
Abstract
Background:
Previous studies indicate that poor oral health may constitute a barrier for labour market success. This study examines whether an oral health promotion intervention has an effect on economic self-support, and proximity to the labour market, among socially disadvantaged unemployed people.
Methods:
From April–June 2018, we enrolled 273 vulnerable people on welfare benefits into a randomised controlled trial. Participants were allocated to either control (n=159), or intervention (n=114). Intervention consisted of individual support to improve individuals’ oral health by reducing significant barriers to dental care. Ten participants were excluded, leaving 263 participants (intervention n=110, control n=153) for analyses. A national register was used to assess economic self-support and proximity to the labour market within 1.5 years post-intervention. Items of information on health and socio-demographics were obtained from a questionnaire and from national registers. Logistic and multiple linear regression modelling was performed.
Results:
Overall, higher frequencies of economic self-support and proximity to the labour market were found in the intervention group, although no significant results were seen for economic self-support alone. Adjusted models revealed significantly higher odds (odds ratio=1.85, 95% confidence interval 1.08–3.17) among the intervention group of achieving proximity to the labour market after 12 months. After 18 months, the intervention group had on average obtained 5 more weeks (95% confidence interval 0.02–9.99) with proximity to the labour market.
Conclusions:
Keywords
Background
Inequality in oral health and utilisation of oral healthcare is a persistent global challenge [1,2]. Over the last two decades, oral health in the Nordic countries has generally improved, although to a smaller degree among the marginalised and socially excluded groups in society, widening the gap in oral health between these groups and the general population [3]. In Denmark, the most disadvantaged members of the population have the poorest oral health and the most infrequent utilisation of oral healthcare, although they have the greatest need [4]. These people are the socially disadvantaged, many of whom are unemployed, with complex problems and facing significant barriers towards employment, including psychological or physical health issues, low educational level, homelessness, and abuse.
The literature indicates that within this disadvantaged group, poor oral health can be an obstacle to employment [5,6]. The consequences of poor oral health are many, including pain, discomfort, embarrassment and a negative impact on overall health, quality of life and social well-being [1,2], resulting in reduced self-esteem, social interaction and employability [6]. Embarrassment and lack of self-confidence can, according to the citizens themselves, deter them from applying for job vacancies, and the general perception was that no one with bad teeth would be entrusted with a job [6]. Thus, poor teeth may constitute a barrier for labour market success, and some studies even suggest that dental treatment increases job-seeking self-efficacy and employment among unemployed citizens [7 –9].
In 2013, the Danish government decided to offer subsidies through the Act on Active Social Policy (§82 and §82a), for necessary and preventive oral care for socially disadvantaged unemployed people with zero or limited financial assets [10,11]. However, the uptake of the programme has been very low, potentially due to a lack of awareness, a highly bureaucratic application process and psychological barriers towards dental treatment [12].
This study is the first to investigate whether an oral health promotion (OHP) intervention targeted to overcome these obstacles has a positive effect on economic self-support (ESS) and proximity to the labour market (PLM) among socially disadvantaged, unemployed citizens. We hypothesised that the intervention would be beneficial, leading to increased self-support or progression towards this.
Methods
Study population and recruitment
We conducted a prospective, randomised and controlled study in a group of long-term unemployed, activity-ready recipients of cash benefits affiliated to a job centre situated in Copenhagen. Cash benefits constitute the lowest level of social and unemployment benefits in Denmark and are only available when no other support option exists [13]. Recipients assessed as activity-ready are not considered ready to enter the labour market in the short term but have the potential to enter the labour market in the long term [14]. These recipients have social and/or health issues, besides being unemployed [14].
Recruitment of the participants took place at the job centre from 16 April–19 June 2018. Randomisation proceeded according to a set schedule, decided by the research team prior to recruitment, in which each calendar day determined whether participants at the job centre were assigned to the intervention group or the control group. The stratification of days was performed alternately between intervention and control, ensuring a similar number of intervention days to control days. A recommended method, among others, to tackle recruitment challenges among socially disadvantaged and other hard-to-reach populations is to operate via community partnerships [15]. The recruitment was therefore handled solely by caseworkers at the job centre, who were unaware of the randomisation sequence in order to ensure unbiased ascertainment of outcomes. The recruitment process started with the caseworker presenting the study as part of the regular interview and asking if the citizen was interested in participation. If this was the case, the citizen was directed to a study station where a research assistant provided a more detailed introduction to the study, including group allocation and information on what the intervention implied. Information on opt-outs was not registered due to the high number of caseworkers involved and the recruitment being perceived as an extra daily task for them. However, it was found that the most prominent reason for opting out was the amount of time required to participate.
Citizens who wished to participate (n=273) signed an informed consent form before filling in a self-administered questionnaire covering information on demographics, health status and quality of life. Members of the control group (n=159) were thanked for their effort, while those in the intervention group (n=114) proceeded to the intervention (Figure 1). The study was approved by the Danish Data Protection Agency and the Committee on Health Research Ethics (H-17033912).
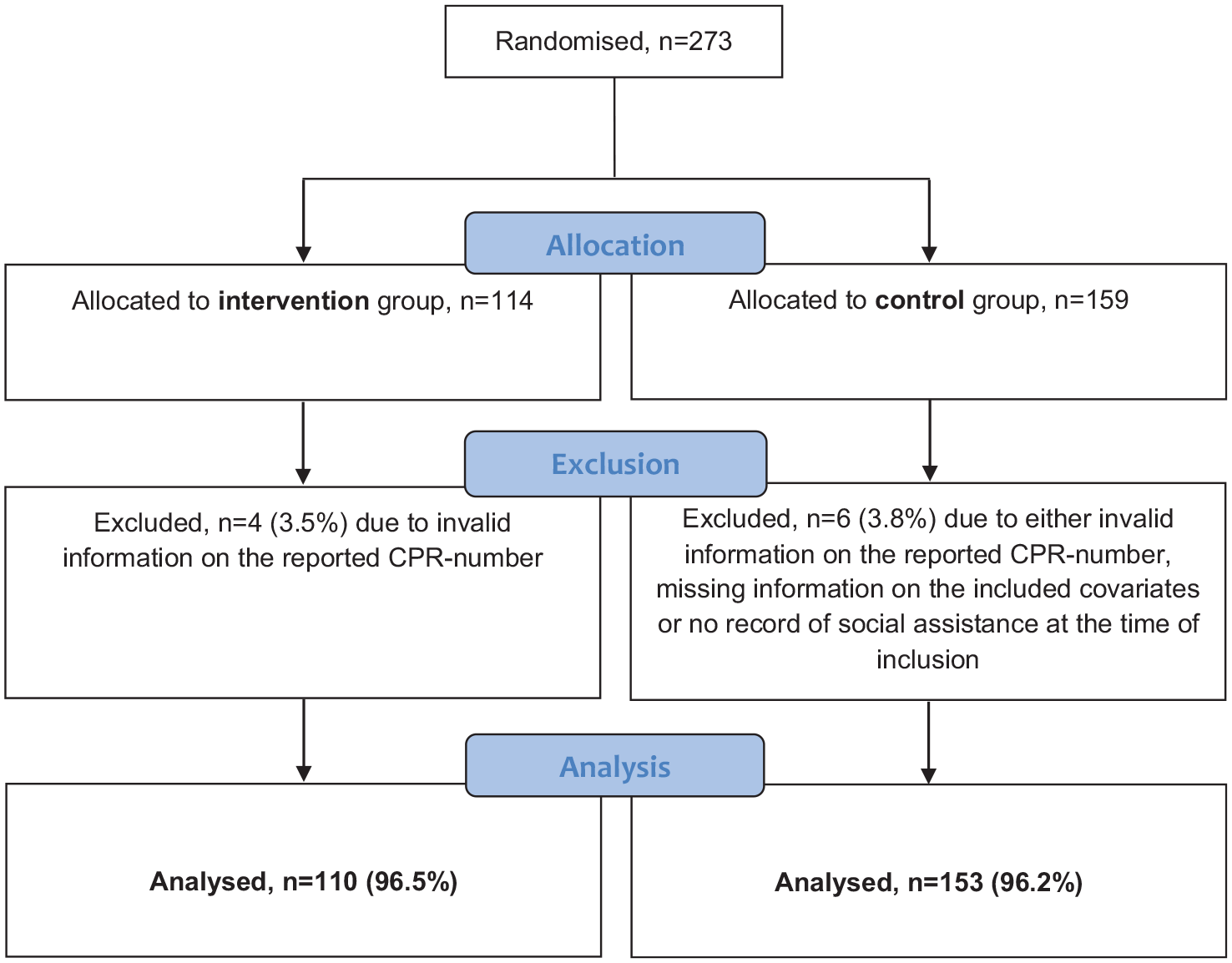
Flow chart of the study population. CPR: Centrale Person Register.
Intervention
The intervention was an individually tailored OHP intervention. Dependent on each participant’s needs and wishes for dental health, the intervention consisted of information, motivation and support for dental treatment, including applying for the oral health subsidy. Some citizens who wished to have dental treatment, but did not know where to go for this, received help from the research team who made an appointment at a dentist for them. Others received information and help in coping with potential dental fear and were encouraged to seek oral treatment. The financial barrier was accommodated by a caseworker who provided individual help with the application for subsidy, which is secured in the municipal subsidy scheme §82 and §82a in the Act on Active Social Policy [10,11]. In some cases the citizen made an agreement with the caseworker to return another day to complete the application, due to the large amount of documentation needed. Overall, the broad variety of elements entailed in the intervention thus aimed to reduce several barriers towards improving the individual’s dental health.
Outcomes
This study included two register-based outcomes, (a) ESS and (b) PLM), both based on information from the Danish employment database (DREAM) of the Danish Ministry of Employment. The database contains codes with information on all disbursed public social benefits, registered on a weekly basis [16]. We obtained data on all participants on an individual basis over 1.5 years (78 weeks) to evaluate the effect of the intervention at intervals of 6 (T6), 12 (T12) and 18 (T18) months from baseline (the week of recruitment). These intervals were chosen to accommodate both the processing time for the application and the period for receiving dental treatment after the intervention.
Our primary outcome, ESS, was recorded if the citizen in at least 4 consecutive weeks received no transfer income except for leave of absence schemes, maternity leave pay and grants from the State Education Fund [16]. The 4 weeks were chosen to accommodate a more persistent measure of self-support and to avoid misclassification due to a vacation or a missing residential address. PLM, the secondary outcome, was defined if the citizen, in at least 4 consecutive weeks, was registered with either ESS or job-oriented progress (on the job training, wage-subsidised jobs, or employment in a flex-job for citizens with reduced work hours and work ability). Both outcomes were coded in binary form into ‘yes/no’. To investigate the effect of the intervention on the accumulated amount of ESS and PLM we also estimated the total number of weeks with ESS and PLM achieved by each participant at T6, T12 and T18.
Covariates
Information on all covariates was obtained at baseline. From national registers, we retrieved data on the history of ESS and PLM, nationality, cohabitation and education. Data on age, sex, self-reported health and oral health-related quality of life (OHRQoL) were accessed from the questionnaire.
From the DREAM database, we calculated the history of ESS and PLM for each participant over a two-year period prior to baseline. History of ESS was dichotomised into (a) no (0–3 weeks) and (b) yes (⩾4 weeks). History of PLM was further categorised into (a) no (0–3 weeks), (b) yes, some (4–14 weeks) and (c) yes, a lot (>14 weeks); since the median among participants with a record of ⩾1 week with PLM was 13.5 weeks. Nationality was also available from the DREAM database and participants were registered as (a) Danish or immigrant/descendant of Western origin or (b) immigrant/descendant of non-Western origin. On the basis of data from other national registers cohabitation was coded in binary form into (a) married or (b) unmarried, divorced or widower/widow; and education was classified according to the International Standard Classification of Education (ISCED) framework [17] and further dichotomised into (a) low educational level (ISCED level 0–2) and (b) high educational level (ISCED level 3–8). The first category also included participants with missing information on their educational level and ‘not elsewhere classified’.
Self-reported health was evaluated using the Short-Form health survey (SF-12v2) [18], which consists of 12 items across eight domains that illustrate a person’s health status within the last 4 weeks. These domains are collectively reported as a Physical Component Summary (PCS) and a Mental Component Summary (MCS), ranging from 0–100 points, with a score of 100 constituting the best possible health status. OHRQoL was evaluated using the Oral Health Impact Profile (OHIP-14) questionnaire [19]. The questions concerned self-evaluated problems in the oral area during the past month, resulting in a score of 0–56 points, with lower scores indicating better OHRQoL.
Statistical analysis
Data was accessible through Statistics Denmark and was linked to nationwide registers through each participant’s unique Civil Registration Number (CPR). All analyses were carried out using SPSS statistics version 27, and results were considered significant when the p-value was <0.05. We excluded 10 participants, due to invalid information on the reported CPR-number, missing information on the included covariates, or there being no record of social assistance at the time of inclusion, leaving 263 participants for analyses. Descriptive statistics were used to calculate frequencies and means for all covariates. Mann-Whitney U and Pearson Chi-Square tests were used to test for statistical significance of differences in baseline characteristics and subsidy take-up between the intervention and the control group at baseline. We used bivariate analyses to determine the proportion of participants achieving ESS and PLM, including the accumulated number of weeks gained for both outcomes at intervals of 0–6 (T6), 0–12 (T12) and 0–18 (T18) months from baseline. The percentage increase was calculated from T6–T12 and T6–T18 to investigate the temporal effect of the intervention.
The primary analysis assessed whether the intervention changed the probability of achieving ESS or PLM at T12 and T18, using binominal logistic regression, and whether the intervention increased the number of weeks obtained with ESS and PLM at T12 and T18, using multiple linear regression. The results were reported unadjusted and adjusted for baseline values and group allocation to increase power [20] with odds ratios (ORs), regression coefficients (b), standard errors (SEs) and 95% confidence intervals (CIs). All models were fitted separately for each of the two outcomes and fulfilled the required model assumptions.
Results
Of the 263 participants, 110 belonged to the intervention group while 153 belonged to the control group. Within the first 6 months after recruitment 46.4% of the individuals in the intervention group (51/110) applied for the oral health subsidy. In comparison only 7.2% of the individuals in the control group applied for subsidy (11/153). The difference in take-up is highly significant (p<0.001).
Baseline demographics (Table I) of the participants revealed a majority to be women, and there was a mean age of 47 years. More than 40% of the participants had non-Western nationality, approximately 80% were unmarried, more than two-thirds had a low educational level, and the majority had no history of ESS and PLM measured 2 years prior to baseline. Overall, no significant differences in baseline characteristics were seen between the intervention and control group.
Baseline characteristics of study participants (n=263).
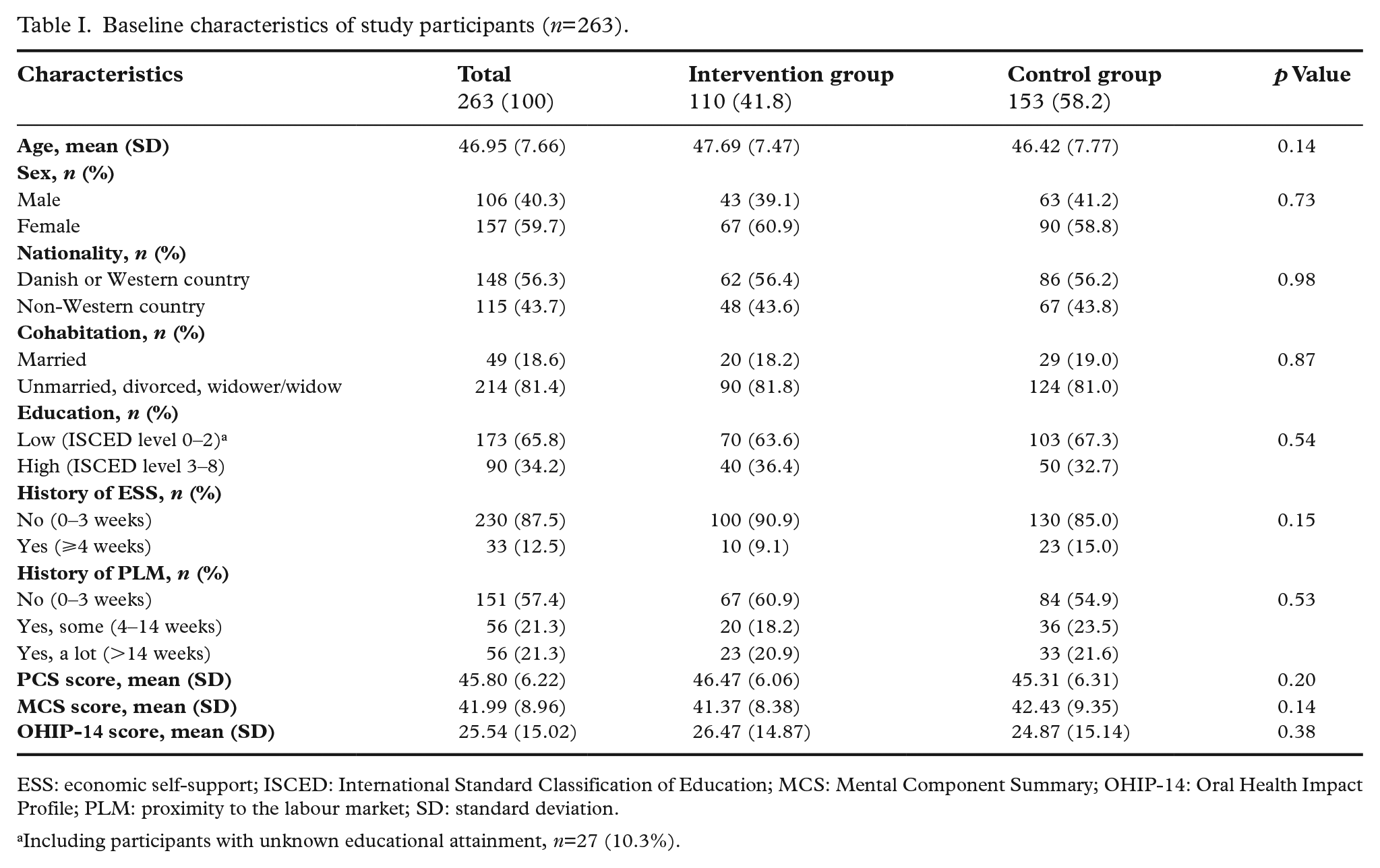
ESS: economic self-support; ISCED: International Standard Classification of Education; MCS: Mental Component Summary; OHIP-14: Oral Health Impact Profile; PLM: proximity to the labour market; SD: standard deviation.
Including participants with unknown educational attainment, n=27 (10.3%).
The temporal and unadjusted effects of the intervention are presented in Table II and Figure 2(a) and (b). A higher proportion of participants in the intervention group than the control group achieved ESS and PLM at T6, T12 and T18, although the results were only statistically significant at T12 for PLM. The accumulated mean number of weeks with ESS were slightly higher for the control group at T6 compared to the intervention group, although it changed at T12 and T18 where the number of weeks with ESS was higher in the intervention group. The number of weeks with PLM was higher at all stages in the intervention group, however, this was not significant. The results in Table II furthermore reveal an overall increase over time in both groups in terms of the proportion achieving ESS and PLM, and in the total amount of weeks accumulated with ESS and PLM. The increase in ESS was however based on low absolute numbers. For both outcomes, the percentage increases were consistently higher in the intervention group.
Trajectory of economic self-support (ESS) and proximity to the labour market (PLM)
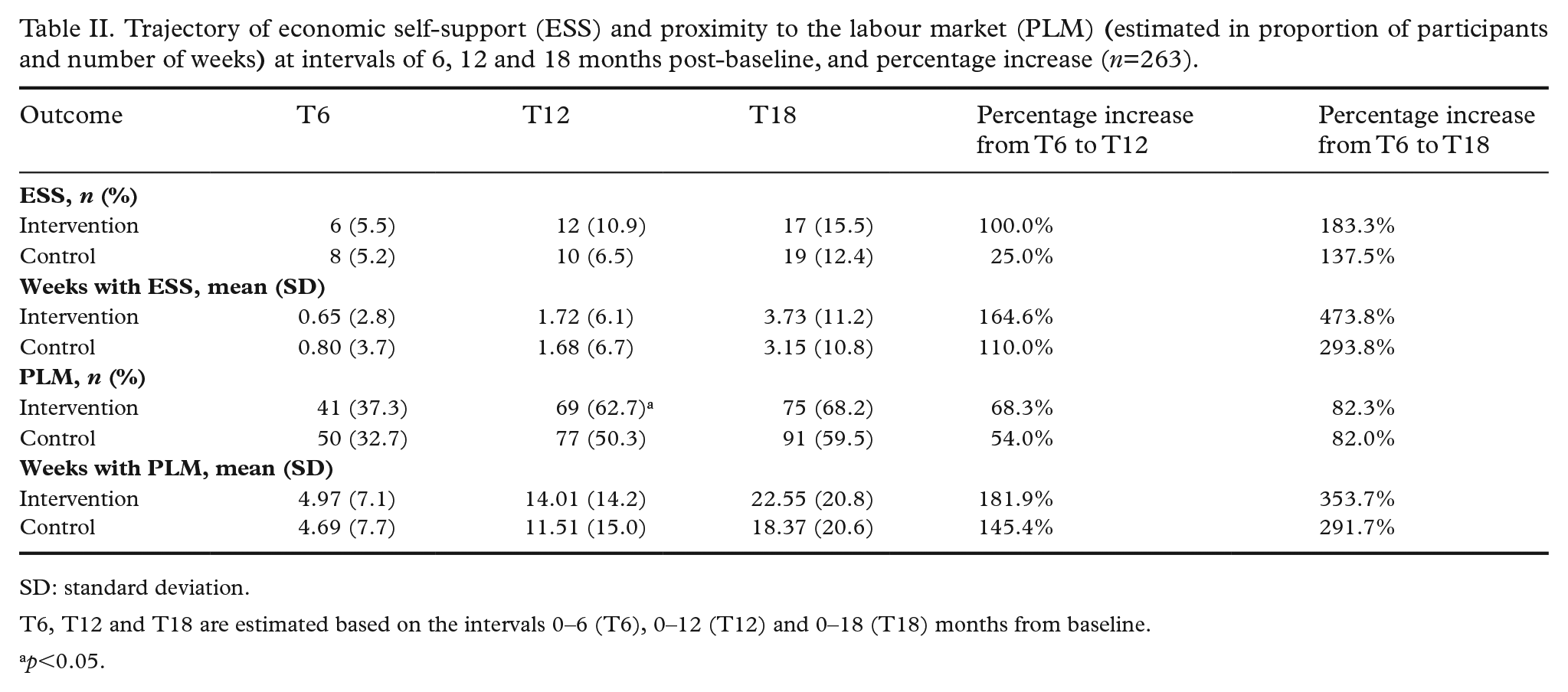
SD: standard deviation.
T6, T12 and T18 are estimated based on the intervals 0–6 (T6), 0–12 (T12) and 0–18 (T18) months from baseline.
p<0.05.
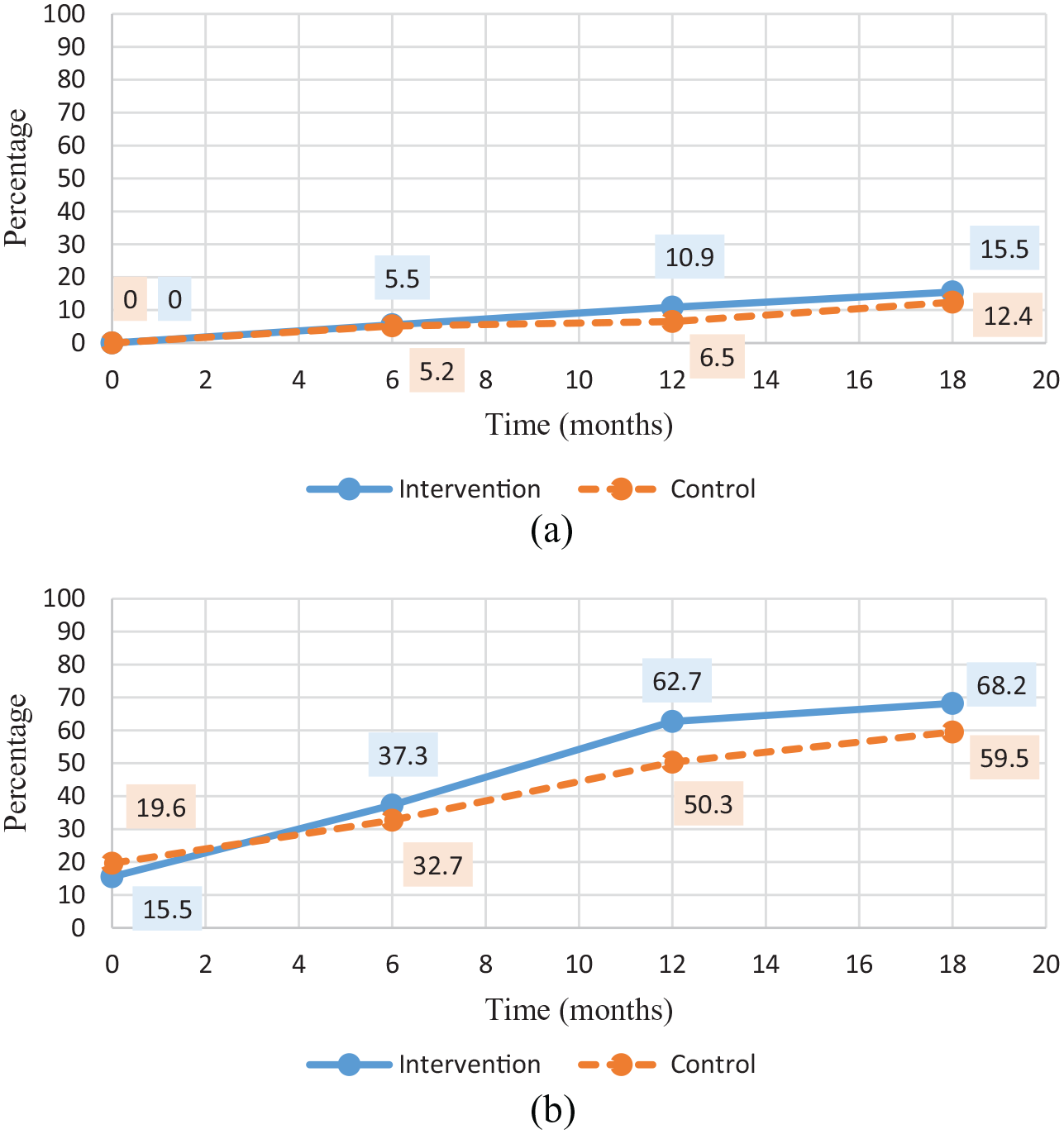
Proportion of participants achieving economic self-support (ESS) and proximity to the labour market (PLM) respectively within 1.5 years post-intervention.
The primary adjusted logistic regression analysis revealed increased odds for the intervention group in achieving ESS and PLM at T12 and T18 (Table III). The intervention group had odds 1.85 times higher (95% CI: 1.08–3.17) of achieving PLM at T12, in comparison to the control group. The results, however, were not significant at T18 (OR: 1.58, 95% CI: 0.90–2.76). The results from the multiple regression analyses revealed higher adjusted regression coefficients for the intervention group at all times, suggesting that this group also accumulated more weeks with ESS and PLM during the study compared to the control group. At T18 the intervention group had on average experienced 5.00 weeks more (95% CI: 0.02–9.99) with PLM than the control group. Estimation results for the more restrictive ESS measure were not significant, however, in line with the findings for PLM with positive point estimates.
Unadjusted and adjusted results from logistic and multiple linear regression analyses of experiencing economic self-support (ESS) and proximity to the labour market (PLM) at T12 and T18 for the intervention group (n=263).
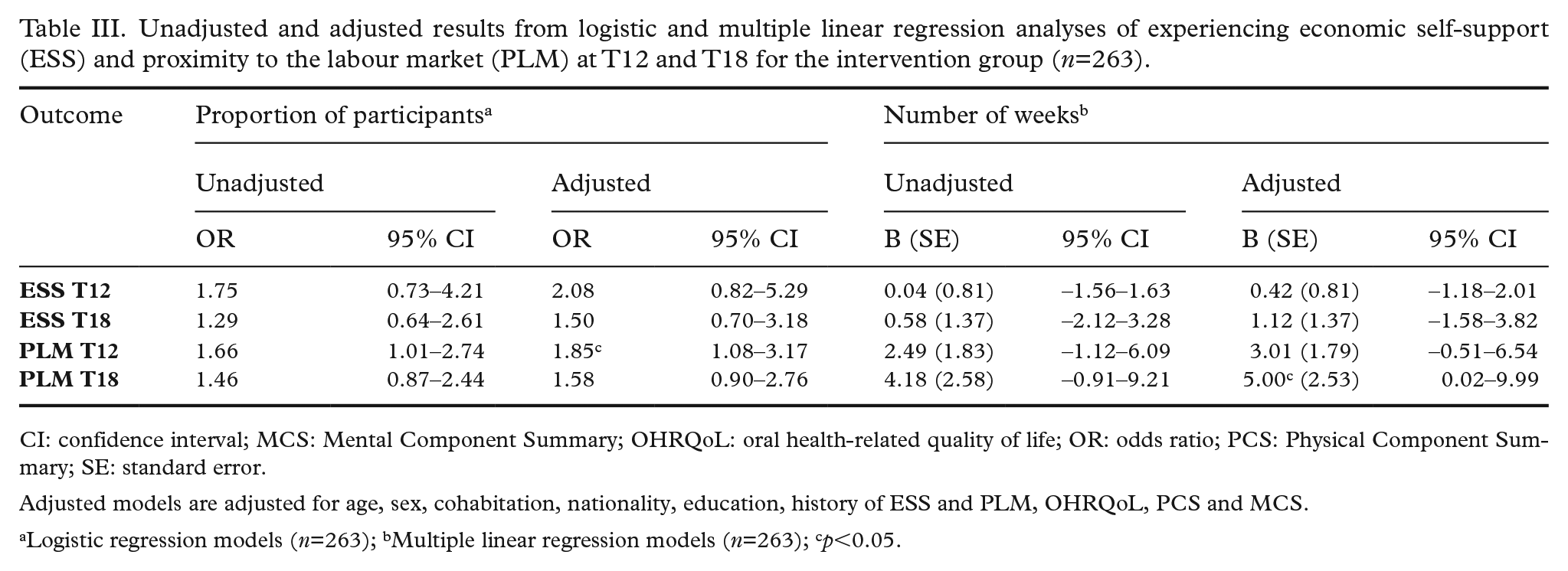
CI: confidence interval; MCS: Mental Component Summary; OHRQoL: oral health-related quality of life; OR: odds ratio; PCS: Physical Component Summary; SE: standard error.
Adjusted models are adjusted for age, sex, cohabitation, nationality, education, history of ESS and PLM, OHRQoL, PCS and MCS.
Logistic regression models (n=263); bMultiple linear regression models (n=263); cp<0.05.
Discussion
To our knowledge, this is the first study to investigate the effect of an OHP intervention on labour market prospects among socially disadvantaged citizens. The existing evidence in this field has mainly focused on the effect of dental treatment provision, showing small but relatively weak results in favour of treatment [9]. Overall, our randomised controlled trial (RCT) indicates that the OHP intervention was beneficial; a higher frequency of individuals achieving ESS and PLM was generally found in the intervention group, as hypothesised. However, the estimated effects were relatively small, and significant results were only seen for PLM.
According to a literature-based framework, the provision of dental treatment potentially improves OHRQoL and self-efficacy, and thereby increases employment opportunities [8]. In this regard, a positive correlation between dental care and self-reported job-seeking self-efficacy among recipients of social assistance has been found [8]. Likewise, it has been found that recipients of social assistance who received preventive dental treatment terminated social assistance more often [21] and had more favourable employment outcomes, compared to people who did not receive dental treatment [7]. The theoretical framework and related findings thus support our hypothesis, that the positive labour market prospects found in our study can be attributed to the OHP intervention. However, it is important to state that, while we have data on labour market outcomes and uptake of the oral health subsidy, we have no information on dental treatment received. This could have strengthened our process theory even more and made it easier to compare our findings with the previous literature in this field. Our study enabled us, however, to investigate the direct effect of a low-cost OHP intervention on the take-up of oral health subsidy and indirectly evaluate the long-term benefits on labour market outcomes, through an intention-to-treat approach. Our intervention, thus, stands in the tradition of so-called ‘encouragement designs’ in which individuals or groups are randomly assigned to receive encouragement to take up an existing programme as seen in similar studies [22,23]. Evaluating the indirect effects of the intervention stands in the tradition of influential earlier RCTs, as seen within other disciplines [24,25].
The only prominent and significant results in our study were seen for PLM. Nordic studies reveal that active labour market programmes, as embedded in PLM, yield a positive effect on subsequent employment and self-support among unemployed citizens [26,27]. The PLM indicator is thus considered robust for possible employment, and our broad definition and use of PLM seems appropriate for capturing all relevant labour market prospects when dealing with this particular group of unemployed and socially disadvantaged people. By comparison, ESS might be too restrictive, with an extremely high barrier to success for this population. In Denmark, few activity-ready citizens leave social assistance and become financially independent, which might be a possible explanation for the non-significant results for ESS, together with the low sample size [28].
Several factors increase the internal validity of the study, namely allocation concealment and the fact that no significant differences were found between the intervention and control group at baseline, which indicates successful randomisation [29]. Furthermore, using register data in accessing the outcome minimised the risk of detection bias [29]. In general, the use of nationwide register data for obtaining baseline characteristics and outcomes measures ensured high accuracy of the applied data. The available data also enabled us to extract information on each participant’s past social assistance record, as well as validated instruments of the participant’s health status [19,30], making it possible to adjust for important aspects of the probability of getting a job or leaving social assistance [14]. As a limitation, we did not have the opportunity to include all determinants that might influence labour market prospects. For example, some studies suggest that alcohol abuse affects employment outcomes [31,32]. The inclusion of this information could have led to more precise estimates of the true effect sizes.
Regarding contamination bias, programme participation by individuals assigned to the control group in an encouragement design commonly does not reflect treatment contamination, but simply regular take-up of the programme in the absence of the additional information received by the intervention group. All our results reflect intention-to-treat effects, since citizens in the control group also had the possibility to apply for subsidy and seek dental treatment. This limits the possibility of quantifying the labour market effects of receiving dental treatment, rather than receiving encouragement to apply for the dental health subsidy and improve one’s dental health. However, the take-up of the subsidy scheme in the control group is low (7.2%), which limits potential biases.
A potential danger to the interpretation of some of our results (in particular, the size of our treatment effects) would be ‘spillovers’ of our intervention into the control group. Such treatment contamination could, for example occur if some individuals in the control group were falsely assigned to receive the information and support, or if they indirectly received the information and encouragement from participants in the intervention group. Our randomisation protocol ensures that treatment spillovers are unlikely to occur in our setting. Firstly, the intervention was assigned by a member of our research team, and not by the caseworker. Secondly, all individuals who participated in the study on a given day were either assigned to intervention or control, such that information leakage by citizens who visit the job centre on the same day can be ruled out.
Overall, employment progress was also seen among those in the control group, possibly caused by the following two reasons: (a) employment progression was expected because participants were sampled among individuals farthest away from employment who still had potential to enter the labour market in the long term, and (b) the control group underwent steps (receiving information, answering questionnaire etc.), which in themselves constituted a type of intervention. The second reason would result in an underestimation of the total effects of our intervention.
One essential limitation of most RCTs involves external validity. In our study, the generalisability to the target population of long-term unemployed, activity-ready recipients of social benefits was limited, since participation was voluntary and selection bias may have occurred, resulting in a skewed distribution of participants in the groups and no record of the total number invited. However, the sample is representative in terms of gender, nationality and education, although not in terms of age, which was lower in the target population [33]. Probably, participants were also more resourceful than the target population, in which case the effects may be incorrect. Although the results of this study are specific for the institutional setting of social assistance in Denmark, the disadvantages of poor oral health are universal across nations and in different labour markets. Therefore, the small but positive labour market outcomes, resulting from the intervention, highlight the potential of oral health promotion in aiding social rehabilitation. Our findings are relevant for decision-makers, who should consider oral health promotion among socially disadvantaged citizens when allocating resources and providing services.
Future well-controlled studies should thus examine the possibility of optimising and upscaling the intervention to reach more people and heighten the effectiveness, which might be increased further by targeting the intervention to people with evident dental problems. Collecting data on oral care received as a result of the intervention should also be prioritised to clarify the association. Furthermore, and importantly, increased labour market prospects are just one outcome following oral health promotion and improved access to dental care. Increasing OHRQoL, health, self-efficacy, and improving the ability of people to eat and speak, should also be motivational factors in promoting oral health and reducing social inequality.
Footnotes
Acknowledgements
The authors would like to thank the caseworkers and managers in the job centre for their help in recruiting participants, and the dentists who made appointments and treatments in their clinic available for the intervention. Data from the participants collected from the questionnaire will be available on reasonable request and only for the purpose of research. Data from the Danish National Registers was made accessible through Statistics Denmark for this study by a granted authorisation, which is necessary as this data is not publicly accessible. Regarding author contribution, EBØ, KDJ, BH and SA conceptualised and initiated the trial. EBØ and KDJ were responsible for the data collection. EBØ, IB and AMS made the analysis plan, and evaluation design, and carried out all analyses including interpretation of the results. AMS drafted the manuscript. All authors contributed to the manuscript, provided critical peer review, and accepted the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was financially supported by research grant A1575 from the Regional Fund for Joint Measure and the Danish Dental Association (identified by the title (in Danish): 'Samfundsgavnlig effekt ved tandbehandling af kontanthjælpsmodtagere').