
Abstract
Aim:
To document admissions, outcomes, and survival in somatic hospital patients aged 80 years and older over two decades.
Methods:
We performed a retrospective study of patients aged 80 years and older admitted to a university hospital in Bergen, Norway, in 2002, 2012, and 2022. Patient factors such as age, sex, and complex multimorbidity were considered important for 12-month survival and were used as predictors in a Cox regression model.
Results:
Annual admissions increased by 74%, from 5589 to 10,273, over the two decades, while the proportion of unplanned admissions (77%) remained constant. Median hospital length of stay decreased from 5 to 3 days, with a moderate increase in the 30-day readmission rate from 14.6% to 17.3%. In-hospital mortality declined from 10% to 4.7%, and one-year mortality declined from 25.1% in 2012 to 23.1% in 2022. The risk of death was higher with increasing age (hazard ratio (HR) 1.13, 95% confidence interval (CI) 1.21–1.26), readmission (HR 2.25, 95% CI 1.56–3.23), complex multimorbidity (HR 1.24, 95% CI 1.85–3.56) and male sex; women had a 26% lower risk of dying compared with men (HR 0.74, 95% CI 0.66–0.82). All predictors were significantly associated with all-cause mortality (Cox proportional hazards model with interaction terms, P<0.001).
Conclusions:
Keywords
Introduction
Background and rationale
The number of older inhabitants (⩾65 years) is increasing worldwide, particularly in developed countries. At the same time, the number of people of working age (18–65 years) is expected to shrink. In Norway, the ratio of the working age group to older adults is projected to decrease from 3:1 at present to 2:1 by 2050 [1], which will place substantial pressure on healthcare services. Most developed countries are expected to experience a significant increase in life expectancy in the coming decades [2], and in Norway this is projected to exceed 90 years for both sexes by 2065. The number of older patients (⩾80 years) is projected to increase from 257,000 in 2024 to 530,000 in 2050, more than doubling in just 25 years [3].
Currently, there are few if any suitable and sustainable solutions to this challenge, which will likely affect hospitals in two ways: an increase in admissions of older patients and a reduction in the available workforce.
Hospital admission rates increase with age, at least up to 90 years [4], so it is important to gain more knowledge about admissions and outcomes after hospital discharge in this age group. Such knowledge is vital to support the changes that will be required to meet the future challenges of an ageing population in healthcare.
Most studies on survival or quality of life after hospital admission in older patients focus on specific subgroups, such as those with stroke, sepsis, acute heart failure, COVID-19, or community-acquired pneumonia [5 –9]. These studies typically describe survival and, in some cases, post-discharge outcomes such as mortality and quality of life. Their findings are therefore not directly comparable with those from a heterogeneous population of older inpatients.
In Australia, a nationwide study examined hospital use in people aged 75 years and older [10]. The authors reported an increase in total bed utilisation between 1993–94 and 2019–20, but the bed-days per admission did not increase as hospital length of stay (LOS) declined. For people aged 75 years and older, the median LOS decreased from 12.2 to 7.1 days over that period.
Apart from age, comorbidity and reason for admission, other factors have been identified as important for understanding hospital survival and quality of life in older patients, including frailty, cognition, and functional status with respect to activities of daily living [11 –13].
Objectives
Our primary aim was to describe acute hospital admissions and survival up to one year in older adults (⩾80 years) admitted to a large Norwegian tertiary hospital over two decades. Secondary aims were to document the effects of age, sex, multimorbidity, and readmissions on one-year post-admission survival in this patient group.
Methods
Study design
This was a retrospective study of administrative data from hospital admissions of patients aged 80 years and over. We performed extended analyses on patient data similar to those routinely transferred from the patient record to the Norwegian National Patient Register.
Setting
The study was conducted at Haukeland University Hospital, Bergen, Norway, using data from three calendar years: 2002, 2012, and 2022. The hospital currently has 863 somatic beds and serves as the local hospital for the city of Bergen and surrounding areas, and as a tertiary (regional) hospital for Health Region West, with 1.2 million inhabitants.
During the study period, the number of inhabitants aged 80 years and over in the catchment area (Hordaland County) increased from 19,737 in 2002 to 24,480 in 2022, and the proportion of admissions involving patients aged 80 years and over rose from 19.5% to 25.4% (Table I).
Demographics and overview of the three cohorts.
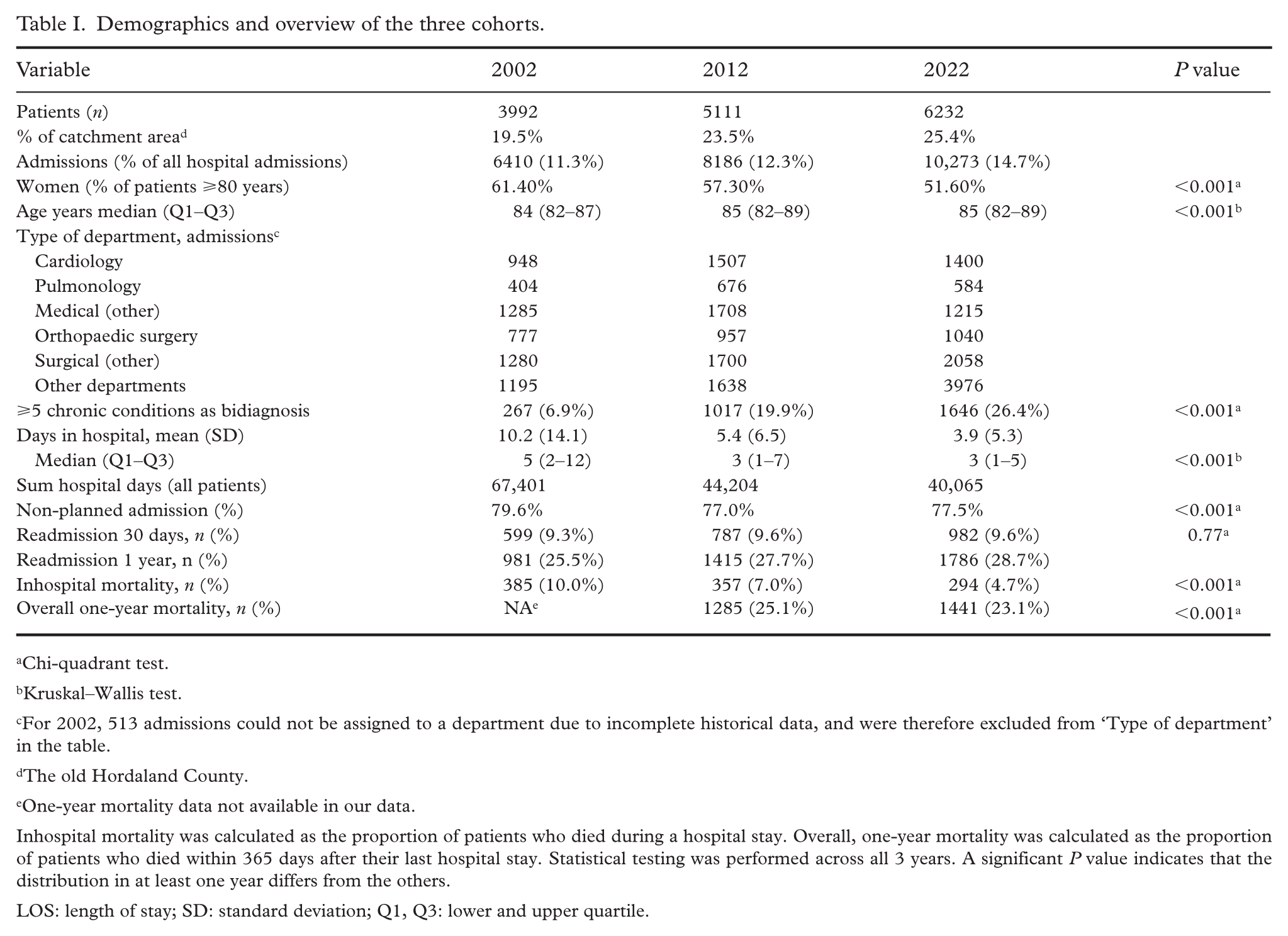
Chi-quadrant test.
Kruskal–Wallis test.
For 2002, 513 admissions could not be assigned to a department due to incomplete historical data, and were therefore excluded from ‘Type of department’ in the table.
The old Hordaland County.
One-year mortality data not available in our data.
Inhospital mortality was calculated as the proportion of patients who died during a hospital stay. Overall, one-year mortality was calculated as the proportion of patients who died within 365 days after their last hospital stay. Statistical testing was performed across all 3 years. A significant P value indicates that the distribution in at least one year differs from the others.
LOS: length of stay; SD: standard deviation; Q1, Q3: lower and upper quartile.
Participants
Routinely registered administrative data were retrieved for all somatic hospital admissions in patients aged 80 years and older.
Variables
We extracted selected data directly from the hospital database with electronic patient records. Age was recorded as age at admission, and the admission department was defined as the department to which the patient was assigned on the day of admission. Discharge status was recorded as dead or alive. Vital status after discharge was continuously updated in the hospital database using data from the Norwegian Population Register.
All-cause survival was assessed for 365 days after the last hospital discharge in each calendar year, and we recorded whether the last hospital stay was a readmission. A readmission was defined as an emergency hospital admission occurring at least one day but less than 30 days after an index stay, which served as the baseline event for analysing readmissions [14]. According to this definition, further readmissions are not counted until a new index stay is established, at least 30 days after the previous one.
Subgroup analyses were performed according to age (80–89 years and ⩾90 years), sex (female/male), complex multimorbidity (low: 0–5 chronic diagnoses; high: >5 chronic diagnoses), and readmission status (yes/no). Multimorbidity was derived from the number of International Classification of Disease, version 10 (ICD-10) diagnoses recorded in the same year as discharge, in a retrospective manner. Because we expected many secondary diagnoses in this patient group, we chose to use the concept of complex multimorbidity and defined this as having at least five chronic secondary diagnoses in addition to the primary diagnosis recorded at the time of hospital discharge, within the same year [15].
Data sources and measurement
Patient characteristics such as age, sex, and total burden of chronic illness were assessed from summarised data in the electronic health record. Population data for the three study years were retrieved from Statistics Norway (https://www.ssb.no/en/forskning).
Statistical methods
The total follow-up time for each patient was defined as the period from the first hospital admission within each calendar year (2002, 2012, or 2022) until death, or until 365 days after discharge from the last hospital stay in that calendar year. For those who did not die within the observation period, data were censored at 365 days. Mortality from any cause was the event of interest.
This event, together with the observation time, was entered into a Cox proportional hazards model using CoxPHFitter from Lifelines, a Python library for survival analysis [16]. We report hazard ratios (HRs) for all-cause mortality with 95% confidence intervals (CIs) for each predictor from the Cox regression analysis. The assumptions of proportional hazards (constant hazard ratios over time) and absence of time-varying covariates were tested using the check assumptions function in Lifelines.
The analysis evaluated the impact of several predictors on all-cause mortality: age, sex, whether the last hospital stay was a readmission, and total burden of chronic illness as measured by multimorbidity. Age was centered around zero to support the use of interaction terms. We incorporated interaction terms between age, readmission, and multimorbidity into the Cox proportional hazards model. The specific interactions were age × readmission, age × multimorbidity, and readmission × multimorbidity. These interactions were included because age, readmission, and multimorbidity may have different effects on all-cause mortality depending on each other’s values. For example, understanding how multimorbidity influences survival in very old patients can help guide optimal treatment strategies during hospitalisation. The Cox analysis was applied only to the 2022 cohort.
The same datasets used in the Cox analysis were applied in Kaplan–Meier survival plots to illustrate survival probabilities across different demographic and clinical strata. These plots were constructed using KaplanMeierFitter from Lifelines, focusing on combinations of age groups (80–89 and ⩾90 years), sex (female/male), and readmission status (yes/no). Figure 1 illustrates the impact of age and multimorbidity; Figure 2 examines the interaction between age and sex; and Figure 3 explores the interaction between age and readmission on all-cause mortality. The Kaplan–Meier plots provide a visual representation of how covariates influence survival over time but should be interpreted alongside the Cox regression results, particularly in the presence of potential confounding variables.
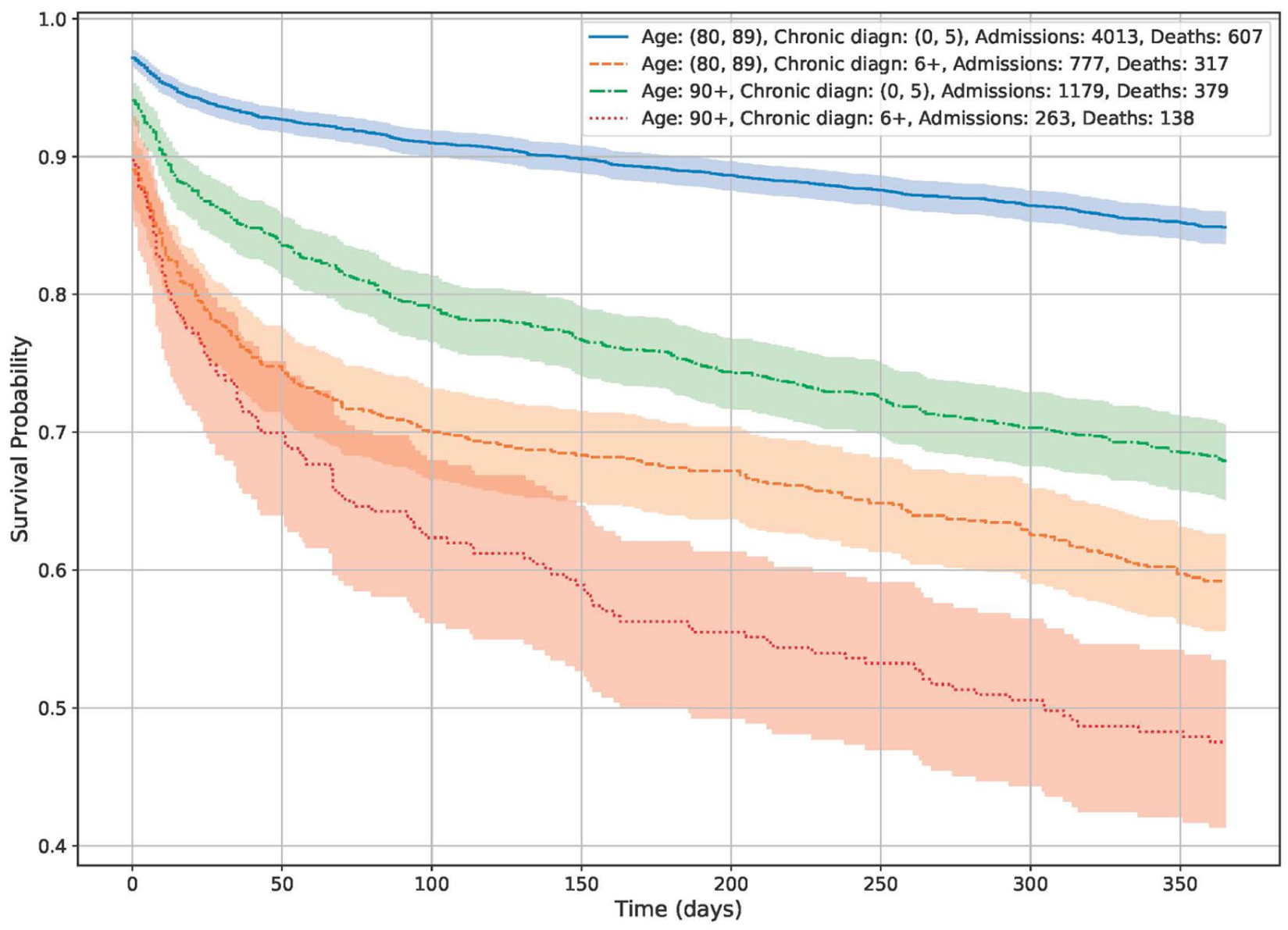
The effect of age divided in two groups (80–89 blue/green) and (90+ red/pink) and multimorbidity (number of chronic diagnosis) (0–5 and >5) on mortality in the first 365 days after the most recent hospital admission. High age and readmissions are associated with higher levels of mortality. The shaded areas are 95% confidence intervals.
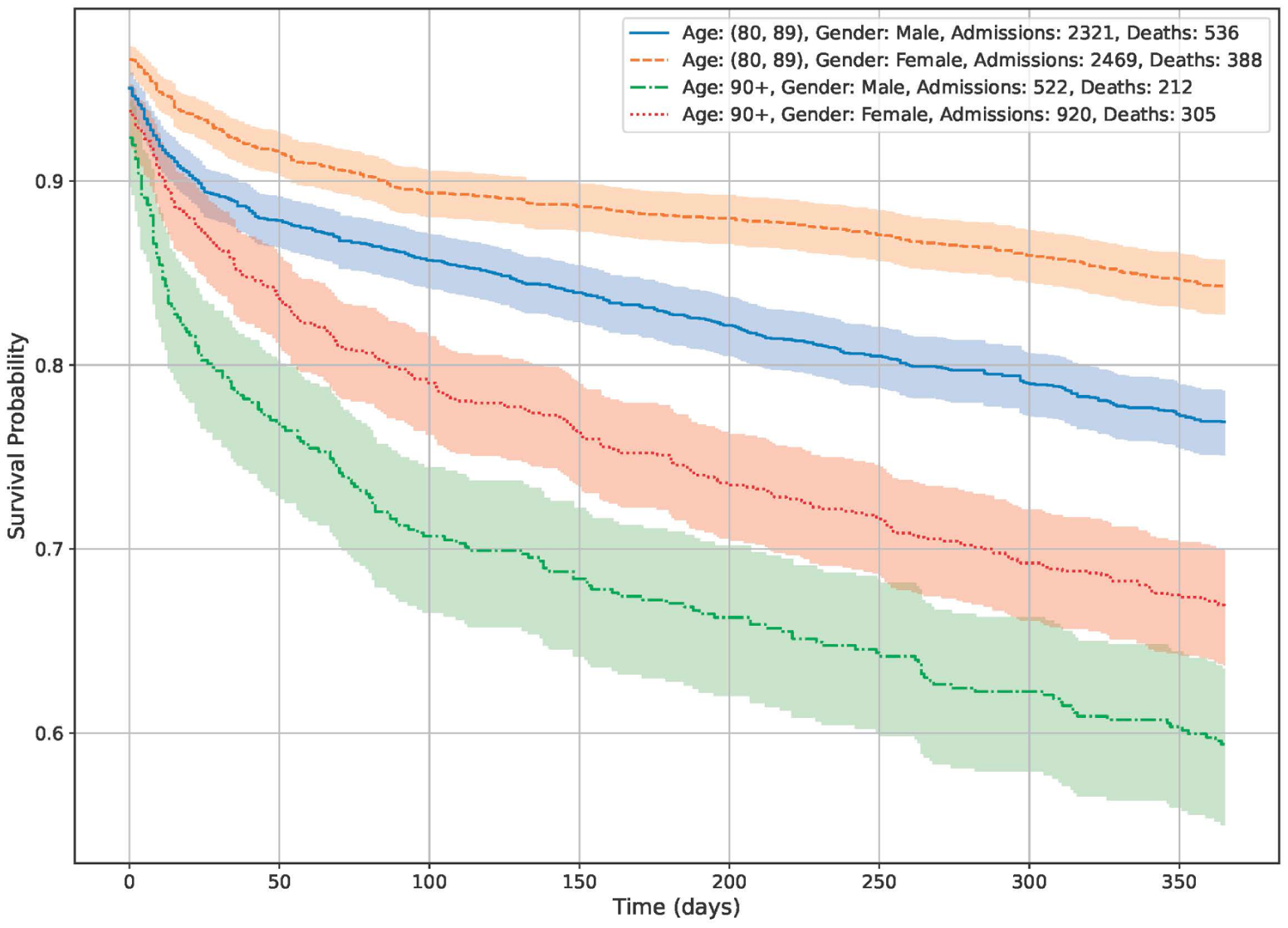
The effect of two age group 80–89 and 90+ years and gender (male or female) on survival in the first 365 days after the most recent hospital admission. Being a man and of advanced age is associated with higher mortality. The shaded areas are 95% confidence intervals.
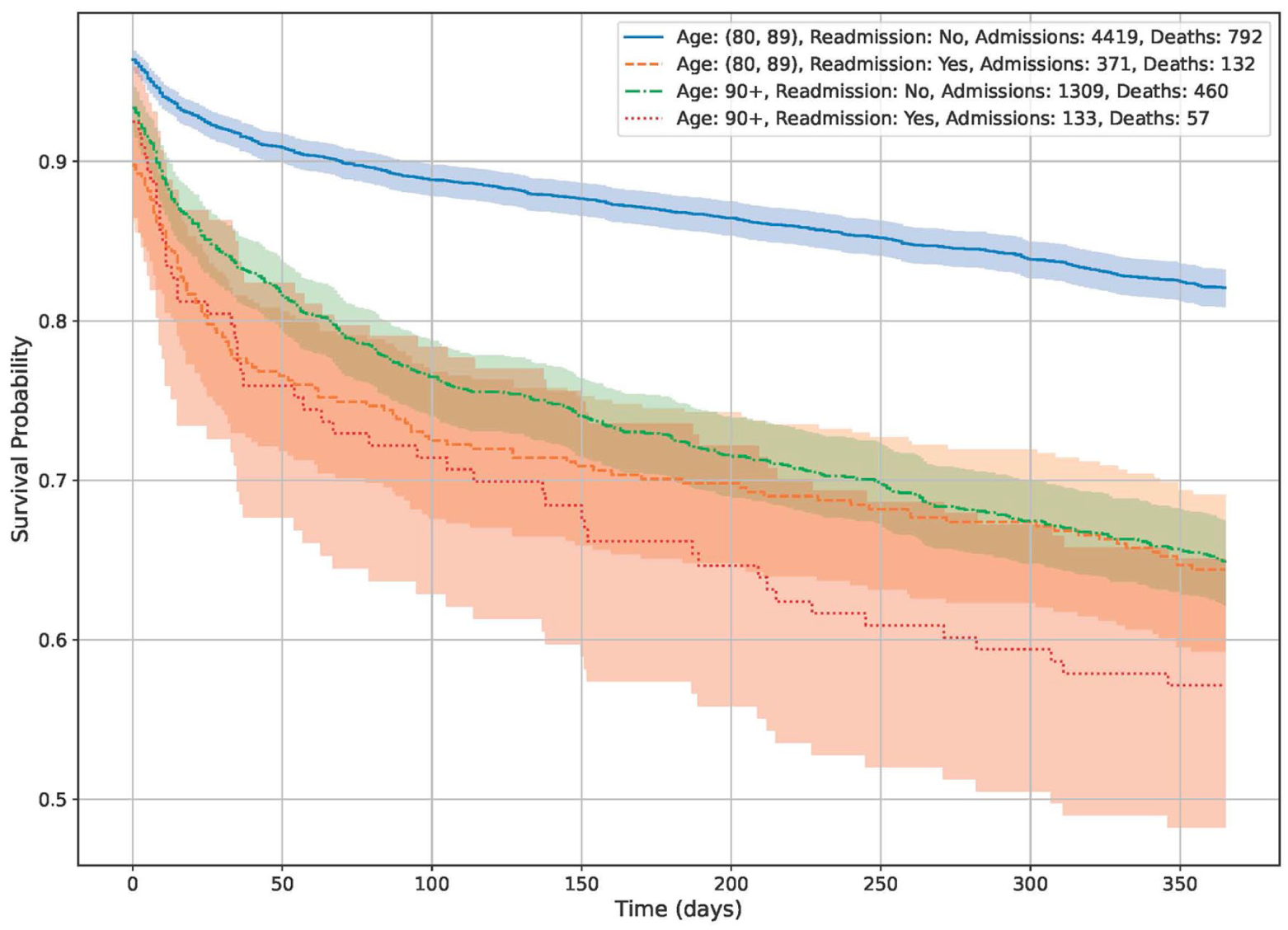
The effect of age (two groups) and readmission (yes/no) on survival in the first 365 days after the most recent hospital admission. Readmissions and advanced age are associated with higher mortality. The shaded areas are 95% confidence intervals.
Ethical considerations
The study was approved by the Norwegian Regional Health Research Committee West (ID 12394). As the analyses were based on the same dataset as that delivered to the Norwegian Patient Registry, informed consent was not considered necessary.
Results
Participants
The absolute number of hospital patients (and admissions) in the age cohort was 3992 (6410) in 2002, 5111 (8186) in 2012, and 6232 (10,273) in 2022. The proportion of all hospital admissions involving this age group increased from 11.3% to 14.7% over the study period (Table I). In the same period, the proportion of older adults (⩾80 years) in the main catchment area (Hordaland County) increased from 19.5% to 25.4% (Table I).
The total follow-up time for the 2012 and 2022 cohorts was 9554 and 12,278 person-years, respectively. Follow-up time for the 2002 cohort could not be calculated because mortality data were missing.
Descriptive data
There was only a modest increase in median age (from 84 to 85 years), and the proportion of women among the older inpatients decreased from 61.4% to 51.6%. The largest increases in admissions were observed in cardiology and in orthopaedic and general surgery. The marked increase in the ‘other departments’ category in the 2022 cohort reflects the establishment of a separate emergency department in 2020, which led to a reduction in admissions to other departments, particularly internal medicine.
Median hospital LOS decreased from 5 to 3 days. The proportion of emergency (unplanned) admissions declined slightly from 79.6% to 77.5% over the period. No relevant change was observed in the 30-day readmission rate (Table I).
Outcome data and main results
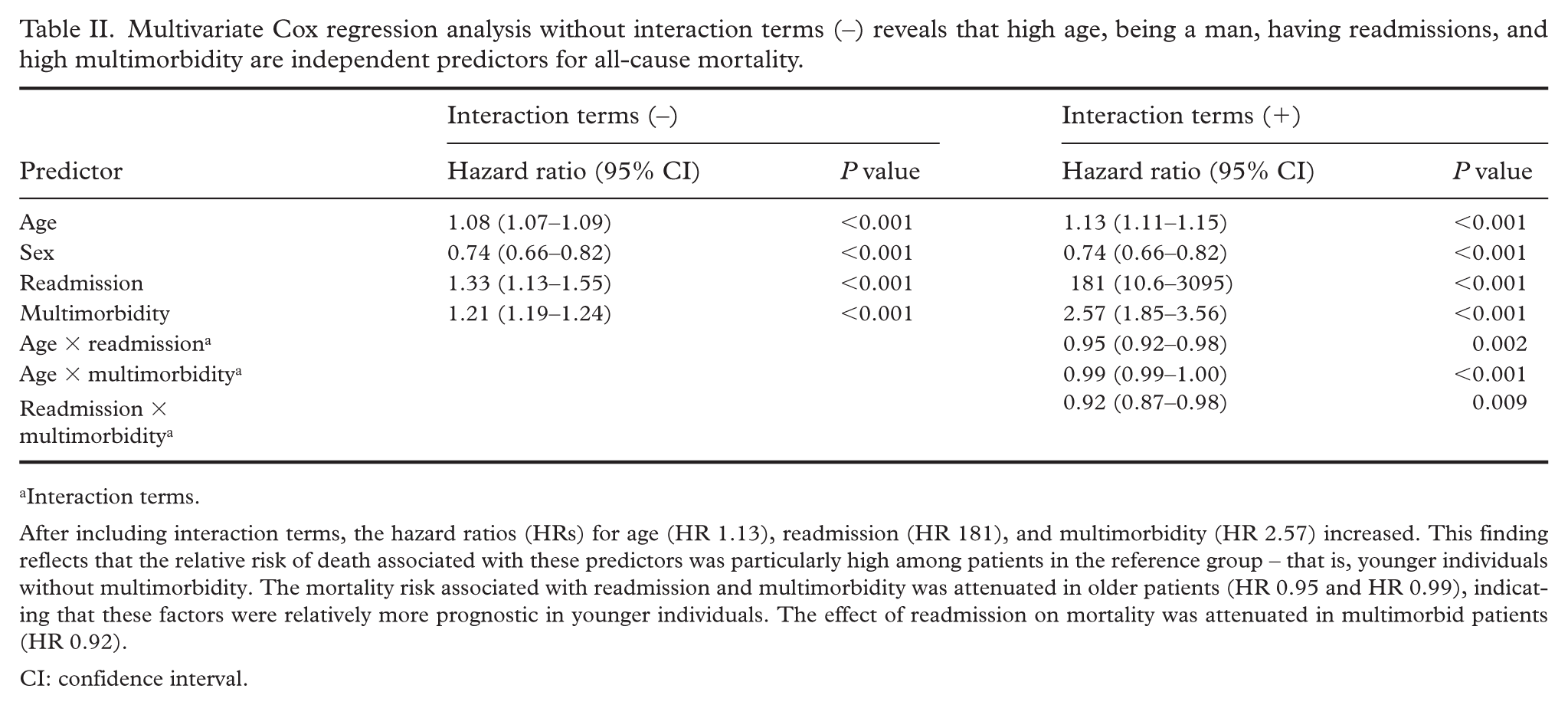
Results from the Cox regression analysis are shown in Table II. In the main effects model, each additional year of age was associated with an 8% higher risk of death (P<0.001, HR 1.08, 95% CI 1.07–1.09). Female patients had a 26% lower risk of death compared with men (P<0.001, HR 0.74, 95% CI 0.66–0.82). Experiencing a readmission was associated with a higher risk of death compared with a non-readmission hospital stay (P<0.001, HR 1.33, 95% CI 1.13–1.55), and higher levels of multimorbidity increased the risk of death (P<0.001, HR 1.21, 95% CI 1.19–1.24).
Multivariate Cox regression analysis without interaction terms (–) reveals that high age, being a man, having readmissions, and high multimorbidity are independent predictors for all-cause mortality.
Interaction terms.
After including interaction terms, the hazard ratios (HRs) for age (HR 1.13), readmission (HR 181), and multimorbidity (HR 2.57) increased. This finding reflects that the relative risk of death associated with these predictors was particularly high among patients in the reference group – that is, younger individuals without multimorbidity. The mortality risk associated with readmission and multimorbidity was attenuated in older patients (HR 0.95 and HR 0.99), indicating that these factors were relatively more prognostic in younger individuals. The effect of readmission on mortality was attenuated in multimorbid patients (HR 0.92).
CI: confidence interval.
In the extended model including interaction terms, the age × readmission interaction suggested that as age increased, the effect of readmission (P=0.002, HR 0.95, 95% CI 0.92–0.98) and multimorbidity (P<0.001, HR 0.99, 95% CI 0.99–1.00) on the risk of death was attenuated. Additionally, the readmission × multimorbidity interaction indicated that the combined effect of these factors on mortality was lower than would be expected if their effects were purely additive (P=0.009, HR 0.92, 95% CI 0.87–0.98). The proportional hazards assumption and the absence of time varying covariates were confirmed, with all predictors showing P values greater than 0.05 in the diagnostic tests.
Overall in-hospital mortality fell from 10% in 2002 to 4.7% in 2022, and one-year post-discharge mortality decreased from 2012 to 2022 (Table I). Post-hospital mortality data for 2002 were not available. In subgroup analyses, we found particularly high mortality in patients aged 90 years and over and in those with complex multimorbidity (Figure 1). There was also a marked sex difference: female patients without readmission had significantly better survival in both age groups (Figure 2). The effect of readmission on mortality is shown in Figure 3, stratified by age 80–89 years and 90 years and older. The impact of readmission was most pronounced in patients aged less than 90 years and less so in those aged 90 years and over. All figures are based on data from the 2022 cohort.
Discussion
In this study, we describe hospital use and outcomes – including LOS, mortality, and readmission – among patients aged 80 years an over in three different years between 2002 and 2022. We observed increases in admissions both in absolute numbers and relative to all hospital admissions within the catchment area. We also found reductions in hospital LOS and in both short and long-term mortality in the selected cohorts. Together, these findings illustrate the hospital’s ability to adapt to a growing patient load.
Regarding predictors of outcome, we found considerable differences in post-hospital mortality according to age group, sex, multimorbidity, and readmission. The worst outcomes, although observed in the smallest subgroups, occurred in patients with combinations of complex multimorbidity, readmission, and age 90 years and above.
Our data confirm previously reported trends of increasing hospitalisation among patients aged 80 years and over, both in absolute numbers and relative to the total hospital population. The absolute rise in admissions is at least partly explained by the growth in the older population during the study period. A nationwide study from Australia reported a 94% increase in hospital admissions, from 745 to 1441 per 1000 inhabitants, between 1993/94 and 2019/20 [10]. We also found a high mortality rate, with nearly one in four patients dying within the first year after discharge. In the general Norwegian population of similar age (85 years), the expected remaining life expectancy is 6.3 years [17].
Mortality was associated with several factors. When the admission was a readmission within 365 days after an index stay, the mortality risk almost doubled across age groups. Female patients, both with and without readmission, had a lower risk of dying within one year of admission. Finally, complex multimorbidity strongly reduced survival, particularly among patients aged 90 years and older. In a recent systematic review on the association between multimorbidity and hospitalisation in older adults, multimorbidity was likewise associated with an increased risk of adverse hospital outcomes [18].
Interpretation
The growing number of admissions and the associated use of hospital resources will have major implications for future healthcare systems. According to population forecasts, the number of older adults in our area will double by 2050 [17]. Assuming a similar case mix and treatment intensity, admissions in this age group at our hospital would increase from around 6000 to 12,000 per year, corresponding to more than 80,000 hospital days annually. It is unlikely that the average LOS (3.9 days) can be reduced further to increase throughput. We will therefore either need to increase the number of beds or find alternatives to hospital admission.
At present, an average of 110 beds per day are occupied by this patient group, representing 13% of the total somatic bed capacity. A proportional increase in staffed beds over the next decades is unrealistic, mainly due to economic constraints and expected limitations in workforce availability. If the younger population (18–65 years) decreases, it might be possible to shift some hospital resources from younger to older patients, but this is unlikely to meet the projected demand fully.
It is important to develop evidence-based strategies for prioritising hospital admissions in older patients and to create alternative care models for those who are not admitted. Our data suggest that restricting hospital admissions only for patients aged 90 years and above with multimorbidity would have a relatively small impact on overall resource use. Instead, we need responsible alternatives to hospital admission for older adults in general, solutions that are feasible and acceptable to patients and the community. Patient preferences should be available as a guide to decisions about admission, but these are often unknown in current practice.
Older patients are also particularly vulnerable to problems associated with hospitalisation [19,20]. Complications such as acute confusion/delirium, hospital-acquired infections, and inactivity leading to loss of muscle mass are common and may contribute to increased post-discharge mortality.
Many older patients are admitted from nursing homes. It will therefore be important to develop closer collaboration between hospitals and these facilities to identify and implement alternatives to hospital admission [21,22]. In another study, it was estimated that four in ten emergency admissions from nursing homes could be avoided by better preventive care [23]. Achieving this will require major changes in health policy, as well as real-time communication and support from hospitals.
Limitations
This was a retrospective study, albeit using prospectively collected data with few missing values. We lacked information on other age-related syndromes such as frailty, which is important for understanding outcomes in very old and acutely ill patients [24]. Frailty has been shown to be crucial; in a recent study, frailty alone and in combination with multimorbidity had pronounced effects on outcomes [19].
Our definition of complex multimorbidity differs from some previous studies, and there is currently no consensus definition. A recently published Delphi study agreed to define multimorbidity as the presence of two or more chronic conditions but did not reach consensus on a definition of complex multimorbidity [25]. Given the large number of comorbidities in older hospital patients, we consider the concept of complex multimorbidity more descriptive for our study population. We also lacked data on living situation (e.g. nursing home vs. own home) prior to admission.
The study includes patients from 2022, two years after the COVID-19 pandemic. According to hospital policy, restrictions on acute admissions in the elderly population had been lifted by the end of 2020 and therefore should not have influenced the 2022 cohort.
A strength of the study is the complete dataset including all admissions in the selected years, allowing us to observe real changes over time in this important patient group.
Conclusions
Our study confirms a substantial increase in admissions of older patients to our hospital over the past 20 years and projects an even greater rise in their admissions in the future. It is unlikely that we will be able to meet this demand relying on hospital admission alone. Our data indicate that restricting admission only in patients aged 90 years and over with multimorbidity would have limited impact. We therefore need to develop responsible alternatives to hospital admission for older adults – solutions that are feasible, acceptable, and aligned with patient preferences, which are too often unknown at present.
The increased use of resources in this group must also be considered within broader discussions on priority setting. Developing alternatives to emergency hospitalisation for nursing home residents in particular may substantially reduce hospital admissions. These are tasks that must be addressed now to prepare for the coming decades.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.