
Abstract
Aims:
The aim of this study was to explore how professionals within the child health, education and welfare sectors perceive the process of identification and how they care for children and young people (CYP) living with problematic substance use (PSU) in their families. We also sought to understand the perceptions of engagements and needs of adolescents living with PSU in their families.
Methods:
We combine five focus group interviews with professionals and six individual interviews with adolescents. We employ systematic text condensation in a cross-case thematic analysis and discuss our findings, considering Bronfenbrenner’s bioecological model.
Results:
Professionals face barriers to identifying affected CYP on multiple levels and uncertainty about signs of adversities, corresponding to the experiences of adolescents who emphasise a need for vigilant adults. However, the results also suggest the school setting as an enabling arena for identification, follow-up and interdisciplinary collaboration. Both parties request a community of experience in support groups with peers for CYP and increased knowledge on how substance use affects family members.
Conclusions:
Keywords
Background
The high global prevalence of adult substance use disorders (SUD) means many children and young people (CYP) grow up with problematic substance use (PSU) in their families, which may have profound negative consequences for them [1,2]. Families describe conflicting needs for privacy and openness, and CYP often internalise the unspoken rule of family secrecy [3]. Although there are familial pressures placed on CYP to keep secret, professionals within the child health, education and welfare sectors, such as educational staff, Child School Health Nurses (CSHN) and Child Welfare Service (CWS) staff are in unique positions to identify and support CYP who experience PSU. Barriers to uncover CYP exposed to PSU exist within both the families and professionals engaging with them. Families also experience that, despite awareness of parental PSU, bystanders—including relatives, neighbours and professionals—often show reluctance to act [4]. The literature on professionals’ practices reveal difficulties in identification and emotional strain that may cause avoidance [5]. The majority of studies on professionals approaching childhood adversities explore perspectives of health and social workers. There is less research on teachers’ roles. However, teachers are well placed to observe students’ mental health over time, but report a perceived lack of requisite proficiency to assess their mental health needs and identify early warning signs [6]. Teachers value interprofessional collaboration with health care professionals [7], and CSHNs share teachers’ views [8]. Exposed CYP need professionals they trust who understand the situation’s complexity [9]. The needs of CYP and the role professionals play can be explored within a framework of bioecological development, which entails understanding children’s development in relation to the environment in which they live (Figure 1) [10]. CYP engage in everyday interactions with their immediate environments, also called proximal processes [11]. These are reciprocally influenced by involved processes, persons, contexts and time (PPCT) and may, if negative, lead to dysfunction [12]. The proximal processes take place only in the context of microsystems in which CYP interact directly, such as in their homes, at school or with peers. The interaction between these microsystems, such as home–school relations, is called the mesosystem. The lives of CYP are also influenced by contexts in which they do not naturally take a part: exo-systems, such as parents’ social network, and macrosystems such as societal norms [10].
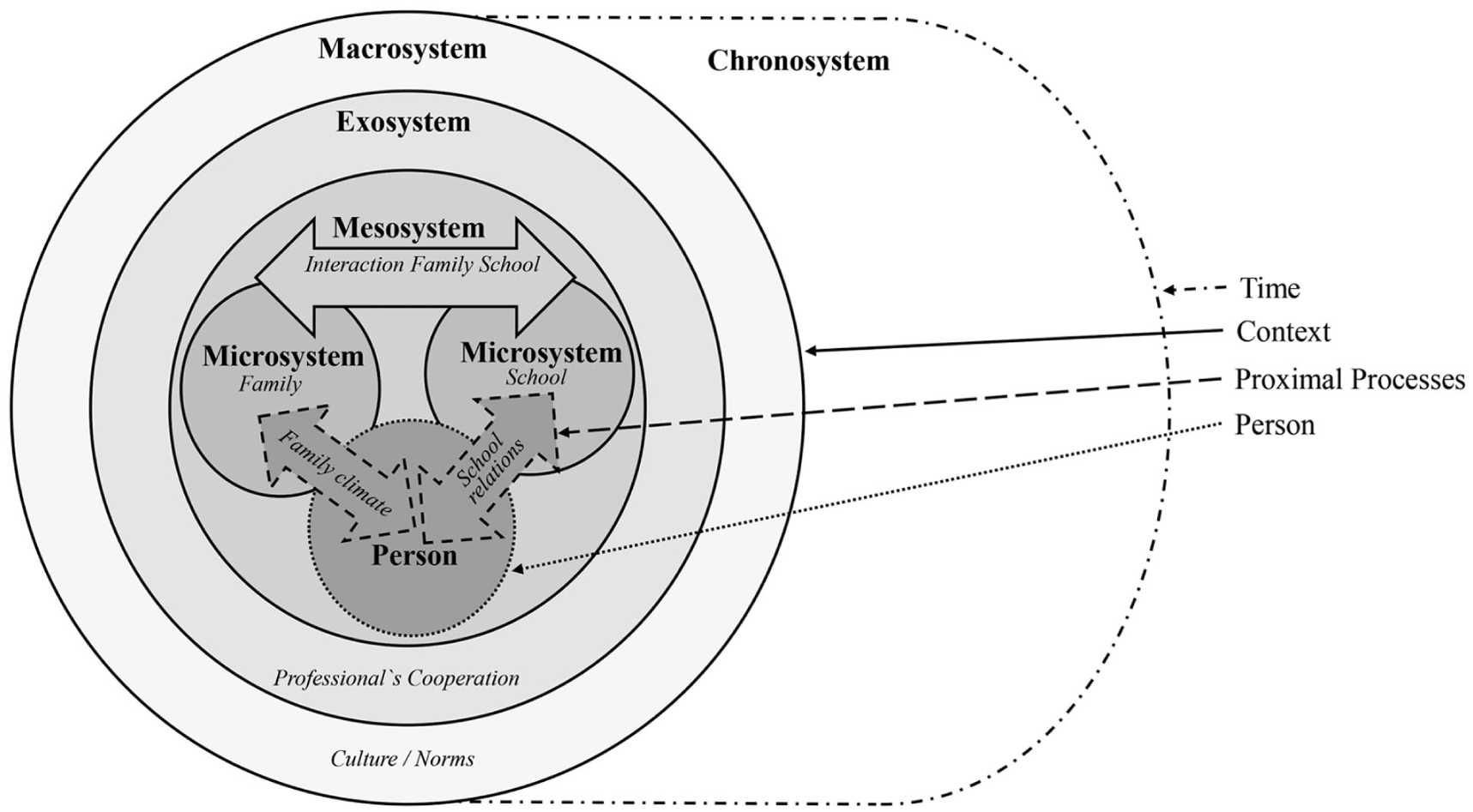
Conceptual model integrating Bronfenbrenner’s original nested layers of environmental system with the PPCT model. The figure has been modified in agreement with its original author to fit the current context [33]. PPCT, process-person-context-time.
Around two students per school class in Norway have at least one parent with an alcohol use disorder [13]. To address the needs of affected CYP, legislative and policy measures have been implemented, including provisions for follow-up when they are next of kin to a family member with PSU [14]. National strategies aim to strengthen students’ psychosocial wellbeing in schools and enhance collaboration among professionals [15]. These multi-level efforts prove there is a will to safeguard the development of CYP, and there is a call for studies on how to identify and understand their needs [16]. Thus, the present study is highly relevant from a public health perspective.
To our knowledge no previous studies have explored, within the same study, the experiences of both adolescents and professionals in identifying and addressing the needs of affected CYP. We aim to explore how professionals perceive the process of identification and caring for CYP living with PSU. By exploring the voices of adolescents, we gain insights into their perceptions of engagements and needs interacting within their surroundings.
Methods
We conducted qualitative semi-structured individual interviews and focus groups, separately (Table I). The purposeful sample of focus group participants comprised in total 25 professionals from CWS (n = 6), teaching staff in primary (n = 4) and secondary (n = 4) schools, CSHNs (n = 4) and kindergarten staff (n = 7)—hereafter collectively referred to as professionals—all working with CYP on a day-to-day basis. The Norwegian child welfare service is family-oriented, prioritising early intervention and support, while also holding the authority to intervene in severe cases of child neglect and maltreatment. As such, it has a dual role within the same organisation [17]. Although the CWS is not situated permanently in all educational institutions, they contribute to interdisciplinary teams in a consultative and supportive role. The CSHNs are present in schools, enabling teacher–CSHN collaboration. We recruited the focus group participants from five different community level institutions. Individual interviews included six adolescents who had attended a psychoeducational programme for family members affected by SUDs, at an addiction unit within regional level specialised health services. Out of 20 possible candidates in the programme in 2016 and 2017, 6 agreed to participate. The psychoeducational program included structured group sessions designed to facilitate peer interaction and the sharing of experiences [18].
Focus group and individual interview participants.
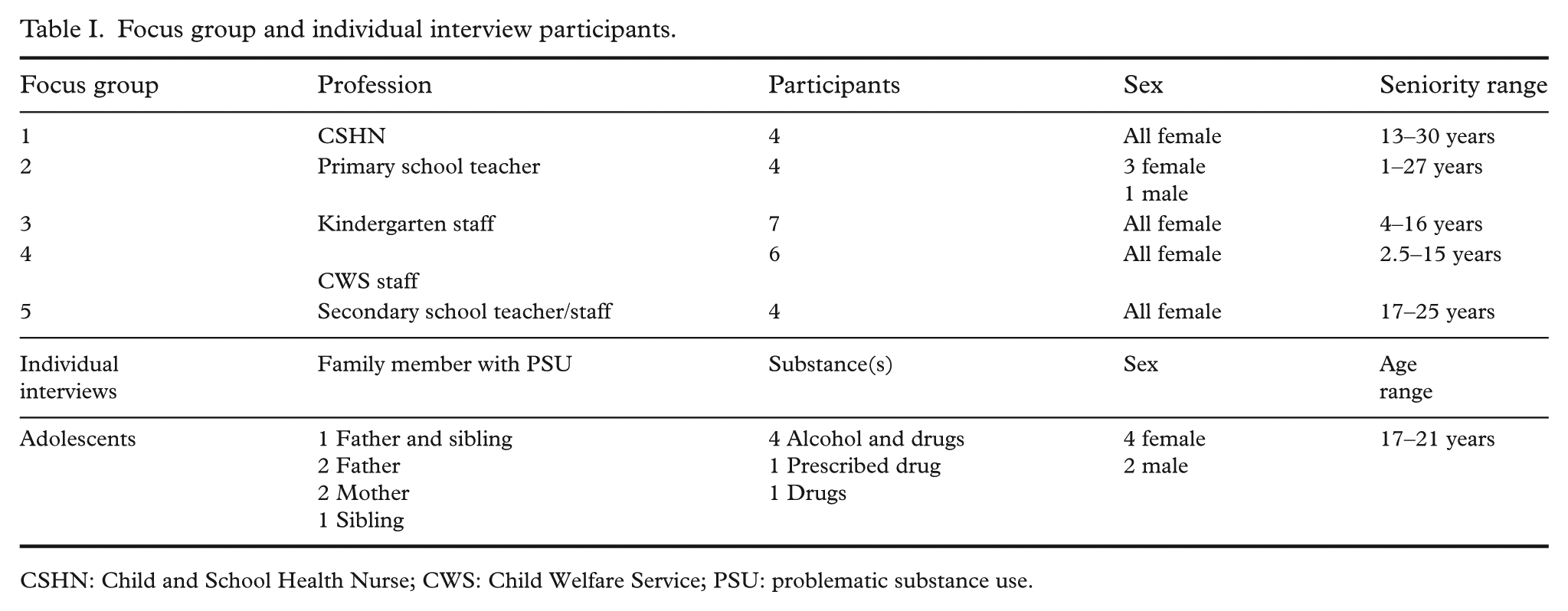
CSHN: Child and School Health Nurse; CWS: Child Welfare Service; PSU: problematic substance use.
Both semi-structured interview guides were developed by the research team (Table II). A user participant was consulted for input on the guide for the individual interviews. The interview guides were employed in a flexible manner, consistent with an exploratory approach. The first author conducted all interviews, with the last author supervising one individual interview and all focus group interviews. The interviews lasted from 50 to 90 min and were audiotaped and transcribed verbatim. We conducted the individual interviews in 2018, while the focus group interviews took place in 2024. Insights from adolescent interviews informed the preparation of the focus group interviews by providing contextual understanding of interactions of CYP with professionals.
Interview guide themes with example questions.
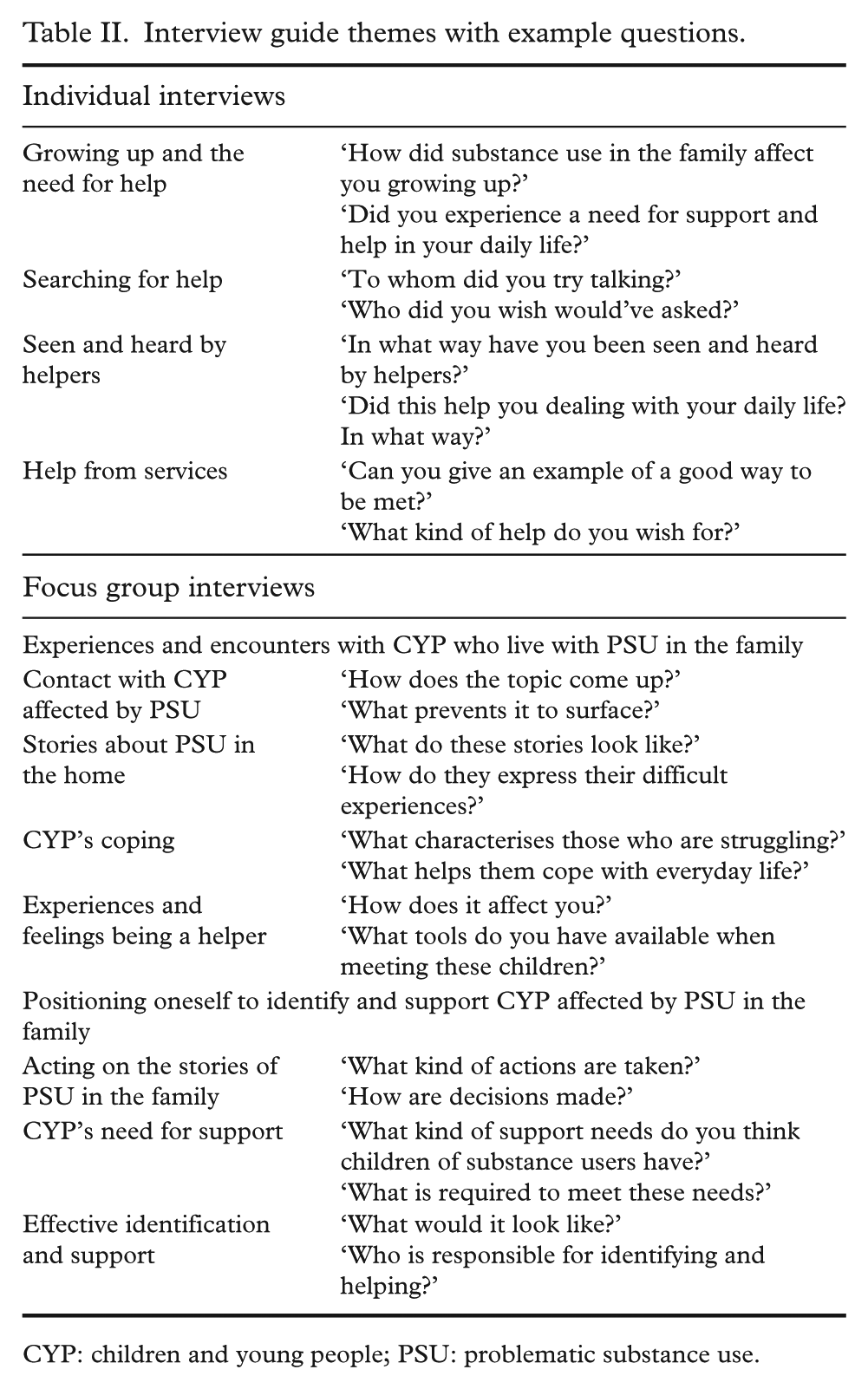
CYP: children and young people; PSU: problematic substance use.
The size of the sample was evaluated according to the concept of information power [19]. The sample specificity was high for the study’s aim, including professionals working with CYP daily and with long-term experience from five different fields, and six adolescents who had diverse experiences with PSU in their family. The researchers possessed extensive clinical experience and proficiency in dialogue techniques, which was expected to enhance the potential for eliciting rich and meaningful dialogues. We sought to strengthen the information power by performing thematic cross-case analysis to obtain descriptions of diverse experiences and applying a theoretical framework that explained relations between aspects. Assessing these dimensions, we deemed that the overall information power was sufficient to conduct a thematic analysis in an inductive and iterative manner.
The authors participated in the four-step process of systematic text condensation, subjected to both datasets [20]. We read the transcripts to (1) identify preliminary themes; the first author then continued the decontextualisation process by (2) identifying and sorting meaning units to the established themes, negotiated to code groups. Further, (3) meaning units were abstracted systematically into agreed upon subgroups and the content reduced to a ‘condensate’, which is an artificial quotation containing the original terminology used by the participants. The final step (4) of recontextualisation entailed synthesising the contents of condensates and quotes from each subgroup, developing an analytical text. Coding and organising text elements was done manually for the individual interviews, while for the focus group we used Nvivo 14 (Lumivero). Each analytical step was discussed thoroughly within the team, negotiating code groups and establishing subgroups, consciously striving to bracket our preconceptions. The iterative process of de- and recontextualisation was reached upon agreement, contributing to consistency across manual and software-assisted coding process. We applied PPCT as a framework for discussing and interpreting our findings [10].
The study was conducted following the principles of the Helsinki Declaration and was approved by the Regional Committee for Medical and Health Research Ethics South-East B, Norway (2015/1561). All participants gave informed written and verbal consent to participate.
Findings
All professionals hoped to centre their efforts towards the child’s best interests in identifying and attending to the needs of this group of CYP. Yet, they faced barriers on multiple levels, leading to perceptions of counteraction and lack of progress in caring for them.
Barriers challenging identification
Through their direct interaction with CYP and their families, the professionals described ambiguities in identifying adversities and that time was expended to uncover them. In the educational setting, CSHNs and teachers mentioned unspecific signs in CYP such as attention deficits, absence from school and aggressive behaviour, while other children were silent and easy to overlook. Lack of parental follow-up, such as parents delivering or picking children up too late, raised awareness.
‘. . . some parents just don’t step up like others do. . . . There’s always excuses . . . and that puzzles me . . . makes me think that something’s just not right, because one ought to put children first.’ (Teacher)
More tangible signs were present, though still unspecific to PSU, such as bruising, no lunch-pack and poor clothing, possibly indicating neglect. Teachers stated that it was still difficult for CYP to talk about their home conditions, as they felt loyal, protective and embarrassed, or feared being reported to the CWS. This limited teachers’ insight into the reasons for CYP’s behaviour: was it violence, substance use or just ordinary matters? Eric (21 years) reflected: ‘Nobody would notice . . . I acted as a normal kid in school. . . . I left my problems back home and had my time off when I was in school . . . I somehow knew inside that . . . if I brought my troubles along to school many eyes would suddenly open. You know, it was out of the question having to move out from home.’
Professionals specifically mentioned challenges in identifying parental misuse of prescribed drugs and alcohol. Some adolescents described trying to find out how much their friends’ parents were drinking, questioning what was considered normal. Parents often downplayed and denied substance use, fabricated coverup stories and avoided detection by moving frequently and refusing cooperation. The CSHNs reflected upon their dual role as professionals, both providing help and being obligated to report to CWS, which may discourage parents from speaking openly with them.
Professionals experienced uncertainty and feelings of incompetency when observing signs. They feared making mistakes and being sanctioned and worried that the child would suffer and about possibly harming a good relationship. Some teachers feared and avoided direct questioning. Looking back, the adolescent participants called for more engaged and accountable grownups. Although they had previously been afraid of being identified, they still longed for an opportunity to share how they were doing, hoping someone would invite them to dare to speak: ‘I wish the teachers . . . paid more attention and maybe talked to my parents so they could’ve followed up on how I was doing. I wanted the teacher to ask me so that I could understand that I didn’t need to feel so shameful, that I was not the only one.’ (Lisa, 18 years)
Establishing good relationships with the CYP and their caregivers was crucial in identifying and tending to their needs. Teachers stated that engaging with students long-term gave them a unique opportunity to make students feel safe enough to talk openly.
‘. . .there was this girl, she had no breakfast or lunch-pack, she often came late and had unkempt clothing. After a while, we had a good relationship, and she told me she woke up by herself and that her mum . . . she slept. I thought to myself that as a first grader you’re too small to get up, dress yourself, make food and go out alone. . . .’ (primary school teacher)
Despite the teachers’ sharing their concerns about a child with colleagues, communication challenges and confidentiality restricted efficient collaboration. Being aware of their duty to report to the CWS, teachers lacked confidence in recognising and accurately interpreting the signs of parental substance use. They also described situations where the CWS had closed a reported case. In such cases, the ball would again be in their court as they observed continuous signs of the child’s poor wellbeing while lacking feedback from CWS about the outcome of the case.
Observing children not thriving, the professionals experienced frustration and powerlessness. Balancing professional distance and compassion was challenging. The professionals aimed to cooperate across services. The CSHNs emphasised teachers as being particularly important, describing mutual benefits of sharing information and concerns. Teachers found CSHNs willing to have open dialogues while maintaining confidentiality, resulting in shared responsibility. A CSHN described proactive teachers: ‘. . .they could hear a story from a child and say . . .because there’s no one who can deny a kid permission to visit the school nurse. . .: “I think you should go visit the school nurse today, ‘cause she’s here, go tell her a little bit about that.”’
Adolescents who finally chose to disclose their concerns to a trusted teacher described the collaboration and being referred to the CSHN as helpful.
‘She [CSHN] tried telling me that it wasn’t anything to be ashamed of because it didn’t have anything to do with me . . . it was him [the father] who had screwed up . . . I felt lighter . . . and less ashamed.’ (Sara 18 years)
Caring efforts
Despite challenges, the professionals gained confidence in voicing the needs of CYP by focusing on each child’s best interests. Professionals aimed to approach the families as a unit, and CSHNs offered family members community experience in support groups, validating shared stories and creating fellowship. The CSHNs especially addressed the importance of children being offered community with peers. The adolescent participants also emphasised the benefit of a peer support group.
By establishing trusting relationships, the CSHNs were able to prioritise these CYPs and offer continuous support over time. As many of them needed ongoing conversations across a lengthy period, this helped them process their thoughts and emotions while drawing on their strengths throughout their school years.
‘. . .I find the strengths they possess and try to focus on that. And I try to give them something so that they can walk out the door feeling better than when entering it.’ (CSHN)
Teachers aimed to maintain a safe and sound school environment as the children experienced chaos and stress at home. They offered emotional support, explaining this was the reason the CYP kept coming back. Additionally, they tried to teach the CYP how to care for and protect themselves and what to do when facing adversity. The adolescent participants and educational staff requested more psychoeducation about substance use, how it affects family members and how to handle it.
Discussion
A notable reluctance to disclose familial circumstances was observed among CYP and caregivers, as reported by professionals in the study, suggesting that such hesitancy may be linked to stigma and fear of negative consequences. Stigma and shame are common within families affected by PSU [3], and pose a challenge to professionals [4]. The adolescent participants expressed a fear of CWS and loyalty toward family members, and strove for normalcy. Yet, they also requested that vigilant grown-ups inquire into their situation. These paradoxical needs may reflect how PSU in a family can lead to concealment out of fear of jeopardising relationships while also creating a need for external support [3]. These findings speak to the dual role of professionals and the CWS and points to a continued need to have a family strength-based approach [21]. It also indicates friction between CYP’s conditions of proximal processes within the family (microsystem) and the interaction between family/school (mesosystem) [10]. Such conflicting interests and unclear signs may help to explain professionals’ delay in identifying and addressing PSU in families.
Parental misuse of prescribed drugs and alcohol was identified as especially difficult to handle, possibly due to the legal and social acceptance of these substances, which complicates identification and intervention. What amount of parental alcohol consumption is considered normal and acceptable likely depends on societal norms and cultural context [22]. PSU in the family is therefore also influenced by perceptions at the society level (macrosystem) [23]. However, even socially acceptable substance use can harm CYP [24].
Other qualitative studies highlight professionals’ perceived barriers to inquiring about PSU, such as fear of intruding [4], and lack of competence in recognising signs in CYP [5]. In line with Todman and McLaughlin [9], professionals in our study were concerned about damaging a good relationship. However, focusing on the child’s best interest gave them greater confidence. Navigating detachment and empathy emerged as a tension, particularly as they observed children struggle over extended periods—an emotionally taxing experience. Education professionals tend to do far more than what is expected of them [25]. Feeling stretched may increase the risks of moral stress and experiencing powerlessness [7]. Such factors may strain proximal processes and inhibit professionals’ potential to act as positive moderators [5,12]. Nevertheless, positive processes took place despite constraints. The adolescents valued conversations with teachers and CSHNs, which reduced their shame. Educational staff and CSHNs reported providing CYP with emotional support and psychoeducation, focusing on maintaining a safe school environment. Thus, by drawing on synergy within the school context, where teachers and CSHN are uniquely positioned to build trusting relationships with CYP over time, such supportive proximal processes can take place [11]. This may reduce the risk of impairments and increase these CYP’s competency and life skills.
The expressed need for opportunities for sharing peer-based experiences as well as increased understanding of PSU, are consistent with a recent review showing that peer support groups and information are helpful for CYP undergoing adversities [26]. However, as our study reveals, there is often uncertainty about the specific nature of a young person’s adversities, which may be difficult to distinguish within the complexity of overall family functioning [27]. As Fredriksen et al. discuss [28], one may question whether PSU should be viewed as an independent entity versus other adversities in the family in regard to its level of negative impact. Considering this and the stigma associated with family adversities [27], a comprehensive approach could be to align peer support groups and psychoeducational initiatives in schools with the broader concept of being next of kin to someone experiencing any type of family burden, not only PSU [29]. To ensure that PSU in the family is addressed sufficiently, the topic could be integrated into the school’s ‘life-skills’ curriculum [30], into peer support groups and into the training and resources provided to school staff. Such a multilevel approach may enhance the likelihood of addressing the adversity of PSU through positive proximal processes within schools [10].
Teachers and CSHNs highlighted challenges related to communication and confidentiality as limiting their efficiency, both at the mesosystems level and, more notably, at the exosystemic level when reporting to and cooperating with CWS. They especially felt marginalised when CWS closed cases without providing feedback, highlighting perceived barriers to accessing CWS support [6]. Thus, we question if current ways of cooperating are truly in the child’s best interest and how they impact professionals’ trust in CWS. The CWS in this study appreciated teachers’ and CSHNs’ collaboration, pointing to their unique positions to identify and assist CYP. Educational staff called specifically for more interdisciplinary collaboration at both the meso- and the exosystemic level. Our findings corroborate earlier research reporting on school personnel’s experiences with PSU in the family and related health and welfare studies, pointing to the need for support and more interdisciplinary collaboration [7,8].
The findings highlight school as a key arena for identifying and supporting CYP facing adversities and for fostering resiliency. Thus, we suggest continued commitment by stakeholders and responsible authorities to strengthening professional and collaborative competence and action within schools. As part of a national strategy, many municipalities in Norway offer peer support groups for children affected by a family member’s illness [31]. Communicating such initiatives from the practice field to schools may contribute to more CYP taking advantage of them.
Few studies have incorporated the teacher–CSHN collaboration addressing PSU in the family, and, to our knowledge, none includes the voice of the adolescent living with it. The triangulation of data in this study has enhanced our understanding of the context and phenomena of PSU in the family by providing various perspectives and insights into the micro- and meso-levels of challenges, needs, and areas to improve [32]. We acknowledge that our findings are context specific. The time lag between individual interviews and triangulation may not fully reflect current awareness and support available to this group of CYP. However, we are not aware of changes in policy or practices that has substantially influenced the process of identification and support offered this group. Despite the time gap, both phases were guided by the overarching aim to understand the experiences and needs of CYP, allowing for meaningful integration of the data. The adolescents’ experiences with peer support and psychoeducation may have improved their understanding and ability to articulate their needs compared with that of a general CYP population affected by PSU.
Conclusion
Over the past two decades, increased awareness, initiatives and legislative changes in Norway have strengthened efforts to identify, follow up and support CYP experiencing adversities. This study highlights ongoing challenges and suggests improvements in identifying and supporting CYP facing PSU in the family from the perspective of professionals and affected adolescents. The school setting offers a unique and partly untapped opportunity to identify and address the needs of these CYP. Enhancing interdisciplinary collaboration and providing greater support could benefit both CYP and the professionals who work with them.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.