
Abstract
Objective:
Investigation of men’s experience of interpersonal violence across the life-course and associations of these experiences with health conditions, assessed by use of national hospital services.
Methods and analysis:
Information on interpersonal violence exposure (child sexual abuse (CSA), non-partner physical violence (NP-PV) and intimate partner violence (IPV)) was obtained from 1054 ever-partnered men through a population-based survey, then linked with publicly funded hospital discharge information. Univariate and multivariable logistic regression was used to explore associations between men’s interpersonal violence experience and hospitalization for different health conditions.
Results:
Men who experienced any interpersonal violence were at increased odds of hospitalization for injury (adjusted odds ratio (AOR) 1.86 (95% confidence interval (CI) 1.30–2.66)) and for non-disease-specific symptoms or findings (AOR 1.89 (95% CI 1.30–2.75)). Men who experienced CSA had increased hospitalization for nervous system disorders (AOR 7.04 (95% CI 3.12–15.92)) and ear diseases (AOR 4.31 (95% CI 1.59–11.68)). Men who experienced NP-PV had increased hospitalization for injuries (AOR 1.53 (95% CI 1.12–2.08)). Men who experienced 1–2 IPV types had increased hospitalization for genitourinary diseases (AOR 1.75 (95% CI 1.03–2.97)), and those exposed to 3+ IPV types had increased hospitalization for injuries (2.64 (1.71–4.05)). Men exposed to CSA (AOR 1.99 (95% CI 1.14–3.47)) and IPV (1–2 types AOR 1.48 (95% CI 1.03–2.15), 3+ types AOR 1.80 (95% CI 1.06–3.06)) were also at increased odds of hospitalization for non-disease-specific symptoms or findings.
Conclusions:
Keywords
Key messages
What is already known on this topic:
There is a paucity of research which had explored men’s experiences of interpersonal violence and associated health effects.
What this study adds:
This study is the first to document how men’s experience of violence is associated with increased hospitalization for diseases at the population level.
Men’s experience of child sexual abuse was associated with nervous system disorders and ear diseases, while experience of non-partner physical violence was associated with hospitalization for injury, and experience of intimate partner violence had some associations with hospitalization for genitourinary conditions and injury hospitalization. Experience of any interpersonal violence was associated with hospitalization for injuries and for non-disease-specific symptoms.
How this study might affect research, policy and practice:
Findings provide new information on the health burden associated with men’s exposure to violence (particularly childhood sexual abuse) and support calls for violence prevention efforts to include men and boys as necessary public health initiatives which may help to reduce hospitalization admissions.
Introduction
Violence prevention is recognized as key to achieving sustainable development globally [1,2], and having population-based data on the scale and gender-specific consequences of violence exposure is considered a prerequisite for informing successful national violence prevention plans [3,4]. While important work has been undertaken to establish the prevalence of violence against women and girls, particularly intimate partner violence (IPV), in many cases this has precluded data collection on men’s experiences [1,5,6], yet we know that, globally, 81% of homicide victims and 90% of homicide perpetrators are men [7].
Exploration of non-lethal violence suggests that men also carry a disproportionate burden of assault-related injuries resulting in hospitalization [8,9] and evidence is emerging about mental health effects associated with violence exposure, particularly for men who have experienced violence across the lifespan and by multiple perpetrators [5,10]. However, much of the current evidence about the health consequences of men’s exposure to violence is derived from non-generalizable samples (e.g. from those already seeking healthcare or support for violence experience) [8,11,12]. Where population-based data is available, most studies rely on health outcomes identified through self-report, which may be subject to recall bias and not accurately gauge real-world health service use [13].
Men’s experience of violence differs across the life-course. As children, boys may be more likely to experience physical abuse, and less likely to experience sexual abuse [1]. Those who do experience child abuse are more likely to have serious and long-term health consequences than those without these adverse experiences [14 –16]. Men are more likely than women to experience physical violence by acquaintances and strangers and less likely to experience sexual violence by non-partners [1,5,6], although the health consequences of these experiences are seldom explored. While overall prevalence rates of IPV experienced by men can be comparable to those reported by the women, data indicates that men experience IPV with less frequency, less severity and fewer consequences (such as injury and fear) than women [6,17,18]. The severity of violence experienced may have implications for health consequences. In one study, men who reported IPV that included being slapped, pushed or shoved did not have a higher prevalence of health conditions than non-victims [19], while other studies indicate that men who experience severe IPV (including stalking) have increased risk of health consequences, such as irritable bowel syndrome, chronic pain, frequent headaches, chronic pain, difficulty sleeping, poor mental health and physical health functioning, and disability [11,19 –22]. Conclusions on the gender-specific impacts of IPV are currently limited, as little research comprehensively assesses men’s exposure to multiple types of IPV using validated and nuanced measures [5].
The present research seeks to understand men’s experience of multiple types of interpersonal violence and to investigate the associations of these experiences with health conditions, as documented through use of national hospital services. To the best of the authors’ knowledge, this is the first study internationally that combines a best practice approach for assessing violence exposure among a community-dwelling and representative sample of men with an objective assessment of national hospitalization service use.
Materials and methods
Data was drawn from the cross-sectional He Koiora Matapopore | 2019 New Zealand Family Violence Study (NZFVS). Methods have been presented elsewhere [23], but a brief overview is provided here.
Study sample
The survey was conducted between March 2017 and March 2019 in three regions (Auckland, Northland and Waikato) which together accounted for approximately 40% of the New Zealand (NZ) population and include a diverse ethnic composition. A population-based cluster sampling scheme was used to randomly select dwellings. Primary sampling units (PSUs) provided starting points for the selection of households and were based on meshblock boundaries which contain between 50 and 100 dwellings. Beginning from a randomly selected starting point in each PSU, every second and sixth house was chosen. Interviewers made up to seven visits to each selected household to identify and recruit study participants. Non-residential, aged-care and short-term residential properties were excluded. In households with more than one eligible resident, the participant was randomly selected. The names of all eligible residents were listed on an administration form in the order of oldest to youngest. The selected respondent number was identified from a random number sheet. If the selected person was available, consent was sought and an interview arranged, otherwise contact details were obtained and further attempts were made to set up an interview.
To be eligible to participate, household members needed to be aged 16 years or older, have lived in the household for at least one month, have slept in the house for four or more nights per week and be able to speak conversational English. The NZFVS included data from 2887 total participants, including men. Complete interviews took place with 1423 men, the household response rate for the survey was 78%, a response rate of 61.3% of eligible men contacted, irrespective of sexual orientation [23]. For this study, only ever-partnered men were included.
Safety and ethical considerations
Ethics and safety recommendations for research on violence were followed [24]. Interviews were conducted in privacy with no one else over the age of two years present. At the completion of the interview, interviewers provided all respondents with a list of support agencies regardless of disclosure status. Participants provided written informed consent for the interview and to link survey responses with health records. Ethics approval was granted through the University of Auckland Human Participants Ethics Committee (Reference 2015/018244).
Survey tool design
The reputable and internationally standardized World Health Organization (WHO) Multi-Country Study on violence against women (WHO-MCS) questionnaire [25] was adapted to the NZ setting and for use with men. Questions assessing child sexual abuse (CSA) experienced before the age of 15 years, non-partner physical violence (NP-PV) and non-partner sexual violence (NP-SV) (after the age of 15 years) were included, as were questions about experience of five IPV types: physical, sexual, and psychological, controlling behaviours and economic abuse experienced by any partner ever in the respondents’ lifetime. Any interpersonal violence indicates participants who recorded a ‘yes’ for at least one of the previous variables (Table I).
Derived variables and definitions used in analysis including questions from the 2019 New Zealand Family Violence Study and National Minimum Dataset (NMDS) International Classification of Diseases (ICD) chapters.
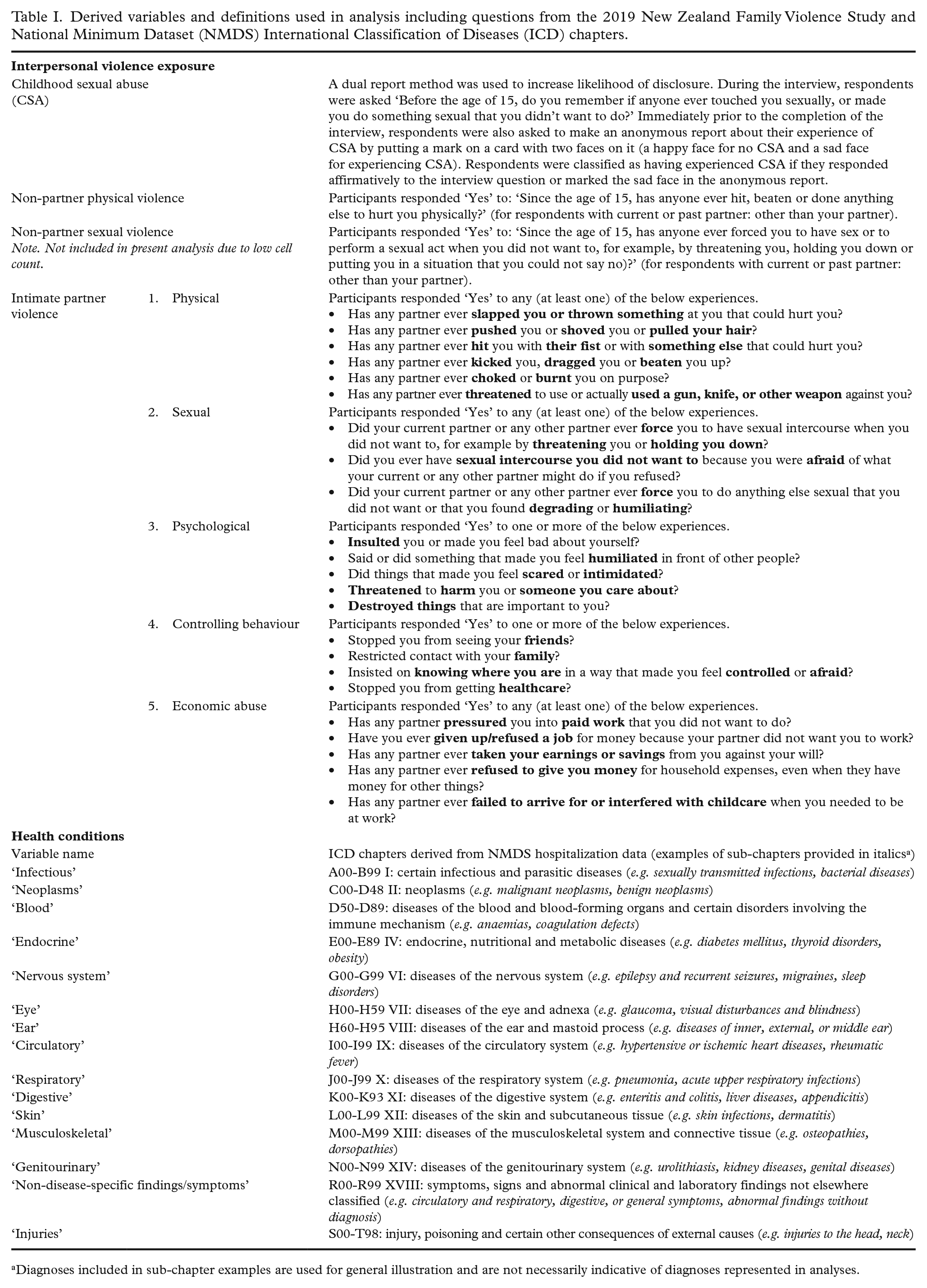
Diagnoses included in sub-chapter examples are used for general illustration and are not necessarily indicative of diagnoses represented in analyses.
National Minimum Data Set on hospital discharges (NMDS)
On behalf of survey participants who provided informed consent, information on all publicly funded hospital discharges from 1988 to 2019 was obtained from the NMDS (31-year look-back period). The NMDS is a national collection of public and private hospital discharge information, including clinical information for inpatients and day patients, administered by the NZ Ministry of Health [26]. Information on individuals’ health service usage is collected and stored by National Health Index (NHI), a unique identifier provided to all users of health and disability services in NZ [27]. The current analysis was restricted to publicly funded events (including those provided in private facilities), which account for approximately 90% of hospitalizations in NZ [28].
Since July 1999, diagnosis has been recorded using the International Classification of Diseases and Health Related Conditions, Version 10, Australian Modification (ICD-10-AM). Admissions prior to 1999 were coded using the Australian Version of The International Classification of Diseases, 9th Revision, Clinical Modification, 2nd edition (ICD-9-CM-A) and were mapped to the associated ICD-10-AM codes by the NZ Ministry of Health according to internal procedures [26].
The current investigation considered only principal diagnoses (represented by a code within the NMDS) to focus on the primary cause of hospitalization or attendance at the healthcare establishment [26], not co-existing additional diagnoses or diagnoses arising during the admission episode.
The analysis was restricted to hospital discharges with principal diagnoses from 15 ICD-10-AM chapters, for which codes and variable names are provided in Table I. Mental and behavioural disorders were excluded from the current analysis as the NMDS does not include admission to psychiatric wards.
Data linkage
Where participant consent was obtained, probabilistic data linkage was undertaken using names (first, middle and surname), date of birth and residential address to link between survey response and NHI. Only this identifying information (not the remainder of survey content) was provided to the Ministry of Health for the purposes of data linkage to obtain NHI numbers. Once obtained, NHI numbers were used to extract relevant hospital records from the NMDS. Deterministic data linkage could not be conducted, as it is not common for people to know and reliably access their NHI information.
Analysis
Analyses were conducted using Stata 13. Survey weighting functions were used to account for sampling methods (clustering by PSU and number of eligible participants per household). Descriptive analyses (weighted percentages) present an overview of the prevalence of interpersonal violence experience: CSA experience (ever/never), NP-PV (ever/never), IPV (1–2 IPV types, 3+ IPV types, compared with no IPV) and any interpersonal violence (at least one type/no interpersonal violence) in the full linked sample and by sociodemographic characteristics (Table II). Owing to low cell sizes, linked sample prevalence of men’s experience of NP-SV is reported but was not included in further analyses. Chi-square tests for co-occurrence between each interpersonal violence type are presented in Table III.
Sociodemographic characteristics and prevalence of interpersonal violence exposure for ever-partnered men with data linked to the National Minimum Dataset.
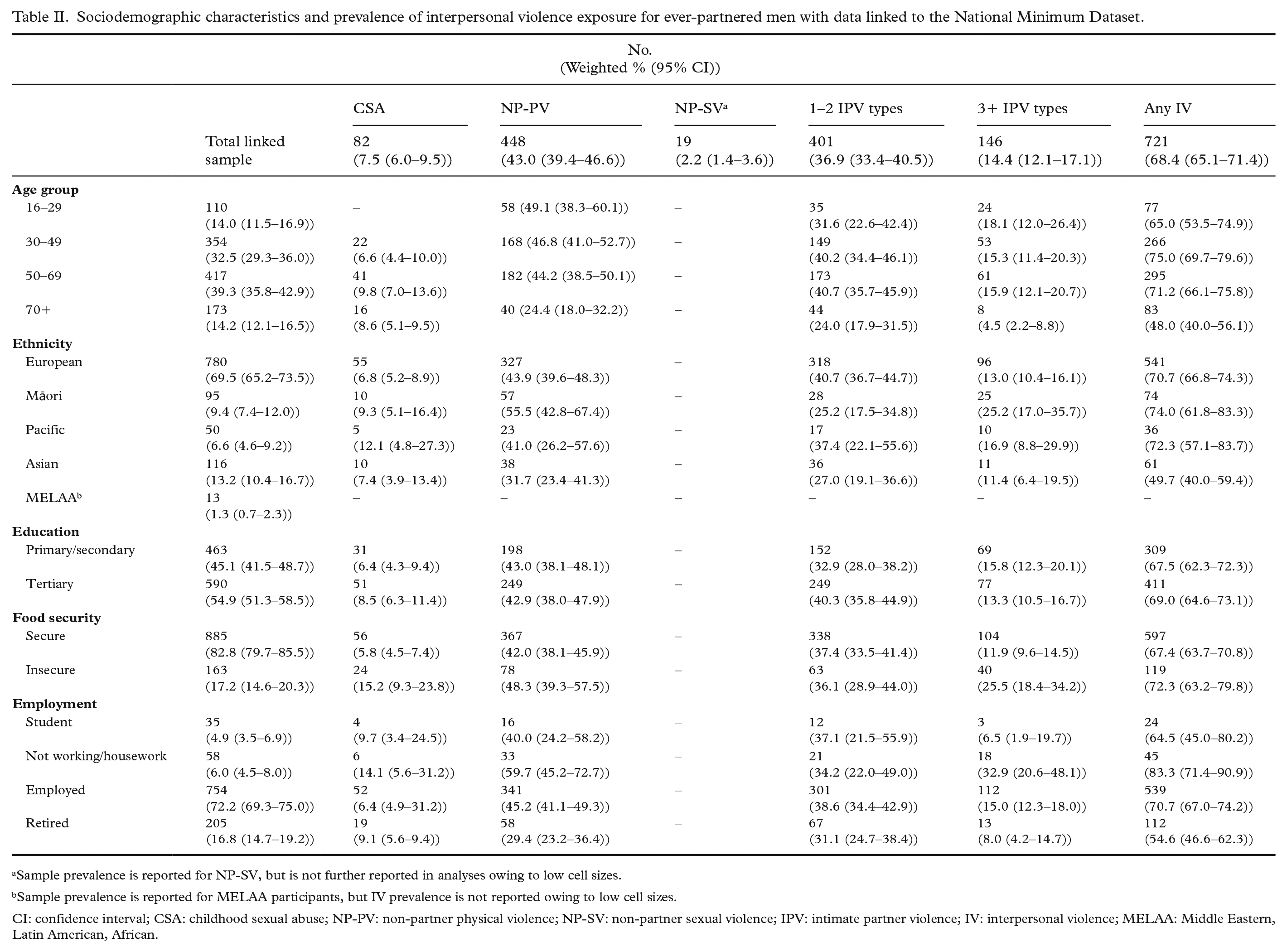
Sample prevalence is reported for NP-SV, but is not further reported in analyses owing to low cell sizes.
Sample prevalence is reported for MELAA participants, but IV prevalence is not reported owing to low cell sizes.
CI: confidence interval; CSA: childhood sexual abuse; NP-PV: non-partner physical violence; NP-SV: non-partner sexual violence; IPV: intimate partner violence; IV: interpersonal violence; MELAA: Middle Eastern, Latin American, African.
Intersecting prevalence estimates of interpersonal violence types experienced by men with data extracted from the National Minimum Dataset.
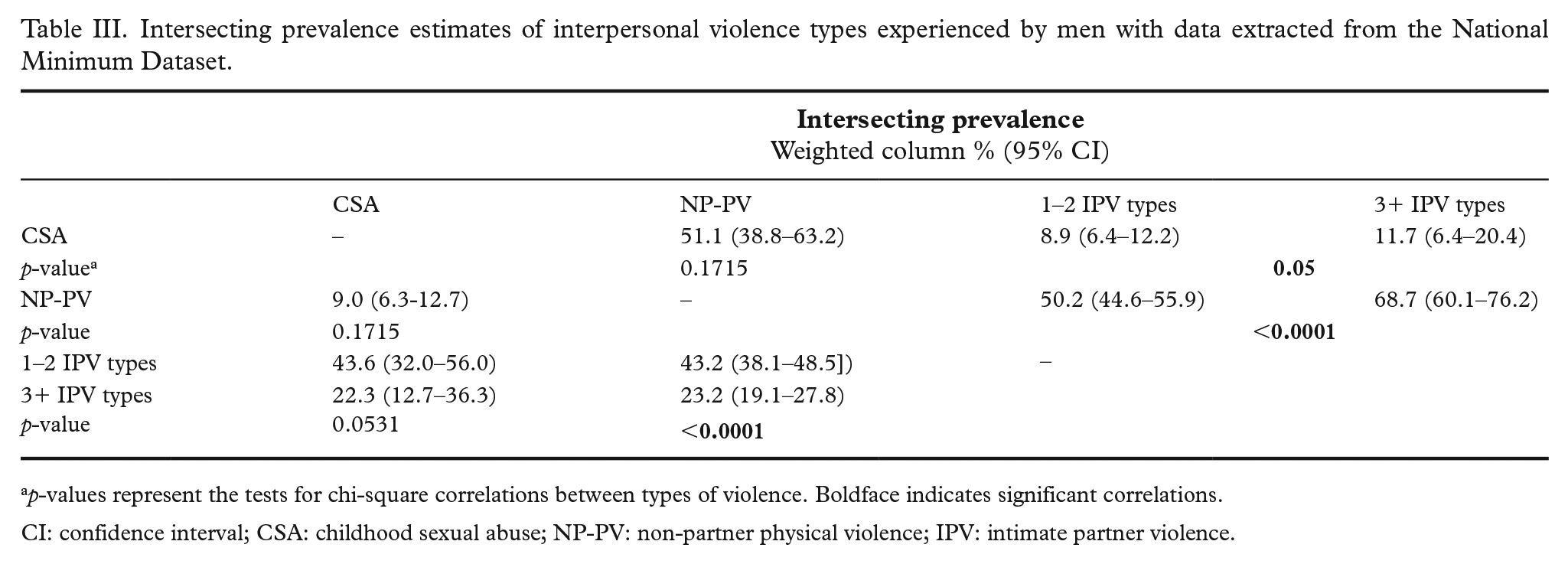
p-values represent the tests for chi-square correlations between types of violence. Boldface indicates significant correlations.
CI: confidence interval; CSA: childhood sexual abuse; NP-PV: non-partner physical violence; IPV: intimate partner violence.
Univariate logistic regression was used to determine the association between hospitalization for a range of health conditions for those who reported exposure to each interpersonal violence type (Table IV). Multivariable logistic regression was used to determine the association between each interpersonal violence type and each assessed health condition, after adjustment for age and ethnicity, given the independent association between each of these variables and a range of health conditions (Table V). Socioeconomic status was not adjusted for in order to capture the real-world impact of violence at the population level, irrespective of individuals’ socioeconomic status. This limits the potential for over-adjustment, given the marginalization of Indigenous people in NZ and other colonized societies which results in disparities in socioeconomic status, accessibility of hospital services, and health outcomes [29,30]. Where a significant relationship was identified, Bonferroni’s test was used to adjust for multiple comparisons.
Univariate associations between men’s exposure to interpersonal violence and health conditions requiring hospitalization.
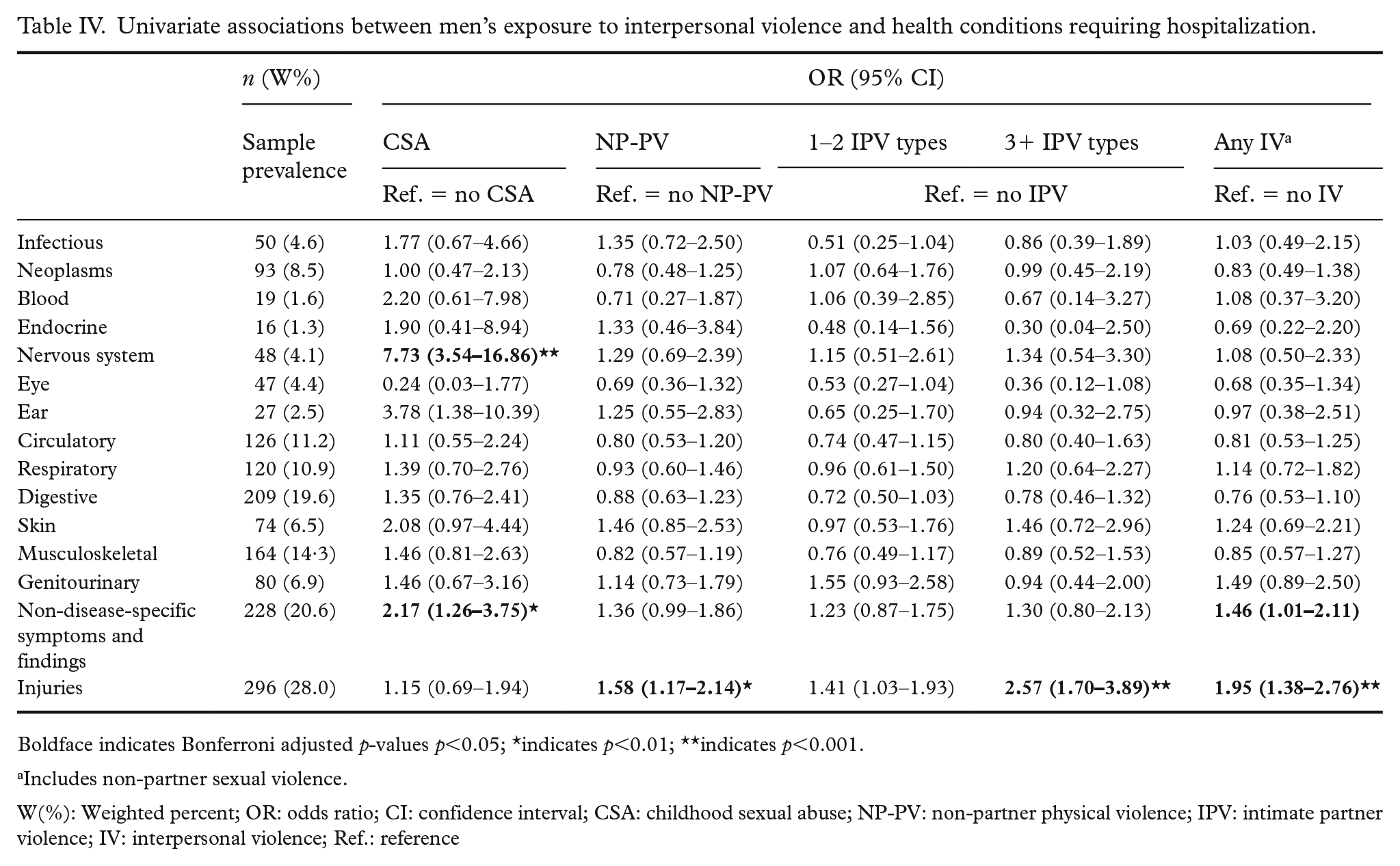
Boldface indicates Bonferroni adjusted p-values p<0.05; *indicates p<0.01; **indicates p<0.001.
Includes non-partner sexual violence.
W(%): Weighted percent; OR: odds ratio; CI: confidence interval; CSA: childhood sexual abuse; NP-PV: non-partner physical violence; IPV: intimate partner violence; IV: interpersonal violence; Ref.: reference
Associations between men’s exposure to interpersonal violence and health conditions requiring hospitalization, adjusted for age and ethnicity.
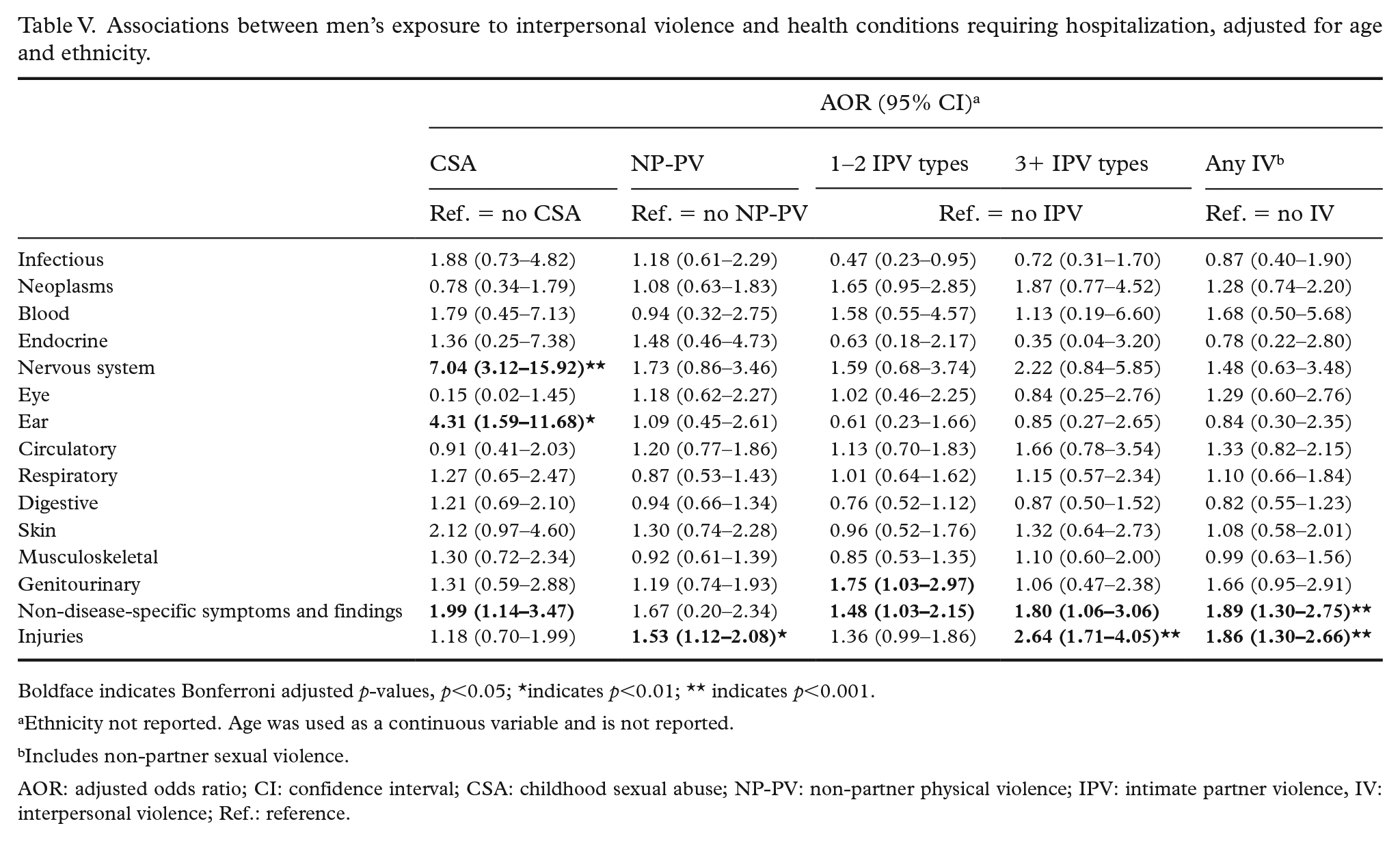
Boldface indicates Bonferroni adjusted p-values, p<0.05; *indicates p<0.01; ** indicates p<0.001.
Ethnicity not reported. Age was used as a continuous variable and is not reported.
Includes non-partner sexual violence.
AOR: adjusted odds ratio; CI: confidence interval; CSA: childhood sexual abuse; NP-PV: non-partner physical violence; IPV: intimate partner violence, IV: interpersonal violence; Ref.: reference.
Missingness issues were minor and therefore not addressed in analysis; less than 1% for all exposure and outcome variables were missing except for CSA (1.52%) and economic IPV (1.8%), where missing was driven by ‘Not applicable’, ‘Don’t know’ or ‘Refused’ responses.
Results
Of 1423 men recruited, 1316 (92.5%) agreed to their survey data being linked with the NMDS. Of these, 51 (3.9%) men had never had an intimate partner and were not included. A total of 1054 of 1256 (83.9%) ever-partnered men were able to be linked to the NMDS and were included in the current investigation.
The mean age of men was 52.2 years (SD: 16.7; range: 18–87 years). Most men were NZ European (69.5%, n=780), with 9.4% Māori (n=95), 6.6% Pacific (n=50), 13.2% Asian (n=116) and 1.3% Middle Eastern, Latin American or African (MELAA) (n=13) (Table II). For the linked cohort, 98.0% (96.8–98.8) identified as heterosexual.
Overall, 7.5% of men reported experiencing CSA, 43% reported experience of NP-PV and 2.2% of men reported experiencing NP-SV. While 48.7% of men reported no IPV experience, 36.9% reported that they had experienced one or two IPV types, and 14.4% reported experiencing 3+ IPV types. By ethnicity, Māori men presented the highest prevalence of non-partner physical violence (55.5%) and 3+ types of IPV (25.2%); NZ European men reported the highest prevalence for 1–2 IPV types (40.7%) and Pacific men reported the highest CSA prevalence (12.1%). Those who were food insecure presented greater prevalence of all interpersonal violence types compared with those who were food secure, except among those who reported 1–2 IPV types (where reported prevalence was similar irrespective of food security; Table II).
Experience of different interpersonal violence types was correlated. CSA was reported by 8.9% of those who experienced 1–2 IPV types and 11.7% of those who reported at least three IPV types (p=0.05). For men, no correlation was found between CSA and NP-PV experience. Compared with those reporting no IPV experience, experience of 1–2 and 3+ types of IPV was correlated with NP-PV (p<0.0001). This suggests that violence experiences can co-occur across the life course (Table III).
Table IV presents the unadjusted associations between interpersonal violence experience and each assessed health condition grouped by ICD chapter. Owing to the low prevalence of NP-SV (n=19), cell sizes by health conditions for this group did not have sufficient data density to produce reliable associations and are not presented in regression models. Men who experienced CSA were at almost eight-fold increased likelihood of hospitalization for nervous system disorders, almost four times as likely to have been hospitalized for ear diseases, and over twice as likely to be hospitalized for non-disease-specific symptoms or findings. Men who experienced NP-PV were more likely to have injury hospitalizations. For men who experienced 1–2 and 3+ IPV types, a stepwise association was observed for likelihood of hospitalization for injuries.
After adjusting for age and ethnicity in the multivariable model (Table V), experience of any interpersonal violence was associated with increased likelihood of hospitalization for non-disease-specific symptoms or findings (adjusted odds ratio (AOR) 1.89 (1.30–2.75)) and injuries (AOR 1.86 (1.30–2.66)). Men who experienced CSA were at increased odds of hospitalization for nervous system disorders (AOR 7.04 (3.12–15.92)), ear diseases (AOR 4.31 (1.59–11.68)) and non-disease-specific symptoms or findings (AOR 1.99 (1.14–3.47)). Men who experienced NP-PV were more likely to be hospitalized for injuries (AOR 1.53 (1.12–2.08)). Men who experienced IPV were at increased odds of hospitalization for non-disease-specific symptoms and findings (for those who experienced 1–2 IPV types: AOR 1.48 (1.03–2.15); for those who experienced 3+IPV types: AOR 1.80 (1.06–3.06)). Men who reported 1–2 IPV types also had increased odds of hospitalization for genitourinary diseases (AOR 1.75 (1.03–2.97)), while those exposed to 3+ IPV types had increased likelihood of hospitalization for injuries (AOR 2.64 (1.71–4.05)).
Discussion
Overall, our findings provide evidence that men’s exposure to interpersonal violence is associated with hospitalization for a variety of health conditions, and these associations vary by type of violence experience. To our knowledge, this is the first study globally to use a representative population-based sample to evaluate associations between men’s experiences of interpersonal violence across the life-course and hospitalization at the national level. It extends previous work by using robust best practice approaches for measuring multiple experiences of interpersonal violence exposure (child sexual abuse, physical violence by non-partners, and five types of IPV) in a population-based sample. Additionally, this study included objective measures of hospitalization service use based on routinely collected data. This is a significant methodological advance on previous work as it eliminates problems of recall bias which can be present in studies relying on self-reported data to assess health problems. The ability to capture the majority (approximately 90% of all reported hospitalizations in NZ) also adds strength to our findings [28]. Hospitalization for injury was more commonly reported by men who experienced violence as adults, including both NP-PV and IPV. Hospitalization for non-disease-specific symptoms and findings was associated with men’s experience of CSA and IPV. Men who experienced CSA were also seven times more likely to be hospitalized for nervous system disorders and over four times more likely to have hospitalizations for ear diseases. While further research is needed, our results signal important intervention and prevention opportunities that need to be implemented, underpinned by appropriate health infrastructure and clinical support [31,32].
Our results substantiate previous research, which has reported associations between men’s experience of CSA and increased risk for nervous system conditions, such as fibromyalgia [1]. The associations found are consistent with evidence that posits child abuse as a form of ‘toxic stress’ that contributes to long-term health outcomes [33]. Our study demonstrates that this relationship translates into increased service use in real world population-level hospital records.
In this study, over 40% of men reported experience of NP-PV, and this experience was associated with increased likelihood of injury hospitalization. Some of these hospitalizations might be for treatment of injuries sustained from violence, as seen in NZ, Australia and the USA [8,9,34], as well as overlap with injuries sustained through violence perpetration [35]. However, it is also possible that these injury-related hospitalizations are from other causes; other studies have reported that those who experience non-partner violence may also have an increased propensity for risk-taking and increased exposure to risky situations [36]. While acknowledging these complexities, findings from the present study show the value of considering hospitalization for an injury sustained through violence as an opportunity for providing support and intervention. Examples include multidisciplinary programmes which link patients with hospital- and community-based resources to address underlying risk factors [37], including intertwined issues of systemic and community disadvantage [9,38].
The present study substantiates and adds to knowledge about the gendered nature of violence experience and self-reported health outcomes [21,39,40], as our findings indicate that men’s interpersonal violence experience was associated with a smaller range of adverse hospital-related health outcomes compared with women who experienced interpersonal violence in our companion study [41]. These differences are likely related to the greater severity, duration and frequency of IPV experienced by women compared with men [17,42 –44]. Also of note was the increased experience of genitourinary diseases for men who experienced IPV. Previous research suggests that men who use violence are more likely to have multiple concurrent sexual partners [45], which may also suggest a pathway for this association.
Our findings also support previous research pointing to the interconnections of violence experience across the lifespan [46,47]. Men who experienced CSA were more likely to report IPV experience, while those who reported IPV experience were also more likely to report NP-PV experience. The potential long-lasting impacts of CSA have clinical implications and highlight the need to develop healing pathways for young people exposed to adverse childhood experiences, including CSA, to interrupt pathways to poor health. Trauma-informed assessment procedures should be used, as only a very small minority of men are likely to report exposure to CSA [48] and identification is a prerequisite to providing referrals to trauma recovery services [49].
Limitations
The cross-sectional nature of this investigation cannot establish the causal direction of the associations. Other limitations likely contribute to underestimation of the associations between interpersonal violence exposure and health consequences, including: a) underestimation of severe violence exposure, as we excluded those residing in facilities such as prisons, b) those who experienced the most severe violence would be been less likely to participate in the survey; and c) men may be less likely than women to disclose interpersonal violence experiences, particularly sexual interpersonal violence [1,5]. Additionally, our study did not include measures of physical violence in childhood, which has been found to contribute to life-course pathways of experiencing violence in adulthood [1]. Also, while we adjusted for age in regression analyses, there is also potential for an age effect to exist. First, younger participants would be less likely to experience many of the chronic health conditions identified. Second, older people may not recognize, or may minimize, previous violence experience, and experiences of violence that resulted in injury hospitalization may not have been captured within the 31-year look-back period available. Further, as respondents were recruited from community-dwelling individuals, with those dwelling in retirement communities or other care facilities excluded, and those who were ill less likely to have participated in the survey, respondents present in our sample were likely to be healthier, and potentially less likely to have experienced violence. These limitations mean our findings are likely to underestimate associations between violence and healthcare usage. Dichotomization of violence exposure measures and ICD chapter codes likely oversimplify nuances related to frequency, severity or chronicity of violence or number of hospitalizations and may therefore underestimate the magnitude of the relationship with health outcomes [17,50 –52].
Because of the small proportion of gay and bisexual men in this investigation it was not possible to explore the association between interpersonal violence and health outcomes for this group [5]. Studies with larger sample sizes undertaking similar analyses in future would be of benefit to confirm or extend these findings, and might enable findings related to differences between groups (e.g. ethnic-specific differences) to be more robustly explored. The role of violence perpetration and its role in cumulative violence experience, including retaliation by victims, and the association of this with hospitalized health outcomes should also be interrogated in future research [46,53].
Conclusion
The current investigation identified associations between men’s experiences of interpersonal violence and adverse health outcomes requiring hospitalization at the population level. While further research is needed to replicate our findings and to identify pathways by which associations occur, the findings presented in this investigation add to the growing literature highlighting the opportunity for healthcare to interrupt pathways of chronic violence exposure. Our findings also point to the importance of preventing violence in childhood and across the life-course as a potential means of decreasing the national burden of hospitalization and contributing to the improvement of men’s wellbeing at national levels.
Footnotes
Acknowledgements
The authors gratefully acknowledge the participants, interviewers and study project team led by Patricia Meagher-Lundberg. Dr Ladan Hashemi is acknowledged for her role in curation of the survey data, and initial sourcing of the NMDS data. Representatives from the Ministry of Justice, Accident Compensation Corporation, New Zealand Police, and Ministry of Education, who were part of the Governance Group for Family and Sexual Violence at the inception of the study, are also acknowledged. This study is based on the WHO Violence Against Women Instrument as developed for use in the WHO Multi-country Study on Women’s Health and Domestic Violence and has been adapted from the version used in Asia and the Pacific by kNOwVAWdata, version 12.03. It adheres to the WHO ethical guidelines for the conduct of violence against women research. The study funder had no involvement in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Author contributions
JLF contributed to conceptualization, funding acquisition, project administration, supervision of the study, and writing – review and editing. PJG contributed to the statistical analysis, conceptualization, funding acquisition, and writing – review and editing. BMM performed the statistical analysis, and contributed to the literature review, conceptualization, and writing – review and editing. VS contributed to conceptualization and writing-review and editing. TKDM contributed to the funding acquisition and writing – review and editing. All authors contributed to manuscript revision, read and approved the submitted version. JLF and BMM accept full responsibility for the finished work and/or the conduct of the study, had access to the data and controlled the decision to publish.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JLF reported receiving grants from the New Zealand Ministry of Justice outside the submitted work. PJG reported being employed at the Health Quality & Safety Commission and being a senior specialist for the Family Violence Death Review Committee. VS reported receiving grants from Auckland Medical Research Foundation, Health Research Council of New Zealand, National Heart Foundation of New Zealand, and New Zealand National Science Challenge (Healthier Lives) outside the submitted work. In addition to her role at the University of Auckland, TKDM is Chief Science Advisor for the Ministry of Social Development.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the New Zealand Ministry of Business, Innovation and Employment (grant number CONT-42799-HASTR-UOA).