
Abstract
The objective of this systematic review was to evaluate the prevalence of periodontal disease in South Pacific Island countries. A literature search was conducted using Scopus, Medline (via PubMed and Ovid), databases, and Google Scholar. The inclusion criteria for the review were the studies that reported on periodontal disease in the 1- to 85-year age group, excluding data from Australia, New Zealand, and protectorates of the United States and France. The findings from the studies were synthesized, noting the demographics, periodontal disease assessment methods, and main outcomes. The initial search yielded 475 relevant articles. After further screening for eligibility, a total of nine articles were included in this systematic review. In the studies included, the population ranged from 185 to 7966 participants with the age range of 1 to 64 years. The studies were heterogeneous, with each study utilizing different criteria to assess periodontal disease. Notably, the latest study eligible for inclusion was published in 2012. The prevalence of periodontitis ranged from 20% to 100%, with greater prevalence in the age group of 40 years or older. The findings from this review highlighted the need for regular prevalence studies to inform public health policy makers and develop strategies to manage periodontal disease proactively.
Keywords
What We Already Know
Periodontal diseases is one of the most common oral diseases affecting humans globally.
There is a challenge in estimating the current burden of periodontal diseases in South Pacific Island countries due to the lack of recent prevalence studies.
In the countries where data are available, a higher prevalence of periodontal disease has been observed in South Pacific Island nations compared to high-income countries.
What This Article Adds
A lack of periodontal disease prevalence studies and management in many of the South Pacific Island countries is noted due to a lack of local expertise, funding, and inter- and intra-country geo-isolation.
Historically, the high prevalence of periodontal disease in South Pacific Island countries may be attributed to minimal access to periodontal services and a lack of regular oral hygiene practices.
There is an urgent need to build local capacity and develop preventive strategies to improve the periodontal health of the population in South Pacific Island countries.
Introduction
Oral disease is estimated to affect 3.5 billion people with periodontal disease accounting for 1 billion worldwide, making it a significant global health burden.1 -3 Periodontal disease, one of the most common oral diseases, is a bacterial infection that causes chronic inflammatory disease of the tissues supporting the teeth, ie, gingivae, alveolar bone, and periodontal ligament. 4 Inflammation of the gingivae (termed gingivitis), if untreated progresses to periodontitis, involving resorption of the alveolar bone and periodontal ligament.5,6 Severe periodontitis is known to be the sixth most prevalent disease globally and may lead to tooth loss that results in compromised aesthetics, nutritional deficiencies, psychological problems, and social self-isolation.7 -9 Multiple studies suggest potential systemic effects of periodontal disease including association with increased risk of cardiovascular diseases, diabetes mellitus, 10 stroke, 11 inflammatory bowel disease, 12 low birth weight infants,13,14 and premature births.2,13,15,16
Epidemiological prevalence studies and preventive and therapeutic measures are critical in early identification and management of debilitating periodontal disease. Particularly in Asia Pacific region, being the most densely populated regions, it has the higher burden of oral diseases (65%) including periodontal diseases. 17 Many developing countries, including countries in the South Pacific, have limited resources to identify and manage periodontal disease. The South Pacific Island countries are in a unique geo-isolated situation, as the island countries are spread over a vast oceanic territory with each country consisting of multiple islands. 18 Commute between the islands is usually by boat due to limited land space to accommodate an airport. During inclement weather, such as tropical storms or cyclones, travel between these islands is limited, affecting essential supplies and health support for the island nations. 19 Furthermore, limited information exists on Oral Health-Related Quality of Life (OHRQoL), in relation to periodontal disease in these countries. 20 There is a paucity of information relating to the prevalence of periodontal disease in the region as well as preventive and therapeutic intervention in managing this disease. Hence, the aim of this review was to identify and summarize the prevalence of periodontal disease in Tonga and other South Pacific Island countries.
Methods
Study Description
This systematic review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines.21 -23 The PROSPERO registration number for this systematic review protocol is CRD42024579379. For the purpose of this review, only periodontal disease data were considered from the included studies.
Literature Search Strategy
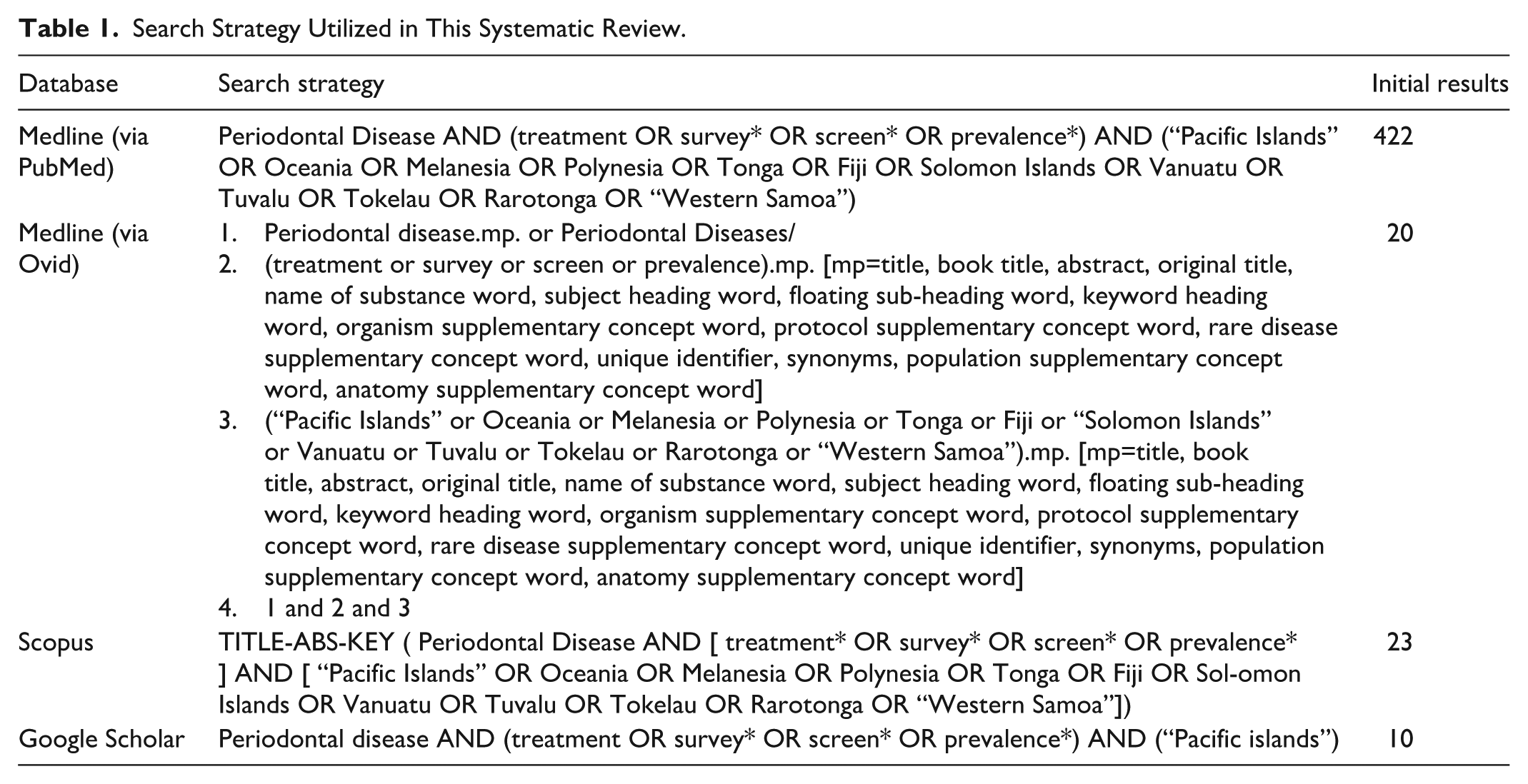
Online databases PubMed, Medline (via Ovid), Scopus, and Google Scholar were searched with the final search completed on May 19, 2025. Authors were contacted if any missing data or additional data were required from the eligible studies. Literature search was conducted using a combination of medical subject headings (MeSH terms—periodontal disease, prevalence, Pacific Islands, Oceania, Melanesia, Polynesia, Tonga, Fiji, Solomon Islands, Vanuatu, Tuvalu, Tokelau, and Western Samoa), and other relevant keywords in consultation with the medical liaison librarian. Appropriate Boolean operators (OR, AND) were used to refine the searches. More details of the search strategy can be found in Table 1. All the studies were screened for relevance by one reviewer and cross-checked by the second reviewer.
Search Strategy Utilized in This Systematic Review.
Inclusion Criteria
The review included all observational, cross-sectional, and longitudinal studies that reported the prevalence of periodontal disease in the South Pacific until May 2025, in the population aged 1 to 85 years except for studies from Australia, New Zealand, and protectorates of the United States and France in the Pacific.
Exclusion Criteria
This review excluded studies where the participants were aged below 4 years and studies published in languages other than English due to the additional need of resources (translation). Non-empirical articles were also excluded.
Risk of Bias Assessment
The methodological quality of the included studies was assessed using the risk of bias tool specifically designed for population-based prevalence studies. 24 This was cross-checked by a co-reviewer and disagreements were resolved through discussion. The tool consists of 10 items, which are divided into two domains, external validity, and internal validity. External validity (dealing with selection and non-response bias) had four items: 1—representation of the target population, 2—sampling frame a true or close representation of the target population, 3—randomization process, and 4—non-response bias. Internal validity had six items: 5—direct data collection from the subjects, 6—acceptable case definitions, 7—validity and reliability of study instruments, 8—consistent mode of collection, 9—length of the shortest prevalence period, and 10—addressing measurement bias and bias-related analysis. Each item was rated as “Yes” (low risk of bias) or “No” (high risk of bias). Each item with insufficient information was classified as “No” (high risk of bias). Overall, each article was rated for bias risk based on 10 items as “High” (score = 0-3), “Moderate” (score = 4-6), or “Low” (score = 7-10).
Results
The PRISMA flow chart (Figure 1) shows the process of identifying the studies for the systematic review. The original search yielded 475 relevant articles. After removal of 52 duplicates and non-English text (n = 4), a total of 56 articles were excluded. In total, 419 articles were screened further based on inclusion criteria such as participant age and geographic region and type of study, with 396 studies deemed not relevant to the focus of the review. The remaining 23 articles were assessed for eligibility by full-text review with 14 studies excluded due to data not reporting on periodontal disease. Consequently, a total of nine articles were included in this systematic review. Due to the high methodological heterogeneity of data measurement within the included studies, no meta-analyses were planned.
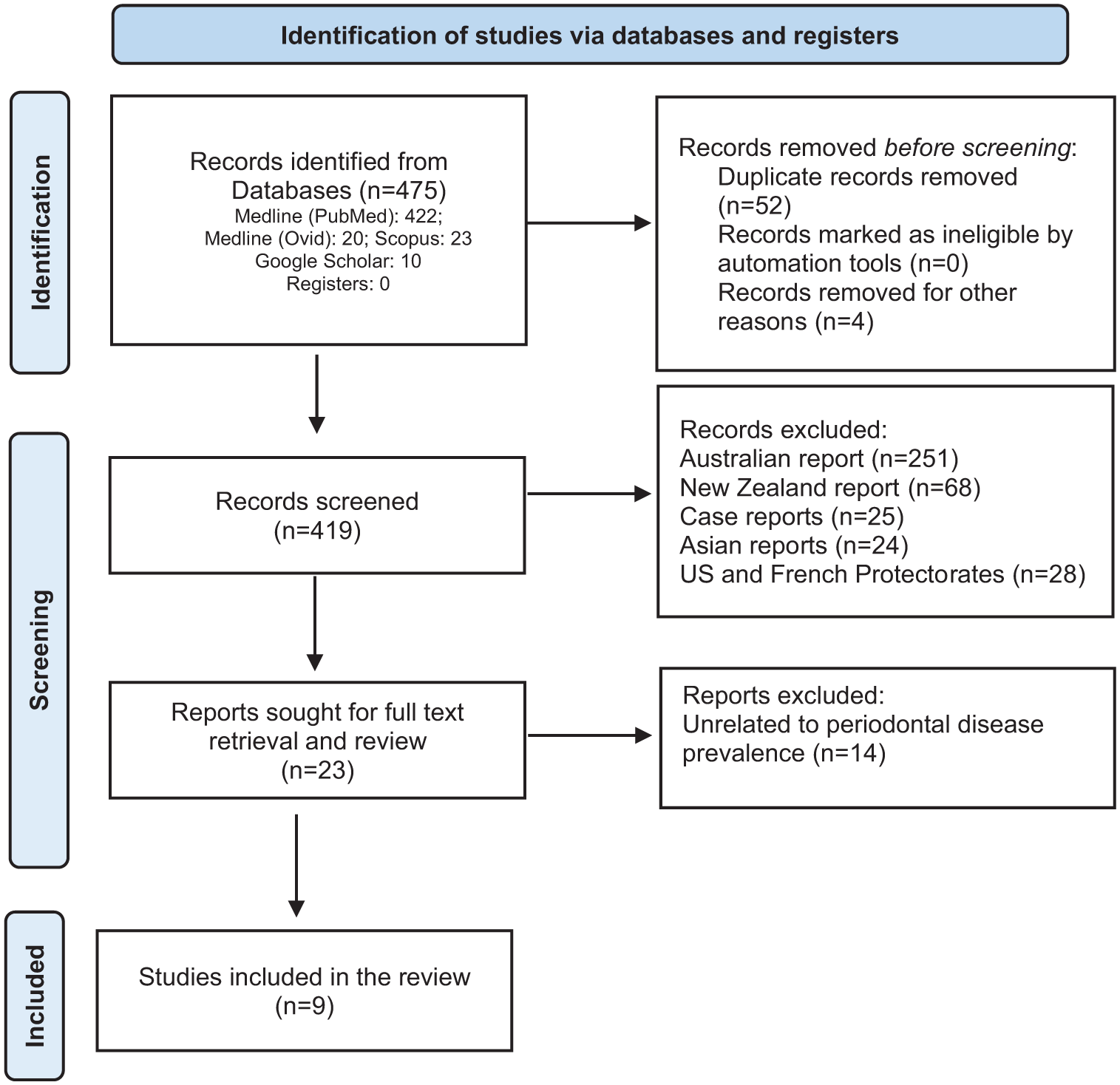
PRISMA flow diagram for the search utilized in this systematic review.
The studies included in this review were conducted across multiple decades ranging from 1956 to 2012. Table 2 provides the key characteristics of the studies included in this review, and Table 3 describes the risk of bias within the included studies. The sample sizes ranged from 185 to 7966 subjects with a population age range from 1 to 64 years. Interestingly, periodontal disease was recorded using a range of methods including Community Periodontal Index for Treatment Needs (CPITN), Full Mouth Attachment Level chart, and clinical (visual) assessment of the gingivae. Based on the included studies, the prevalence of periodontal disease in the South Pacific Island countries varied, ranging from 20% to 100% across the countries and periods assessed. One common finding was that the disease prevalence increased with age, as noted in Tonga and Samoa studies with 90% of adults over 40 years of age with periodontitis, while in Fiji, 97% of adults between 45 and 55 years had periodontitis.28,30
Characteristics of the Included Studies.
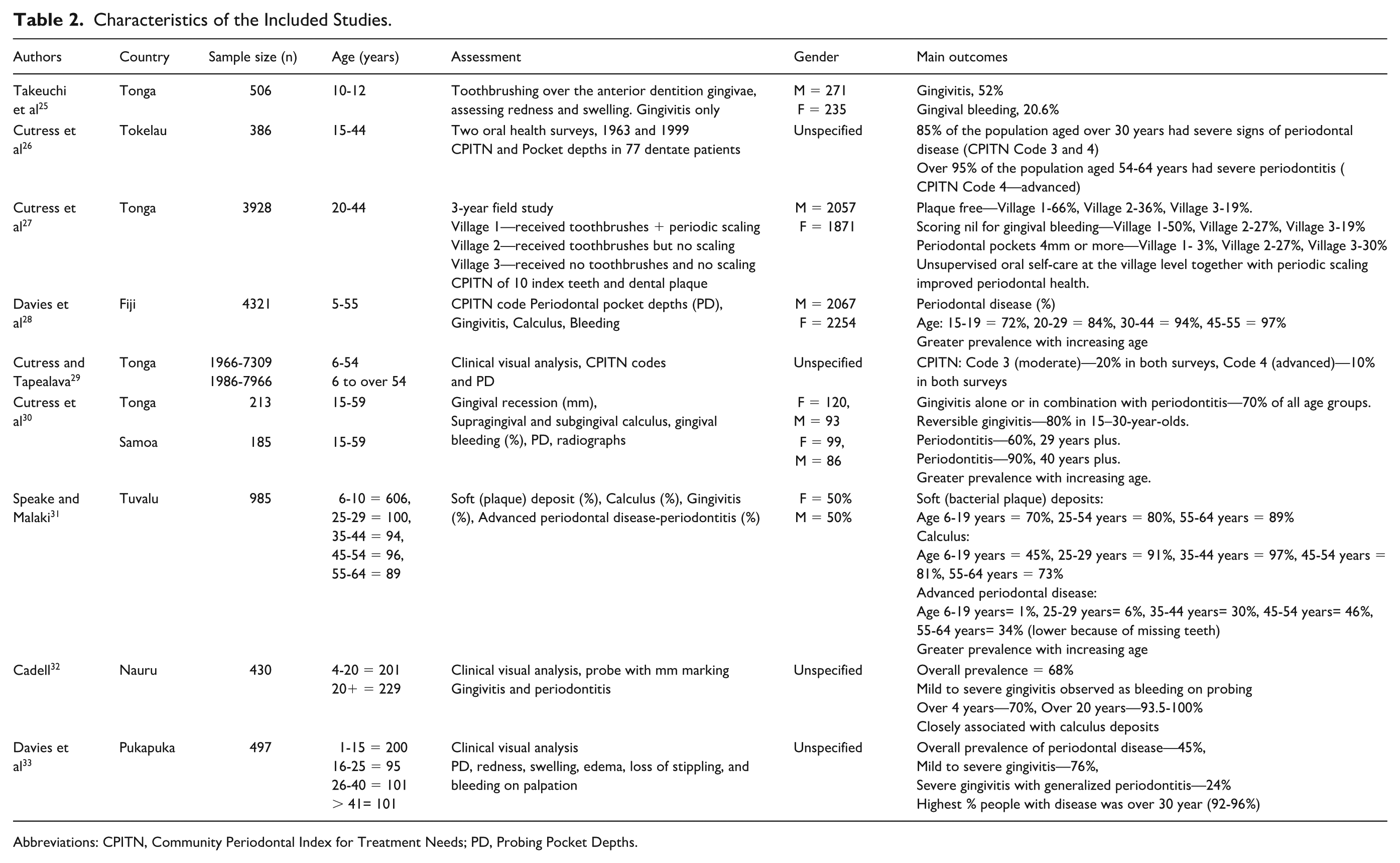
Abbreviations: CPITN, Community Periodontal Index for Treatment Needs; PD, Probing Pocket Depths.
Assessing Risk of Bias in Prevalence Studies. 24
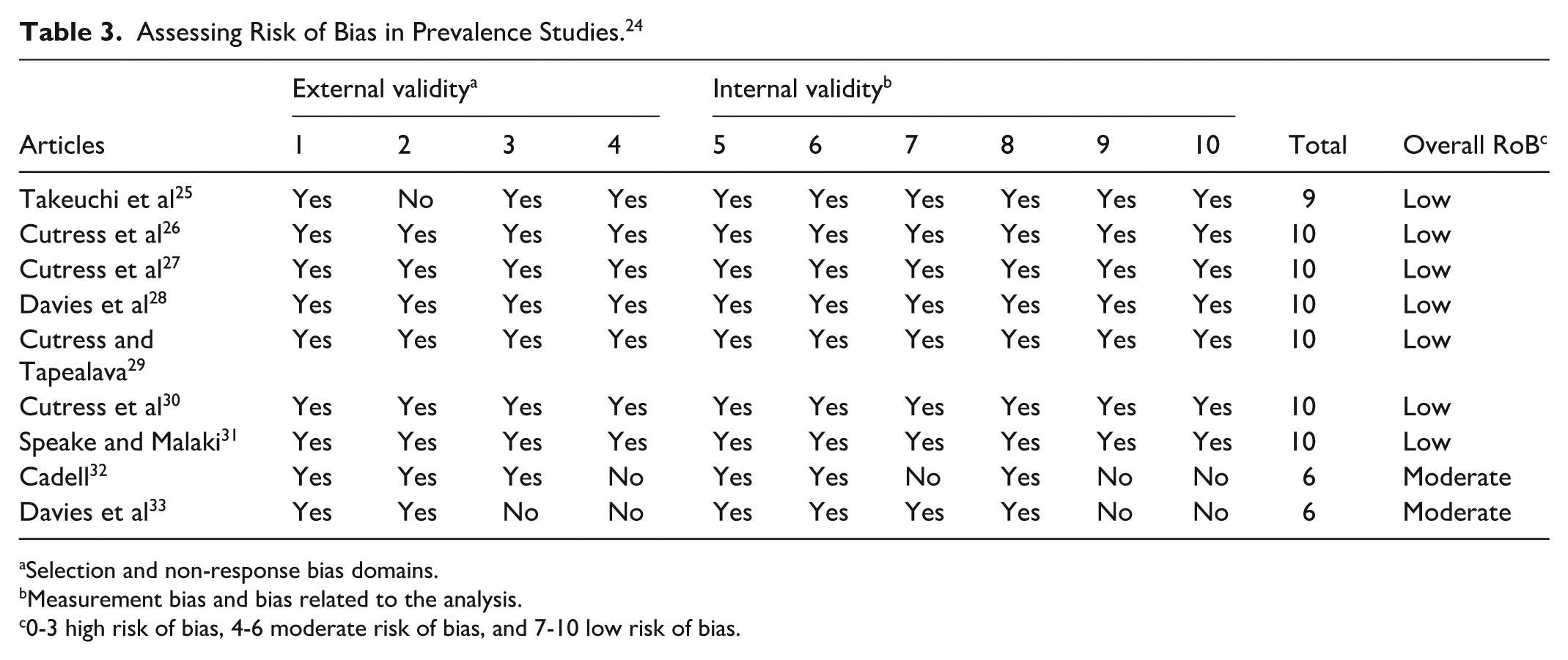
Selection and non-response bias domains.
Measurement bias and bias related to the analysis.
0-3 high risk of bias, 4-6 moderate risk of bias, and 7-10 low risk of bias.
One of the early studies compared periodontal disease in Tongan and Samoan population aged 15 to 59 years. 30 Multiple periodontal disease features were recorded, and 70% of all age groups were reported to have some form of periodontal disease. 30 Authors reported that the overall periodontal condition in both regions was similar but more prevalent at an earlier age in Tonga. The scores for all criteria were lower for females than males in both countries. In a later study in Tonga, a 3-year (1986-1989) community-based adult (20-44 years) periodontal disease preventive program was conducted involving three villages. 27 The baseline data collected in 1986 used a CPITN probe on the 10 index teeth. 34 While one village received oral hygiene aids and periodontal health education along with periodic ultrasonic dental scaling, village 2 received the same intervention except for dental scaling with village 3 as control (no hygiene packages or dental scaling). Dental plaque-free surfaces were reported to be at 66% with 50% of teeth recording no gingival bleeding in village 1 and 36% in villages 2 (27% no bleeding) and 3 (19% no bleeding). In relation to periodontal pockets, patients in village 3 presented a significantly higher number (30%) of periodontal pockets of 4 mm or more compared with village 2 (27%) and village 1 (13%). 27
The largest study included in this review compared oral conditions in Tongans over two national surveys. 29 In 1966, 7309 subjects, about 9.5% of the population, were examined, while 7966 subjects were examined in 1986. Overall, 20% of the population was assessed to have moderate periodontitis, compared to 10% with advanced periodontitis. More recently, the Tonga dental department conducted the oral disease preventive program for children called the MaliMali (Smile) Program.25,35 Apart from other investigations, a gingivitis and bleeding on probing was recorded. 25 In this study, 52.0% had features of gingivitis and 20.6% had gingival bleeding. 25
A Fijian national oral health survey conducted over the period 1985 to 1986 reported on the periodontal disease prevalence. 28 The criteria and method of examination in these surveys were based on the World Health Organization (WHO) manual of Oral Health Surveys—Basic Methods (1977 edition). 36 It was noted that periodontal disease affected about 60% of the study population aged 15 to 57 years. They reported moderate to severe disease with 14% of those over 30 years of age had advanced disease. While 74% of patients over 55 years had calculus, 18% had periodontal pockets of 4 to 5 mm, ie, CPITN code 3 and 2% had deep pockets 6 mm or more, ie, CPITN Code 4. In addition, 73% to 98% of adults required periodontal care, oral hygiene instructions, and scaling. 28
Another study from Tuvalu involved 985 people and reported on periodontal disease and its consequences. 31 Teeth were lost due to periodontal disease as one grew older and was significant between 45 and 54 years of age. Periodontal treatment needs commenced at about 10 years of age with full maxillary and mandibular dental clearances (extractions) commencing at 19 years of age. This increased to about 50% of the older age group with partial denture needs increasing in the 25- to 29-year age group. 31 A similar study based in Tokelau reported on a survey of 386 people (about 14% of the population), in two oral health surveys conducted in 1963 and 1999. 26 Although only 77 were dentate subjects were assessed for periodontitis, 95% of those aged 54 to 64 years were found to be having severe periodontitis.
One of the older studies conducted by Davies reported on the dental conditions of the PukaPuka Island (Danger Island) population in the Cook Islands. 33 The grading of periodontal disease included the presence or absence of different severities of gingivitis with associated generalized periodontitis. Overall, the prevalence of periodontal disease was noted to be at 45%. Of this, 76% were mild to severe gingivitis, while 24% were severe. Over 92% had supragingival and subgingival calculus in the over 40-year age group with males and females being equally affected. 33 Similar periodontal findings were reported in Nauru population. 32 It was noted that 70% of those more than 4 years and 90% of those more than 20 years had mild to severe gingivitis.
Risk of Bias
The risk of bias assessment revealed seven studies with low risk and two with moderate risk (Table 3). The older studies conducted in 1956 and 1959 showed the moderate risk of bias due to a significant lack of details in the methodology and choice of assessment protocol that utilized clinical assessments conducted visually or with minimal description of the assessment protocol.
Discussion
This systematic review was conducted to assess the prevalence of periodontal disease in the eight South Pacific Island countries, based on the limited literature available. Nine studies were identified that reported on the prevalence ranged from 20% to 100% with the greater prevalence in the 45- to 55-year age group and increased with advancing age in all countries. This is an expected finding, as periodontal disease is a chronic disease, and if untreated, it is expected to cause progressive deterioration as one grows older. 37
The WHO at the 74th World Health Assembly has brought attention to Oral Health and alluded to periodontal disease as a non-communicable disease (NCD) affecting about 796 million people globally. 3 The main regions affected are the countries in South-East Asia and the Western Pacific region (our area of interest), which are the worst affected. These countries depend on experts and funding mainly from New Zealand and Australia through the New Zealand Department of Foreign Affairs (NZDFAT) and the Australian Department of Foreign Affairs, respectively. This highlights the need for the Pacific community public health unit to take a leading role in advising member countries in relation to oral disease surveillance, especially periodontal disease prevalence studies to effectively manage periodontal disease in the South Pacific. 38 The limited number of dental officers locally adds to the challenge in conducting prevalence studies in the South Pacific. For example, some island countries such as Niue have two dental officers providing oral health care for their population (2000 inhabitants) and their focus is mainly on primary dental care. 39 Member states have been called upon to integrate oral health into their national health policies, improve their workforce models for oral health services, and ensure surveillance and monitoring of oral diseases. 40
A sustainable and significant collaborative effort is needed in the region to improve oral health and access to dental services in the region. Organizations based in the region such as the International College of Dentists (ICD), Section VIII, comprising Australia, New Zealand, and the South Pacific have recently set up the South Pacific Liaison Committee to provide much-needed support and expertise to the island nations. In addition, the chief dental officers of the South Pacific Island nations have recently initiated the Suva Declaration 2023 as part of the Oral Health Pacific Islands Alliance (OPIA) to address oral health which includes periodontal disease and are currently developing a memorandum of understanding with ICD to work toward improved oral health in these countries. 37
A significant lack of periodontal disease prevalence studies in the South Pacific Island countries was noted within the review with the most recent study published in 2012. This can be attributed to a lack of local expertise, funding, as well as inter-and-inter-country geo-isolation making access a significant barrier. Tropical inclement weather contributes to difficulties and restrictions in performing prevalence studies as many of the islands lack airports or airstrips and are reliant on marine transport for travel. To address the limitations due to geo-isolation, the WHO have also advocated the use of teledentistry services. 41 Building local capacity for periodontal disease management, as part of in-service training, can also aid in achieving optimal periodontal health for the population. This is supported by Finau, who emphasized that the dentists’ training programs should occur within their home countries in the Pacific region. 42 It was reported that overseas education was deemed unsuitable as many dentists chose not to return to their country, and the training curricula did not consider the needs of the Pacific countries. Consequently, a dentists’ training program delivered within their home countries in the Pacific region is preferred. 42 This could be achieved by a combination of remote learning initiatives and on-site training blocks (weeks of intense hands-on training) to ensure that the island nations’ workforce and service delivery are least affected while upskilling dental practitioners.
Notably, no studies in the South Pacific Island countries proposed or developed therapeutic and preventive strategies for managing periodontal disease in their respective study populations. When comparing the prevalence to a developed country like the United States, the prevalence of periodontal disease was less compared to the South Pacific islands. A study reported that over 47% of the population between 30 and 65 years were suffering from periodontitis, while for those over 65 years, 64% of the population had either moderate or severe periodontitis. 43 While comparing to a relatively similar demographic region from the Kolar district in India, this revealed that the prevalence was 95.4% and similar to that reported in South Pacific Island countries. 44 Indigenous populations are known to have a higher prevalence of periodontal disease compared to non-indigenous populations. 45 These variations call for a change in approach to develop strategies to evaluate the prevalence of a disease and include approaches to prevent it, with ongoing international collaboration and partnerships between academia and national health departments. 46 This collaboration is expected to build both clinical and public health capacity for local empowerment and strengthen their health systems in the planning and management of periodontal disease. 47
The limited number of studies in the region and the lack of optimal utilization of periodontal assessments warrant further comprehensive oral health surveys to inform health policies including public health, preventive, and therapeutic interventions to manage periodontal disease. The high prevalence of periodontal disease in the 45- to 55-year-old age group in the South Pacific can be due to a multitude of reasons, including lack of periodontal care services, lack of regular oral care, and a patient approach that they present for dental care only in an emergency usually managed by dental extractions. There is a growing aging population and an associated increased incidence of elderly patients suffering from periodontitis, and their needs are to be addressed in the national oral health plan. 46 Further studies to improve periodontal disease management locally, as well as address its association with comorbidities such as diabetes mellitus and cardiovascular disease are needed.2,11
Historically, various approaches and protocols have been used in assessing and quantifying periodontal diseases in epidemiological and clinical studies. It is worth noting that the CPI, a modified version of CPITN, is generally preferred method of periodontal disease screening. 48 Clinical Attachment Level (CAL) also known as the Full Mouth Periodontal Attachment Level (FMAL) chart is usually used for more comprehensive assessment and treatment planning in a clinical setting. Interestingly, when the FMAL chart was used to assess the prevalence of periodontal disease in the US population, 47.2% of the population were found to suffer from this disease. 43 However, when the CPITN was used in the same population, and at the same time, only 27% of the population were affected. 43 Studies also highlighted that the CPI is not intended to replace the FMAL chart but to act as a simple screening tool that can be used to screen the extent of periodontal disease in each population. 49 Hence, CPI is recommended for future periodontal disease screening and prevalence studies in the South Pacific. The choice of assessment techniques reveals differing findings in relation to periodontal disease prevalence, which can influence health policy decisions.
The assessment of strengths and limitations of this systematic review reveals the varying methodological approaches used in the included studies. Across the studies, there was heterogeneity in periodontal examination protocols and the diversity in the case definitions across studies may introduce variability, complicating the interpretation of the prevalence rates. Nevertheless, the review relied on the PRISMA guidelines throughout the preparation and reporting of the review to minimize the risk of bias. In addition, the finding of this review should be contextualized carefully due the most recent study included in this review, involving the Tongan population was published 13 years ago. 30 Nevertheless, this systematic review, to our knowledge, is the first to provide an estimate of periodontal disease in the South Pacific countries and identifies the need for ongoing oral health surveys at regional and national levels using standardized assessment protocols.
Conclusion
Although only nine articles with varying methodology and significant heterogeneity were available, a need for further periodontal disease research in the region is evident. Use of a standardized assessment protocol such as CPI for further studies in the South Pacific would be critical. In addition, development of local resources and targeted preventive strategies to improve the periodontal health of the population in the South Pacific Island countries are needed. Although the most recent study eligible for inclusion in this review was published over a decade ago (in 2012), the findings of this review can inform public health, clinical, and community stakeholders of the need for workforce strategies for managing periodontal disease in their respective populations.
Footnotes
Ethical Approval
Ethical approval for this type of study is not required by our institute.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.