
Abstract
Introduction/Objectives:
To describe health outcomes of older adults enrolled in the Mayo Clinic Care Transitions (MCCT) program before and during the COVID-19 pandemic compared to unenrolled patients.
Methods:
We conducted a retrospective cohort study of adults (age >60 years) in the MCCT program compared to a usual care control group from January 1, 2019, to September 20, 2022. The MCCT program involved a home, telephonic, or telemedicine visit by an advanced care provider. Outcomes were 30- and 180-day hospital readmissions, emergency department (ED) visit, and mortality. We performed a subgroup analysis after March 1, 2020 (during the pandemic). We analyzed data with Cox proportional hazards regression models and hazard ratios (HRs) with 95% CIs.
Results:
Of the 1,012 patients total, 354 were in the MCCT program and 658 were in the usual care group with a mean (SD) age of 81.1 (9.1) years overall. Thirty-day readmission was 16.9% (60 of 354) for MCCT patients and 14.7% (97 of 658) for usual care patients (HR, 1.24; 95% CI, 0.88-1.75). During the pandemic, the 30-day readmission rate was 15.1% (28 of 186) for MCCT patients and 14.9% (68 of 455) for usual care patients (HR, 1.20; 95% CI, 0.75-1.91). There was no difference between groups for 180-day hospitalization, 30- or 180-day ED visit, and 30- or 180-day mortality.
Conclusions:
Numerous factors involving patients, providers, and health care delivery systems during the pandemic most likely contributed to these findings.
Introduction
COVID-19 has been a disruptive force in health care. It changed care delivery models through greater use of telehealth services and growth of virtual community-based care models. The Mayo Clinic Care Transitions (MCCT) program has successfully provided in-home medical care after hospitalization for over 10 years. 1 In our initial evaluation of home-based face-to-face visits, we found that the 30-day rehospitalization rate was 12% in an enrolled group and 20% in a matched control group (P = .002). 2 During the COVID-19 pandemic, the MCCT program shifted a large portion of visits to telephonic care, which decreased the number of face-to-face home visits. In assisted living facilities, telemedicine was rarely available because of a lack of available technology and telepresenters. The use of telemedicine during COVID-19 was widespread within our nursing home practice 3 and other home-based practices. There were other widespread changes in practice and patient behavior that led to a decreased number of cardiovascular-related hospital admissions overall. 4 Practice patterns are continuing to change as mask mandates change and vaccinations become widespread.
The medical and societal changes that occurred with the COVID-19 pandemic have been accompanied by changes to practice patterns and patient behavior. During the initial 6 months of the pandemic, a hospital system had a 50% decrease in skilled nursing facility (SNF) admissions but no change in hospital readmissions. 5 In a health system, changes to transitional care models included an initial doubling of telehealth visits to 30% of all transitional care management visits. 6 While the initial phase of the COVID-19 pandemic changed operational patterns such as hospital admissions and SNF placement, it has become less clear how home-based care transitions programs changed since the COVID-19 pandemic began.
Our primary aim was to determine the difference in 30-day hospital readmission rates for older adults between MCCT patients and a group of patients who were not admitted to the MCCT program before and after the COVID-19 pandemic began. A secondary aim was to determine the difference in other health outcomes (180-day hospital readmission, 30- and 180-day emergency department [ED] visit, and 30- and 180-day mortality) for MCCT patients compared to the usual care control group. As an exploratory analysis, we also compared differences in health outcomes between MCCT patients and a usual care group after the COVID-19 pandemic began.
Methods
Design and Setting
This retrospective cohort study included patients enrolled in MCCT and a usual care group not enrolled in the MCCT program. Both groups received primary care at Mayo Clinic in Rochester, Minnesota, with access to the MCCT program. We defined the beginning of the COVID-19 pandemic as March 1, 2020, and used medical records from January 1, 2019, to September 20, 2022. We conducted the study within the framework of the Declaration of Helsinki. 7 The Mayo Clinic COVID-19 Research Committee reviewed and approved the study, and the Mayo Clinic Institutional Review Board reviewed the study and waived the need for approval. We prepared the manuscript in accordance with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies 8 (Supplemental Table 1).
MCCT Participants
Participants in the MCCT cohort met clinical criteria for inclusion within the MCCT program. All participants had an index hospitalization (medical or surgical), which was the hospitalization that preceded enrollment in CT. They were 60 years or older, and had an Elders Risk Assessment (ERA) score greater than 16, which placed patients in the top 10% for the risk of hospital admission within 2 years. 9 MCCT patients were excluded if they were enrolled in hospice or other care management programs. We excluded participants if they had refused medical record review in accordance with the Minnesota state statute. 10 Patients were also excluded if they lived outside the usual catchment area for the hospital or were discharged to a hospice program or a skilled nursing care facility.
Usual Care Participants
Usual care participants were hospitalized patients who met MCCT criteria but were not subsequently enrolled in the program. All patients in both usual care and MCCT groups received standard dismissal planning, including a written dismissal summary, medication reconciliation, and communication with the primary team in accordance with principles to reduce readmission. 11 We determined the reason for not being enrolled and included adults who were not in the MCCT program because of the capacity of the program. We did not include patients who refused MCCT enrollment. Patients in the usual care population had similar ages, comorbid health conditions, and risks for hospital readmission (according to the ERA scores). 9 We excluded usual care participants who refused medical record review, lived outside the normal catchment area for the hospital, or were discharged to hospice or nursing homes. 12
MCCT Program
Details of the MCCT program before the COVID-19 pandemic have been described.2,13 The primary goal of the CT program is to identify the patients who have the highest risk for hospital readmission and provide more resources to them. This program has reduced hospital readmission. 2 We enrolled patients who were hospitalized with an Elder Risk Assessment Score of 15 or higher, which placed them at high risk for readmission. Patients were not offered enrollment if they were in other care management programs such as dialysis or hospice. We called the patient or their caregiver to ask if they would like to be enrolled in the program. 14 An advanced practice provider (APP) evaluated patients within 5 business days at their home. The APP performed a detailed geriatric assessment that included medication reconciliation, acute disease management, evaluation of community resources, advanced care planning, and chronic disease management. 14 The MCCT team included a registered nurse who performed care management through telephone visits. 2 All participants are discussed in an interdisciplinary team meeting with a geriatrician, nurse, and APP. 1 Participants were enrolled in the program for 180 days, which differs from the 60 days previously reported. 2
During the initial months of the COVID-19 pandemic, the MCCT practice shifted a large part of its follow-up care to telephonic care, but the exact percentage was not quantified.3,15 We considered telehealth as the use of a video-based method of communication and telephone care as non–face-to-face care. The senior housing facilities where patients lived often had visitor restrictions, which have been described by others.16,17 In a few assisted living facilities we used telemedicine technology with an iPad (Apple Inc) and a Teladoc platform (Teladoc Health, Inc). This technology allowed visual evaluation of the patient and caregiver but not the use of peripheral devices (eg, a stethoscope). Patients were allowed to use family members for assistance and help with the visit. When telemedicine was not an option, telephone-based care was used with the medical team (an APP, a physician, or a registered nurse).
Primary Outcome
The primary outcome was 30-day hospital readmission after hospital dismissal. Secondary outcomes were 180-day hospital admission, 30- and 180-day ED visits, and 30- and 180-day mortality. We determined hospital readmission from billing codes, which included both inpatient stay and outpatient observation from the electronic health record (EHR). We determined ED visits from EHR billing codes. Mortality at 30 and 180 days was recorded within the medical record from hospital and community resources. We determined mortality within the community and our cohort with the use of existing algorithms, which closely approximated data from the National Vital Statistics Reports. 18
Predictors
We collected primary predictors for hospitalization from literature on hospital readmission. To decrease referral bias, we used the community-based population. We reported the following demographic factors from the EHR: age (in years); gender (self-reported as male or female; data for sex at birth were missing); marital status (yes for married/life partner; no for other categories of marital status); race (Asian/Pacific Islander, Black, White, or Other); primary language (English or Other); and ethnicity.
We also collected data on medical and hospitalization predictors. For medical complexity and comorbidity, we used the Elixhauser Comorbidity Index and International Statistical Classification of Diseases, Tenth Revision (ICD-10) codes for 31 illnesses. 19 Use of the Elixhauser Comorbidity Index should approximate a frailty index score 20 as developed by Rockwood et al. 21 We also determined a dementia diagnosis from ICD-10 codes (Supplemental Table 2). We determined the index hospital length of stay, discharge date, and intensive care unit (ICU) stay from billing codes and EHR information. We calculated the Area Deprivation Index (ADI) for participants from zip codes with census blocks mapped to the ADI state rankings as reported through the University of Wisconsin-Madison Neighborhood Atlas. 22 The ADI uses 17 parameters of socioeconomic status, including income and employment, to determine a score that is associated with a higher or lower socioeconomic status. 22 Differences in the ADI have been associated with mortality rates. 23 We calculated ADI for our cohort from state ADI values for Minnesota, Iowa, and Wisconsin.
Analysis
We included all MCCT and usual care participants who met the inclusion criteria during the time frame of the study, and we described the records that were not used in the study. Descriptive statistics are reported for patient characteristics of the MCCT and usual care groups with both mean (SD) and median (IQR). We summarized categorical data with frequencies and percentages and reported χ2 values to investigate group differences. We selected t test comparisons for continuous variables.
We compared health outcomes between the MCCT participants and the usual care group with use of a fully adjusted model for age, gender, marital status, race, ethnicity, ICU stay on index hospitalization, length of hospital stays, Elixhauser Comorbidity Index, and the ADI score. We used Kaplan-Meier survival curves to compare the groups at the bivariate level and then used the log-rank test to investigate differences in events between groups. Cox proportional hazards regression models were used to determine the independent effect of the intervention with adjustment for covariates. We considered differences between groups as significant if P was less than .05 and the 95% CI did not include zero. For our secondary outcome of subgroup analysis of MCCT patients and usual care participants enrolled after COVID-19 measures were implemented, we applied similar methods as above. To investigate differences during the COVID-19 pandemic, the study team reported models after admissions that occurred after March 1, 2020. We used the same fully adjusted Cox proportional hazards models for comparisons between the MCCT group and the usual care group and for a noninferiority analysis to assess any differences in the impact of the MCCT model during the COVID-19 pandemic by comparing outcomes for patients who were enrolled in the MCCT program before the pandemic to those for patients enrolled during the pandemic.
Results
Population
Of the 1749 patients initially considered for our study, 737 were excluded because they did not provide consent for research authorization, they lived outside the catchment area, or they were discharged to hospice or a SNF. The remaining 1012 participants included 354 who were enrolled in MCCT and 658 in the usual care group (Figure 1). The mean (SD) age was 81.8 (8.9) years in the MCCT group and 80.7 (9.1) years in the usual care group (P = .049). In the MCCT group, 46.9% were female compared to 47.4% in the usual care group (P = .87), and 95.2% in the MCCT group were White compared to 93.0% in the usual care group (P = .30). The mean (SD) number of comorbid health conditions was 8.9 (3.2) in the MCCT group and 8.9 (3.2) in the usual care group (P = .73). The overall average ADI was 44.8 (17.7) for the entire cohort, which is not in a disadvantaged area. 24 There were no significant differences between the MCCT group and the usual care group for primary language, ethnicity, marital status, dementia diagnosis, ADI score, initial hospital length of stay, or ICU stay at initial admission (Table 1).

Flow diagram of patient enrollment in Mayo Clinic Care Transitions program.
Demographic Characteristics of Patients Enrolled in MCCT and Patients Not Enrolled in MCCT.
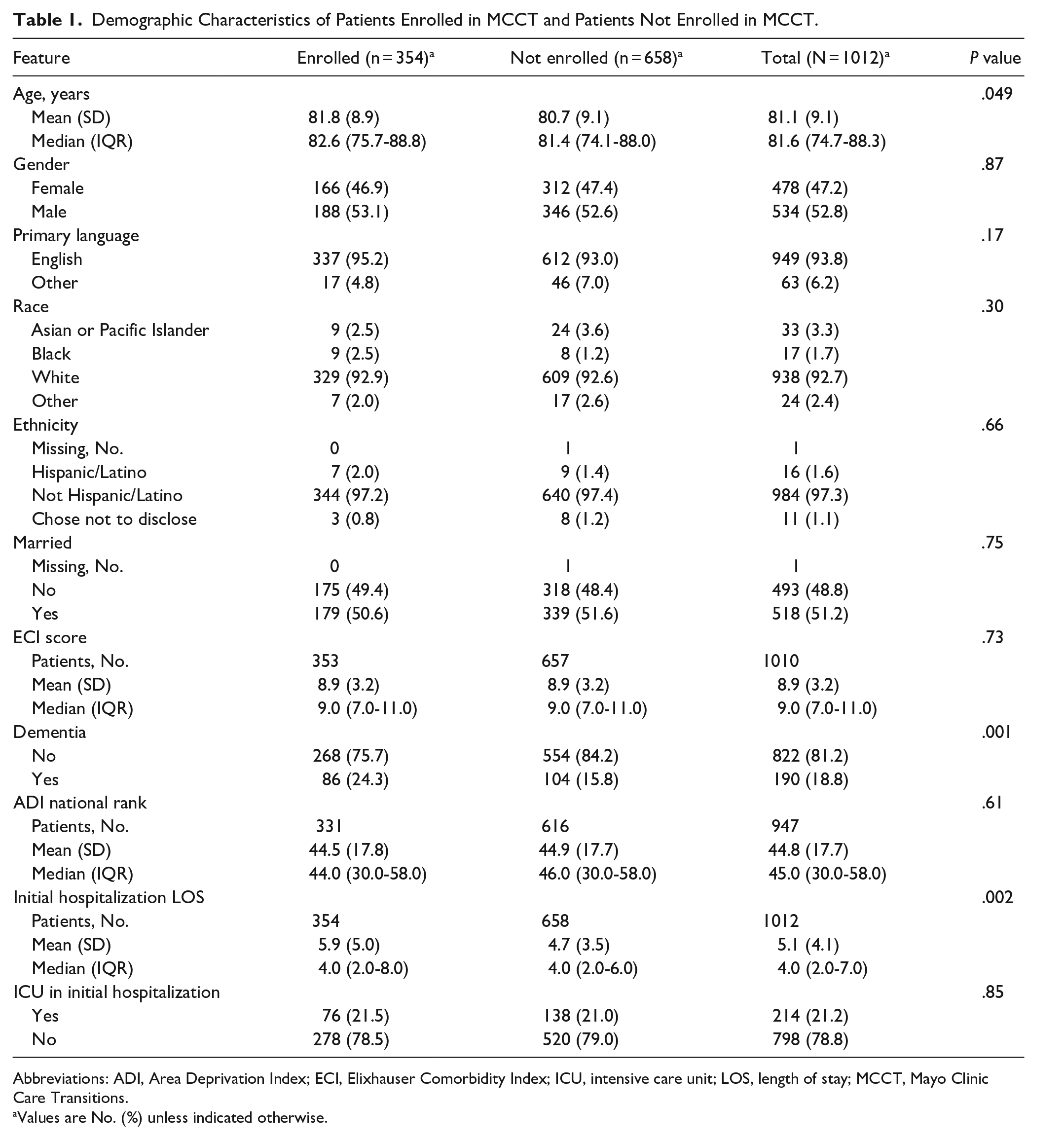
Abbreviations: ADI, Area Deprivation Index; ECI, Elixhauser Comorbidity Index; ICU, intensive care unit; LOS, length of stay; MCCT, Mayo Clinic Care Transitions.
Values are No. (%) unless indicated otherwise.
Hospital Admissions and Health Outcomes for Overall Cohort
Within 30 days of hospital dismissal, 60 patients (16.9%) were admitted from the MCCT group compared to 97 patients (14.7%) in the usual care group (hazard ratio [HR], 1.24; 95% CI, 0.88-1.75) after full adjustment. At 180 days, 128 patients (36.2%) were admitted from the MCCT group compared to 227 (34.5%) in the usual care group (HR, 1.09; 95% CI, 0.87-1.37). Mortality was similar between the 2 groups: 3 MCCT patients (0.8%) died, and 11 usual care patients (1.7%) died (HR, 0.33; 95% CI, 0.10-1.37). There were no significant differences between the MCCT group and the usual care group for 30-day ED visit, 180-day ED visit, or 180-day mortality (Table 2).
Cox Proportional Hazards Models for Outcomes at 30 and 180 Days After Discharge for Patients Enrolled in MCCT and Patients Not Enrolled in MCCT.
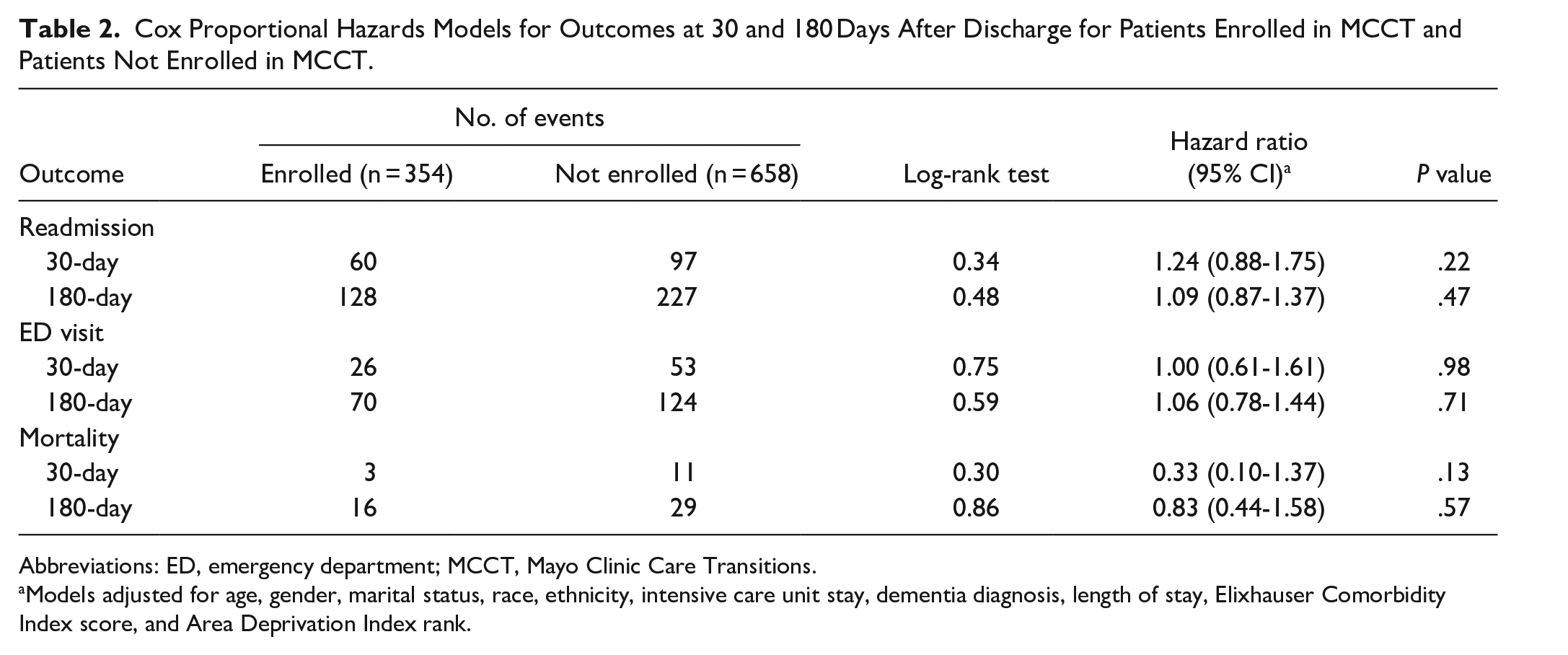
Abbreviations: ED, emergency department; MCCT, Mayo Clinic Care Transitions.
Models adjusted for age, gender, marital status, race, ethnicity, intensive care unit stay, dementia diagnosis, length of stay, Elixhauser Comorbidity Index score, and Area Deprivation Index rank.
Hospital Admissions and Health Outcomes for MCCT Patients and Usual Care Group Patients After the COVID-19 Pandemic Began
In the subgroup of patients seen after the COVID-19 pandemic began (MCCT enrollment after March 1, 2020), we found similar outcomes for hospital admissions and health outcomes. The 30-day hospital readmission rate was 15.0% (28 of 186 patients) for the MCCT group and 14.9% (68 of 455 patients) for the usual care group (HR, 1.20; 95% CI, 0.75-1.91). The 30-day mortality was 0.5% (1 of 186 patients) for the MCCT group and 2.2% (10 of 455 patients) for the usual care group (HR, 0.23; 95% CI, 0.03-1.84). Similarly, outcomes were not different between the MCCT group and the usual care group for 180-day hospital readmission, 30-day ED visit, 180-day ED visit, and 180-day mortality (Table 3).
Cox Proportional Hazards Models for Outcomes at 30 and 180 Days After Discharge for Patients Enrolled in MCCT and Patients Not Enrolled in MCCT During the COVID-19 Pandemic. a

Abbreviations: ED, emergency department; MCCT, Mayo Clinic Care Transitions.
Enrollment after March 1, 2020.
Models adjusted for age, gender, marital status, race, ethnicity, intensive care unit stay, dementia diagnosis, length of stay, Elixhauser Comorbidity Index score, and Area Deprivation Index rank.
Hospital Admissions and Health Outcomes for MCCT Patients Before and During the COVID-19 Pandemic
In the within-group analysis, we found no significant differences in outcomes for patients who were enrolled in the MCCT model during the COVID-19 pandemic compared to patients enrolled before the pandemic. The 30-day hospital readmission rate was 15.0% (28 of 186 patients) during the pandemic and 19.0% (32 of 168 patients) before the pandemic (HR, 0.79; 95% CI, 0.47-1.31). The 30-day mortality was 0.5% (1 of 186 patients) during the pandemic and 1.2% (2 of 168 patients) before the pandemic (HR, 0.44; 95% CI, 0.04-4.83). Similarly, outcomes were not different before and after the pandemic for 180-day hospital readmission, 30-day ED visit, 180-day ED visit, and 180-day mortality (Table 4).
Cox Proportional Hazards Models for Outcomes at 30 and 180 Days After Discharge for Patients Enrolled in MCCT Before and During the COVID-19 Pandemic.
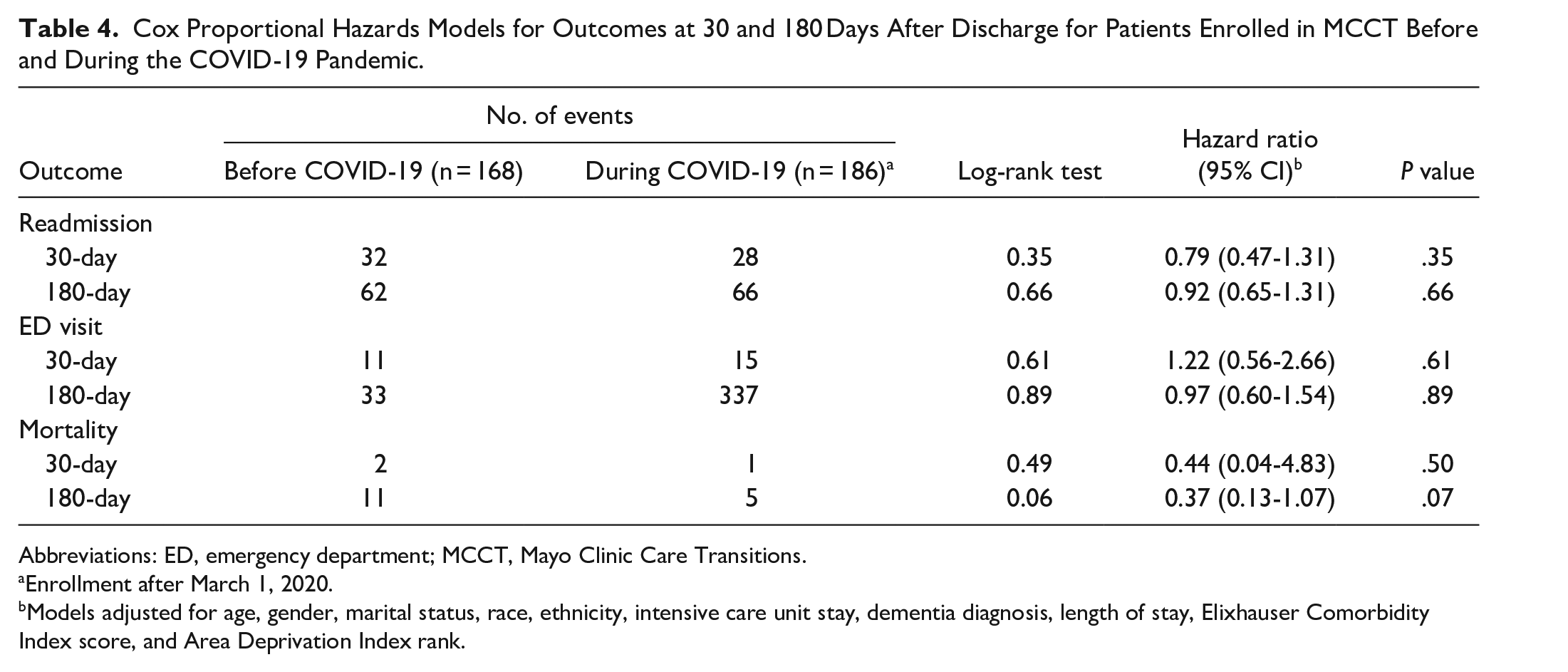
Abbreviations: ED, emergency department; MCCT, Mayo Clinic Care Transitions.
Enrollment after March 1, 2020.
Models adjusted for age, gender, marital status, race, ethnicity, intensive care unit stay, dementia diagnosis, length of stay, Elixhauser Comorbidity Index score, and Area Deprivation Index rank.
Discussion
In our study of 354 MCCT patients, we did not find a difference in 30-day hospital readmission compared to an adjusted usual care population overall and during the COVID-19 pandemic. These findings differ from our previous experience, which showed an absolute risk reduction in 30-day hospital readmission of 7.7%. 2 When compared to readmission rates in previous studies, the 30-day hospital readmission rates of 16.9% for the MCCT group and 14.7% for the usual care group in the present study are slightly higher for the MCCT group and much lower for the usual care group. 2 We learned that the readmission rate for CT did not worsen during the pandemic; however, we did not maintain a lower readmission rate.
Generally, use of care transitions has been favorable for most health systems. In recent systematic reviews of care transitions for patients with heart failure, authors have described the efficacy of care transitions that provide communication by telephone or telemonitoring. 25 In a systematic review of older adults with multiple medical conditions, authors found a decrease in hospital readmission among patients enrolled in care transitions programs compared to patients receiving usual care. 26 In other studies performed before the COVID-19 pandemic, care transitions programs have shown a general reduction in 30-day readmission; however, in some trials the programs have not shown efficacy. 27 Many care transitions programs use an in-person component such as an APP for visits. 28 In our program, patients reported that the presence of the provider within the home improved communication and peace of mind. 29 Our study provides some novel findings that show the efficacy of a care transitions program before and during the COVID-19 pandemic as our care model changed.
In comparing our overall findings and the findings during the pandemic, we found that changes related to the pandemic may have decreased the efficacy of the MCCT program. Specifically, the 30-day hospital readmission rate was higher for the MCCT group (16.9%) compared to the usual care group (14.7%), but the difference was not significant (P = .22). There are several potential explanations for these findings. The MCCT program relies heavily on continuity of care in face-to-face visits with patients and informal caregivers, and this process was disrupted during the COVID-19 pandemic. While telephonic follow-up was used, this modality may have less efficacy in this high-risk population. In a meta-analysis of patients with heart failure, the use of management by telephone showed no effects on hospital readmission. However, in a separate study with patients who had comorbid conditions, the findings suggested that telephone visits had some efficacy. 30 Thus, the efficacy of the telephone is not completely clear. Moreover, the pandemic decreased the availability of family visits, and this factor may have also contributed to delays in identification of changes in the patient’s condition. Patients may have increased their familiarity with the health system and sought more care as situations arose. The reasons for the apparent decrease in readmissions for the usual care group are less clear. However, hospital ED visits in the US decreased by 42% during this time. 31 Hospital admissions were highly restricted during the pandemic, and it is possible that discretionary readmissions were decreased. More analysis would be needed to see whether other quality measures were affected.
Our study had strengths and some weaknesses. Strengths include the relatively large number of admissions (>300) into the MCCT program, which has been operating for more than 10 years. Also, our integrated medical system with team-based care allows communication between primary care, hospital, and speciality care providers. 32 In contrast, we recognize the weaknesses that are often inherent in cohort studies. We may have missed outcomes or potentially predictors if patients went to different health systems; this was minimized because we have an integrated medical system and a geographically contained region for medical care. We aggregated readmissions because of the size of our study. Apart from what we have already hypothesized, there may have been other disruptions during the COVID-19 pandemic that have not been identified or quantified. The population of Olmsted County, Minnesota, is predominantly White and representative of the Upper Midwest of the US. 33 Similarly, our cohort was a predominantly non-Hispanic White population. Therefore, our findings may not generalize to other regions or other countries. Specifically, access to health care may vary among racial and ethnic groups.
Conclusion
We found that the efficacy of our MCCT program most likely was diminished during the COVID-19 pandemic as we did not find a difference in 30-day readmission between those enrolled in the program and those not enrolled. This differs from our previous findings, and the present findings most likely have several reasons, some of which are identified and perhaps some not yet well identified, to explain what we found during a once-in-100-years pandemic.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241226547 – Supplemental material for Impact of Program Changes Including Telemedicine and Telephonic Care During the COVID-19 Pandemic in Preventing 30-Day Hospital Readmission for Patients in a Care Transitions Program
Supplemental material, sj-docx-1-jpc-10.1177_21501319241226547 for Impact of Program Changes Including Telemedicine and Telephonic Care During the COVID-19 Pandemic in Preventing 30-Day Hospital Readmission for Patients in a Care Transitions Program by Paul Y. Takahashi, Bjorg Thorsteinsdottir, Rozalina G. McCoy, Priya Ramar, Rachel E. Canning, Gregory J. Hanson, Lori J. Baumbach, Anupam Chandra and Lindsey M. Philpot in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_21501319241226547 – Supplemental material for Impact of Program Changes Including Telemedicine and Telephonic Care During the COVID-19 Pandemic in Preventing 30-Day Hospital Readmission for Patients in a Care Transitions Program
Supplemental material, sj-docx-2-jpc-10.1177_21501319241226547 for Impact of Program Changes Including Telemedicine and Telephonic Care During the COVID-19 Pandemic in Preventing 30-Day Hospital Readmission for Patients in a Care Transitions Program by Paul Y. Takahashi, Bjorg Thorsteinsdottir, Rozalina G. McCoy, Priya Ramar, Rachel E. Canning, Gregory J. Hanson, Lori J. Baumbach, Anupam Chandra and Lindsey M. Philpot in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We acknowledge the Division of Community Internal Medicine, Geriatrics, and Palliative Care for support of this study. Randall J. Fritz, DVM, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading, administrative, and clerical support. The authors have authorized Scientific Publications to submit the manuscript on their behalf and the authors have approved all statement and declarations.
Author Contributions
The authors contributed to the study in the following ways: Collection of data: R.E.C.; Analysis of data: R.E.C., P.R.; Interpretation of results: P.Y.T., B.T., R.G.M., G.J.H., L.J.B., A.C., L.M.P.; Writing: P.Y.T., R.E.C., P.R., L.M.P.; Reviewing manuscript with revisions: all authors; Funding: P.Y.T.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Division of Community Internal Medicine, Geriatrics, and Palliative Care, Mayo Clinic, provided support for this study.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The authors retained full control of the study.
Data Availability Statement
All relevant data supporting the findings of this study are reported within the article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.