
Abstract
Aims:
Psychotherapy is a widely used treatment for mental disorders, but whether it also improves employment and other labour market outcomes remains inconclusive. This study examined the effectiveness of a nationwide subsidized psychotherapy programme using extensive register-based data.
Methods:
The sample consisted of individuals who applied for rehabilitative psychotherapy in Finland in 2009–2012 (n = 35,083). Prior to 2011, some applications were rejected due to the limited budget that the central government provided for the programme. From 2011, all eligible applicants were granted rehabilitation. We used propensity score matching to create balanced samples of those who received a negative decision in 2009–2010 (n = 2047) and those who were granted rehabilitative psychotherapy in 2011–2012 (n = 12,046) in terms of their sociodemographic background characteristics, prior labour market attachment and health status.
Results:
We found that compared to the applicants who were not accepted to the programme, the granted applicants with similar background characteristics had, on average, a six-percentage-point higher employment rate, €2100 higher annual earnings and a six-percentage-point lower probability of becoming a disability benefit recipient five years after their first application. Further sensitivity analyses confirmed that these results were not biased, for example, by differences in macroeconomic conditions during the follow-up.
Conclusions:
Background
Mental illnesses are one of the leading reasons for long-term and permanent work disability. In OECD countries, mental disorders account for 30–40% of disability benefit caseloads and these numbers have increased over time [1]. Poor mental health leads to earnings losses, weak labour market attachment and increased work absences [2,3].
Psychotherapy is a widely used treatment for mental disorders [4], but whether it also improves employment and other labour market outcomes remains inconclusive. Prior meta-analyses on randomized-controlled studies show that psychological interventions have a small positive effect or no effect on return to work [5,6]. Most previous studies of occupational outcomes, however, have been based on relatively small samples or focused on specific interventions [5–10]. The availability and providers of psychotherapies vary in different countries, as do the possibilities for reimbursements [11]. Different measures have been taken to improve the access to care, but many countries still have shortcomings in their provision of psychotherapeutic treatments and their follow-up [12]. It is, therefore, crucial to obtain evidence on the effectiveness of treatment in different country contexts and in larger populations. Some evaluations are available from the US, Britain and the Nordic countries, suggesting that psychotherapy improves employment outcomes [13–15]. Our study contributes to this scarcely researched field by studying a Finnish nationwide subsidized psychotherapy programme using extensive register-based data.
In Finland, public healthcare, arranged by municipalities and hospital districts, is responsible for organizing mental healthcare [16]. A large part of psychotherapy, however, is provided by the private sector [17]. The Social Insurance Institution of Finland (KELA) compensates the costs of rehabilitative psychotherapy, which aims to improve patients’ work ability and labour market prospects. Before 2011, KELA compensated the expenses of psychotherapy according to a limited annual appropriation funded by the central government. In 2011, the provision of psychotherapy became statutory, and it is now available to all eligible applicants – although all applications are still evaluated by KELA. The principles and eligibility criteria of rehabilitative psychotherapy did not notably change [18]. We based our analysis on this change in the law. Before 2011, budgetary reasons led to some applications being rejected, while since 2011, all eligible applicants were granted psychotherapy. Thus, it can be assumed that a fraction of applicants who were denied access to psychotherapy before the policy change in 2011 would have been granted psychotherapy if they had applied in the later period. Using propensity score matching, we sought to find counterparts for the rejected applicants prior to 2011 from among those who were granted psychotherapy after the policy change, based on relevant background characteristics. It is reasonable to assume that a comparison group with similar background characteristics can be found especially from this pool of applicants who were granted psychotherapy after the policy change. By comparing the matched rejected and granted applicants, we analysed whether the programme achieved its goals – that is, whether the participants of the programme had better labour market attachment during the follow-up of five years than the rejected applicants. Because a limitation of this research design was that the treatment and control group were followed up in partly different calendar years and macroeconomic conditions, we also made several additional comparisons as sensitivity analyses to account for the potential confounders.
Methods
Study design
The study was based on Finnish administrative register data on individuals who applied for KELA psychotherapy subsidy between years 2009 and 2012. The costs of therapy may be subsidized by KELA as rehabilitative treatment (maximum of three years and 200 sessions) if the following minimum eligibility conditions are met: the applicant is 16–67 years old, has a diagnosed mental health problem hampering the coping with work or studies, has already received appropriate care for three months and has a plan for rehabilitation with a statement from a treating psychiatrist [19]. Even if the above-listed eligibility conditions are met, KELA can deny the access to the programme if the candidate’s prospects to benefit from the programme are evaluated to be weak, or before the policy change in 2011, if the budget for the programme had run out. In the evaluation, KELA considers, for example, applicants’ life situation and motivation to participate in psychotherapy [20]. Before 2011, the limited funding was targeted towards those who, according to medical evaluation, were most in need of rehabilitation to cope with work or studies [18]. The aim was to secure the continuation of ongoing psychotherapies, and the allocation of funds to new clients was based on regional and monthly quotas (Eija Lehtinen and Veli-Matti Vaden, KELA, October 2019, personal communication). Before 2011, the limited budget thus denied applicants with certain characteristics that would have been granted after the policy change. For these reasons, we constructed the main comparison groups from those who were denied psychotherapy before the policy change in 2009–2010 and those who were granted after the policy change in 2011–2012 and followed up their labour market attachment for five years.
Data and variables
We utilized data from KELA for 2007–2017, combined with background and employment data from Statistics Finland. The sample (n = 35,083) was restricted to individuals who applied for rehabilitative psychotherapy between 2009 and 2012 for the first time (27,497 individuals). It was further restricted to individuals who had full register data for five years before and five years after the first application round in Statistics Finland and did not die or retire on old age pension during these years (n = 26,053). After we included only individuals who were 18–60 years old in their first application year, 24,795 individuals remained in the sample. In the main analysis, we matched individuals who had been denied psychotherapy before 2011 to a group of individuals who were granted psychotherapy in 2011 or after.
This study was approved by KELA and Statistics Finland, and the data were combined and anonymized by Statistics Finland for research purposes. According to the Finnish legislation, the review of the ethics committee and consent to participate is not required in research based on only registry data.
Access to rehabilitative psychotherapy
Information on applications to rehabilitative psychotherapy and the decisions received (granted vs denied) was based on registers of KELA. Individuals can make several applications to rehabilitation within a year. We defined acceptance as an affirmative decision on any of the applications sent during the first application year, otherwise we classed them as a rejection.
Dependent variables
The labour market outcomes were measured with three variables based on register data from Statistics Finland. These variables included disability benefits (a dummy indicating whether or not the person received permanent or temporary disability benefits at the end of each year), employment status (a dummy indicating whether or not the person had any employment spells as a wage-earner or was self-employed within a year), and income as a sum of wage and salary, and self-employment income (measured at 2017 level deflated using cost-of-living index). Disability benefits are usually paid after work disability has continued more than one year [21].
Background variables
We matched the groups based on the sociodemographic factors available from Statistics Finland. In addition to gender and age in the application year (18–25, 26–35, 36–45 and 46–60 years), information on the following variables was included from the year preceding the application: highest education (basic, secondary and tertiary education), labour market status (indicating individuals’ situation during the last week of the calendar year and categorized into four groups: employed, unemployed, student and other), place of residence (southern, southwest, eastern, western and northern Finland). We also adjusted for the level of the outcome variables (employment status, earnings and receiving disability benefits) in years 1–4 preceding the application.
Main diagnosis in the application to the rehabilitation retrieved from the KELA registers was categorized into four groups: mood disorders (F30–39), anxiety disorders (F40–49), other mental health problems (other F-diagnoses) and other diseases [22]. A dummy variable indicated if the applicants had any KELA compensated sickness absences (lasting >10 working days) in the year prior to the application year. Another variable based on KELA registers indicated whether the applicant had purchased any antipsychotics, anxiolytics, hypnotics and sedatives, or antidepressants (ATC codes N05A, N05B, N05C, N06A) [23], and whether the individual was entitled to special reimbursement on the basis of psychosis or other severe mental health problems (F01, F03, F06.0–F06.3, F20–F25, F28, F29, F30.1, F30.2, F31, F32.3, F33.3, F84, G10, G20, G30.0, G30.1, G30.8, G30.9, G31.0, G35, G40.9) [24] in the year preceding the application year. For descriptive evidence, information on sickness absences and psychopharmaceutical purchases were included also from two years preceding the application.
We also had information on municipal unemployment rates, the field of education and family characteristics a year prior to the application available from Statistics Finland, which we did not use in the main matching procedure. The field of education was categorized to nine categories (see Table I). Dummy variables indicated whether the individual had children under 18 living in their household and whether the individual was married/cohabiting.
Descriptive information on applicants of rehabilitative psychotherapy according to timing (pre = 2009–2010, post = 2011–2012) and decision on application.

Based on the classification of Statistics Finland, indicating individuals’ situations during the last week of the calendar year.
ICD-10 classification: mood disorders (F30–39), anxiety disorders (F40–49), other mental health problems (other F-diagnoses) and other diseases [22].
Statistical methods
We first describe the background characteristics of all applicants who applied to psychotherapy rehabilitation before and after the policy change and according to the decisions they received. We used propensity score matching to compare those with denied access (n = 2047) to rehabilitative psychotherapy in 2009–2010 to those who were granted rehabilitation in 2011–2012 (n = 12,046). As noted above, there was high selection to receive a positive decision for rehabilitation, as the treatment is targeted towards those who are evaluated to benefit from it in terms of their employment and education prospects. Propensity score matching ensures that the groups are more similar in terms of their observed characteristics. The reform strengthens the suitability of the method, creating randomness in who received treatment. Prior to the reform, a fraction of the rejected applications was due to the budget constraint set by the state and not subject to individual characteristics or suitability to take part in the programme.
The purpose was to create balanced samples of individuals denied and granted psychotherapy considering the most relevant factors measured before applying for rehabilitation – such as health conditions and previous labour market attachment – which are associated with both the treatment and later labour market attachment. As the group of denied applicants was much smaller than the group of granted applicants, we sought to find pairs for each denied applicant from the group of granted applicants. The matching algorithm thus calculated the propensity of each applicant to receive a negative decision based on variables measured in the first application year (gender, age and health diagnosis in the application), from the year preceding the first application (educational level, labour market status, region, sickness absences, psychopharmaceutical purchases and special reimbursement for severe mental health problems), and from 1–4 years preceding the first application (disability benefits, employment and annual earnings).
The propensity score was estimated using a logit model. The main analysis was based on matching five nearest neighbours with replacement and excluding cases without common support. The balance of covariates among the matched samples was estimated using standardized mean bias [25]. For comparison, we conducted analyses based on one nearest neighbour with a caliper value of 0.01.
We compared the difference of labour market attachment and work ability among the matched sample and reported the average treatment effect of being treated (ATET) in each of the five follow-up years with 95% confidence intervals. As the matching algorithm calculates the propensity of receiving denied decision, in practice, the ATET refers to the average treatment effect of being untreated. For the ease of interpretation, in the Results section we show graphically the situation of the granted group in comparison to the denied group. Information on the outcome variables in the fifth year prior to the first application was not included in the matching algorithm and served as a robustness point for the main outcomes. If the treatment assignment is not associated with the outcome variables measured before the first application and not used in the matching algorithm, we can be more confident that the post-treatment effects are not based on prior differences between the groups [26].
We also made the following sensitivity analyses. We included family covariates and municipal unemployment rates in the matching algorithm as additional covariates. In another analysis, we excluded one third of the originally rejected applicants who had been successful in later applications to psychotherapy and received compensated therapy sessions within the follow-up of five years.
We performed three additional comparisons to take into account that the treatment effect in the main analysis could be driven by differences in macroeconomic situation during the follow-up. First, we compared those who were granted access before the policy change to those who were granted access after the policy change. If the macroeconomic situation is not affecting the results, the differences between these groups should be small. Second, we compared applicants only from 2011 and 2012, after the policy change. After the policy change all denied applicants should be ineligible to the programme and the differences between the granted and the denied applicants should be larger. Third, we compared only applicants from 2009 and 2010, before the policy change. The benefit of this comparison is that the applicants were followed up in the same calendar years.
Lastly, in the main analyses, our aim was to find a comparison group for those who were denied psychotherapy before the policy change, and, thus, the results are generalizable to this population of denied applicants. In an additional analysis, we sought to find pairs for those who were granted rehabilitation after the policy change from among the smaller group of those who were denied access before the policy change. The purpose of this analysis was to detect whether the treatment effects are similar and generalizable to the population of granted applicants.
All propensity score matching analyses were conducted with Stata version 16 using PSmatch2 [27], and standard errors were calculated based on Abadie and Imbens [28].
Results
Descriptive results
Table I presents descriptive information on individuals, who applied for the rehabilitative psychotherapy for the first time in 2009–2012 and who met the inclusion criteria of this study described in the Methods section (n = 27,497). Before the policy change in 2009–2010, in total 11,379 individuals applied for psychotherapy for the first time, and 2047 of them were denied and 9332 were granted rehabilitative psychotherapy. After the policy change in 2011–2012, the number of applicants was 13,416, and 1370 of them were denied and 12,046 were granted rehabilitation. The proportions of affirmative decisions among those who applied for psychotherapy in 2009 and 2010 were 80% and 84%, respectively, whereas the proportions of successful applications after the law changed in 2011 and 2012 were 88% and 91%, respectively.
The background characteristics of the applicants had not markedly changed around the policy change in 2011 (Table I, columns 1–2). Thus, the change in law did not encourage markedly different individuals to apply for rehabilitation. In both periods, most of the applicants were women (76%), employed (68%) or students (19%).
In both periods, those who received an affirmative decision were more commonly women, employed and had tertiary education compared to the individuals whose applications were rejected (Table I, columns 3–6). The groups who received an affirmative decision were also quite similar in terms of covariates both before and after the law changed, while the differences among those with rejected applications were larger around the policy change. Figure 1 shows the means in the outcome variables over time among the accepted and rejected applicants with respect to the timing of their applications. The pool of rejected applicants changed after the policy reform. Those who were rejected in the later period had poorer labour market attachment than those who were rejected in the earlier period – that is, before the law changed.
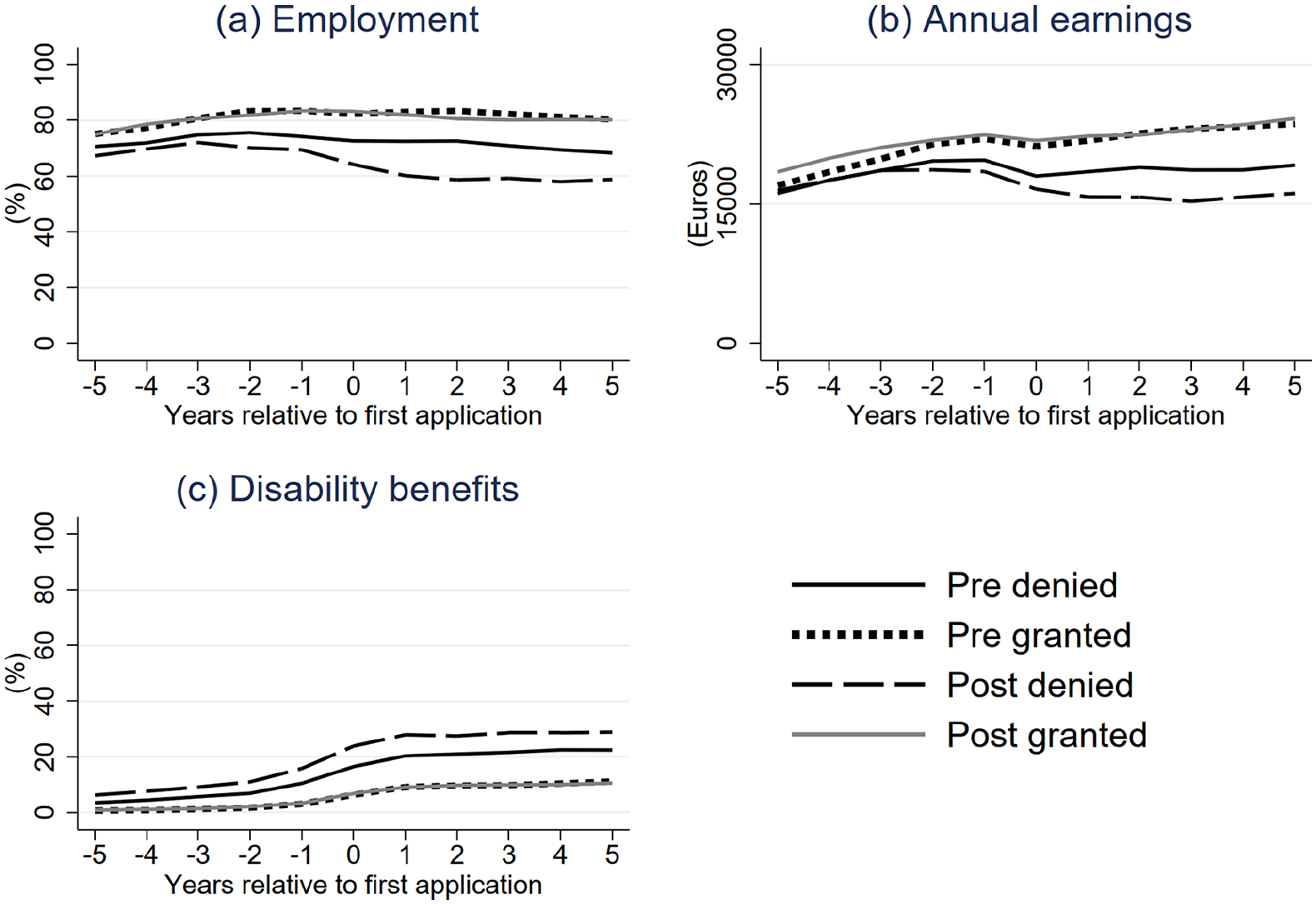
Annual employment rates (a), earnings (b) and proportions of disability benefit receivers (c) among applicants of rehabilitative psychotherapy according to timing (pre = 2009–2010, post = 2011–2012) and decision on application.
Those who were granted psychotherapy in their first application year had, on average, 111 compensated therapy sessions during the follow-up, while only 2% of them had no sessions at all. Most of the accepted applicants had therapy sessions already during the first application year (83%), and during the following three years (94%, 74%, 54%). In total, 41% of denied applicants reapplied, and one third of the originally denied applicants received compensated therapy sessions within the next five years.
Propensity score matching results
Propensity score matching enabled us to find pairs for 2039 rejected applicants in 2009–2010 from the pool of accepted applicants in 2011–2012 (Table II). The propensities for receiving a negative decision overlapped sufficiently between the groups of rejected and accepted individuals, and the distribution of the propensities were very similar in the matched sample (online Supplementary Figure a). The standardized mean bias in covariates decreased from 13.6% to 1.2% after matching, and remained below 5% for all covariates included in the matching algorithm (Table II). In addition, the distribution of field of education and the means of the municipal unemployment rates were quite balanced in the matched groups, although these variables were not explicitly included in the matching algorithm. On the other hand, those who received a negative decision were less commonly married or cohabiting (49%) or had children (33%) than the accepted applicants (54% and 39%, respectively). In a sensitivity analysis, we also included family variables and municipal unemployment rates in the matching algorithm.
Descriptive information on applicants of rehabilitative psychotherapy before and after policy change (pre = 2009–2010, post = 2011–2012) and in corresponding matched sample.

Variable not included in matching algorithm.
Based on the classification of Statistics Finland, indicating individuals’ situations during the last week of the calendar year.
ICD-10 classification: mood disorders (F30–39), anxiety disorders (F40–49), other mental health problems (other F-diagnoses) and other diseases [22].
Figures 2 and 3 show that the matched groups were similar in terms of employment, earnings and work ability five years prior to the first application year. However, some differences already emerged during the application year (year 0), as this was the year when the treatment group already had therapy sessions. Compared to the group of denied applicants, the accepted applicants had 2–6 percentage points higher employment rates during the follow-up, and the difference was statistically significant each year (Figure 3 and online Supplementary Table a). The accepted applicants also had higher annual earnings each year in the follow-up and the difference was statistically significant in the third, fourth and fifth year. At the end of the follow-up, the accepted applicants had, on average, €2100 higher annual earnings. Accepted applicants were also 5–6 percentage points less commonly on disability benefits at the end of each year in the follow-up, and the difference was statistically significant each year.
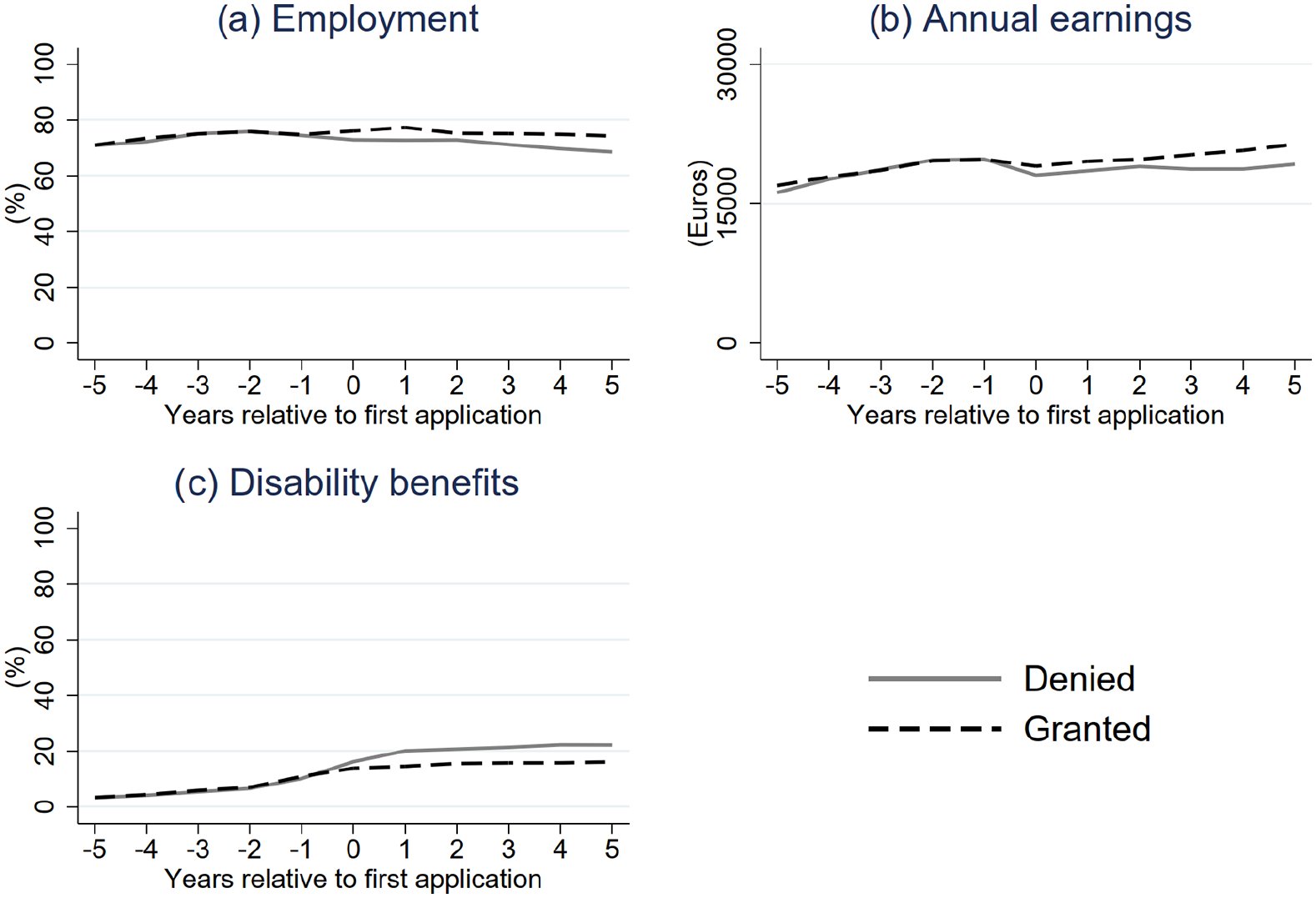
Annual employment rates (a), earnings (b) and proportions of disability benefit receivers (c) in matched sample.
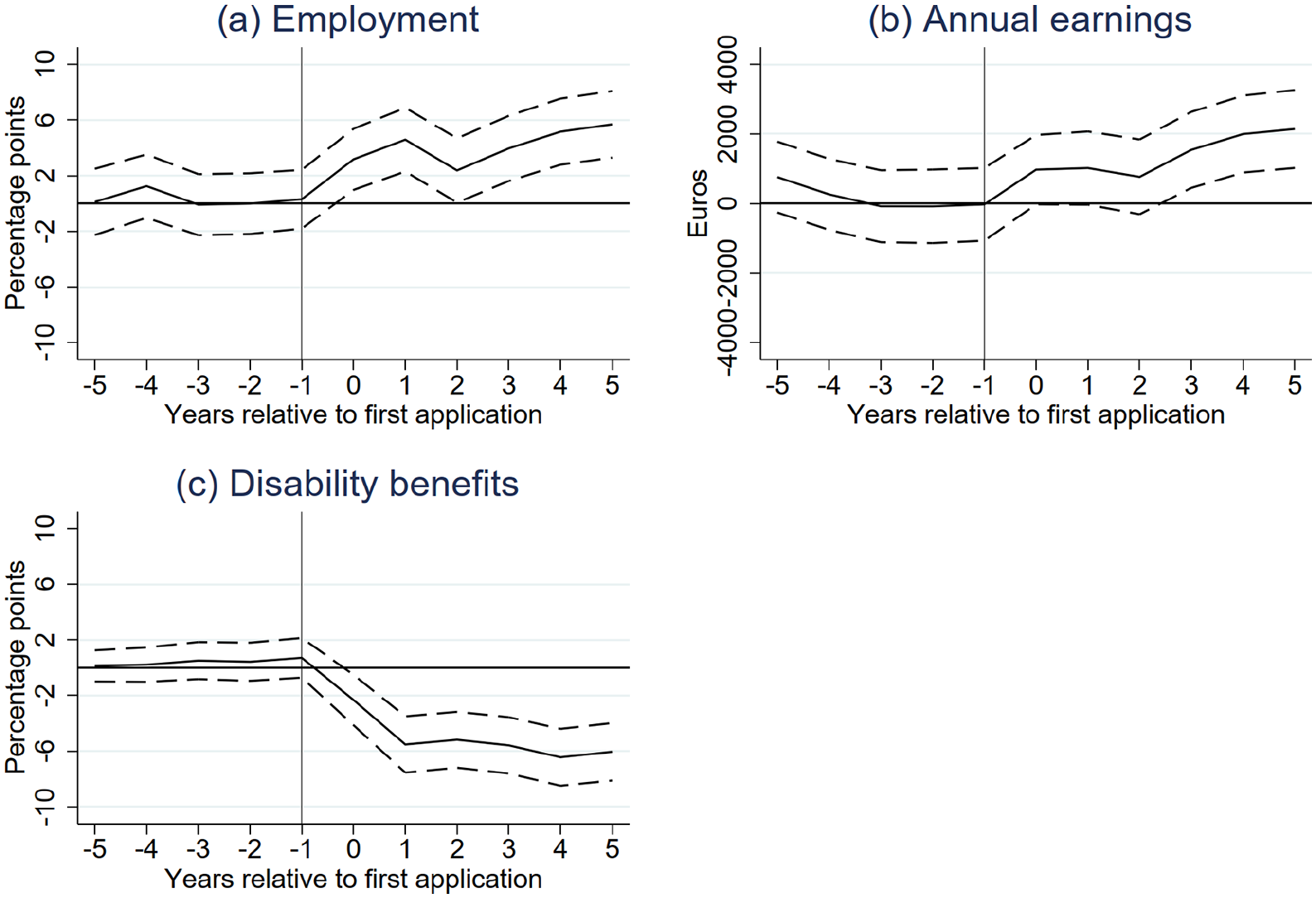
Difference in employment rates (a), earnings (b) and proportions of disability benefit receivers (c) in matched sample (granted vs denied) with 95% confidence intervals. In the matching algorithm, the propensity of receiving a denied decision is calculated and the figures report average treatment effect of being denied. To ease the interpretation, we show the estimates comparing the granted group to the denied group.
Sensitivity analyses
The results of the sensitivity analyses are shown in online Supplementary Table b. The results were qualitatively similar with 1:1 matching based on a caliper value of 0.01 and when additionally including family covariates and municipal unemployment rates in the matching algorithm. The treatment effects were stronger when excluding one third of the originally rejected applicants who had been successful in later applications.
Three additional sensitivity analyses were conducted to consider the differences in the macroeconomic situation during the follow-up. First, the differences between those who were granted access before the policy change and those who were granted access after the policy change were small in most of the time points. In some of the time points, those who were granted access before the policy change had higher employment rates and earnings. This finding mainly suggests that our main results may be an underestimation of the actual treatment effect. As expected, the treatment effects were larger in a comparison based on denied and granted applicants only from 2011 and 2012, after the policy change. The treatment effects were quite similar or stronger in the analysis including applicants only from years 2009 and 2010, before the policy change.
Lastly, we sought to find pairs for those who were granted rehabilitation after the policy change from among the smaller group of those who were denied access before the policy change. Compared to the main analysis, the treatment effects were similar but slightly smaller.
Discussion
This study analysed the effects of a nationwide psychotherapy rehabilitation programme on participants’ labour market attachment using comprehensive register-based data from Finland. The main finding was that compared to the applicants who were not accepted to the programme, the accepted participants with similar background characteristics had, on average, a six-percentage-point higher employment rate, €2100 higher annual earnings and were six percentage points less likely to be on disability benefits five years after their first application.
Our results contribute to prior research on the labour market effects of psychotherapy by extending the analysis to a nationwide programme and using register-based data during a five-year follow-up. The strengths of this study were its credible control group and its use of large register-based data, consisting of accurate information on the participants’ health and employment. The main results are qualitatively similar to those of prior studies with shorter follow-ups and different research designs [7,13–15]. As the target groups, programmes and outcome variables are somewhat different, it is not possible to directly compare the quantitative size of the effects to those in prior studies.
The identification of the effects was based on the policy change in 2011, which made rehabilitative psychotherapy a subjective right. Prior to 2011, a fraction of the applicants were denied rehabilitation because of limited funding. One limitation of our research design is the differences in the follow-up periods and macroeconomic situation between the treatment and control groups. However, there were no major changes in unemployment and unemployment rates or in the general macroeconomic conditions in Finland during the 2010s (online Supplementary Table c). Sensitivity analyses also confirmed that the treatment effects were not driven by a better macroeconomic environment in later years – that is, when the applicants who were accepted rehabilitation started psychotherapy and were followed up. The results were also verified by including additional control variables and using a different matching algorithm.
Although the analysis was based on the effects of granted versus denied access to rehabilitation, equivalent to intention-to-treat effects, in practice, the results can also be interpreted as actual treatment effects. Only 2% of the applicants who received an affirmative decision had no compensated therapy sessions in the following five years. However, one third of the originally rejected applicants also had compensated therapy sessions during the five-year follow-up. Thus, the main results partly show benefits of starting psychotherapy earlier rather than in later years. Early access to psychotherapy may improve labour marker attachment, which, in turn, may further strengthen the effects of the therapy.
It is also possible that the rejected group had some psychological treatment in the primary care, in occupational healthcare or at their own expense, but this information is not available in nationwide registers. Given that it is quite expensive to have psychotherapy without the reimbursement, we can expect that the rejected applicants did not commonly have long-term psychotherapy. In general, only a small proportion of individuals with mental disorders receive psychotherapeutic treatments [29,30]. A large part of the costs is still covered by the individual and the supply of therapists is too limited for the demand, partly because their education is costly. These issues are currently receiving substantial media attention and a citizens’ initiative for guaranteed therapy and an initiative related to education of psychotherapist are under consideration in the parliament of Finland.
This study compared individuals who had applied for rehabilitative psychotherapy but of whom KELA evaluated only some as suitable for treatment. Some of the applicants were rejected due to budgetary reasons, while others would have received a negative decision even without the budget limit. Although we took several relevant background characteristics into account in the matching analysis, it is possible that a substantial proportion of the rejections both before and after the policy change was related to unobserved applicant’s characteristics – such as motivation to participate in the therapy and apply for labour market – which are associated with poorer employment outcomes compared to the granted applicants. However, it is also possible that the decisions of KELA include some irregularities at any time, related to, for example, regional variations in practices and interpretations of the applicants’ situations. For example, the denial rates were larger in southern Finland compared to other regions, which is not explained by the observed characteristics of the applicants. An important issue for all applicants also is that the treating psychiatrist had supported the application to receive psychotherapy. In the first-stage evaluation, the most severe mental health conditions requiring more immediate or medication-based treatment are excluded from the applicant pool. In addition, the required three-month treatment period before being eligible to apply excludes individuals with only mild symptoms who may recover spontaneously without intervention.
Conclusions
This quasi-experimental study showed that compared to denied application, access to subsidized rehabilitative psychotherapy was significantly associated with higher employment rates and earnings and lower risk of work disability. Although several relevant background factors were included in the analysis, it is possible that some unobserved factors explain both access to psychotherapy and subsequent labour market outcomes. Future studies are needed, for example, to analyse the effectiveness of this kind of interventions among different subgroups and consider the length of the therapy in relation to its outcomes.
Supplemental Material
sj-pdf-1-sjp-10.1177_14034948221074974 – Supplemental material for Effects of rehabilitative psychotherapy on labour market success: Evaluation of a nationwide programme
Supplemental material, sj-pdf-1-sjp-10.1177_14034948221074974 for Effects of rehabilitative psychotherapy on labour market success: Evaluation of a nationwide programme by Laura Peutere, Terhi Ravaska, Petri Bӧckerman, Ari Vӓӓnӓnen and Pekka Virtanen in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
We thank Henri Salokangas for helpful comments on the manuscript.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Finnish Work Environment Fund (180048 to LP and TR) and the Yrjö Jahnsson Foundation (20187100 to LP and 20187103 to TR]. AV was also supported by KELA (18/26/2020).
Data availability
The data used in this study are not publicly available. This study was approved by KELA and Statistics Finland. Since April 2020, the Data Permit Authority Findata reviews all requests that ask for the combining data from different registers.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.