
Abstract
Keywords
Background
Gambling disorder (GD) is a behavioural addiction with similar aetiology and symptoms to those of substance use disorders (SUDs) (Grant et al., 2010). Gambling disorder refers to repeated problem gambling behaviour that becomes increasingly destructive over time and is associated with long-lasting consequences. In the Diagnostic and statistical manual of mental disorders (DSM-5) published by the American Psychiatric Association (APA, 2013), GD replaced the term pathological gambling, which was previously categorised as an impulse control disorder. In the revised edition of the International statistical classification of diseases and related health problems (11th ed., ICD-11, World Health Organization, 2019), the diagnostic term was also changed and GD was placed in the category of substance use and related disorders. Although current diagnoses of GD are based on the ICD-10 criteria, the term GD is considered more modern, and is thus used in this report.
Problem gambling, a broader concept also including less severe forms than GD, affects 0.1–5.8% of adults worldwide; however, these figures are based on a variety of measurements and survey methods used (Calado & Griffiths, 2016). Respectively, international comparison of the standardised problem gambling prevalence rates indicated variation from 0.5% to 7.6%, with the average rate across all countries being 2.3% (Williams et al., 2012). The prevalence of GD has varied from 0.6% to 1.5% within Finland depending on time period, instrument and methodology used in the survey (Salonen et al., 2020; Salonen, Lind, Castrén, Lahdenkari, et al., 2019). Swedish register-based prevalence rates (Håkansson et al., 2018) were notably lower than survey-based rates, which implies that many individuals experiencing GD symptoms are not reached by the healthcare services.
Problem gambling is more prevalent among men (Allami et al., 2021; Sharman et al., 2019), but an increasing number of women are affected by problem gambling (McCarthy et al., 2018; Salonen et al., 2020). For women, the onset age for gambling tends to be higher, and gambling becomes problematic more quickly compared to men (Grant et al., 2012). Furthermore, risk groups for GD are younger people (Allami et al., 2021; Dowling et al., 2017) and older adults (Sharman et al., 2019). The results of a Swedish register-based study implied an upward trend of diagnosed GD (Håkansson et al., 2018). Based on surveys, there has been a downward trend in problem gambling rates worldwide (Williams et al., 2012).
To our knowledge, empirical evidence about recent trends in the prevalence of diagnosed GD in the total population is scarce. The Nordic countries’ national registers provide an extraordinary resource for research. Prior Swedish studies have covered outpatient and inpatient data from specialised healthcare visits (e.g., Håkansson et al., 2018; Karlsson & Håkansson, 2018). This study aims to fill the gap in the literature and examines the annual prevalence of GD among the Finnish adult population in the recent decade. The study includes both primary and specialised healthcare registries including analyses of gender- and age-related differences among persons with GD.
Methods
Participants and measures
Data on primary and secondary diagnoses and the long-term diagnosis of GD (ICD-10, F63.0) between 2011 and 2020 for persons aged 18 years or older living in Finland were retrieved from the national healthcare registers maintained by the Finnish Institute for Health and Welfare (THL). The Register of Primary Health Care Visits (RPHCV) covers all primary healthcare centres in Finland. Health visits at occupational healthcare services and private clinics are also included. The Care Register for Health Care (CRHC) contains data on specialised outpatient and inpatient care including information regarding each visit, such as diagnoses. The Care Register for Social Welfare (CRSW) covers registers of social welfare institutions, such as nursing homes, disability homes, inpatient substance use care and other 24/7 sheltered accommodation. In Finland, GD is always diagnosed by a physician both in health services and in the context of social services.
The data were obtained by writing a data request and order for the THL in 2021. According to their data policy and national regulations, the research material was not subject to authorisation. Diagnoses of underaged persons (n = 90) and individuals living in Åland Island (n = 9) were excluded. The data covering 2021 (n = 796; 548 men, 248 women) were not complete yet, and were therefore excluded. Based on the data retrieval, 2,647 persons with GD diagnosis were found from the CRHC, 1,897 from the RPHCV and 10 from the CRSW. The same person might have had several diagnoses during the same year; however, each person was counted only once per year. If a person had diagnoses in different years, each diagnosis was counted separately.
The study population varied annually from 4,282,714 individuals in 2011 to 4,460,177 in 2020. Ultimately, a total of 4,282 persons with GD diagnosis and complete background. Information were included, with some of them overlapping in different years. The population was stratified by gender and age group (18–29, 30–44, 45–59, 60+ years).
Statistical analysis
The results are based on descriptive statistics. Data were analysed and visualised using Microsoft Excel for Mac (version 16.55) and R ggplot2 package (Wickham, 2016). The annual prevalence rates were calculated using the average population during a calendar year as a denominator. The increase in annual prevalence rates was calculated by dividing the annual prevalence from 2020 by the prevalence rate of 2011. Crude odds ratios were calculated in order to examine the increase in the prevalence of GD between 2011 and 2020.
Ethics
This study did not require separate approval from the ethics committee nor procedure to obtain informed consent: data were aggregated. Any results based on fewer than five cases are not reported.
Results
The data included 2,617 persons with GD (1,858 men, 759 women) and their 4,282 GD diagnoses (men 3,011, women 1,271). Overall, the number of persons per year with GD increased from 195 to 796, being 4.1 times higher in 2020 than in 2011 (Table 1). The annual prevalence of GD increased from 0.005% to 0.018%, the latter figure being 3.6 times higher than the former. Between 2011 and 2020, persons with GD had a mean age of 36.7–40.0 years, a median age of 33.5–36.0 years, and min–max age of 18–92 years. The proportion of GD as a main diagnosis increased from 52.8% to 69.5%, being 1.3 times higher at the end of the study period.
Persons with gambling disorder (GD) diagnoses based on administrative health registers in Finland between 2011 and 2020.
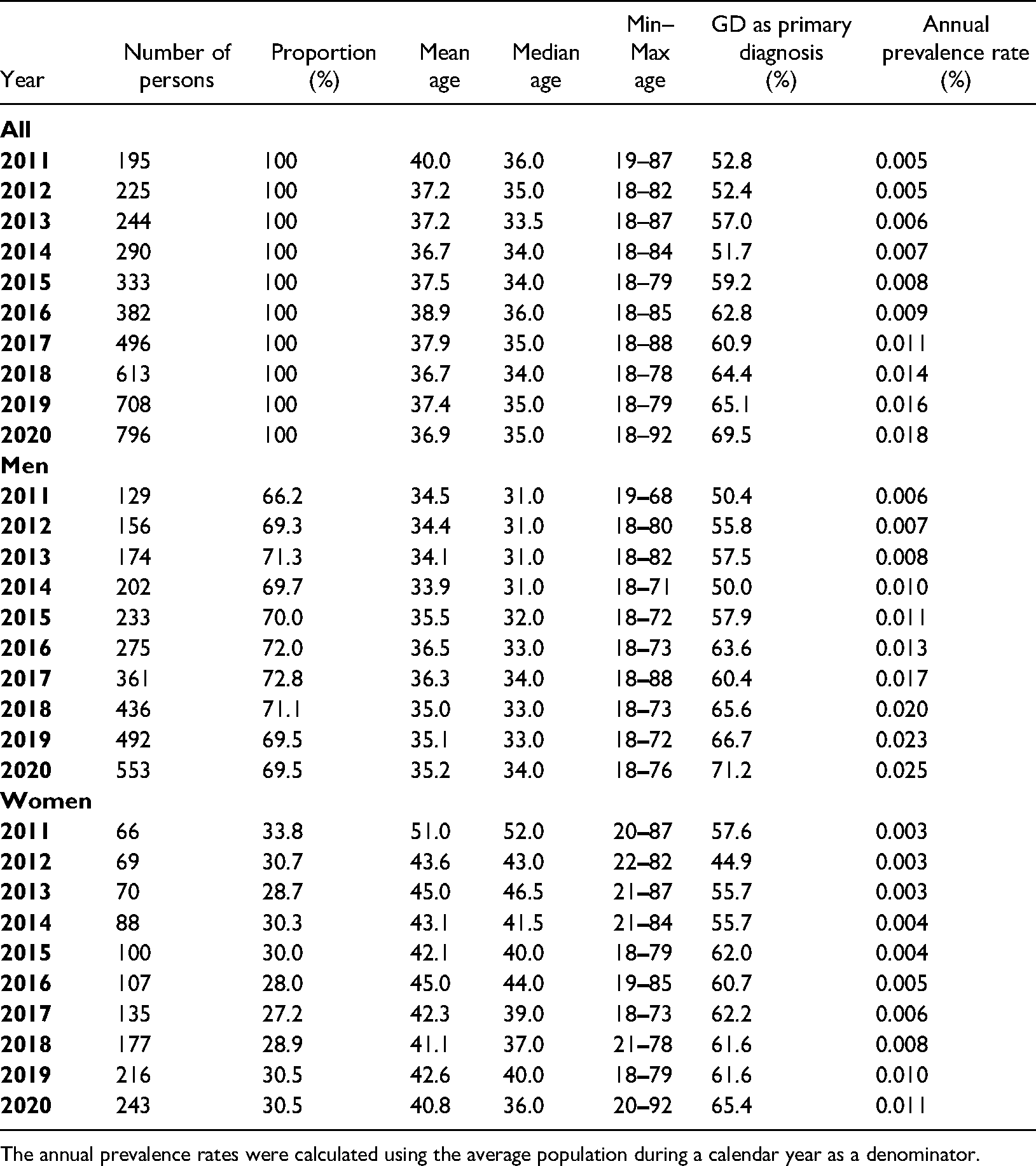
The annual prevalence rates were calculated using the average population during a calendar year as a denominator.
Of the persons with GD, 27.2–33.8% were women (Table 1). Between 2011 and 2020, the number of women with GD increased from 66 to 243 individuals, whereas the number of men with GD increased from 129 to 553 individuals. The annual prevalence rate of GD increased from 0.006% to 0.025% among men and from 0.003% to 0.011% among women. The ages of women with GD varied from 18 to 92 years, with the mean age varying from 40.8 to 51.0 and the median age from 36.0 to 52.0 years. The corresponding figures among men were: min–max 18 to 88 years, mean age 33.9–36.5 years and median age 31.0–34.0 years.
The number of persons with GD and the annual prevalence rate increased between 2011 and 2020 in all age groups across genders, apart from women aged 60 or over (Figure 1). Results showed that during recent years, the absolute number of persons with GD was highest among 30–44-year-olds across gender. The age group with the highest annual prevalence of GD was 18–29-year-olds in men and 30–44-year-olds in women.
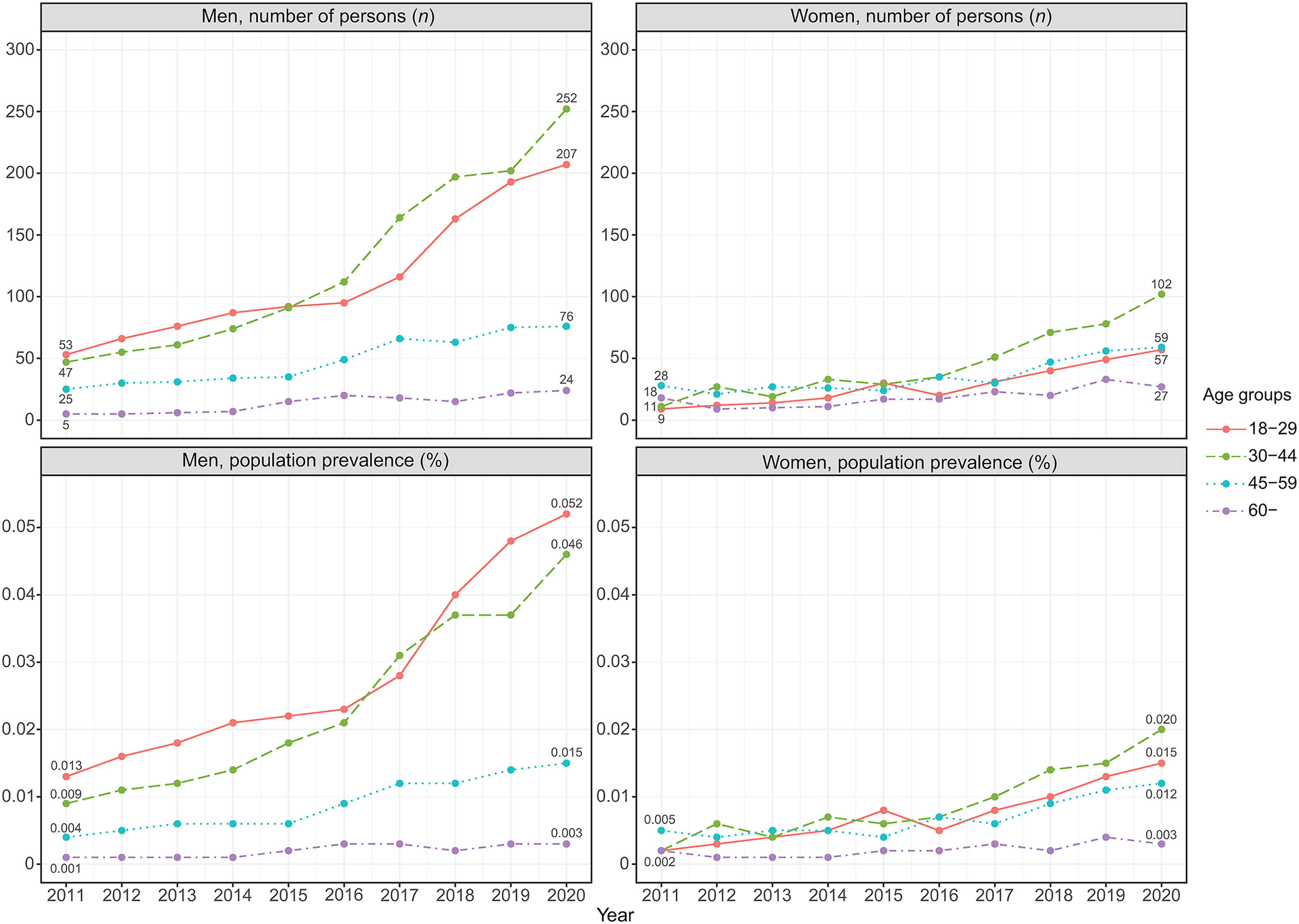
The annual number of persons and population prevalence of diagnosed gambling disorder by gender and age between 2011 and 2020.
The prevalence of GD increased from 2011 to 2020 among men (OR = 4.08, 95% CI = 3.37–4.95) and women (OR = 3.56, 95% CI = 2.71–4.68). Age-stratified analyses among the male population further showed that the increase from 2011 to 2020 was moderate across all age groups. Among women, there was an increase in the prevalence of GD among 18–29-year-olds and 30–44-year-olds, in particular, and also among 45–59-year-olds. However, there was no increase in the prevalence rate of diagnosed GD among women aged 60 years or older (Table 2).
Increase in the prevalence of gambling disorder (GD) diagnoses between 2011 and 2020 among men and women based on administrative health registers in Finland.
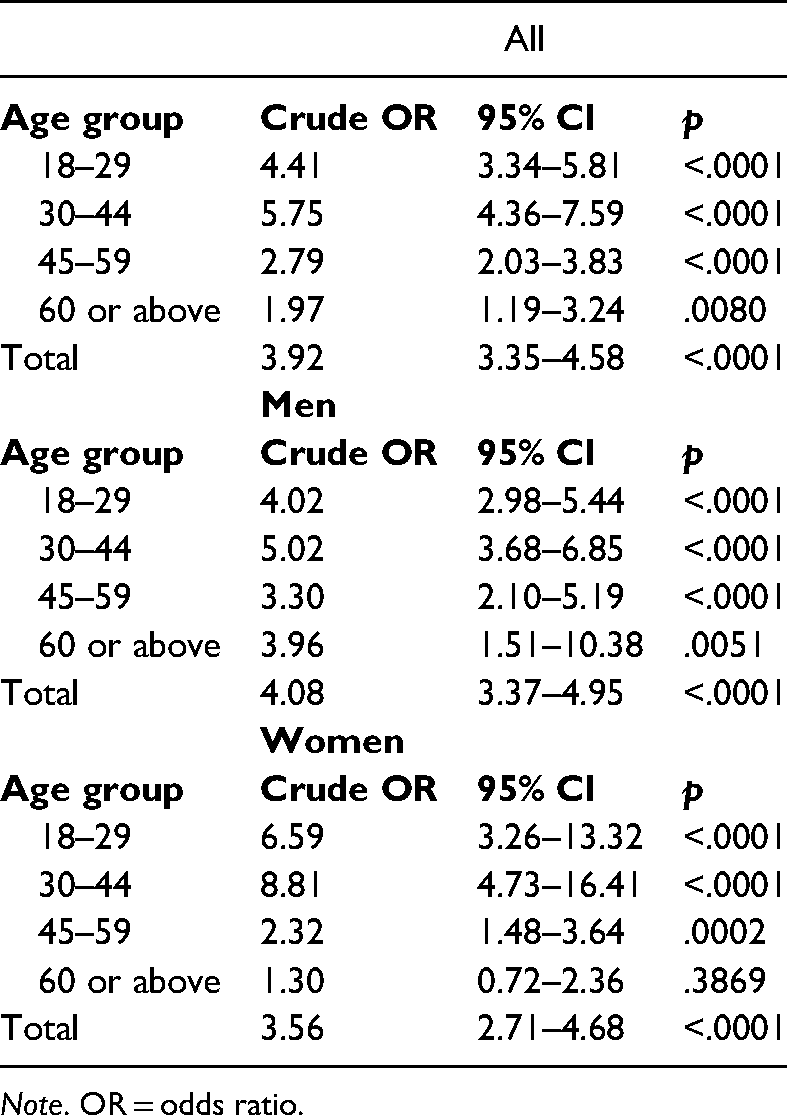
Note. OR = odds ratio.
Discussion
This study examined the prevalence of diagnosed GD in the Finnish adult population between 2011 and 2020. Although annual rates of GD increased across gender and age groups, the prevalence rates were notably low (0.005–0.018%). These observations are in line with a similar Swedish study (Håkansson et al., 2018). Meanwhile, the observed survey-based prevalence rate of probable GD in Finland has increased from 1.0% to 1.4% (Salonen et al., 2020). Although the increase in the diagnosed prevalence rates indicates that the recognition of GD has improved, a significant discrepancy between register-based estimates and the results of surveys suggests that GD as a behavioural addiction with long-lasting consequences for the individual is under-diagnosed in the healthcare system.
Currently, even though GD symptoms may be present, they are not systematically screened for (Achab et al., 2014) or recognised (Tikkinen et al., 2012) in health care. Further, a lack of time, skills and resources to deal with identified problems exists among healthcare professionals (John et al., 2020), probably contributing to under-recognition of GD. The low prevalence rate could also reflect treatment barriers: the treatment system is incoherent and may result in challenges for individuals to obtain adequate treatment. In general, persons with GD tend to seek help only when their problems are prolonged and result in significant harm (Bellringer et al., 2008). Also co-occurring mental health disorders and SUD (e.g., Dowling et al., 2015; Theule et al., 2019), may affect both treatment seeking and recognition of the GD. Together with lower-than-expected prevalence rates, the fact that, when diagnosed, GD was more often than not the primary diagnosis, suggests that GD is under-recognised and/or documented, when the reason for seeking treatment is something else, e.g., depression or anxiety.
From a clinical perspective, the conceptualisation of GD, the diagnostic criteria and the threshold for diagnosis have changed (APA, 2013; WHO, 2019). Simultaneously, treatment has shifted towards interventions (e.g., motivational interviewing, cognitive behavioural therapy) known to be effective in treating other addictions (Dutra et al., 2008). Consequently, implementation of these treatment modalities for GD has been going on in Finland, with evidence-based treatment guidelines underway. However, much is yet to be done in order to improve early detection and screening procedures. The upcoming implementation of ICD-11 criteria may improve the use of diagnostics, especially with a new specification (hazardous gambling or betting; QE21), which is less severe than gambling disorder (6C50) and enables detection and treatment of a problem at an earlier stage.
Low prevalence rates of diagnosed GD suggest that although the general interest towards behavioural addictions and their treatment among professionals has increased, many persons with GD do not seek treatment. Shame, denial and stigma are typical reasons preventing or slowing down individuals from seeking treatment (Kaufman et al., 2017; Suurvali et al., 2009). The Finnish evidence base on harmful gambling has strengthened during recent years (e.g., Castrén, 2013; Joutsa, 2012; Raisamo et al., 2022). Furthermore, public discussion on gambling has been active in Finland resulting in increased awareness of GD and perhaps reducing stigma, which may facilitate treatment-seeking and to some extent explain the increase in prevalence figures observed in this study. Moreover, an increase in GD could be explained by the national helpline statistics indicating that gambling-related harms have become more severe (Silvennoinen & Vuorento, 2020). Treatment in outpatient health care has also increased in Sweden, with an increasing treatment intake of younger individuals (Håkansson et al., 2018).
During the study period, the gambling environment has also changed, and online gambling has increased significantly (Salonen et al., 2020). Furthermore, the Finnish gambling system was reformed in January 2017 when the country's previous three monopoly operators were merged into a single company. Based on population surveys conducted in three southern regions, gambling-related harms did not change among the general population between 2016 and 2017 (Salonen, Lind, Castrén, Lahdenkari et al., 2019). Help-seeking gamblers, however, experienced significantly more harms in 2017 than 2016 (Salonen, Lind, Castrén, Heiskanen, et al., 2019; Silvennoinen et al., 2018). Based on annual reports from the national helpline Peluuri, the total number of contacts from help-seeking gamblers increased from 736 to 1,366 between 2011 and 2019 (Silvennoinen & Vuorento, 2021; Sjöholm et al., 2015). However, the number of contacts decreased to 1,074 in 2020, which may be due to the Covid-19 pandemic.
Gambling disorder was more prevalent among men, but the age of persons with GD was systematically higher among women. Of all GD diagnoses, one in three at most were among women, while the corresponding figure in Sweden was one in five (Håkansson et al., 2018). The progression of GD differs between genders (APA, 2013). Women may start to gamble and to develop gambling problems at an older age compared with men, but clinical studies support the “telescoping effect”, meaning that, among women, problems tend to proceed faster into GD (Grant et al., 2012). The prevalence of GD increased the most among 30–45-year-olds, especially with women. Recently, women's gambling participation and survey-based problem gambling have increased in Finland (Castrén et al., 2018; Salonen et al., 2020) and internationally (McCarthy et al., 2019).
Strengths and limitations
Our data include the whole Finnish adult population living in mainland Finland also covering primary care, which represents a clear strength. Furthermore, the administrative registers used are of high validity and coverage. A systematic review of the Quality of Finnish Hospital Discharge Register indicated that completeness and accuracy in the register varies from satisfactory to very good (Sund, 2012). After 2012, the validity of the registers has been rated good or very good as well (e.g., Heino et al., 2018; Jokela et al., 2019). It should be acknowledged, however, that very little is known about the validity of GD diagnoses. The observed temporal changes in the number of persons with GD appear to suggest improved recognition of GD as well as increased help-seeking behaviour in the adult population. However, some of the figures from the most recent years may still be updated retrospectively. Both individuals living in Åland Island and under-aged individuals were excluded; however, some very young children had GD diagnoses which implies that GD diagnoses may be used for symptoms related to video gaming, defined as gaming disorder in the revised ICD-11. In fact, the Finnish translation for the diagnostic term “pathological gambling” is “pelihimo”, where the noun “peli” is the equivalent of “game” and “himo” the equivalent of “urge”. This may have caused confusion between the two disorders as noted also by Karlsson and Håkansson (2018). Even though the ICD is an official world classification, the DSM is used for example in the US, which limits international comparability. In this study, we used aggregated data; therefore, we were not able to examine the paths or trajectories of the disease. Further research on this topic is needed using individual-level register data.
Conclusions
The prevalence of diagnosed GD was extremely low in Finland, but it increased across genders and age groups, except for the 60-year-old or older women, during the past decade. Gambling disorder was more prevalent among men; however, the largest increase in prevalence was observed among 30–44-year-old women. Gambling appears to be under-recognised and under-diagnosed by professionals, thus further efforts are needed to increase the awareness and knowledge of both primary and specialised healthcare professionals and the public, as well as to develop low-threshold treatments that may be easily accessible for those in need. Paradigm changes in GD and the revised ICD criteria may improve recognition of GD in the future.
Footnotes
Acknowledgements
We wish to thank Planning Officer Anna Mikkola for implementing the data request and Chief Physician Jutta Järvelin for consulting help.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was funded by the Ministry of Social Affairs and Health, Finland, within the objectives of the §52 Appropriation of the Lotteries Act. Daily work of the authors AHS, SC, TL and TG at the Finnish Institute for Health and Welfare, Finland, was also funded by the Ministry. The Ministry has had no role in the study design, analysis, or interpretation of the results of the manuscript or any phase of the publication process.