
Abstract
Background:
A growing proportion of children born in Europe are born to immigrant parents. Knowledge about their health is essential for preventive and curative medicine and health services planning.
Objective:
To investigate differences in diagnoses given in secondary and tertiary healthcare between Norwegian-born children to immigrant and non-immigrant parents.
Methods:
Data from the Medical Birth Registry of Norway, the Norwegian Patient Registry and Statistics Norway were linked by the national personal identification number. The study population included children born in Norway aged 0–10 years between 2008 and 2018 (N=1,015,267). Diagnostic categories from three main domains of physical health, given in secondary or tertiary care; infections, non-infectious medical conditions and non-infectious neurological conditions were included from 2008 onwards. Hazards of diagnoses by immigrant background were assessed by Cox regressions adjusted for sex and birth year.
Results:
Children of immigrants generally had higher hazards than children with Norwegian background of some types of infections, obesity, nutrition-related disorders, skin diseases, blood disease and genital disease. Children of immigrants from Africa also had higher hazards of cerebral palsy, cerebrovascular diseases and epilepsy. Conversely, most groups of children of immigrants had lower hazards of acute lower respiratory tract infections, infections of the musculoskeletal system, infections of the central nervous system, diseases of the circulatory system, hearing impairment, immune system disorders, chronic lower respiratory disease and headache conditions.
Conclusions:
Children of immigrants did not present with overall worse health than children without immigrant background, but the distribution of health problems varied between groups.
Introduction
Child health is important for current wellbeing and function, but also for future adult health, development and opportunity across different spheres of life. Both psychosocial and material circumstances in early life are important contributors [1].
In Europe, a significant proportion of children have immigrant background, and this proportion is expected to rise in the coming decades [2]. Some of these children have migrated themselves, but the majority are born in the host country. Children born to immigrant parents are not directly exposed to negative health effects of migration. However, their health may still be influenced by the situation of their parents, which may include parental trauma, socioeconomic disadvantage, language barriers, or lack of knowledge of the healthcare system in the host country. There is limited knowledge about the health of this group. Such knowledge is essential for both preventive and curative medicine and health services planning, and may also provide an indication of the conditions of the children’s upbringing and more broadly their quality of life.
Most studies from high income countries categorise children by the parents’ country of origin, but do not distinguish between children with and without a migration experience. These studies, which have generally focused on one or a just a few conditions, suggest that children of immigrants are at increased risk of overweight and obesity [3–6], type 1 diabetes [7], vitamin D deficiency [8], skin diseases [9, 10] and tuberculosis [11] compared with other children. The incidence of cancer among children with immigrant background relative to other children varies with the type of cancer, but there are indications of higher mortality [12].
In Norway, 12% of children under the age of 18 years are born to immigrant parents [13]. The largest proportion is born to parents from Asia, followed by the European Union (EU) and Africa. In a Norwegian study of the use of primary healthcare services and medication use, Norwegian-born children of immigrants differed from children with Norwegian-born parents in several ways. They had higher proportions with respiratory tract infections, renal, oral and gastrointestinal conditions, eczema, fever and nausea, but lower proportions with attention-deficit disorder, anxiety, allergy and neurological and musculoskeletal conditions [14, 15]. Further, Norwegian-born children to immigrant parents had lower use of most kinds of medicines than children of Norwegian-born parents [14].
Differences in health-seeking behaviour between immigrant parents and native-born parents may vary between secondary/tertiary and primary healthcare. There may also be differences in how healthcare workers refer children with and without immigrant parents to secondary/tertiary healthcare. Further, diagnoses given in secondary/tertiary healthcare may inform us about conditions requiring treatment beyond what is offered in primary care, and which are often chronic conditions. In Norway, primary care has a key role in diagnosis and treatment of a range of diseases, but is also the gatekeeper to secondary/tertiary healthcare. This means that patients must approach primary care in order to be referred to secondary/tertiary healthcare.
In this article, we utilise Norwegian register data from secondary and tertiary healthcare to investigate differences in diagnoses between Norwegian-born children of immigrant and non-immigrant parents. We include children aged 0–10 years, as the youngest children are the ones most influenced by the parents’ involvement, decisions and health-seeking behaviour. We focus on physical health; infections, non-infectious medical conditions and non-infectious neurological conditions, and include data from the Norwegian Patient Registry from 2008 to 2018.
Methods
Study population
The Norwegian Patient Register [16] comprises all diagnoses given in secondary and tertiary healthcare, with individual-level data from 2008 onwards. We include diagnoses given in secondary and tertiary healthcare from 2008 to 2018. The study population included children who were born in Norway and who were 0–10 years of age between 2008 and 2018 (i.e. children born in 1998–2017). The number of years of follow-up varied by year of birth. For example, children born in 1998 had one year of follow-up (aged 10 years in 2008), children born in 2008 had 10 years of follow-up (2008–2018) and so on. Data from the Medical Birth Registry of Norway and the Norwegian Patient Registry were linked by the national personal identification number, and also to data from Statistics Norway on immigrant background and parental country of origin. We excluded those who had one immigrant parent and one Norwegian-born parent (N=142,332), those who were registered as emigrated (data on emigration year not available) (N=23,744), children who were registered as stillborn (N=9010) or late abortions (N=4520), children who died prior to 2008 (N=2176), as well as those without information on immigrant background (N=867), leaving a sample of 1,015,267 children for the analysis.
Variables
The Norwegian Patient Registry contains Inter-national Classification of Disease, version 10 (ICD-10) diagnoses given in secondary and tertiary healthcare (both inpatient and outpatient) from 2008 onwards. We included 37 diagnostic categories from three main domains of physical health; infections, non-infectious medical conditions and non-infectious neurological conditions (ICD-10 diagnostic codes are shown in Supplemental Table I). In the present study, children who had a specific diagnosis from secondary or tertiary healthcare at least once during the specified age and time frame were classified as having the respective diagnosis.
Children born to two Norwegian-born parents are referred to as having ‘Norwegian background’. Among Norwegian-born children to immigrant parents, region of origin was classified according to national standards [17], using information about parents’ country of birth (if different; mother’s); ‘EU/European Economic Area (EEA), Oceania, United States of America (USA) and Canada’, ‘Europe outside the EU/EEA’, ‘Asia’, ‘Africa’ and ‘Latin America’.
The percentages receiving each diagnosis according to region of origin were reported. In Cox proportional hazard regressions, hazard ratio (HR) with 95% confidence intervals for each diagnosis were calculated for region of origin compared with children of Norwegian background, adjusted for sex and year of birth. Each participant was followed from 2008 or year of birth (if later than 2008) until year of diagnosis, year of death, year of reaching 10 years of age (if earlier than 2018), or until the end of 2018. Analyses were performed using STATA 16.
Results
The sample comprised 1,015,267 children, of whom 13.6% were born to immigrant parents (Table I). The largest percentages of children of immigrants had parents from Asia, followed by EU/EEA/Oceania/USA/Canada and Africa. The percentage of children receiving at least one of the included diagnoses in secondary or tertiary care between 2008 and 2018 varied between 32.4% among children with a background from EU/EEA/Oceania/USA/Canada and 43.5% among children with a background from Africa (Table I). Children with parents from Africa also had the highest percentage with three or more diagnoses (Table I). Percentages who received different diagnoses by region of origin are shown in Table II.
Numbers of children by regional background, and percentages with one or more and three or more diagnoses.
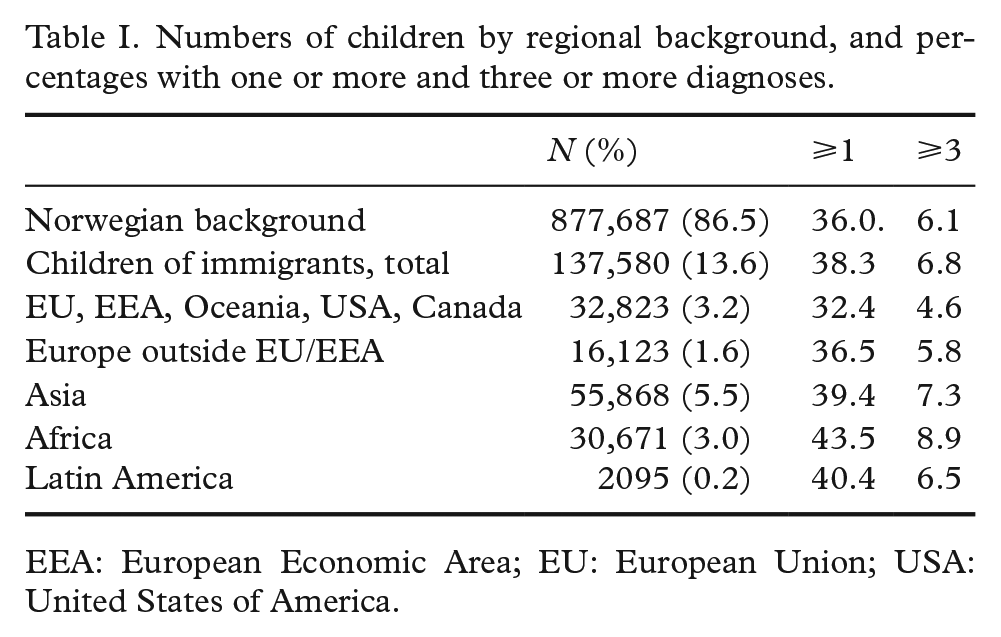
EEA: European Economic Area; EU: European Union; USA: United States of America.
Numbers and percentages with diagnosis given in secondary and tertiary healthcare between 2008 and 2018 among children aged 0–10 years, by parental region of origin, N (%).
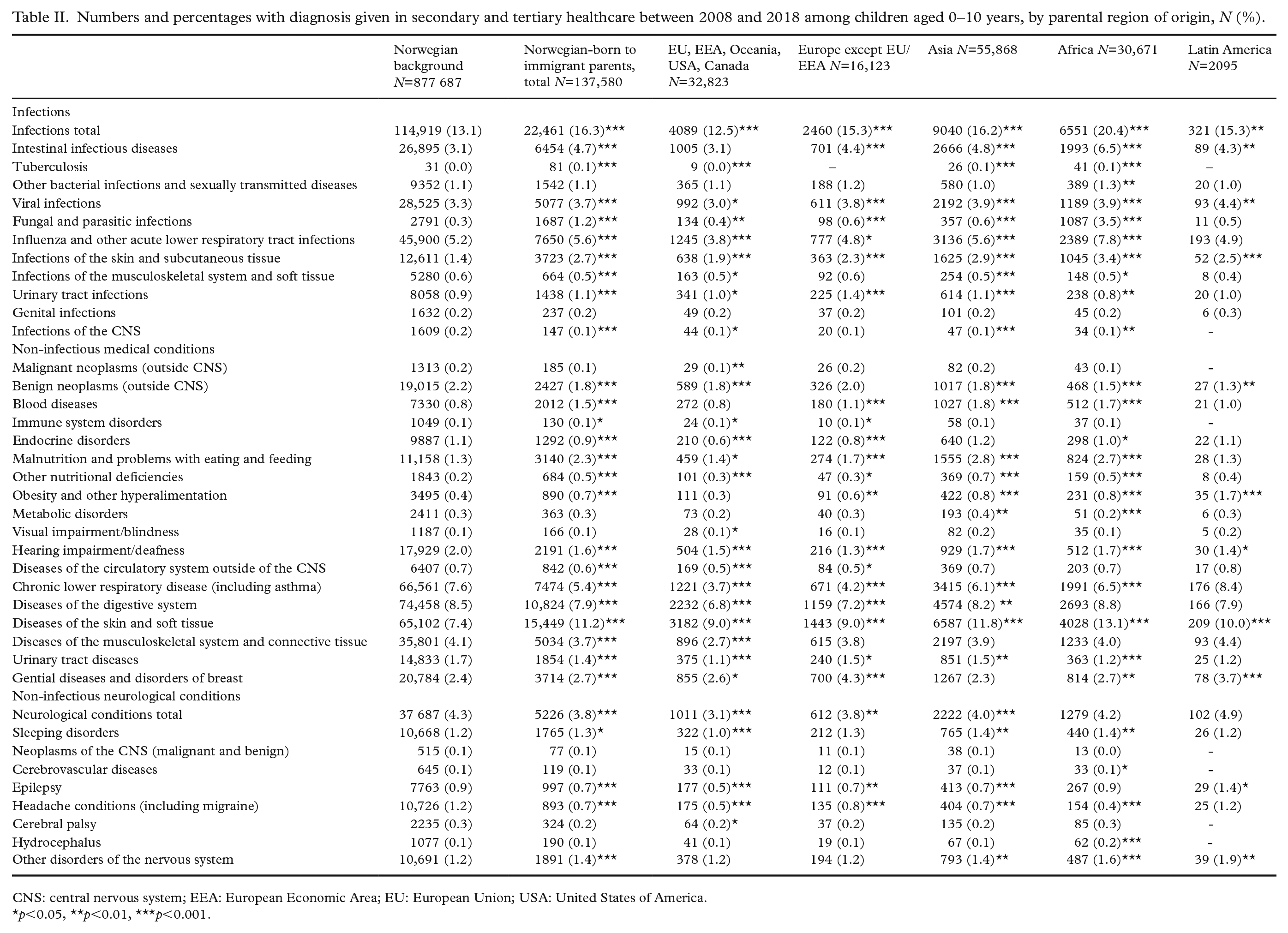
CNS: central nervous system; EEA: European Economic Area; EU: European Union; USA: United States of America.
p<0.05, **p<0.01, ***p<0.001.
Infections
Children of immigrants generally had higher hazards of viral infections, fungal and parasitic infections, infections of skin and subcutaneous tissue, intestinal infectious diseases and of tuberculosis than children of Norwegian background, but lower hazards of influenza and other acute lower respiratory tract infections, infections of the musculoskeletal system and soft tissue and infections of the central nervous system (Table III). Children of immigrants from EU/EEA/USA/Canada/Oceania had, in contrast to other groups of children of immigrants, lower hazards of viral infections and intestinal infectious diseases (Table III).
Hazard ratios (95% confidence intervals) for diagnoses given in secondary and tertiary healthcare between 2008 and 2018 among children aged 0–10 years, by parental region of origin.
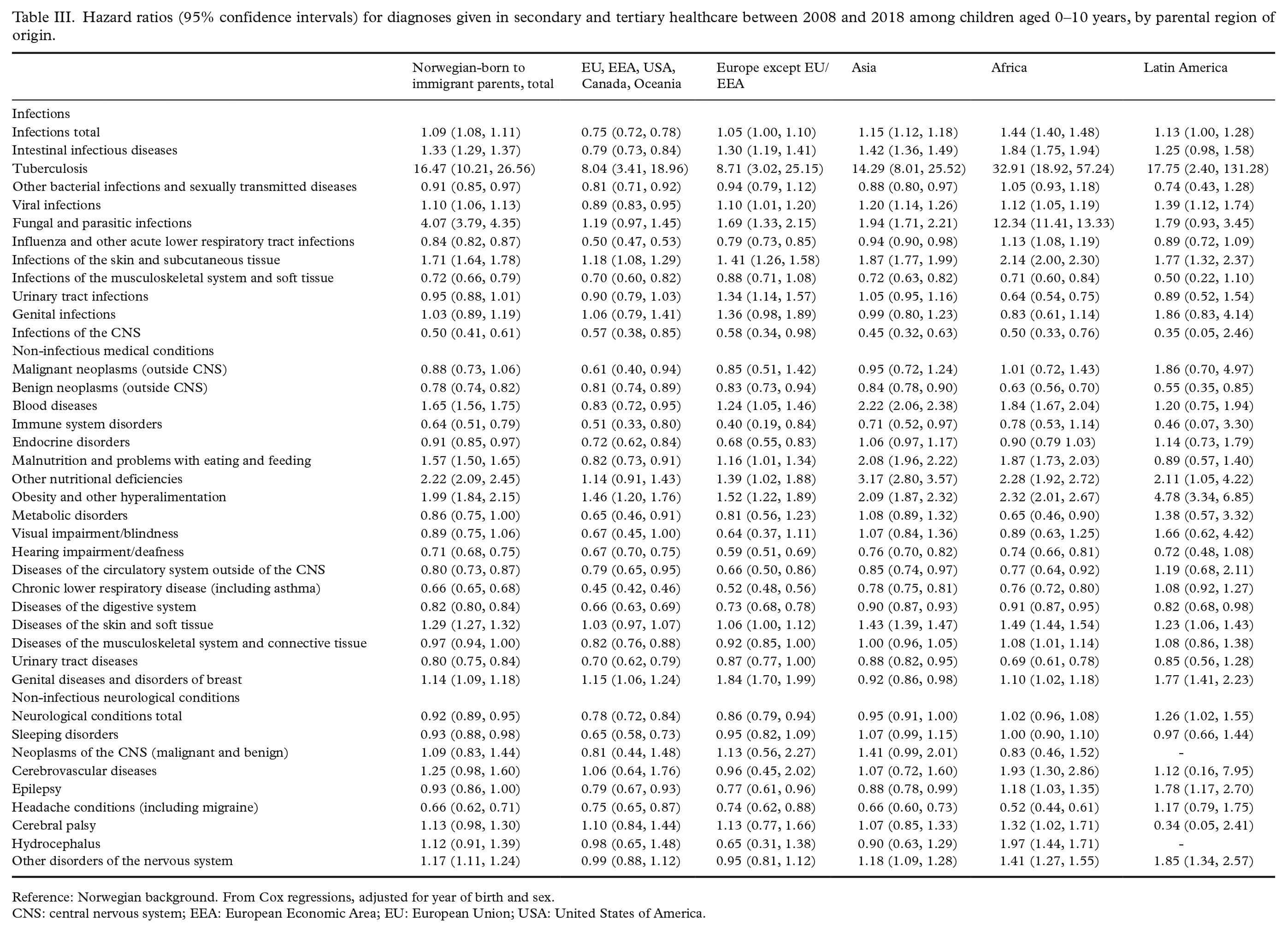
Reference: Norwegian background. From Cox regressions, adjusted for year of birth and sex.
CNS: central nervous system; EEA: European Economic Area; EU: European Union; USA: United States of America.
Non-infectious medical conditions
The hazards of obesity were higher in all groups of children of immigrants as compared with children of Norwegian background (Table III). The hazards of malnutrition and other nutrition-related disorders were also higher among children of immigrants from Europe outside EU, Asia and Africa. Hazards of skin diseases, of blood disease and of genital diseases were higher among most groups of children of immigrants (Table III).
Compared to children of Norwegian background, children of immigrants from all regions had lower hazards of gastrointestinal disease and of benign neoplasms (Table III). Children of immigrants from most regions also had lower hazards of diseases of the circulatory system, hearing impairment, immune system disorders and of chronic lower respiratory disease.
Non-infectious neurological conditions
Compared to children of Norwegian background, children of immigrants from Africa had higher hazards of cerebral palsy, cerebrovascular diseases and epilepsy (Table III). Most groups of children of immigrants had lower hazards of headache conditions, and children of immigrants from EU/EEA/USA/Canada/Oceania, Europe outside EU and Asia also had a lower hazards of epilepsy. Children of immigrants from Asia, Africa and Latin America had higher hazards of other neurological conditions, such as disorders of the peripheral nervous system and neurodegenerative disorders.
Discussion
Overall, children of immigrants did not appear to have poorer health than children of Norwegian background. Children of immigrants from EU/EEA/USA/Canada and Oceania generally had similar or lower hazards of diagnoses given in secondary or tertiary healthcare as children with Norwegian background. Among children of immigrants from other parts of the world, the picture was more complex, with both lower and higher hazards of disease, varying with diagnosis and region of origin. Obesity, malnutrition and other nutrition-related diseases, skin diseases and some types of infections were more common among children of immigrant parents.
Diagnoses with high hazards across groups of children of immigrants are consistent with findings from previous studies. Notably, most of these previous studies do not distinguish between children born in the host country to immigrant parents and children with a migration experience.
Children of immigrants had higher hazards than others of being diagnosed with obesity. It may be that secondary/tertiary health services for childhood obesity is better in larger cities, and as many immigrants live in larger cities, this could explain some of the overrepresentation of childhood obesity among children of immigrants. However, a high percentage with obesity is in line with results from cross-sectional studies in Norway and other European countries, showing higher prevalence of obesity among children with immigrant background, especially from ‘non-western’ countries. The exceptions are children of African descent, in whom rates of overweight have been low [4, 5, 18–21]. A high prevalence of obesity among children of immigrants has been associated with low parental socioeconomic status (SES). However, differences in obesity prevalence by immigrant status is not fully explained by immigrants having lower SES [18, 19]. Others have indicated that the high prevalence of obesity among immigrant children can be explained, to some or a large extent, by differences in lifestyle, such as screen time, frequent visits to fast food restaurants, high consumption of soft drinks and snacks, low physical activity, alone or in combination with parental SES [3, 5, 6, 18, 21]. Differences in fetal growth by mother’s region of origin [22] and large weight gains in the first months of life have also been highlighted as possible contributors to high prevalence of obesity among immigrant children [20, 23]. Although environmental factors are crucial for the development of childhood obesity, genes may also play a role [24]. A higher prevalence of diabetes among women of Asian and African descent might also contribute to the increased prevalence of obesity among children born to immigrant parents [25]. Childhood obesity based on diagnoses in secondary and tertiary healthcare would be underreported as the majority of patients with obesity are treated within the primary healthcare system.
The high percentage with skin disease among children of immigrants is in line with previous studies [9, 10], and an overrepresentation of children of immigrants with eczema has also been reported in primary care in Norway [15]. That these children are overrepresented in both primary and secondary/tertiary healthcare suggests that children of immigrants do have more severe disease, rather than representing late presentations no longer able to be treated within primary care.
Children of immigrants had higher percentages with tuberculosis, viral infections, fungal and parasitic infections, infections of the skin and subcutaneous tissue and intestinal infectious diseases compared with children without immigrant background. Visits to and from parents’ country of birth may explain higher percentages with tuberculosis and fungal and parasitic infections [26]. Importantly, although hazards of tuberculosis are high among children of immigrants compared to other children, percentages with tuberculosis are low in all groups. High percentages with infectious intestinal disease and infections of the skin may be related to crowded housing and large groups of siblings.
Children of immigrants from most regions had lower hazards of chronic lower respiratory disease, resembling findings among children born to immigrants in Norway in a previous study of primary healthcare data [15]. In the same study, children who themselves immigrated had higher proportions with chronic disease in the lower respiratory tract [15]. In studies from Canada [27] and Sweden [28] children of immigrants (both those who were born in the host country and those who immigrated) had a lower risk of asthma than other children. Asthma was only part of a broader diagnosis category in our study. Low SES and deprived living conditions, such as damp and mold at home, are proposed to play a role in the development of chronic disease in the respiratory tract [29, 30]. As children of immigrants often experience low SES and worse housing conditions, such conditions do not appear to explain our finding of lower hazards in this group.
Children with background from EU/EEA/Oceania/USA/Canada had lower hazards of most diagnoses than children without immigrant background. A large percentage of this group probably have parents with SES comparable to, or even higher than, the general Norwegian population, both in terms of education, employment and income. Most of them have good English skills, which makes communication easier compared with immigrants from other regions. The role of socioeconomic position in health among children of immigrants should be assessed in future studies.
Differences between groups in hazards of diagnoses may reflect real differences in health, or may indicate underuse (or excess use) of services by some groups, or underdiagnosis in other groups. Differences in diagnostics may relate to between-group variation in interpretation of symptoms, related healthcare-seeking behaviour and possibly quality of care given. Immigrant parents may face barriers to initiating contact with healthcare services, such as difficulty navigating a new and unfamiliar health system, language barriers or low health literacy, which may result in their children being less likely than others to receive a correct and timely diagnosis and relevant follow-up and treatment. Children of immigrants had lower percentages of several conditions than other children, which could reflect barriers to seeking healthcare among their parents. However, as our results also show higher percentages for other diagnosis among children of immigrants than among other children, they do not necessarily indicate that immigrant parents in general face significant barriers to seeking or receiving help from secondary or tertiary healthcare. It may also be that primary healthcare personnel respond differently to contact from immigrant parents and refer children of immigrants to a larger or lesser extent than other children. Difficulties in communication about health problems and needs could lead to fewer referrals, but also to excess referrals if health workers are unsure about the needs of a child with immigrant parents.
Strengths and limitations
The strengths of our study include the use of register data over a range of diagnoses, with national coverage and with linkage to immigrant-related variables from Statistics Norway. Differences between groups could reflect both differences in health, but also differences in healthcare usage. Our data pertain to diagnoses given in secondary or tertiary healthcare only. However, the results may be affected by differences in the use of primary health; for example, if children develop more severe conditions as a consequence of not receiving timely treatment in primary care. Thus, data on diagnoses given in primary care could have nuanced the picture in this study. Furthermore, we have focused on physical health in this study. We included all children in the age range 0–10 years between 2008 and 2018. Thus, the time and age of follow-up varied between children. This was handled by using Cox regressions and by adjustment for year of birth. We did not include children born in Norway to one Norwegian-born and one foreign-born parent. These children are a heterogenous and growing group in Norway and warrant special attention in further studies.
We chose to use 95% confidence intervals for percentages and hazards and did not adjust these for multiple comparisons. Consequently, some hazards in children of immigrants may be different from the reference category simply by chance. However, the purpose of the study was not statistically to test the hazard of each specific disease category, but to study disease patterns and the overall occurrence of disease and healthcare use.
The study generates knowledge about differences in diagnoses between children of immigrants and other children, which is important for doctors and other health personnel, but also for other occupational groups and persons working with children and parents and who have impact on their health-seeking behaviour. Timely and correct diagnosis and treatment is essential for the prevention of future illness.
Conclusion
Children of immigrants did not present with worse health overall compared to children without immigrant background. The higher prevalence of obesity among immigrant children poses a public health challenge.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948211039397 – Supplemental material for Variation in disease in children according to immigrant background
Supplemental material, sj-docx-1-sjp-10.1177_14034948211039397 for Variation in disease in children according to immigrant background by Marte Kjøllesdal, Angela S. Labberton, Anne Reneflot, Lars J. Hauge, Samera Qureshi and Pål Surén in Scandinavian Journal of Public Health
Footnotes
Authors’ contributions
The study was initiated by PS. Data were prepared by LJH. MK did the statistical analyses and drafted the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Availability of data and material
The datasets analysed during the current study are not publicly available, but anonymous data are available from the corresponding author on reasonable request.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The study was approved by the Regional Ethics Committee South-East (REK 2019/1286).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was performed at and financially supported by the Norwegian Institute of Public Health.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.