
Abstract
Aims:
Mental health literacy (MHL) is increasingly recognised as a key component of public mental health promotion. While widely cited definitions focus on recognising and managing mental disorders, recent perspectives call for broader, more holistic frameworks that also address positive mental health. However, conceptual and measurement inconsistencies persist, highlighting the need for a clearer understanding of how MHL is defined and applied across disciplines.
Methods:
This umbrella review synthesised 40 systematic and scoping reviews (2000–2024) to explore how MHL is conceptualised and operationalised across disciplines. Following a registered PROSPERO protocol, the review applied rigorous methods across five databases and assessed quality using the JBI Checklist.
Results:
Most studies relied on a common definition by Jorm and colleagues, focusing on knowledge and beliefs about mental disorders. More recent frameworks, such as that proposed by Kutcher and colleagues, adopt a broader, salutogenic view, emphasising positive mental health, stigma reduction and help-seeking efficacy. Thirty-three MHL measures were identified, with most tools prioritising disorder-related literacy over wellbeing-focused components. The most common way the reviews operationalised MHL was by exploring it as an outcome variable in intervention studies.
Conclusions:
Keywords
Background
Mental health literacy (MHL) has emerged as a ‘hot topic’ in contemporary mental health research in recent years [1]. Although interest in MHL is high, the concept still lacks a universally agreed-upon definition, underlining the need for continued inspection [2]. A popular definition by Jorm and colleagues (1997) formulates MHL as ‘knowledge and beliefs about mental disorders which aid their recognition, management, or prevention’ [3]. Prevailing MHL conceptualisations and measures therefore tend to focus on recognising symptoms of different mental disorders, assessing help-seeking behaviour, and mental health related stigma [3]. Similarly, MHL programmes often prioritise pathogenic aspects of mental health, that is, those concerned with illness, over salutogenic ones [4], which focus on factors that promote and sustain wellbeing [5].
MHL has emerged as a valuable focus of research and intervention. Previous research links higher levels of MHL to positive health behaviours [6], for example, predicting more supportive attitudes towards mental health difficulties, and help-seeking behaviours [7]. Despite these encouraging findings and the demonstrated value of this approach, scholars [8] have pointed out the importance of adopting a broader perspective to MHL, one which also incorporates positive components of mental health [9]. A more nuanced understanding of MHL also acknowledges factors that enable individuals to thrive and function optimally, echoing the 1948 assertion of the World Health Organization (WHO) that ‘health is not merely the absence of disease or infirmity, but a state of complete wellbeing’ [10]. This approach aligns with the Dual Continuum Model, which conceptualises mental health and mental illness not as opposite ends of a single spectrum, but as two distinct yet interconnected dimensions [11]. It emphasises that even in the presence of mental illness, individuals can (and should have opportunities to) promote the positive continuum of mental health [11]. Therefore, definitions of MHL should arguably encompass knowledge of both continuums, necessitating both broader conceptualisations and more comprehensive approaches to measurement. Spiker and Hammer support this view, and stress the need for improved definitions of MHL, as well as developing clarity and a shared language around the concept [2].
The growing interest in MHL is a promising trend that aligns well with contemporary public health approaches to mental health promotion, aiming to foster opportunities for positive mental health across all population groups [12]. Mental health promotion is built on the premise that broader determinants such as education, employment, housing and social inclusion as well as the day-to-day environments in which people live are key influencers on population mental health [13,14]. From a public health perspective, MHL is therefore not only an individual asset but also a population-level determinant that can influence mental health outcomes across communities.
Actions that promote mental health are inherently multifaceted and can be implemented at individual, community and societal levels [15]. Comprehensive approaches to MHL may serve as a valuable complement to mental health promotion strategies [16]. Such comprehensive approaches are particularly important as many initiatives that claim to promote mental health in practice focus primarily on reducing symptoms of depression and anxiety, rather than actively fostering positive mental health and wellbeing [17]. Although actions might overlap at times, conceptual clarity is a crucial step when distinguishing between prevention and promotion, true also for MHL [12]. A broader line to mental health promotion is also reflected in the Mental Health in All Policies approach, which integrates mental health considerations across all sectors to create more inclusive, mentally healthy environments [18].
Diverse approaches necessitate appropriately aligned methodologies for effective evaluation and assessment. Assessing how individuals understand mental health (i.e. MHL) can provide valuable insights to inform and potentially justify mental health promotion efforts. This approach is grounded in the premise that mental health awareness is a necessary foundation for effective promotion, an idea supported by previous research, which identifies awareness as a critical enabler of mental health initiatives across diverse sectors of society [19,20].
Aims
Despite this growing recognition of MHL, universal agreement around its definition remains elusive. The growing interest in MHL underscores its significance, evidenced by the increasing volume of academic literature dedicated to the topic. Like any novel topic, it takes time to place all the pieces of the puzzle. Umbrella reviews, as a high-level synthesis method, aggregate findings from multiple systematic reviews and meta-analyses, making them particularly valuable for evaluating emerging topics [21]. They are well-suited for synthesising complex or interdisciplinary evidence, identifying research gaps or inconsistencies [22] and assessing the quality and consistency of existing reviews which are critical steps in exploring new or evolving areas of study [23].
The current umbrella review aims to contribute to the growing body of literature on MHL by offering a high-level synthesis that enhances both conceptual and operational clarity, thereby supporting the development of more coherent definitions and robust measurement approaches. The research question guiding this umbrella review explores how MHL has been conceptualised and operationalised in academically oriented review articles over the past 25 years. This approach seeks to advance understanding in two key areas: (1) by synthesising how MHL has been conceptualised in recent reviews, it identifies common definitions and theoretical frameworks that underpin the literature; and (2) by summarising how MHL has been operationalised – through measurement, implementation, or application – it examines the tools, scales and indicators used to quantify MHL. Examining how other scholars have distilled findings around MHL can yield important insights into key areas of interest and avenues for further development. Such analysis may also enhance conceptual clarity by identifying the primary contexts in which MHL is studied, mapping commonly used assessment measures and revealing potential gaps or opportunities for further development.
Methods
The review followed the guidelines outlined in the PROSPERO protocol CRD42024585946 [24].
Search strategy
Systematic searches were conducted in the following databases: CINAHL, MEDLINE, Life Sciences Databases, Ovid, PsycInfo. The search covered English language literature published between January 2000 and October 2024. The search strategy comprised three levels: a) the conceptualisation of MHL, b) measures and measurement, implementation, or utilisation of MHL, c) reviews (see Supplemental material Table I online for example of search strategy). Furthermore, the reference lists of the included systematic reviews were hand-searched for backward and forward citation chains to identify additional reviews. Resulting articles were imported into the Rayyan QCRI software to facilitate the study selection process [25].
Inclusion and exclusion criteria
The search strategy was designed to be broad enough to allow for an extensive approach while still remaining true to the research questions. Key distinctions of the three different levels are as shown in Table I.
Inclusion criteria and reasoning.
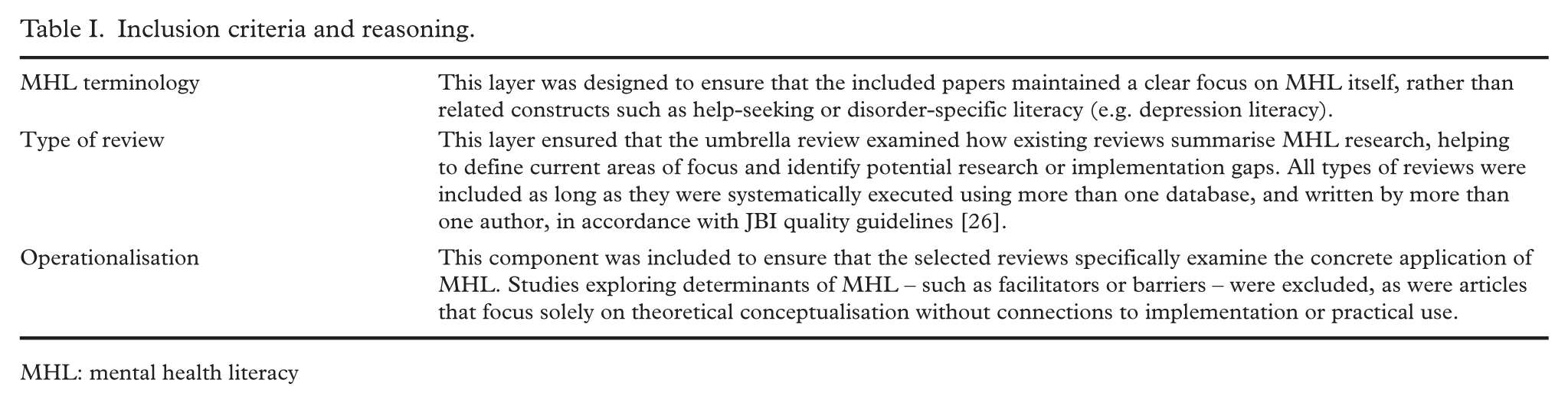
MHL: mental health literacy
Data extraction and quality assessment
All reviews were independently assessed in pairs, with each pair comprising a combination of the reviewing authors (MH, RG, PS, DS, KL, SV, JCS, HS, CM). In the initial screening phase, each article was evaluated at the title and abstract level. Articles selected for full-text assessment were reviewed in the same manner. Any discrepancies between reviewers were resolved through discussion until consensus was reached, with a third author available to facilitate resolution when necessary.
Data extraction was performed by several authors (AS, CM, DS, HS, JCS, KL, MH, MH, RB, RG, SOL, ÖA) and results collated into a data extraction document, including details such as author information, year of publication, research area or discipline, review type, number of studies included, MHL definition used, mental health definition (if included), summary of research question and results, measurement tools and their description.
Quality assessment of included systematic reviews was conducted in accordance with the JBI Checklist for Systematic Reviews and Research Synthesis [26]. Several authors (AS, AS, CM, DS, HS, JCS, KL, MH, ÖA, RB, RG, SOL) completed the quality assessment in blinded pairs, documenting rationales for their assessments. Disparities were resolved through discussion, with a third author available if needed.
Data synthesis
The findings from the included reviews were synthesised into summary tables and a narrative overview, providing a consolidated account of how MHL has been conceptualised and operationalised over the past 25 years.
Results
Following the initial database searches and removal of duplicates, 686 articles were screened at the title and abstract level. Of these, 69 articles were selected for full-text review. After applying the predefined inclusion and exclusion criteria, 37 articles were retained. An additional three articles were identified through forward and backward citation chaining, bringing the total number of included studies to 40. For a detailed overview of the selection process, refer to the PRISMA flow diagram in Figure 1 [27].
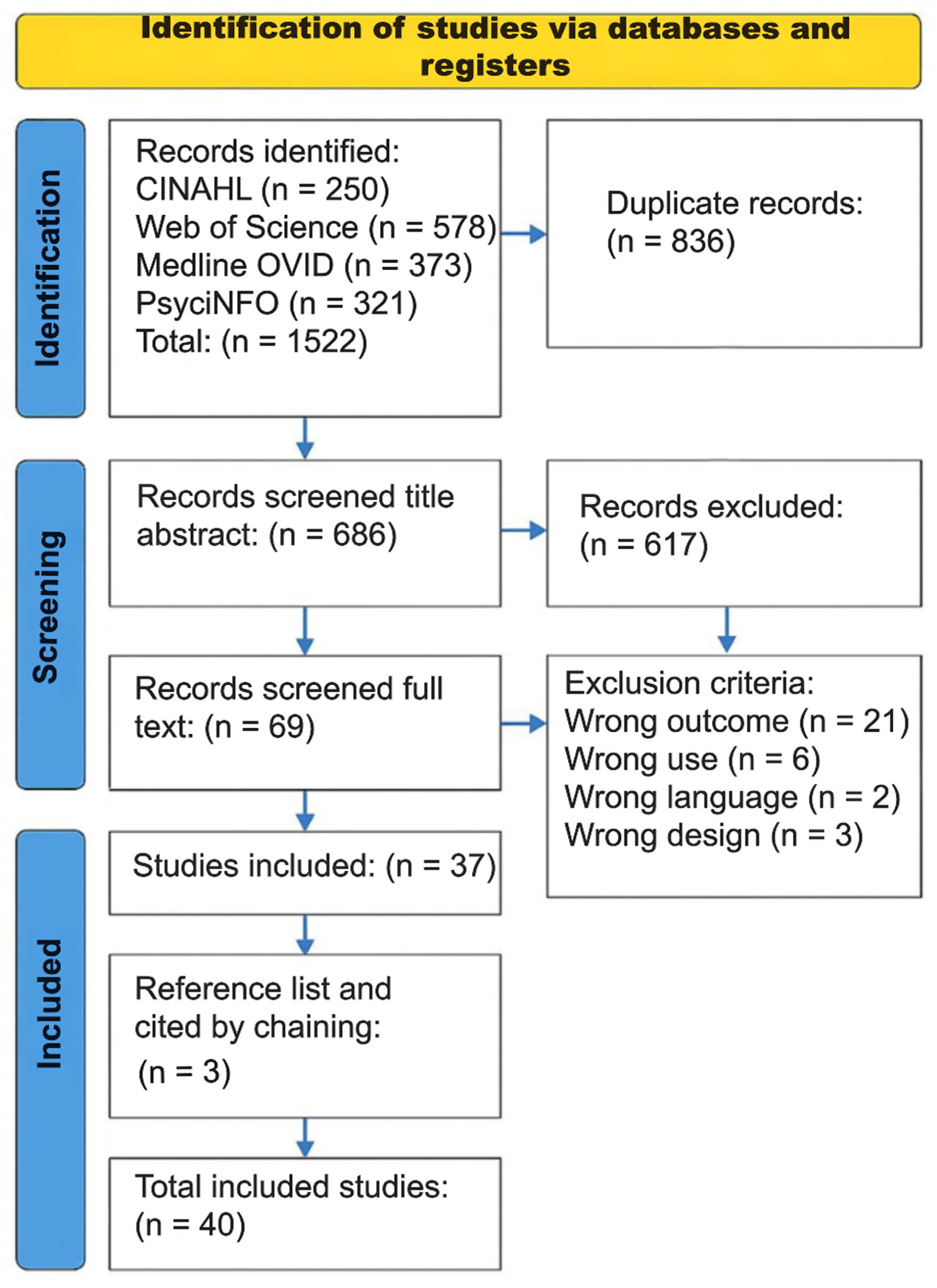
PRISMA flow diagram of selection process [27].
Characteristics of included reviews
The inclusion criteria included all types of review articles, with the most common review type being systematic review (n = 25), followed by scoping review (n = 6), systematic review with meta-analysis (n = 8) and systematic mapping review (n = 1). The included reviews derived from several research areas (according to affiliation of first author) including education (n = 9), psychology (n = 8), public health (n = 6), sports and exercise sciences (n = 3), policy development (n = 1), medicine and health sciences (n = 6), mental health (n = 3), social sciences and arts (n = 4). The reviews included a range of populations, the most common being children, adolescents, young people and students (n = 20). Half of the reviews stem from high income countries, with the majority stemming from Australia (n = 7) and the UK (n = 6), followed by China (n = 5) and the USA (n = 3).
MHL definitions
Although there was some heterogeneity in definitions, there was a clear preference; see Supplemental Table III for detailed definitions. Across the reviewed literature, the most frequently cited definition of MHL was that of Jorm et al. (1997) [3]: ‘Knowledge and beliefs about mental disorders which aid their recognition, management or prevention’, which appeared in at least 35 reviews, often with minor elaborations. Also, later work by Jorm (2000) [28], (2012) [29] and (2015) [30] was popular. These iterations expanded the original definition into six key components: (1) the ability to identify specific disorders, (2) knowledge of how to obtain mental health information, (3) knowledge of risk factors and causes, (4) knowledge of self-care methods, (5) knowledge of available professional assistance, (6) attitudes that encourage recognition and appropriate help-seeking [30]. Another prevalent definition was that by Kutcher et al. (2016) [16], describing MHL as: ‘understanding how to obtain and maintain positive mental health; understanding mental disorders and their treatments; decreasing stigma related to mental disorders; and, enhancing help-seeking efficacy (knowing when and where to seek help and developing competencies designed to improve one’s mental health care and self-management capabilities’, which was referenced in at least 15 reviews. This definition broadens the concept of MHL to include components such as stigma reduction, help-seeking efficacy, and positive mental health. Other definitions of MHL were developed by scholars from China, notably Wei et al. (2013, 2015), who emphasised domains such as mental health knowledge, attitudes (including stigma), confidence in helping, intention to help, and actual helping behaviour [8,31], cited in at least four reviews. Similarly, Chao et al. (2020) emphasised domains such as mental health knowledge, attitudes including stigma, and help-seeking efficacy; their definition was cited on two occasions [32]. Further similar yet less frequently cited definitions of MHL include that proposed by Hao et al. (2020) [33] and Jiang et al. (2021) applying a multidimensional construct including knowledge, attitudes and behaviours [34]. A unique definition by Bale et al. (2020) was cited once, denoting a child-focused model with five domains: recognising changes, help-seeking, influences, coping, attitudes [35], as was a definition by the WHO (2013) which emphasised three interconnected concepts: knowledge, attitude, help-seeking efficacy [36]. Overall, the literature demonstrates both consistency in referencing foundational definitions, and an increasing trend toward multidimensional and context-specific conceptualisations of MHL.
Different MHL measures
A total of 33 distinct MHL measures were identified across the reviewed studies (see Table II), bearing in mind that not all reviews mentioned specific measures. The most frequently utilised instrument was the Mental Health Literacy Scale (MHLS), developed by O’Connor and Casey (2015) [37], appearing in 15 reviews. This was followed by the Mental Health Knowledge Schedule by Evans-Lacko et al. (2010) [38], cited in nine reviews, the Mental Health Literacy Questionnaire by Campos et al. (2016) [39], which appeared in six reviews, while the Positive Mental Health Literacy Scale (MHPK-10) by Bjornsen et al. (2017) [40] was mentioned in three reviews. These measures have certain similarities, but focus on different dimensions of MHL; see Table II.
Description of most commonly included mental health literacy measures.
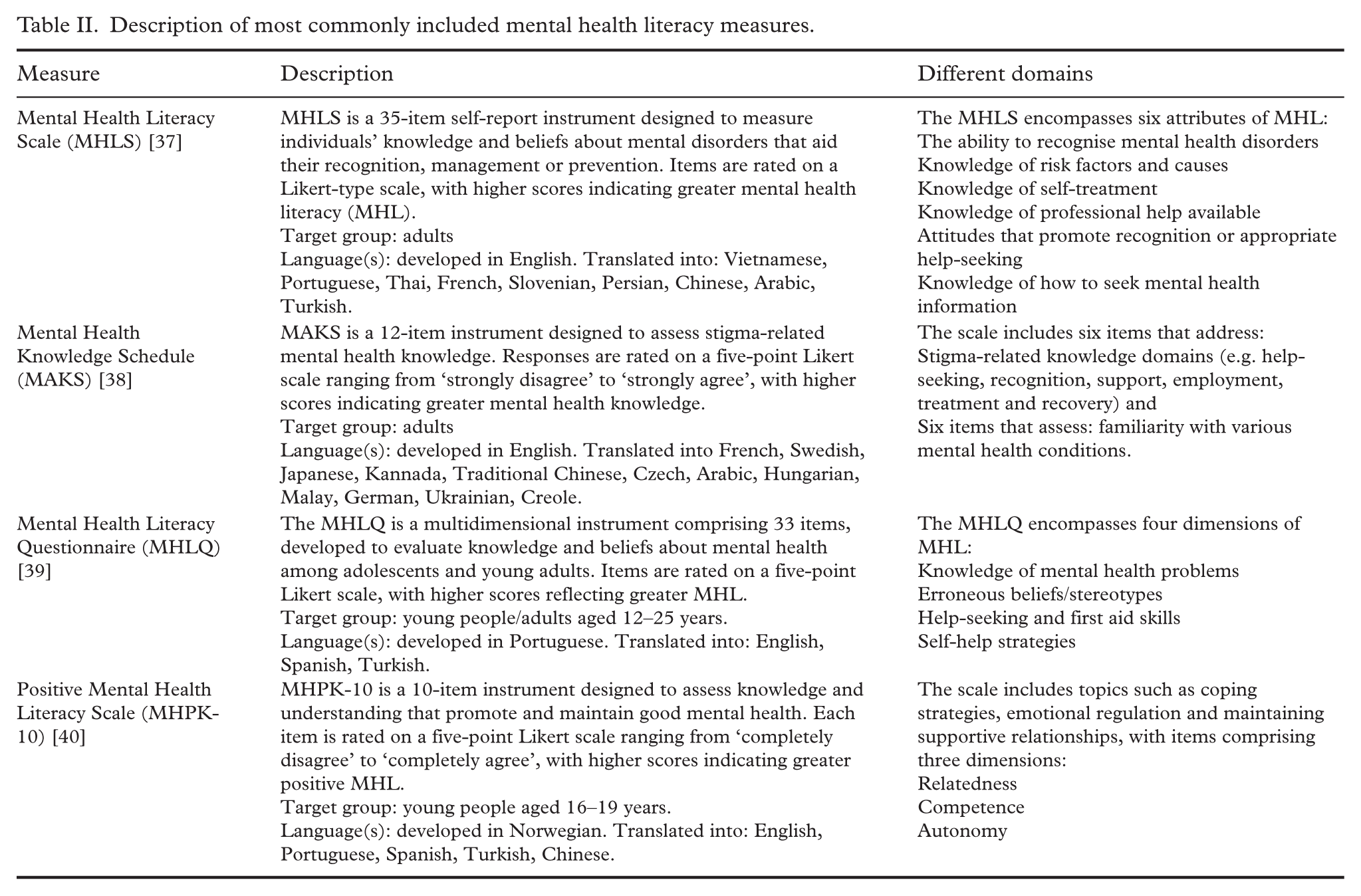
All measures except for the MHPK-10 [40] included domains relating to identifying and understanding different mental health disorders, as well as awareness of when and how to seek help, and attitudes that support doing so, and knowledge of self-treatment, emotional regulation and personal coping methods. In contrast, the MHPK-10 [40] focuses on maintaining mental wellbeing, emotional health and supportive relationships. Domains such as knowledge of mental disorders, stigma-related attitudes, help-seeking behaviours and self-help strategies were generally more commonly represented in the measures than positive mental health domains, including coping, emotional regulation and supportive relationships.
How MHL was operationalised
Although the reviews encompassed a range of study designs, the operationalisation of MHL could be categorised into distinct types (see Supplemental Table IV). The majority of reviews (n = 30) operationalised MHL as an outcome variable, for example, in relation to intervention studies. The interventions varied in format, including individual, group-based and web-based approaches, and typically aimed to enhance mental health awareness, promote help-seeking behaviours and reduce stigma. The second most common way of operationalising MHL was through its assessment within a specific population at a single point in time (n = 8), followed by those that evaluated the methodological or psychometric properties of MHL measurement instruments (n = 7). A smaller number of reviews examined MHL in relation to other outcomes (n = 2) with one review focusing on evaluating MHL interventions and their content and contexts (n = 1).
Research questions of included reviews
Research questions (see Supplemental Table IV) in the included reviews focused predominantly on effectiveness of MHL interventions, for example, in school environments [41–44], among athletes and sports communities [45–47], for healthcare professionals [48,49] and in digital formats [50–53]. Another popular research focus was that of measuring MHL in specific populations, such as across cultural and national contexts [54 –61], among youth and adolescents [62–69], parents and caregivers [70–73], in teachers and school staff [74, 75] or workers in predominantly male industries [76].
Furthermore, research questions centred around topics such as exploring psychometric properties of MHL measures [77–79], conceptual development over time [5,78] or across language and population validity [55,57–61].
Summary of concluding remarks or results from reviews
The concluding remarks and recommendations for further study listed in the reviews revealed several key priorities for advancing MHL study and its application (see Supplemental Table IV). A number of reviews emphasised the need for further conceptual clarity and more precise definitions of MHL and its constituent components, such as positive continuums of MHL. The development of unified conceptual frameworks and continuum-based models was highlighted as a critical opportunity to strengthen theoretical foundations.
Additionally, there was a strong emphasis on the need for methodological rigour and standardisation of MHL operationalisation, including the adoption of robust, theory-informed research designs and the use of standardised outcome measures. Many reviews also called for validated, psychometrically sound instruments to be developed and applied which are capable of comprehensively assessing all dimensions of MHL. Furthermore, ensuring that MHL interventions are accessible and relevant to diverse populations was identified as essential for promoting equity and effectiveness in mental health promotion. This involves addressing language barriers, cultural beliefs and the varying age groups and life circumstances.
Quality of evidence
According to the JBI Checklist for Systematic Reviews and Research Synthesis [26], out of the 40 reviews, eight received the maximum score of 11 ‘Yes’ responses. Affirmative answers indicate a high methodological quality, with regard to clarity of the research question, appropriateness of inclusion criteria, rigor in data collection and analysis (see Supplemental Table II). Although the JBI Checklist does not explicitly define thresholds for medium or low quality based on affirmative responses, it is noteworthy that 36 out of the 40 included reviews received nine or more ‘Yes’ answers. This suggests that the majority of the reviews were of high methodological quality.
Discussion
This umbrella review examined how MHL has been conceptualised and operationalised in the academic literature over the past 25 years. By synthesising definitions, frameworks and applications, the analysis offers insights that clarify key contexts, common measures and areas for future development. MHL has emerged as a growing area of interest, as demonstrated by the significant increase in review articles published over the past 25 years. This trend was evident in our review, which identified 686 articles, with 40 reviews meeting the inclusion criteria – all published within a very recent timeframe. This finding is further corroborated by a recent bibliometric mapping study, which documented an approximately sixfold rise in the number of MHL-related publications between 2005 and 2019, spanning various publication types [80]. The authors also reported the majority of publications to originate from high-income countries, with the most frequently used keywords being ‘stigma’ and ‘depression’, reflecting an illness-oriented perspective [80].
Considering that the definition of MHL significantly shapes its practical application, our first step was to examine how MHL was conceptualised in the literature. Jorm and colleagues were pioneers in the field of MHL, their influence also demonstrated here by most of the included reviews citing one or more of Jorm and colleagues’ definitions of MHL [3,29-30]. The work of Jorm et al. highlighted gaps in public understanding, such as difficulties in recognising mental disorders, misconceptions about their causes and treatments, barriers to seeking help, including attention to mental health related stigma [3]. Their research emphasised the need for community-wide interventions, including educational programmes, Mental Health First Aid training and awareness campaigns to improve MHL [29]. Jorm and colleagues’ work represents a pivotal contribution to public mental health, laying a vital foundation for the development of MHL.
Another popular definition of MHL reported in the current review is that of Kutcher and colleagues, who expanded on the work of Jorm et al. and developed the definition of MHL further by including the phrasing ‘understanding how to obtain and maintain good mental health’ [16]. This definition lines up more closely with current approaches of mental health promotion by including a focus on promoting the positive continuum of mental health [12]. Mansfield et al. [5] criticised the field for its focus on mental ill health, lack of mental health promotion, conceptual confusion and inconsistent measurement. They call for a shift from ‘mental disorder literacy’ to ‘critical mental health literacy’, advocating for a multi-construct approach that distinguishes domains like recognition, knowledge, stigma and help-seeking, and for the development of culturally and developmentally appropriate measures for adolescents [5]. Recent developments in the field reflect a growing emphasis on expanding MHL beyond disorder-focused definitions, toward more comprehensive frameworks that incorporate mental health promotion, contextual sensitivity and multidimensional understanding.
This approach was also reflected in work by Soria-Martínez et al. (2024), who emphasised that MHL should extend beyond mental disorders to include broader mental health concepts [81]. Interestingly, the authors also highlight the importance of accounting for individual and sociocultural contexts in both interventions and measurement tools, in order to reflect the complexity and variability of MHL across diverse populations and settings [81]. This view was reflected in the findings of the current review, with the second most common way of operationalising MHL being its assessment within a specific population at a single point in time. It can therefore be noted that the concept of MHL has evolved from Jorm and colleagues’ foundational focus on disorder recognition and public education approach to a broader, multidimensional understanding that incorporates mental health promotion, cultural and developmental sensitivity, and the complexity of individual and sociocultural contexts. This ongoing evolution highlights the importance of adopting holistic and contextually relevant approaches to MHL in both research and practice.
In a similar vein, a study by Zeng et al. offers further relevant insights into the nature of MHL that warrant consideration, although not included in our results owing to the predefined inclusion criteria [85]. Specifically, Zeng et al. (2024) highlight the multidimensional nature of definition of MHL, identifying three core themes: cognitive understanding, affective empowerment and behavioural change. Cognitive understanding focuses on knowledge and beliefs about mental health, including recognition of disorders, causes and how to seek information. Affective empowerment highlights emotional and relational aspects such as reducing stigma, fostering supportive attitudes and strengthening interpersonal connections. Behaviour change emphasises practical actions such as help-seeking, self-management strategies and promoting mental wellbeing through informed coping and treatment choices. Together, these themes denote MHL as a multidimensional concept integrating knowledge, emotion and action, and advocate for future MHL research to place greater emphasis on behavioural, more action oriented aspects prioritising practical application and implementation in order to enhance ‘. . . MHL’s real world impact and relevance across diverse contexts’ [82]. This approach was echoed in a further bibliometric analysis with the same lead author, emphasising the need for a comprehensive understanding of the interactions between mental health knowledge, behaviours and demographic factors [83].
Building on our initial examination of MHL conceptualisations, we extended our approach to explore how MHL has been operationalised. Since the measurement of MHL is closely tied to operationalisation, the next step was to explore how this concept has been translated into measures. The most common measure of MHL reported in the current study is the MHLS, developed by O’Connor and Casey (2015) [37], which includes the following domains: (1) the ability to recognise disorders, (2) knowledge of risk factors and causes, (3) knowledge of self-treatment, (4) knowledge of professional help available, (5) attitudes that promote recognition or appropriate help-seeking, (6) knowledge of how to seek mental health information. This measure is built upon definitions by Jorm and colleagues [3,28-30], as are most measures reported in Table II, notwithstanding the MHPK-10 [40], which cites Kutcher and colleagues’ definition of MHL [16]. The MHPK-10 [40] is also the only measure that includes items on the positive continuum of mental health, and has no items related to mental health difficulties or disorders. A MHL measure that incorporates the positive continuum of mental health could effectively support initiatives aimed at promoting mental health. The rationale behind this is that, in order to effectively promote mental health, it is crucial to first understand what it entails and how it can be nurtured [6,7]. Comprehensive MHL measures may therefore be necessary to capture this complexity as current conceptualisations of MHL might not adequately support this aim. In their mapping analyses, Zeng et al. [82, 83] also identified an interest in enhancing the field’s empirical foundation, and a growing emphasis on the reliability, reproducibility and validation of MHL measurement tools. Mental health promotion extends beyond psychoeducation focused on specific disorders, encompassing broader elements such as fostering optimism, hope and creativity – dimensions that might not be captured by existing MHL measures [84]. Existing measures focus more on domains relating to knowledge of mental disorders, stigma-related attitudes, help-seeking behaviours and self-help strategies, and less on positive mental health. This imbalance underscores the need for further development work, including new assessment tools which more comprehensively capture the positive aspects of mental health.
Steps in this direction have already been initiated. Carvalho and colleagues [85] employed structural validation techniques to inform a concept analysis, framing positive MHL as a dynamic construct. They conceptualise it simultaneously as: (a) an outcome of mental health promotion efforts – positively associated with physical health, social functioning, problem-solving ability, productivity, self-esteem, learning outcomes, resilience, and motivation; and (b) a resource or mediator of mental health and wellbeing [85]. This dual perspective positions positive MHL as a multifaceted and evolving construct essential for understanding the mechanisms that enhance mental health and support healthy behaviours [85]. Spiker and Hammer highlight the importance of refining the conceptual definition of MHL, proposing that it be framed as a theoretical model to enable rigorous empirical testing [2]. The current review supports this progress by summarising existing reviews on the topic and highlighting areas for development.
The growing interest in MHL might warrant a renewed examination of its conceptualisation and operationalisation, particularly with regard to its theoretical foundations and the consistency of its measurement [2]. The disciplinary breadth of the review authors, spanning public health, education, mental health, social sciences and the arts, reflects the wide-ranging academic engagement with MHL as a multifaceted concept. This interdisciplinary interest aligns with mental health promotion principles, which emphasises the importance of supporting positive mental health across sectors and everyday settings. It also resonates with recent policy developments in various countries that increasingly adopt a wellbeing-centred approach, making the assessment of potential impact ever more critical [86]. The manner in which MHL was operationalised across the included reviews revealed a strong interest in being able to use MHL as an outcome variable, particularly within intervention studies aimed at improving components of MHL such as awareness, help-seeking and stigma reduction. Another key area of interest was assessing MHL within specific populations, offering opportunities for cross-group comparisons and for identifying populations that might benefit from targeted interventions. These findings highlight the importance of advancing conceptual clarity, developing robust and validated instruments, and ensuring culturally relevant approaches to MHL research and practice.
Strengths and limitations
This umbrella review synthesises findings from 40 reviews, offering a broad and high-level overview of how MHL has been conceptualised and operationalised over the past 25 years. The value of conducting an umbrella review lies in its ability to adopt a bird’s-eye-view of existing evidence helping to identify gaps, inconsistencies and areas of debate. Umbrella reviews are increasingly recognised as a robust tool for shaping policy and guiding future research directions [22]. This approach is especially valuable for consolidating findings from multiple, heterogeneous systematic reviews, and optimising research efforts, enhancing generalisability and relevance of the findings across disciplines and populations.
A key methodological strength of this approach is its adherence to a registered PROSPERO protocol and established guidelines for conducting umbrella reviews, ensuring transparency, rigour and reproducibility [21]. Quality assessment was conducted using the JBI Checklist for Systematic Reviews and Research Syntheses, ensuring transparency and methodological robustness [26]. The included reviews span diverse fields such as education, psychology, public health, and medicine, reflecting the interdisciplinary nature of MHL and allowing for a richer understanding of its applications and interpretations. By comparing definitions and measures of MHL, the review highlights the dominance of disorder-focused frameworks and the underrepresentation of positive MHL. This insight is valuable for guiding future research and tool development.
Limitations should be noted regarding the broad inclusion criteria, which were designed to capture a wide range of reviews while maintaining a focus on operational aspects of MHL. Although this approach enabled a comprehensive synthesis, it also led to a larger-than-anticipated number of studies, introducing heterogeneity that might limit the specificity of conclusions. Furthermore, despite the comprehensive search strategy and clearly defined inclusion criteria, there remains a possibility that some relevant articles were inadvertently excluded, particularly in relation to the third level of the search strategy, operationalisation, which required the highest degree of interpretative judgment by the reviewers. Additionally, variations in terminology across studies might have influenced which articles were ultimately included, although every effort was made to ensure a thorough and balanced synthesis. Lastly, the predominance of reviews from high-income countries – particularly Australia, the UK, and the USA – might restrict the generalisability of findings to low- and middle-income settings.
Conclusion
This umbrella review highlights the evolving conceptualisation and operationalisation of MHL across a range of disciplines and contexts. The findings support the development of more holistic MHL frameworks and measures, aligning with contemporary mental health promotion strategies and informing policy initiatives that emphasise positive mental health. While foundational definitions remain influential, there is increasing recognition of the need to incorporate the positive continuum of mental health into both theoretical models and measurement approaches. MHL can be operationalised in various ways; the current review found the greatest interest in using it as an outcome variable and in measuring MHL within specific populations. The review underscores the importance of developing practically oriented, comprehensive and context-sensitive MHL frameworks that can effectively support mental health promotion in everyday settings. Future research should prioritise refining definitions, improving measurement tools and operationalising interventions and other actions which promote mental health to reflect the multifaceted nature of MHL. A clearer understanding of MHL levels on a population level can also inform policy design, helping to raise awareness, reduce barriers and foster more supportive environments for mental health across society.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261422936 – Supplemental material for Conceptualisation and operationalisation of mental health literacy: An umbrella review
Supplemental material, sj-docx-1-sjp-10.1177_14034948261422936 for Conceptualisation and operationalisation of mental health literacy: An umbrella review by Johanna Cresswell-Smith, Hedvig Sultson, Carolina Murd, Merle Havik, Robert Griebler, Denise Schütze, Roberta Bevilacqua, Arianna Sgolastra, Kaia Laidra, Sólrún Ósk Lárusdóttir, Ösp Árnadóttir and Pia Solin in Scandinavian Journal of Public Health
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project (GA – 101128023) is co-funded by the European Union. Views and opinions expressed are however those of the authors only and do not necessarily reflect those of the European Union or European Health and Digital Executive Agency (HaDEA). Neither the European Union nor HaDEA can be held responsible for them. GA: Grant Agreement. For more information about Grant Agreement, please visit this webpage: ![]()
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.