
Abstract
Background:
Lolland-Falster Health Study (LOFUS) was a health examination survey that included self-administered questionnaires, clinical examinations, and the collection of biological samples, undertaken in 2016–2020 in a rural, socioeconomically deprived area with the lowest life expectancy in Denmark. The aim of this study was to examine the determinants of non-participation in LOFUS to evaluate the extent to which LOFUS data reflected the general population of the area.
Methods:
LOFUS invited randomly selected subjects together with their entire household. As determinants of non-participation, we analyzed age, sex, municipality of residency, citizenship, residency status, socioeconomic status, invitation type, and year of invitation. Relative risk regression was used to estimate the association between determinants and non-participation rate, mutually adjusted for other determinants.
Results:
In total, 53,313 subjects were invited of whom 18,949 (36%) participated. In the multivariable analysis, men had a 3% higher non-participation rate than women; subjects with citizenship other than Danish had a 3% higher non-participation rate than Danes. In-migrants had 6% higher non-participation than long-term residents. Compared with self-supported subjects aged 30–64, both publicly supported subjects of this age and younger and older subjects had higher non-participation rates: 16%, 16%, and 13%, respectively. Compared with self-supported, long-term residents, publicly supported in-migrants had 23% higher non-participation.
Conclusions:
Keywords
Introduction
The Nordic countries have a strong tradition of population-based health examination surveys, for instance the Västerbottom studies [1] and the HUNT study [2]. Over the past 40 years, health surveys have increased not only in numbers, but also in scope and content: from short questionnaire-based surveys to comprehensive health examination surveys including the collection of biological samples [3]. As the scope, content, and complexity of health examination surveys have increased, participation rates have tended to decrease [4 -6]. Low participation rates may imply selective participation with systematic differences between participants and non-participants [7]. When this happens, the health profiles of participants are no longer representative of the target population.
To assess representativity, determinants of participation have been investigated in several health examination surveys. Sex, age, and socioeconomic status are well-known determinants of participation with women, the middle-aged, and more highly educated persons normally having higher participation than men, younger, and less educated persons [8-10]. Moreover, participation has been associated with health status [11], trust in healthcare [12], and research altruism [13-14], indicating that a broad spectrum of factors may affect participation.
Lolland-Falster is a rural-provincial area in Den-mark with two municipalities: Lolland and Guld-borgsund. With a life expectancy of 78.8 years, the area had the lowest life expectancy in Denmark in 2018–2022 [15]. As in all of Denmark, life expectancy here was approximately 4 years lower for men than for women [16]. The Lolland-Falster Health Survey (LOFUS) was conducted between 2016 and 2020 [17]: a traditional health examination survey including self-reported questionnaires, health examinations, and the collection of biological samples. In the present study, we aimed to identify determinants of non-participation in LOFUS with the purpose of evaluating to what extent the LOFUS data reflect the entire Lolland-Falster population.
Material and methods
LOFUS: study population and recruitment
Lolland-Falster is a rural-provincial area including two main islands in the southeastern part of Denmark. The present number of inhabitants is 103,000 [15]. The aim of LOFUS was to create a database and biobank affording the opportunity to investigate cross-sectional differences and longitudinal changes in risk factors and disease burden within and between individuals, families, and households. A special focus was given to the examination of family and household patterns of poor health and the ability to cope with life challenges [17].
Lolland-Falster inhabitants were invited to LOFUS on a daily basis. Inhabitants aged ⩾18 and not pr-eviously invited were randomly selected from the updated population register (CPR) and invited together with all members of their household. Invitations were issued via e-Boks (a digital communication service between public authorities, private companies, and citizens in Denmark). The few persons exempted from use of e-Boks were invited by letter. If a person agreed to participate, he/she was sent a personal code enabling them to electronically fill out the self-administered questionnaire. Persons who could not master the electronic version filled out the questionnaire on paper. Appointments for the clinical examination could be booked via mail, phone, or text message. People not responding within 2 weeks were reinvited, and if still not responding, attempts were made during the following 2 weeks to find their telephone number via publicly available databases (118, KRAK, etc.), and to reach them by phone/SMS. As the reminder process lasted only a month, only a few persons moved out/died between the first invitation and the phone reminder.
Participants were invited subjects who signed the consent to participate and contributed to the clinical examination. Non-participants included invited subjects who declined participation, could not be reached, completed the questionnaire but not any of the clinical examination, withdrew a previously signed consent, and the few persons who had moved out of the area/died during the recruitment process. The clinical examination, including the sampling of biological specimens, took place in three clinics in the area and lasted approximately 1 h for adults and 20–45 min for children. The study population included all 53,313 subjects invited to LOFUS between February 2016 and February 2020.
The LOFUS database uses the MS SQL Server as its back-end data storage. The front-end user interface was developed in MS Access. For proper protection of the participant-related data, the Access file contains no data. The database is used for both data storage and administrative management of the project and is stored on statutory logged drives. During the data collection period, the results of same-day analyses of blood and urine and the data from completed electronic questionnaires were uploaded on a nightly basis, whereas other data were entered by the LOFUS staff. The completeness and correctness of datasets were controlled regularly. Only authorized personnel had access to the LOFUS database, and all activity was logged.
Determinants of non-participation
From the LOFUS database of invited subjects, we retrieved data on personal identification number (CPR), age, sex, citizenship, municipality of residency, year of invitation, and type of invitation/reminder.
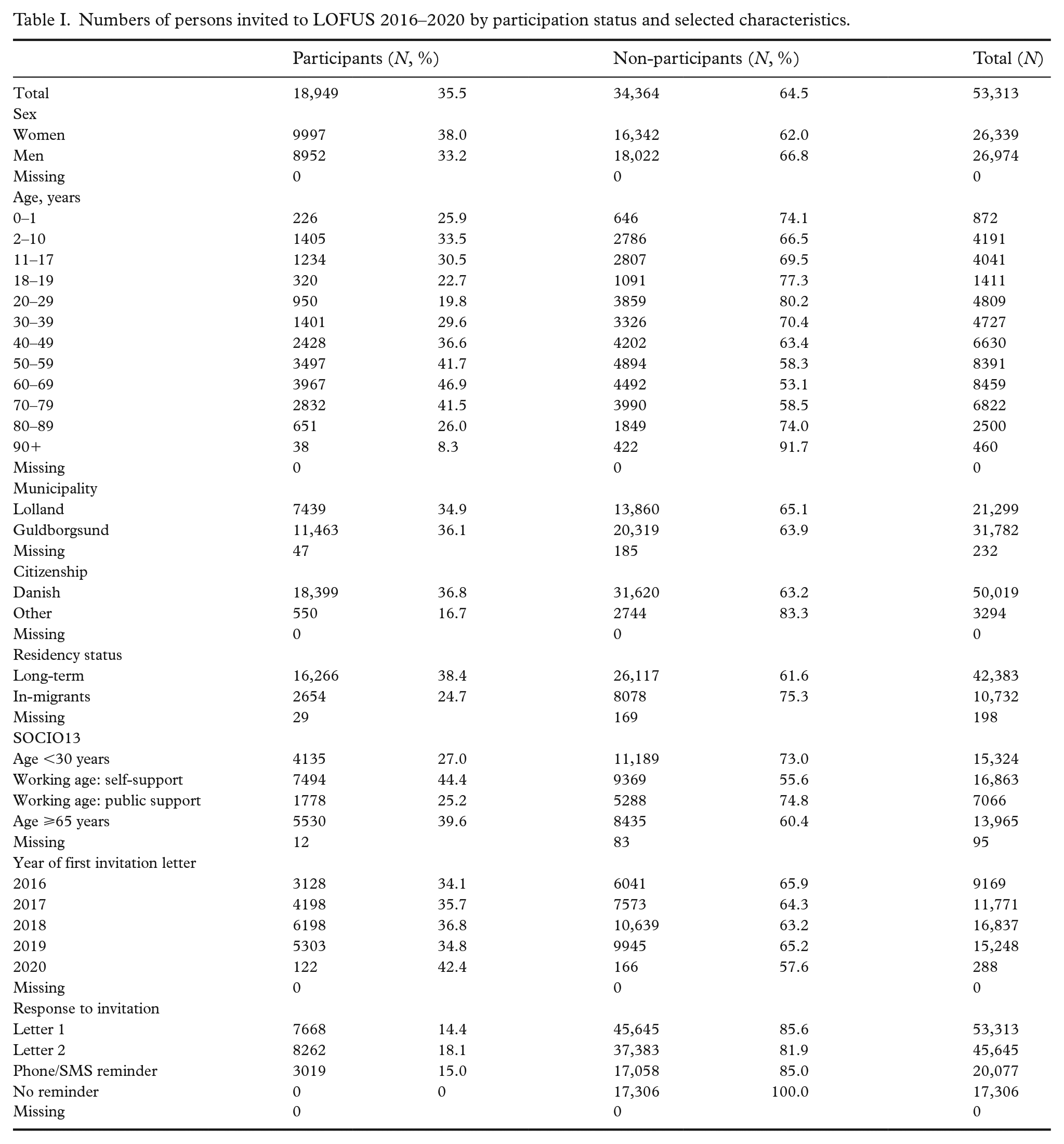
The dataset was uploaded to a research server in Statistics Denmark where it was linked with national data on residency history and socioeconomic status. Residency status was based on current and historical address data in the CPR. “Long-term residents” had lived in Lolland-Falster during at least the 10 years prior to invitation to LOFUS, and “in-migrants” did not fulfill this criterion. It should be stressed that in-migrants included almost exclusively subjects who had moved to Lolland-Falster from other places in Denmark. Socioeconomic status was retrieved from the national SOCIO13 register, reflecting the subject’s main income source during the last year [18]. For subjects of working age, determined as being between 30 and 64 years, we distinguished between “self-supported” subjects earning their own income and “publicly supported” subjects on a transfer income. Transfer income included early retirement pension, cash benefit, unemployment benefit, sick leave benefit, and a number of other categories, as the main income source in the year before invitation to LOFUS (for details see Supplementary Table 1). Invited subjects aged <30 years and ⩾65 years were not classified by socioeconomic status. Sex, age, citizenship, municipality of residence, residential history, and socioeconomic status were included in the analysis because we hypothesized these personal characteristics would affect a person’s probability of participating in LOFUS. Year of invitation and type of invitation were included in the analysis because we hypothesized these external conditions could also affect the probability of participation (see Table I for details).
Numbers of persons invited to LOFUS 2016–2020 by participation status and selected characteristics.
Statistical analysis
Age- and sex-specific participation rates were calculated by dividing the number of participants by the number of invited subjects. The few persons who moved out/died during the recruitment process were tabulated together with non-participants. To estimate the associations between the eight determinants (age, sex, municipality, citizenship, residency status, SOCIO13, year of invitation, and invitation type) and non-participation in LOFUS, relative risk regression analysis was used [19]. The analysis was done univariately and mutually adjusted and presented as relative risks (RRs) with 95% confidence intervals (CIs). To assess the RR of non-participation by combination of residency and SOCIO13 status, the adjusted RRs were multiplied. R version 4.1.3 (R Core Team, 2020) and SAS version 9.4 (SAS Institute, Cary, NC) were used for the statistical analysis.
Results
In total, 53,313 subjects were invited to LOFUS, and 18,949 participated, resulting in a participation rate of 36% (Table I). Participation after the first invitation was 14%, after the second invitation 18% responded, and for those contacted by phone/SMS it was 15% (Figure 1). Participation was higher among women (38%) than men (33%), highest at ages 60–69 (47%), and lowest at ages ⩾90 (8%) and among young adults aged 20–29 years (20%). Overall, up to the age of 80, participation was lower for men than for women: it was lowest at 16.5% for men aged 20–29 (Figure 2). Participation was higher for Danish (37%) than for non-Danish (17%) citizens; and higher in long-term residents (38%) than in in-migrants (25%). In the 30–64 age group, participation was higher in self-supported (44%) than in publicly supported subjects (25%). By year of invitation, the participation rate varied between 34% and 37%, except for the small group invited in 2020 (42%).
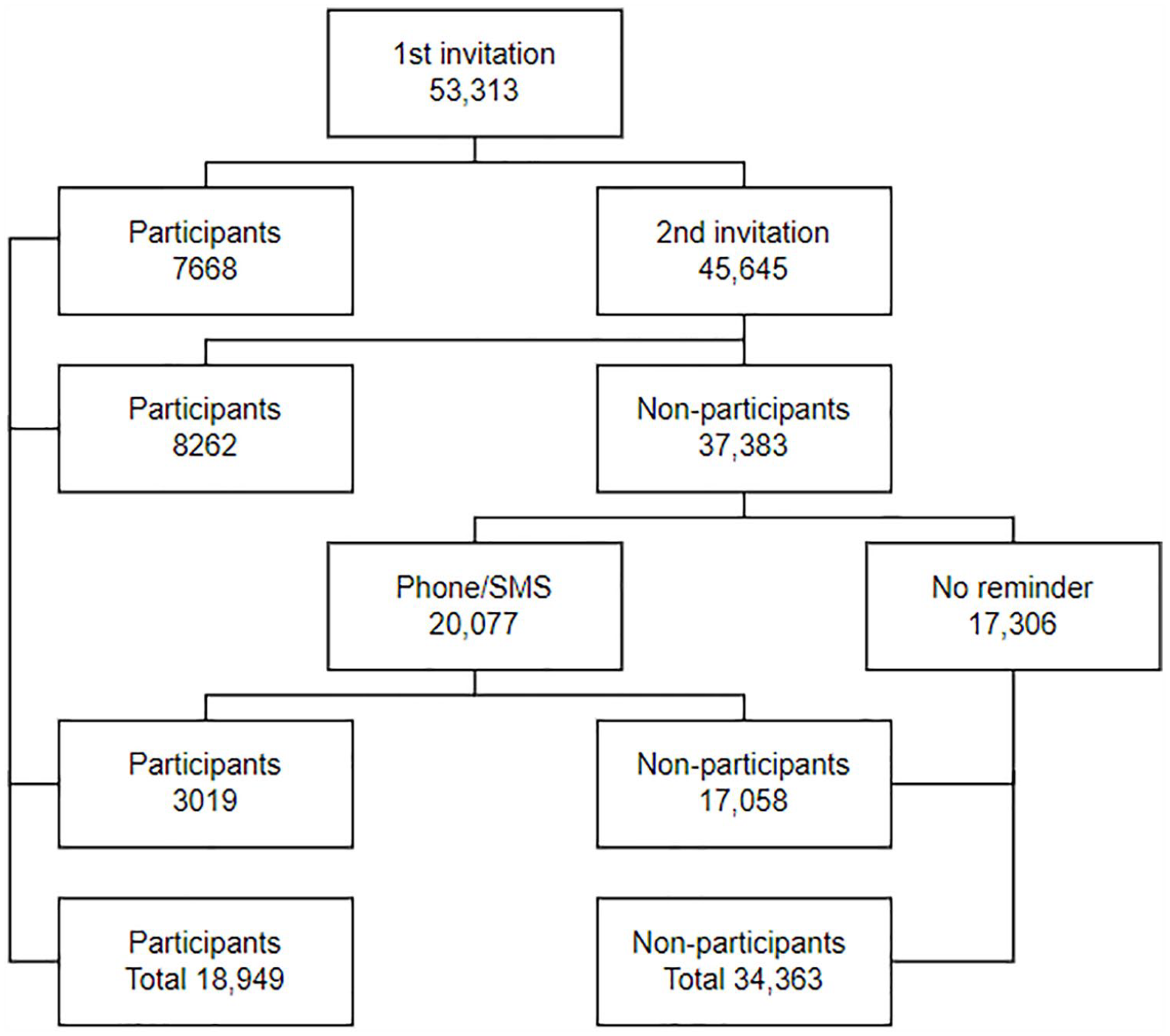
Flow diagram of participation in the Lolland-Falster Health Study (LOFUS).
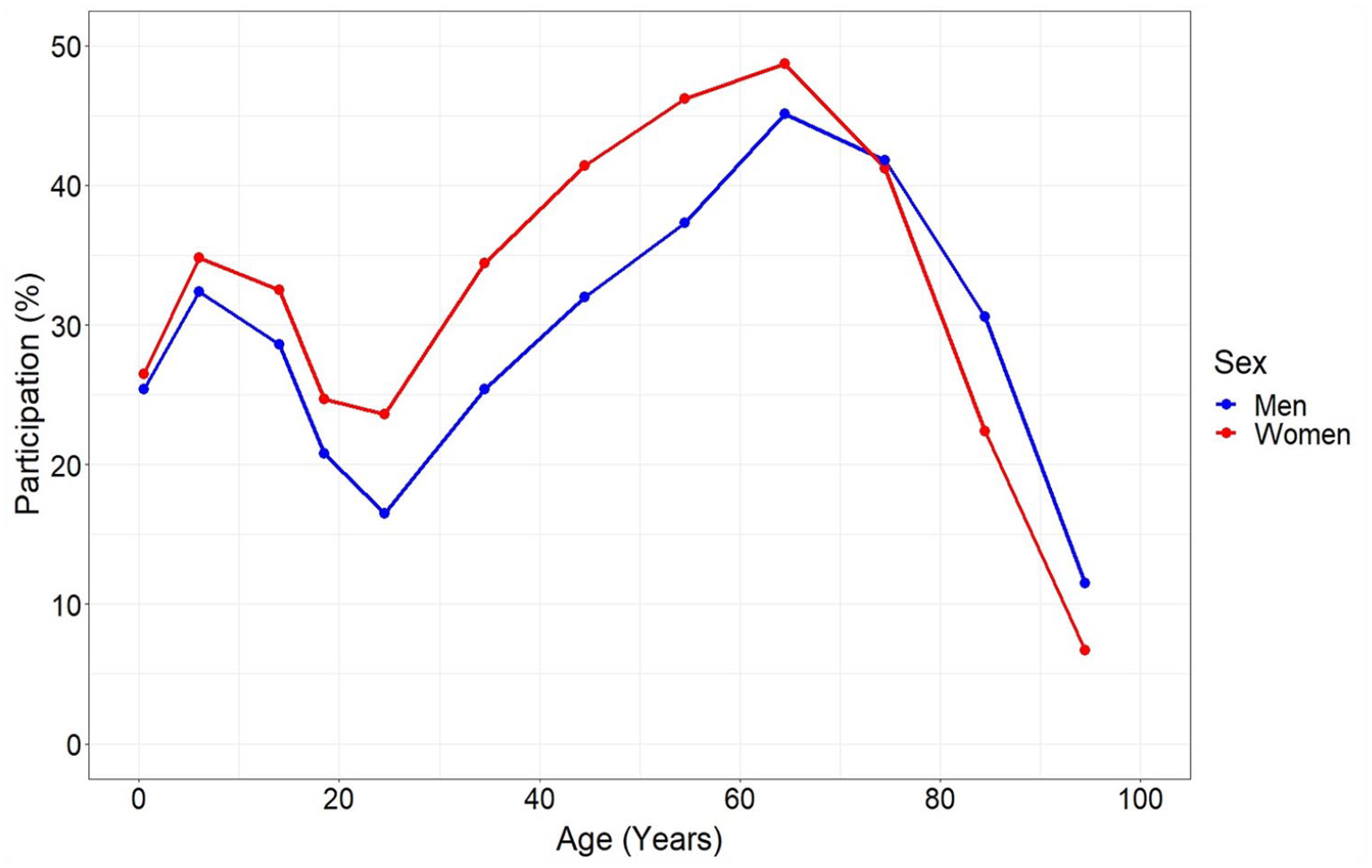
Participation rate in LOFUS by sex and age.
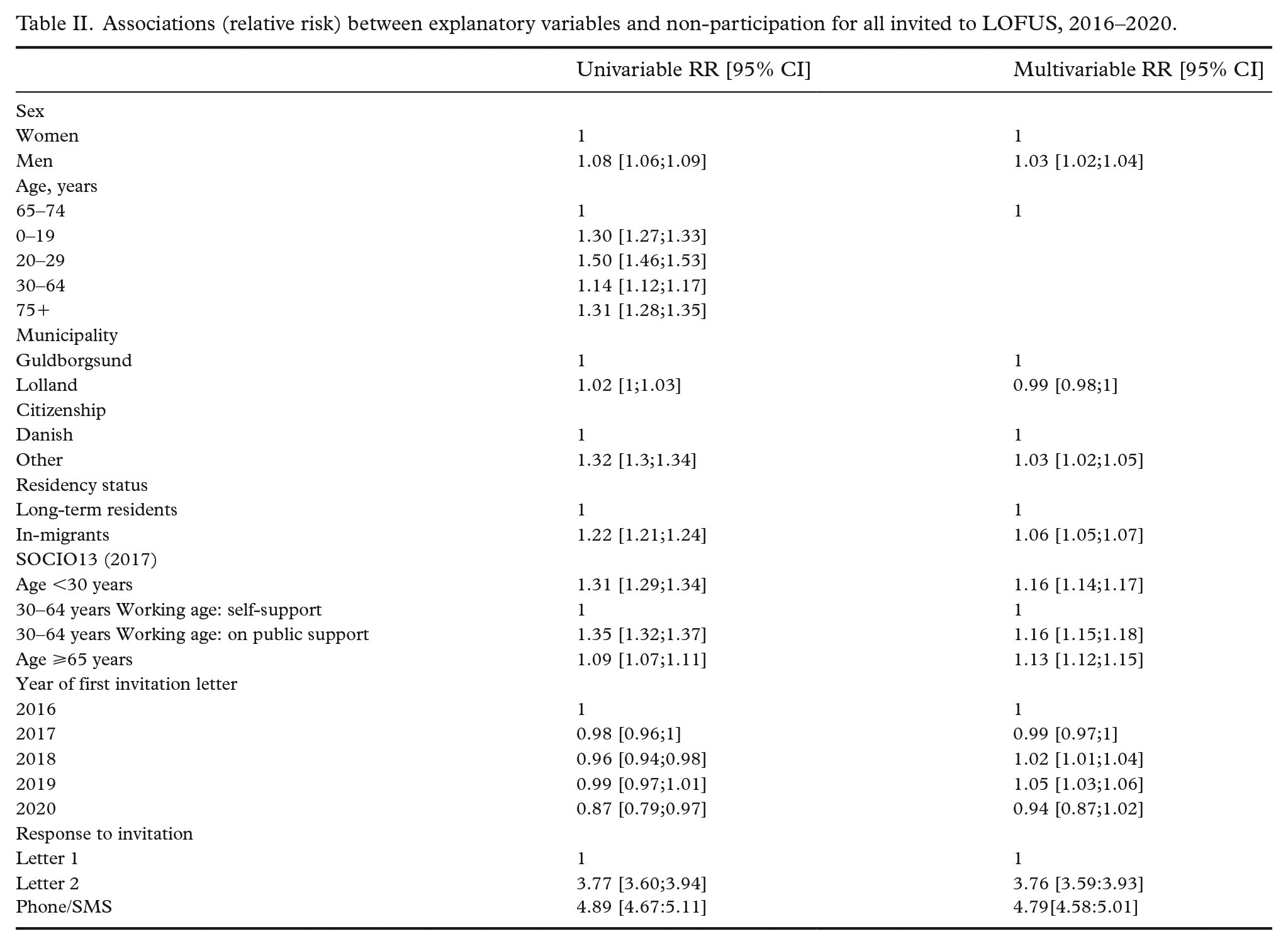
In the multivariable analysis, the non-participation rate was 3% higher for men than women (Table II). There was no significant difference in non-participation between people residing in Lolland or Guldborgsund municipalities. Non-Danish citizens had a 3% higher non-participation rate than Danish citizens, and in-migrants had a 6% higher non-participation rate than long-term residents. The non-participation rate was 5% higher among subjects invited in 2019 than among those invited in 2016. In the 30–64 age group, the non-participation rate among subjects on public support was 16% higher than among self-supported subjects.
Associations (relative risk) between explanatory variables and non-participation for all invited to LOFUS, 2016–2020.
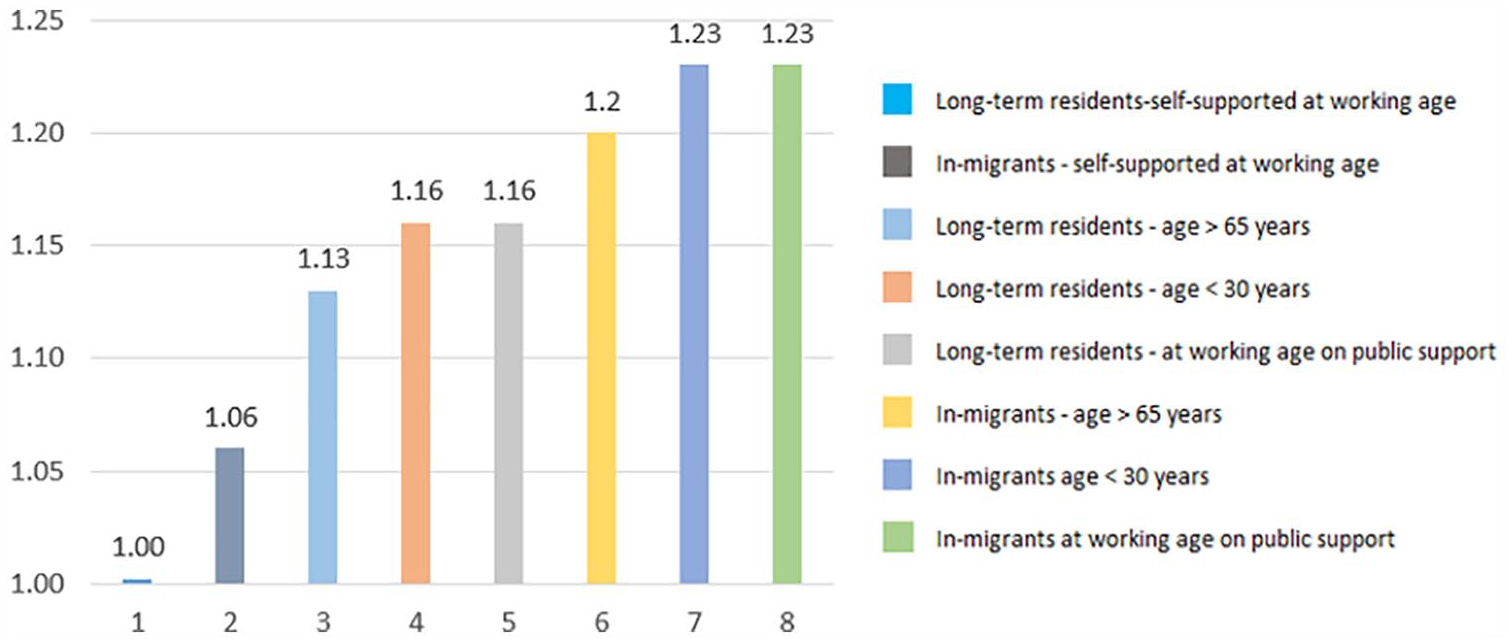
When using self-supported, long-term residents of working age as the baseline, the excess risk of non-participation was 23% for publicly supported in-migrants of working age as well as for in-migrants <30 years, and 20% for in-migrants ⩾65 years (Figure 3). For all other combinations, the subjects had excess risks of non-participation varying between 6% and 16%.
Association (RR) between the explanatory variables and non-participation in LOFUS 2016–2022.
Discussion
Main results
In Lolland-Falster, a rural-provincial area of Denmark, 36% of invited subjects participated in the population-based health survey LOFUS. The mortality rate in this area is known to be higher than that in the rest of Denmark. Publicly supported in-migrants from other parts of Denmark especially contributed to this excess mortality. Previous studies have shown that the mortality of publicly supported in-migrants to Lolland-Falster was sixfold that of self-supported long-term residents [18]. Against this background, the relatively flat gradient in non-participation in LOFUS across subjects defined by the combination of residence and socioeconomic status was noteworthy. Non-participation was 3% higher in men than in women, 6% higher in non-Danish than in Danish citizens, and 6% higher in in-migrants than in long-term residents. The non-participation rate of publicly supported in-migrants was 23% higher than that of self-supported long-term residents. This means that if these invited groups were of equal size there would be five non-participants from the former group for every four non-participants from the latter. We found this to be a relatively modest difference, implying that the heterogeneity within the Lolland-Falster population would be fairly well reflected in the LOFUS data.
Previous studies
Notwithstanding reservations about the methodological differences between studies, the overall participation rate of 36% in LOFUS was comparable with that of other recent Danish population-based health examination surveys. The Copenhagen Aging and Midlife Biobank (CAMB) had a participation rate of 31% [10]; the Diet, Cancer and Health–Next Generation (DCH-NG) had a rate of 22% [20], and the Diet, Smoking, Alcohol and Physical Activity (KRAM) survey a rate of 10% for completing the health examination [21]. Among the recent health examination surveys in Denmark, only the Danish General Suburban Population Study (GESUS) at 43% [22] had a participation rate higher than LOFUS. The Copenhagen Greater Population Study started in 2003 and is still recruiting subjects aged ⩾20 years from municipalities west and north of Copenhagen; its participation rate has been reported to be 43% [23], but no details were provided.
All these surveys took place within the last 15 years and included both men and women, yet some differences existed between LOFUS and the other surveys. LOFUS included subjects of all ages, whereas DCH-NG and KRAM focused on subjects ⩾18, GESUS on subjects ⩾20 years, and CAMB on selected subjects aged 49–61 years. Despite the inclusion of both children and the elderly—age groups known for low participation—LOFUS still had a higher participation rate than DCH-NG, KRAM, and CAMB, even when similar age groups were compared. Thus, age did not seem to explain the differences in participation rates across surveys. LOFUS included all nationalities, whereas only Danish citizens were included in GESUS. If assuming similar participation rates for non-Danish as for Danish citizen in LOFUS, the overall participation rate for LOFUS would increase by 2%, thus, approaching the GESUS rate. With the household-based invitation, LOFUS furthermore relied on parents to fill out the questionnaire and bring their children.
In addition to the digital invitation letters, LOFUS recruited people by phone/SMS. All other studies recruited only by mail or digital contact. In total, 16% of the participants in LOFUS were recruited by phone/SMS. Even when excluding phone recruitments, the participation rate in LOFUS would remain higher than those of DCH-NG, CAMB, and KRAM. Thus, even though recruitment methods can affect participation, this did not explain the differences across the surveys. The clinical examination in LOFUS took place at three locations, whereas most other surveys operated with one examination location only. KRAM used a mobile test facility but had the lowest participation rate of all surveys. Thus, accessibility did not explain the differences in participation rates.
LOFUS and GESUS—the surveys with the highest participation rates—were undertaken in provincial and rural areas, whereas DCH-NG and CAMB took place in urban areas only. KRAM collected data throughout Denmark, and the highest participation rate of 20% was found in the small rural island of Ærø, compared with rates of 8%–12% in other municipalities [24]. This indicates a higher participation rate for surveys undertaken in provincial and rural locales than in urban areas.
In LOFUS, people on public support had higher non-participation rates than self-supported people with an adjusted RR of 1.16. In DCH-NG, the odds of participation were higher for economically active than inactive people, with a gradient from the highest to the lowest socioeconomic level [20]. A similar social gradient in participation was reported for the first wave of the Diet, Cancer and Health Study [25]. GESUS did not report an association between socioeconomic status and participation [22]. Even though residency status has been found to be a factor of importance for health in Lolland-Falster [18], we found a modest association only between residency status and LOFUS participation. Non-participation of in-migrants was only 6% higher than that of long-term residents. No other surveys have reported participation by residency status. In preliminary GESUS data, 27% of participants and 28% of non-participants had comorbidity, as identified from registers. Finally, it is worth noting that both LOFUS and GESUS were local surveys aimed to improving local health issues, whereas KRAM, CAMP, and DCH-NG had a nationwide focus.
Neither study design, age, sex, nationality, recruitment method, nor accessibility seemed to explain the differences in participation rates across Danish health examination surveys, however, participation was highest in non-urban settings and in surveys with a local focus. Nevertheless, all recent Danish surveys had participation rates below 50%, in line with the generally declining participation in health surveys [3]. In all types of survey, the weighting of responses according to the population distribution is a commonly used technique to obtain representative response patterns. However, even though weighting simulates the demographic distribution of the population, the weighted response pattern may still not be representative of the population, as there is likely to be differences between participants and non-participants in their health behavior and status [26].
In Denmark, health surveys based exclusively on questionnaires have also been undertaken. The Danish Health and Morbidity Survey has been carried out on a regular basis since 1987 [27]. From 2010 onwards, it has been part of the Danish National Health Survey undertaken in 2010, 2013, 2017 [28], and most recently in 2021 [29]. The response rates in these questionnaire-based surveys have been higher, for instance 56.7% in the latest Danish National Health Survey, thus considerably higher than the response rates in the health examination surveys.
Strengths and limitations
A strength in the present study was the random selection of subjects via the CPR allowing linkage with data on residential history and socioeconomic status. These data were of high quality, as correct data on residence status in Denmark are essential for administrative purposes, and the SOCIO13 data were validated by Statistics Denmark before being released for research purposes.
As an indicator of socioeconomic position, we distinguished between self-supported and publicly supported persons instead of the typically used highest attained level of education. The reason being that level of education does not differentiate well in the Lolland-Falster population where few people, especially in middle and older age groups, have completed secondary/tertiary education. Furthermore, level of education and income did not correlate well, for instance, although self-employed craftsmen had a lower education level than schoolteachers, they had a considerably higher disposable income. Unfortunately, we were not able to partial out people who moved away or died during the recruitment process from the non-participants, however, the numbers of such cases were expected to be small given that the recruitment process lasted only 1 month. For logistic reasons we were not able to link LOFUS data with register data on the use of health services, and unfortunately, data on marital status had originally been collected for participants only.
In survey data, both odds ratio (OR) and RR can be used as measures of association, however, when an outcome is common among the studied population, as is the case with participation/non-participation, an OR tends to overestimate the size of the association [30]. The use of RR as the measure of association was therefore a strength of the study, and the RRs were easier to interpret than ORs would have been.
Public health implications
With the declining tendency for participation in health examination surveys, revealing the underlying reasons for non-participation is an issue that researchers need to address. Many studies like LOFUS, with linkages to national register data, have been undertaken to uncover the determinants of participation. Age, sex, and socioeconomic status have consistently been identified as key determinants. Several attempts have been made to facilitate the participation of young adults and the oldest age groups, men, and lower socioeconomic groups. These attempts have included tailored recruitment, such as recruitment by phone/SMS, email, websites, information helplines, online questionnaires, mobile test facilities, and flexible opening hours at test facilities. However, no recent survey has succeeded in recruiting at least half of the invited subjects. If health examination surveys are to continue to play a significant role in future health research, it will be important to explore the personal and/or psychosocial factors that make participation in health examination surveys meaningful.
Conclusions
A decline in participation rates has been observed in health examination surveys over recent decades, and previous studies have reported a social gradient in participation. Nevertheless, LOFUS, a survey from a rural-provincial, deprived area of Denmark, was able to achieve a reasonably good participation rate compared with rates from surveys in urban, economically privileged areas. Furthermore, surprisingly small differences were seen in non-participation across sociodemographic groups. The LOFUS experience could indicate that dedicated, local health examination surveys may have the best chance of mobilizing potential participants.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948231206879 – Supplemental material for Non-participation in a health examination survey in a rural-provincial area of Denmark – results from the Lolland-Falster Health Study (LOFUS)
Supplemental material, sj-docx-1-sjp-10.1177_14034948231206879 for Non-participation in a health examination survey in a rural-provincial area of Denmark – results from the Lolland-Falster Health Study (LOFUS) by SIGNE LYNGSØE, SØREN LOPHAVEN, RANDI JEPSEN, THERESE HOLMAGER, ASTRID JANSSENS and ELSEBETH LYNGE in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
The Lolland-Falster Health Study (LOFUS), Nyk-øbing Falster Hospital, Denmark, is a collaboration between Region Zealand, Nykøbing Falster Hospital, and Lolland and Guldborgsund Municipalities. The authors are grateful to LOFUS for making the LOFUS research data available. However, LOFUS bear no responsibility for the analysis or the interpretation conducted within this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Nykøbing Falster Hospital, core budget
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.