
Abstract
Aims:
Existing research on relationships provides strong evidence of couple similarity on a wide range of variables including physical attributes, abilities, and attitudes. However, couple similarity with respect to disability has not been researched. This study investigated couple similarity with respect to both physical and mental disabilities, as well as associations with life satisfaction, among adult cohabiting couples in Denmark.
Methods:
The study analysed data on self-reported mental and physical disabilities from a national survey involving 18,957 participants aged 16 to 65 years.
Results:
The results showed that participants with a disability were more likely to have a partner with a disability. Further, results showed similarity by type and severity of disability as well as age of onset of disability. Having a partner with a disability was found to be associated with low life satisfaction among men with a disability. Results also showed an association among men with a disability between low life satisfaction and the onset of their disability after (as opposed to before) the start of their relationship. These associations were not found among women with a disability.
Conclusions:
Introduction
The tendency to associate with others who are similar to oneself [1] plays out in intimate relationships: research on couples and spousal relationships provides strong evidence for similarity rather than complementarity or difference [2, 3]. Studies have found that couples tend to share physical characteristics, personality traits, cognitive abilities, levels of psychological wellbeing, and religious and political affiliations and attitudes [2, 4–6]. The evidence suggests that these findings are explained by ‘active assortment’ or preference for similarity rather than by other dynamics such as convergence over time [5, 7, 8].
A straightforward explanation for couple similarity is that sharing the same sociodemographic, behavioural and other characteristics makes it more likely that people who are similar will meet and establish a connection. In short, similarity breeds connection, as the established principle of homophily propounds [1]. The effect of proximity is part of this explanation: a now classic study by Festinger et al. [9] found that students at a university dormitory were more likely to establish friendships with those living in the same building (and even more likely with those living in neighbouring rooms) than with those living in a different building. Another way of understanding couple similarity is that we are attracted to people who are similar to us because they make us feel better: they are more likely to give positive feedback on our interests, attitudes and so on, and thereby to support feelings of positive self-esteem [10]. In line with this, some research has shown that couple similarity is associated with higher levels of subjective satisfaction and satisfaction with the relationship [11, 12], although other studies have found that marital satisfaction is not related to spousal similarity [2].
Almost no research exists on couple similarity with respect to disability, or on life outcomes such as life satisfaction in relation to disability and relationships. This is a surprising gap, given that disability is known to have profound social and psychological implications for both the individual with a disability and their partner. For example, physical disability is known to have sexual and social effects for the individual, with consequences for their relationship [13]. Living with a disability also requires adaptation and reciprocity in relationships and, if severe, may entail significant dependency on partners. It may be conjectured that the life satisfaction of an individual with a disability is impacted by whether or not their partner has a disability: there may be a benefit in mutuality and shared understanding, but equally there may be a benefit in having the support of a non-disabled partner. Similarly, in terms of partner choice, it could be conjectured that people with similar disability are likely to meet and be drawn together because of perceived mutual understanding and anticipation of needs; on the other hand, it may be that individuals with a disability are more likely to prefer a partner without a disability in order to be better supported [13]. Cultural gender norms for partner preference and couple dynamics (e.g. in terms of providing care or showing self-reliance) [14–16] may also play a particular role with respect to disability. There may therefore be gender differences in terms of life outcomes such as life satisfaction.
The aim of the research here was to investigate by way of a questionnaire study factors of similarity as well as life satisfaction among couples in cohabiting relationships in which disability was present. Through its exploration of the significance of relationships for disabled people’s lives and wellbeing, this research not only adds to the literature on couple similarity but is also of public health import. The research questions were: (a) Are individuals with a disability more likely to have a partner with a disability than those without a disability?; (b) In couples in whom both partners have a disability, to what degree do they share the type of disability, severity of disability, and age of onset of disability?; and (c) For individuals with a disability, is having a partner with a disability associated with higher or lower levels of life satisfaction?
Methods
Participants
Data were drawn from the Survey of Health, Impairment, and Living Conditions in Denmark in 2012/2013, undertaken by the Danish National Centre for Social Research [17]. The survey was conducted among a random selection of 32,810 citizens aged 16 to 65 years by way of personal identification numbers from Statistics Denmark. Selectees were sent a letter inviting them to complete a questionnaire online or participate in a phone interview. Of the selectees, 18,957 (57.8%) responded, with 15,292 (81%) completing the questionnaire online and 3665 (19%) participating in a phone interview. Informed consent was obtained from all participants.
Measurements
Physical and mental disability
Different self-reported measures of physical and mental disability drawn from the existing survey were included [17]. Participants were asked if they had ‘a long-term physical health problem or disability’ and/or ‘one or more mental disorders’ (1 = yes, 2 = no). If the response was yes, they were asked to specify the type of their most serious disability or disorder. The categories of physical disability were: problems with arms or hands, legs or feet, back; low vision or blindness; deafness, hearing loss, speech problems; skin disorder, allergy, problems breathing; blood circulation issues; problems with stomach, liver, kidneys; diabetes; epilepsy; intellectual impairment; cerebral palsy; dyslexia; chronic progressive disorder including cancer or sclerosis; and ‘other’ physical disability. The categories for mental disorders were: mental disorders related to alcohol or drug abuse; schizophrenia or psychosis; depression or bipolar disorders; stress or anxiety disorders; personality disorders; autism spectrum disorders; attention deficit disorders; eating disorders; and ‘other’ mental disorder. Participants were asked the age of onset of their disability. Further to these items, a self-reported evaluation of the severity of disability was included in the study: the participants were asked if their most serious disability or disorder was ‘minor’ (1) or ‘major’ (2). Henceforth, this study refers to physical and mental disabilities rather than disorders.
Other similarity variables
A few further similarity variables were included for comparison: self-reported body height (centimetres), weight (kilos), and level of educational attainment (ordinal scale, 1 = no further education to 8 = 5 years or more of higher education).
Relationships
Participants were asked if they were in a cohabiting relationship (with a spouse, partner, girlfriend or boyfriend) and how many years they had been living together. Participants were asked the same questions as above about physical and mental disability for their partner (1 = disability, 2 = no disability). The onset of the participant’s disability either after (1) or before (2) the start of the relationship was calculated from the participant’s age, age of onset of disability, and years living together with their partner.
Life satisfaction
The following question about life satisfaction from the World Values Survey [18] was included: ‘All things considered, how satisfied are you with your life as a whole these days?’. Participants responded on a five-point Likert scale ranging from very satisfied (1) to very dissatisfied (5).
Analytical procedure
First, frequency and correlation analyses were carried out. Second, logistic regression models, separated by gender, were built. The first logistic regression model was as follows: the dependent variable was the physical disability status (with or without physical disability) of the partner; and the independent variables were the disability status (with or without disability) of the participant, age, and level of education. The second logistic regression model was as follows: the dependent variable was the mental disability status (with or without mental disability) of the partner; and the independent variables were the disability status (with or without disability) of the participant, age, and level of education. The third logistic regression model was as follows: the dependent variable was the life satisfaction (high or low) of the participant with a disability; and the independent variables were the disability status (with or without disability) of the partner, age, and level of education. The fourth logistic regression model was as follows: the dependent variable was the life satisfaction (high or low) of the participant with a disability; and the independent variables were the onset of the participant’s disability (before or after the start of their relationship), age, and level of education. Cases with missing data were excluded from the analysis. The level of significance was 0.05. SPSS version 20 was used.
Results
Of the 18,019 participants, 4519 reported a physical disability and 1398 reported a mental disability (see Table I for details).
Frequencies of participants and partners without a disability, with a physical disability, and with a mental disability, respectively.
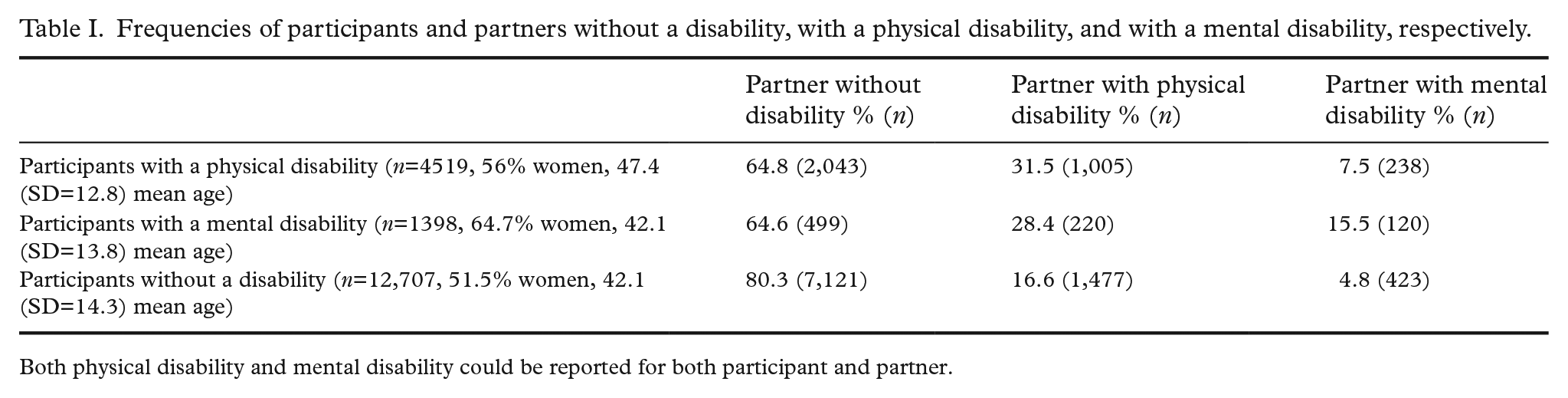
Both physical disability and mental disability could be reported for both participant and partner.
Similarity and disability
Table I shows frequencies for having a partner without a disability, with a physical disability, and with a mental disability. The results show that just over a third of participants with a disability (35.2% of those with a physical disability and 35.4% of those with a mental disability) had a partner with a disability. In comparison, one in five participants without a disability had a partner with a disability. Among participants with a physical disability, 31.5% had a partner who also had a physical disability, compared with 16.6% of participants without a disability. Among participants with a mental disability, 15.5% had a partner with a mental disability, compared with 4.8% of participants without a disability.
Table II shows correlations between participants and their partners with respect to sharing a physical or mental disability, severity of the disability (minor or major), and age of onset of the disability. All correlations were significant with correlation coefficients between 0.108 and 0.552. The correlations between participants and partners sharing a disability were 0.158 for physical disability and 0.108 for mental disability. Correlations for severity of physical and mental disability were 0.218 and 0.217, respectively. For age of onset of disability, the correlation was 0.392 for couples with physical disabilities and 0.552 for couples with mental disabilities.
Correlations between participants and partners with regard to sharing physical disability, mental disability, severity of disability, and age at onset of disability, respectively.

Spearman’s correlation coefficients: *P<0.05; **P<0.01.
In order to compare with non-disability similarity variables, correlations for height, weight, and level of educational attainment were also calculated. Among all participants, correlations for height, weight, and level of educational attainment were 0.094 (P<0.001), 0.194 (P<0.001) and 0.523 (P<0.001).
Table III shows the frequencies for participants and partners with the same physical or mental disability. Among those with physical disabilities, 29.9% shared type of physical disability. Of these, the highest frequencies were for back problems, deafness, allergy and ‘other’. Among those with mental disabilities, 64.1% reported having the same type of mental disability. Of these, the highest frequencies were for depression or bipolar disorder, autism spectrum disorder, stress or anxiety disorders, and ‘other’.
Frequencies and associations of types of physical and mental disabilities of participants and partners.
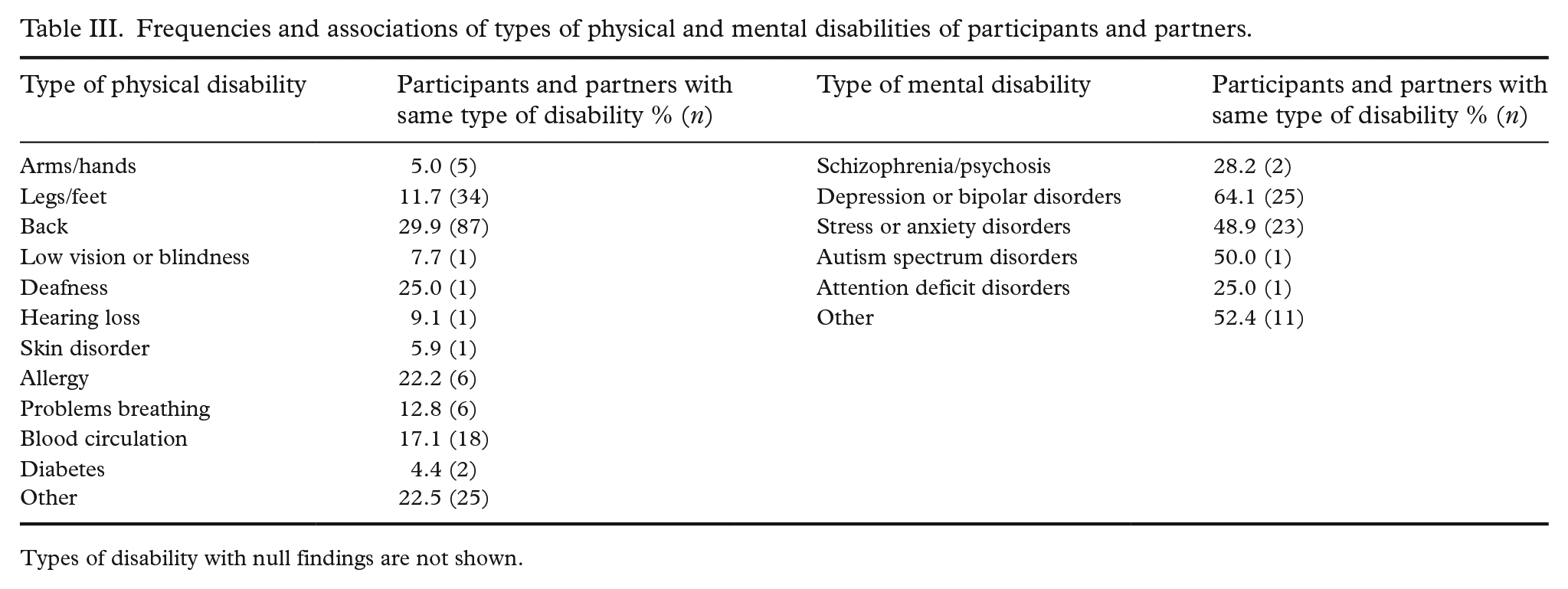
Types of disability with null findings are not shown.
Tables IV and V show logistic regression models, separated by gender, of variables associated with participants having a partner with or without physical and mental disability, respectively. The participant’s own disability was associated with having a partner with a disability in all models. Further, for both male and female participants, higher age and lower levels of education were associated with having a partner with a physical disability. Having a partner with a mental disability was associated with lower levels of education for both male and female participants and with younger age for male participants.
Logistic regression models, separated by gender, with partner’s physical disability as dependent variable and participant’s disability as independent variable.
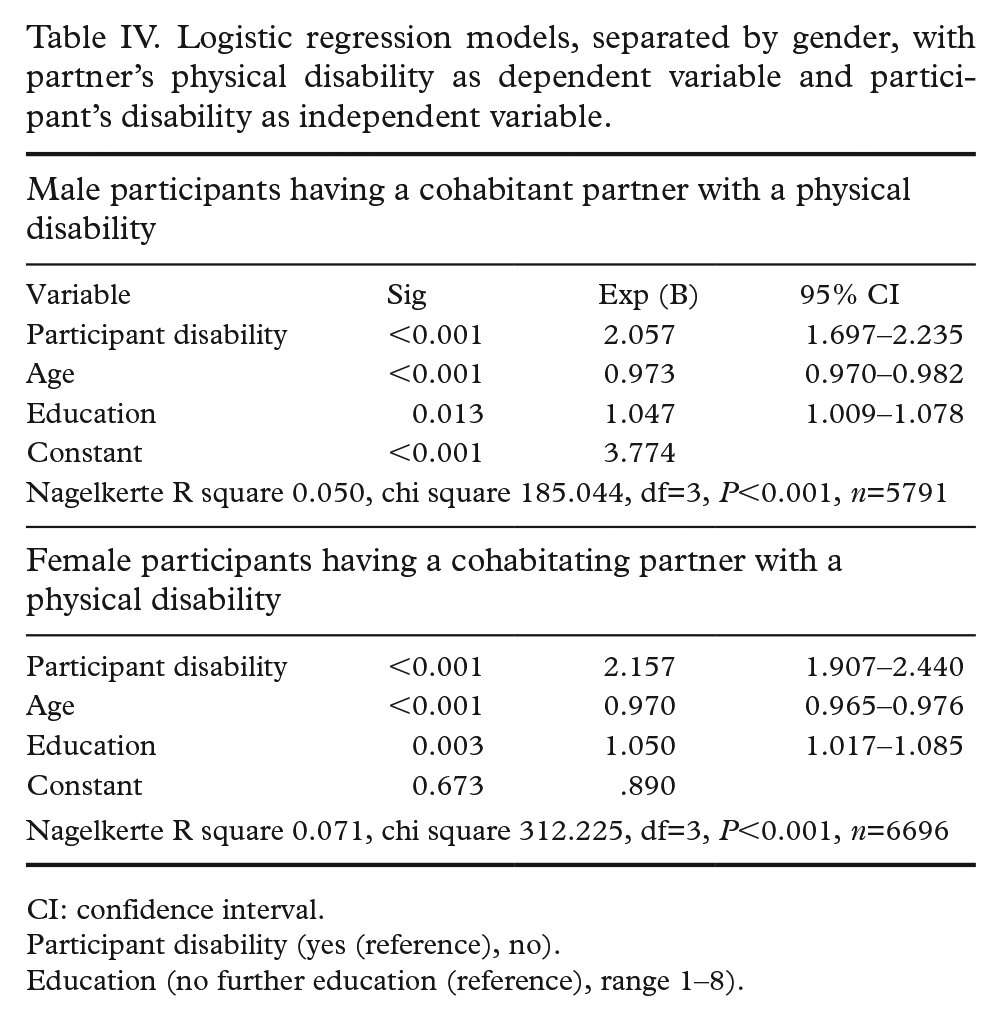
CI: confidence interval.
Participant disability (yes (reference), no).
Education (no further education (reference), range 1–8).
Logistic regression models, separated by gender, with partner’s mental disability as dependent variable and participant’s disability as independent variable.
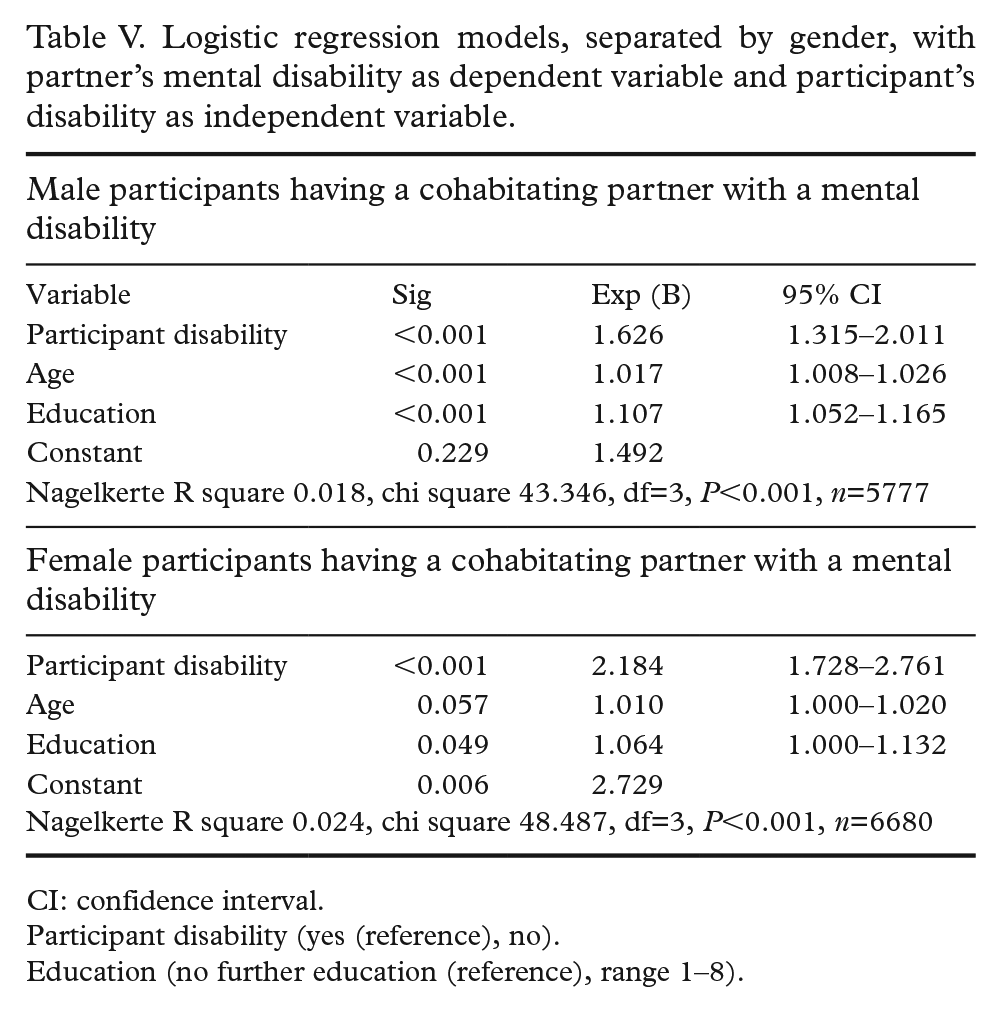
CI: confidence interval.
Participant disability (yes (reference), no).
Education (no further education (reference), range 1–8).
Life satisfaction
Associations for life satisfaction (high or low) among participants with a disability were investigated through logistic regression models. As shown in Table VI, having a partner with a disability was associated with low life satisfaction for male but not female participants with a disability. Further, for female participants with a disability, younger age and lower levels of education were associated with a low level of life satisfaction, but these associations were not significant for male participants with a disability.
Logistic regression models, separated by gender, with life satisfaction of participant with a disability as dependent variable and partner’s disability as independent variable.
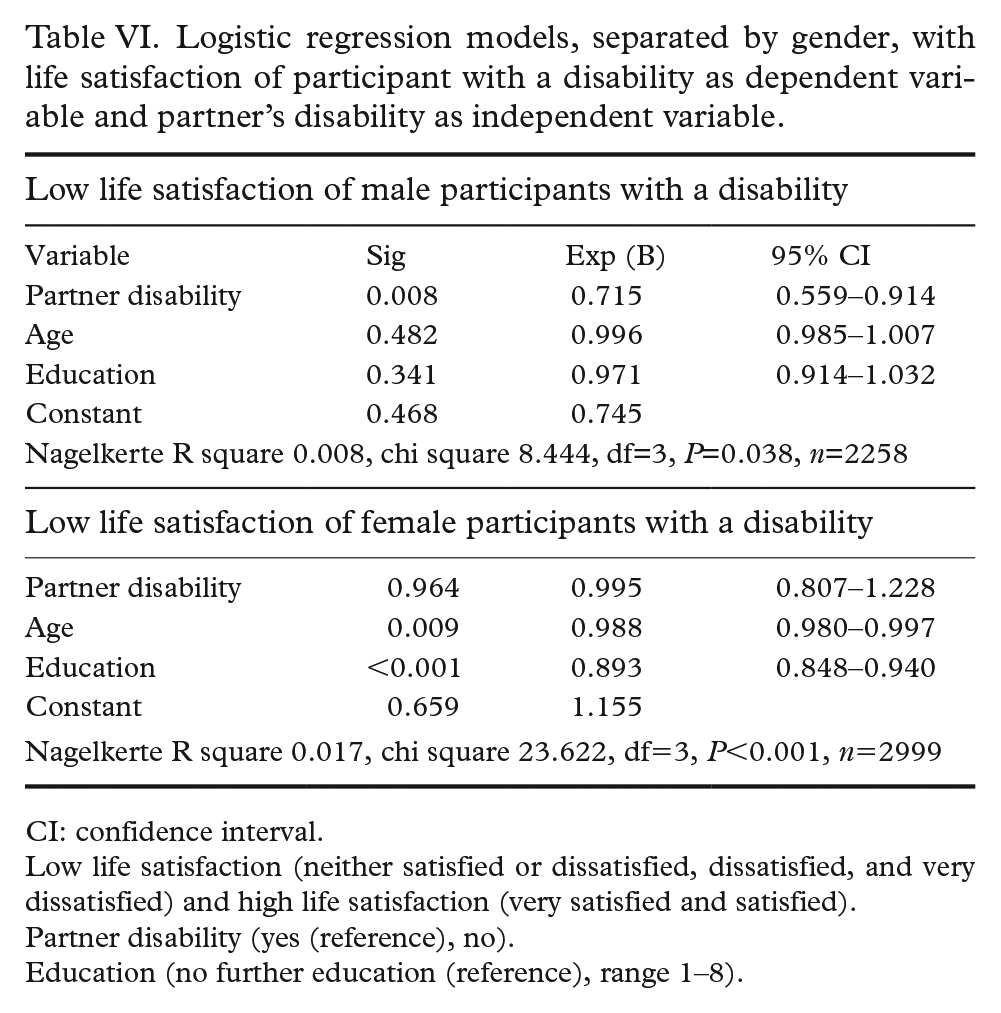
CI: confidence interval.
Low life satisfaction (neither satisfied or dissatisfied, dissatisfied, and very dissatisfied) and high life satisfaction (very satisfied and satisfied).
Partner disability (yes (reference), no).
Education (no further education (reference), range 1–8).
For male participants with a disability, an association was found between low life satisfaction and the onset of their disability after (as opposed to before) the start of their relationship (see Table VII). This association was not found for female participants with a disability. Similar to findings for the models in Table VI, younger age and lower levels of education were found to be associated with low life satisfaction for female participants, but not for male participants.
Logistic regression models, separated by gender, with life satisfaction of participant with a disability as dependent variable and onset of participant’s disability as dependent variable.
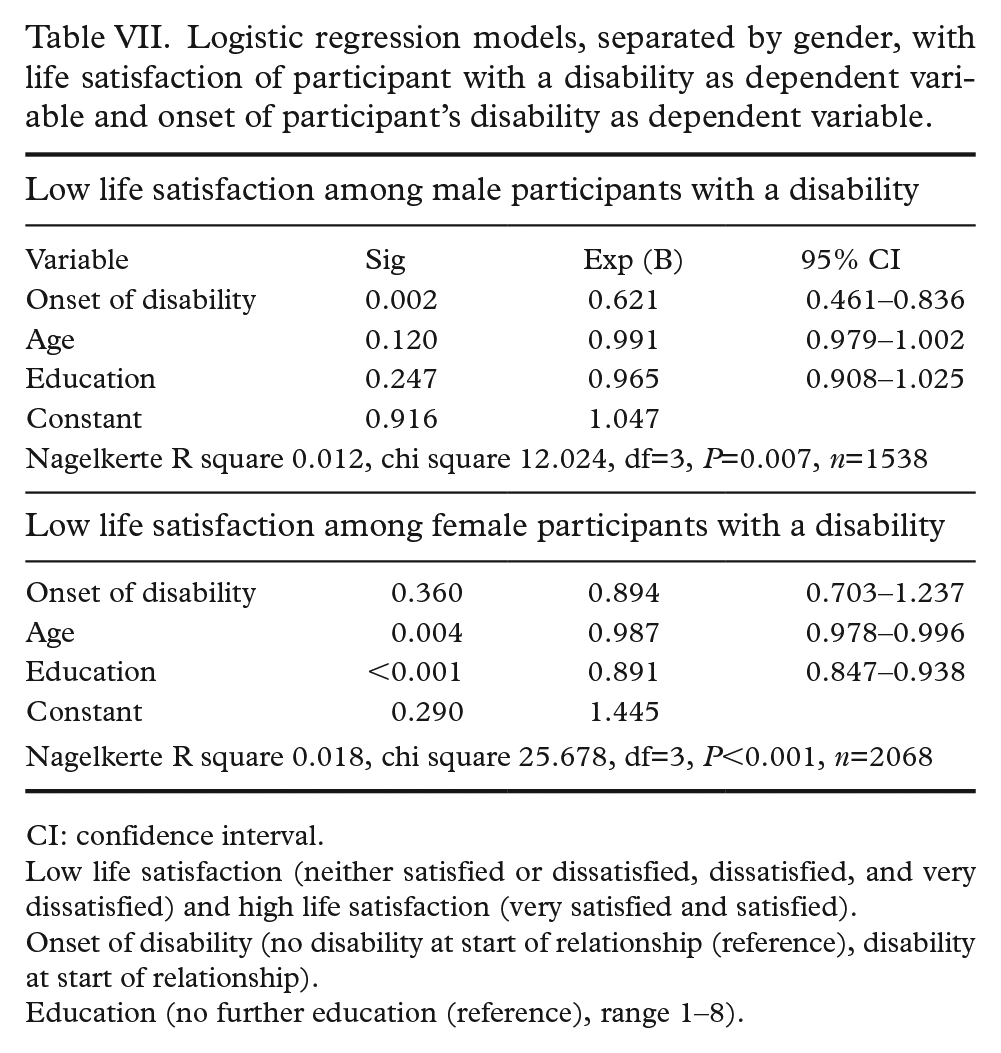
CI: confidence interval.
Low life satisfaction (neither satisfied or dissatisfied, dissatisfied, and very dissatisfied) and high life satisfaction (very satisfied and satisfied).
Onset of disability (no disability at start of relationship (reference), disability at start of relationship).
Education (no further education (reference), range 1–8).
Discussion
Overall, this study found clear evidence for couple similarity with respect to disability. Participants with a disability were more likely than those without a disability to have a partner with a disability. Specifically, participants with a physical disability were more likely to have a partner with a physical disability, and participants with a mental disability were more likely to have a partner with a mental disability. Further, participants were also more likely to have a partner with the same kind of physical or mental disability. Finally, participants with a minor or major disability were more likely to have a partner with a minor or major disability, respectively.
More research is needed to understand the associations found here and the possible causalities. One part of the explanation may be the effects of familiarity and similarity, whereby people are more likely to meet and develop relationships with those they are familiar with and those who are socially similar to them [1]. Applying this to disability, it may be supposed that people with the same disability are likely to meet, for example through special education and health and social care services. Further, the experience of disability and involvement in disability-related activities, such as campaigns for disability rights, might result in similarities of attitudes and opinions. Distinct communities and cultures may also arise, as is the case for the deaf community [19]: indeed, in this study, one of the highest frequencies for similarity was found for deafness. Overall, the findings here speak to preference for similarity in relationships [8]. However, other factors may also be implicated, such as social marginalisation and others’ attitudes towards disability, particularly with respect to physical disabilities [13]. This requires further research.
Another aim of this study was to examine if life satisfaction was associated with having a partner with a disability. The study found that having a partner with a disability was associated with low life satisfaction for men with a disability, although not for women with a disability. This may warrant further investigation, particularly as previous research has found that people with physical disabilities have difficulties forming intimate relationships and establishing sexual relationships [13]. The study here also found that high life satisfaction among men with a disability was associated with their disability being present at the start of the relationship, as opposed to the disability developing after the relationship had started. The association was not significant among female participants. Further investigation is required to explore how later onset of disability may threaten a relationship and thereby life satisfaction, and also how factors of similarity and difference impact over time with respect to different types of disability. For example, existing research shows that, for individuals with mental health issues, the impact of having a partner without such issues may be helpful over time. Specifically, research has shown how spouses of people with a mental health issue supported their partners to develop healthier habits and engage in less risky behaviour [20]. The effects of relationships have also been researched for couples in whom physical disability is present. For example, one study reported that spousal communication and perceived support predicted psychological wellbeing in couples in whom one partner acquired deaf/blindness, in line with the ‘relationship intimacy model’ that recognises the significance of a couple’s relationship for both partners’ psychosocial adjustment to illness [21]. Such research suggests the diverse factors that are likely to positively mediate how having a disability affects relationships and wellbeing. On the other hand, and as suggested by the associations found in this study, an accumulation of challenges may arise if both partners have or acquire a disability. More and longitudinal research is required to understand relationship processes of life satisfaction and wellbeing if one or both partners have a disability.
The gender differences found in this study also demand further investigation. Known gender differences in relationship preferences, for example that men value the physical appearance of a partner more highly than women do [14–16], may play a particular role with respect to disability. Gender-specific stigma and cultural gender norms around providing care and support, as well as around showing strength and self-reliance, might also profoundly affect how couples cope with disability and communicate about illness and needs [22]. Overall, the findings of this study call for a better understanding of how having a disability affects relationship formation and, further, how an acquired disability affects wellbeing and relationship satisfaction. These issues are of public health importance, and future disability research would do well to explore the interrelations of relationships, gender and wellbeing in order to inform policies on inclusion and how best to support women and men with disability.
Limitations
The information on physical and mental disabilities in this study was self-reported and therefore carried the risk of response bias in relation to both the participant’s own disability and that of their partner. Further, the study was at risk of participation bias in that people with severe disabilities, including those with low literacy skills, would be less likely to participate. Finally, as this study was a cross-sectional study, it is not possible to draw conclusions as to the causality of the associations found.
Footnotes
Availability of data
The data is accessible from the Danish National Centre for Social Research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The Danish National Centre for Social Research is an independent government institution and conducts research according to national research ethical codes.
Informed consent
Informed consent for participation and use of data was obtained from all participants included in the study.