opioid analgesic-related deaths among individuals with multiple dispensations suggests a higher risk of opioid analgesic-related overdose in this group. Ideally, this relationship would be quantified as overdose death rates across categories of dispensing frequency. However, data on the number of opioid dispensations among all opioid analgesic-exposed individuals were not available, and such rates could therefore not be calculated.
The number of dispensations alone may not adequately reflect ‘type, dose and potency’. For instance, some patients receive large quantities per prescription, while others receive smaller amounts more frequently, depending on clinical assessment. More detailed measures of dispensed dose and potency might therefore provide a clearer understanding of overdose risk.
Several limitations should be noted. First, the exposure window for all dispensed opioid analgesics per year did not perfectly align with dispensations within 12 months prior to overdose death. This discrepancy has minimal impact on results for weak opioid analgesics owing to the stable number of dispensations over time. For strong opioid analgesics, with increasing dispensations over time alongside a stable number of deaths, a certain overestimation of death risk may be expected. Second, sex and age specific denominators were estimated from 2013, making such analysis exploratory. Third, the NCDR data could not distinguish deaths due to legally dispensed versus illicitly obtained opioid analgesics. Fourth, lack of inclusion of methadone (ATC group N07BC) as a painkiller will have a minor effect on the estimates. Total dispensing of methadone is small compared with opioid analgesics and dispensing in tablet form for treating chronic pain constitutes a very low proportion of the total volume of methadone dispensations.
Prevention measures should prioritize adults under 50 years who are prescribed strong opioids, because of their elevated risk of overdose death. Women and older adults, who constitute a large proportion of opioid analgesic recipients, should also be considered for intervention when evidence-based measures are available, despite their lower individual risk. Identifying those at highest risk remains challenging given the overall low risk of overdose death, highlighting the need for population level public health measure strategies. Physicians in Norway are already required to carefully evaluate the indication, benefits and risks when prescribing opioid analgesics, with risk of overdose death being a critical consideration [23,24].
Conclusion
The risk of overdose death following exposure to strong opioid analgesics was low but higher than the population death rate for men under 50 and women under 40 years. Preventive strategies based on risk markers such as sex, age and opioid analgesic strength, combined with other known risk markers, can help guide safer prescription of opioid analgesics and reduce overdose death.
Footnotes
Acknowledgements
We acknowledge a significant contribution by Linn Gjersing at Lovisenberg Diaconal University College/Norwegian Institute of Public Health, providing access to data from her project and for critically reviewing the initial drafts of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data for the project ‘Drug-Induced Deaths 2003–2018’ used by EJA in this manuscript were funded by the Norwegian Directorate of Health. SS and IO were partially funded by the Research Council of Norway, project number 320360.
Access to data
Extraction of data for the project ‘Drug-Induced Deaths 2003–2018’ was based on the Personal Protection Regulation (GDPR) Article 6 No. 1 e and Article 9 No. 2 j with a national supplementary legal basis. The project consisted of medical and healthcare research and had prior approval from Regional Committees for Medical Research Ethics South East Norway (REK South East), with reference to sections 10 and 35 of the Norwegian Health Research Act. The data cannot legally be released to researchers not approved in the project. The Norwegian Institute of Public Health (NIPH) permits aggregated data from the NorPD website (![]() ) to be stored electronically, printed, reproduced and further processed as long as the source «Norwegian Prescription Database, The Norwegian Institute of Public Health (NIPH)» is cited on every report, table or figure.
) to be stored electronically, printed, reproduced and further processed as long as the source «Norwegian Prescription Database, The Norwegian Institute of Public Health (NIPH)» is cited on every report, table or figure.