
Abstract
Aims:
During the first wave of the COVID-19 pandemic, Sweden registered a high level of excess deaths. Non-pharmaceutical interventions adopted by Sweden have been milder compared to those implemented in Denmark. Moreover, Sweden might have started the pandemic with a large proportion of vulnerable elderly with a high mortality risk. This study aimed to clarify whether excess mortality in Sweden can be explained by a large stock of ‘dry tinder’ instead of being attributed to faulty lockdown policies.
Methods:
We analysed weekly death counts in Sweden and Denmark from July 2007 to June 2020. We used a novel method for short-term mortality forecasting to estimate expected and excess deaths during the first COVID-19 wave in Sweden and Denmark.
Results:
In the first part of the epiyear 2019–2020, deaths were low in both Sweden and Denmark. In the absence of COVID-19, a relatively low level of death would be expected for the later part of the epiyear. The registered deaths were, however, way above the upper bound of the prediction interval in Sweden and within the range in Denmark.
Conclusions:
‘Dry tinder’ can only account for a modest fraction of excess Swedish mortality. The risk of death during the first COVID-19 wave rose significantly for Swedish women aged >85 but only slightly for Danish women aged >85. The risk discrepancy seems more likely to result from differences between Sweden and Denmark in how care and housing for the elderly are organised, coupled with a less successful Swedish strategy of shielding the elderly.
Keywords
Introduction
The importance of lockdown measures during the COVID-19 pandemic is still being debated, especially concerning Sweden [1,2]. In the period from March to June 2020 – the first wave of the COVID-19 pandemic – Sweden did not undergo a strict lockdown compared to Denmark and most other European countries. Estimates of excess deaths (observed deaths minus expected deaths if COVID-19 had not struck) reveal that death rates in Sweden were significantly higher than in Denmark and elsewhere [3,4].
Mortality was low in Sweden in pre-pandemic months and in the previous years [5,6]. Hence, Sweden might have entered the pandemic with many people at high risk of death – a stock of ‘dry tinder’ [6].
Objective
This study aimed to shed light on whether excess deaths in Sweden from March through June 2020 were a natural consequence of low mortality from July 2018 to early March 2020.
Methods
We analysed data from the Short-Term Mortality Fluctuations (STMF) of the Human Mortality Database [7] on weekly death counts in Sweden and Denmark from July 2007 to June 2020. We compared these two countries, which are similar in terms of culture, health-care delivery and finance but different in their responses to COVID-19. We focused on epidemiological years (epiyears) that start on 1 July and end a year later. Epiyears are preferred in seasonal mortality analysis because they contain only one mortality peak of the winter months.
In our analysis, every epiyear is divided into two segments: an earlier segment from July (week 27) through to early March (week 10) and a later segment from week 11, when the pandemic started in Sweden and Denmark, through to the end of June (week 26). We previously studied ratios of deaths in the later segment of an epiyear to deaths in the earlier segment [8]. Since this ratio was close to constant over the 12 epiyears prior to the pandemic in Sweden and Denmark, we used its average value to forecast deaths in the second segment of epiyear 2019–2020 (when COVID-19 struck) based on data for the first segment. By subtracting these expected counts from the observed deaths, we estimated excess deaths.
Results and discussion
Figure 1 shows the later/earlier ratios across epiyears for Sweden and Denmark. Note the remarkably high value for Sweden in 2019–2020.
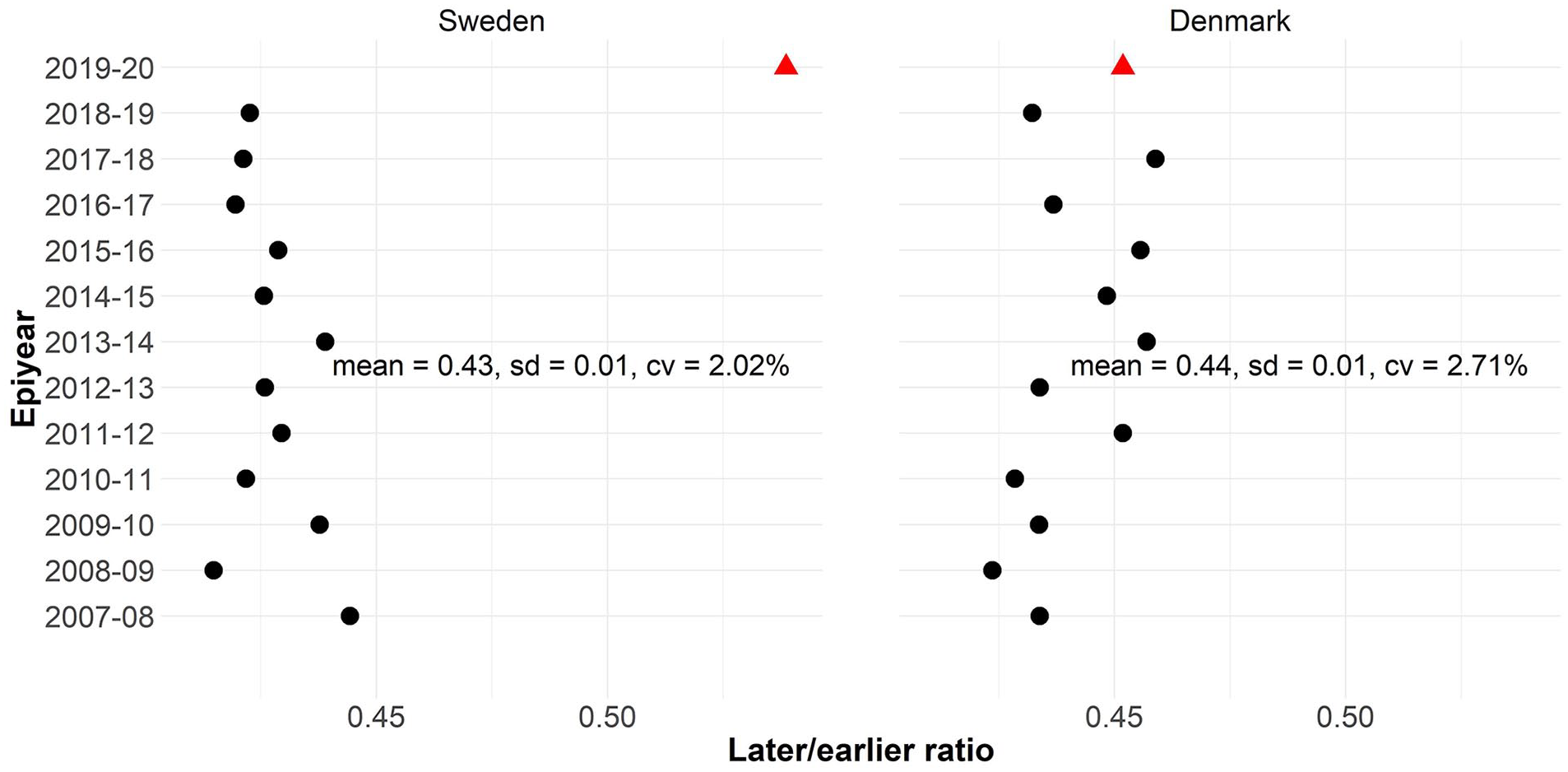
Ratios between deaths in the later and earlier segments of epiyears from 2007–2008 to 2018–2019 (dots) and 2019–2020 (triangles). Means, standard deviations and coefficients of variation are based on the 12 epiyears prior to the pandemic. Underlying data from the Human Mortality Database.
In epiyear 2019–2020, the first eight months – from July 2019 to the beginning of March 2020 – were characterised by low levels of deaths, particularly in Sweden, compared to other epiyears, which was probably the result of a very mild flu season (Figure 2). Death counts in the earlier part of 2019–2020 were about 60,000 in Sweden and 37,000 in Denmark. In the absence of COVID-19, around 26,000 deaths in Sweden and 16,000 in Denmark would be expected for the later part of the epiyear. The 95% prediction interval ranged from 24,100 to 27,800 for Sweden and from 14,900 to 17,400 for Denmark [8]. During the second part of the epiyear, 32,000 deaths were observed in Sweden – well above the upper bound – and 16,600 in Denmark – within the prediction interval and only 600 more than expected.
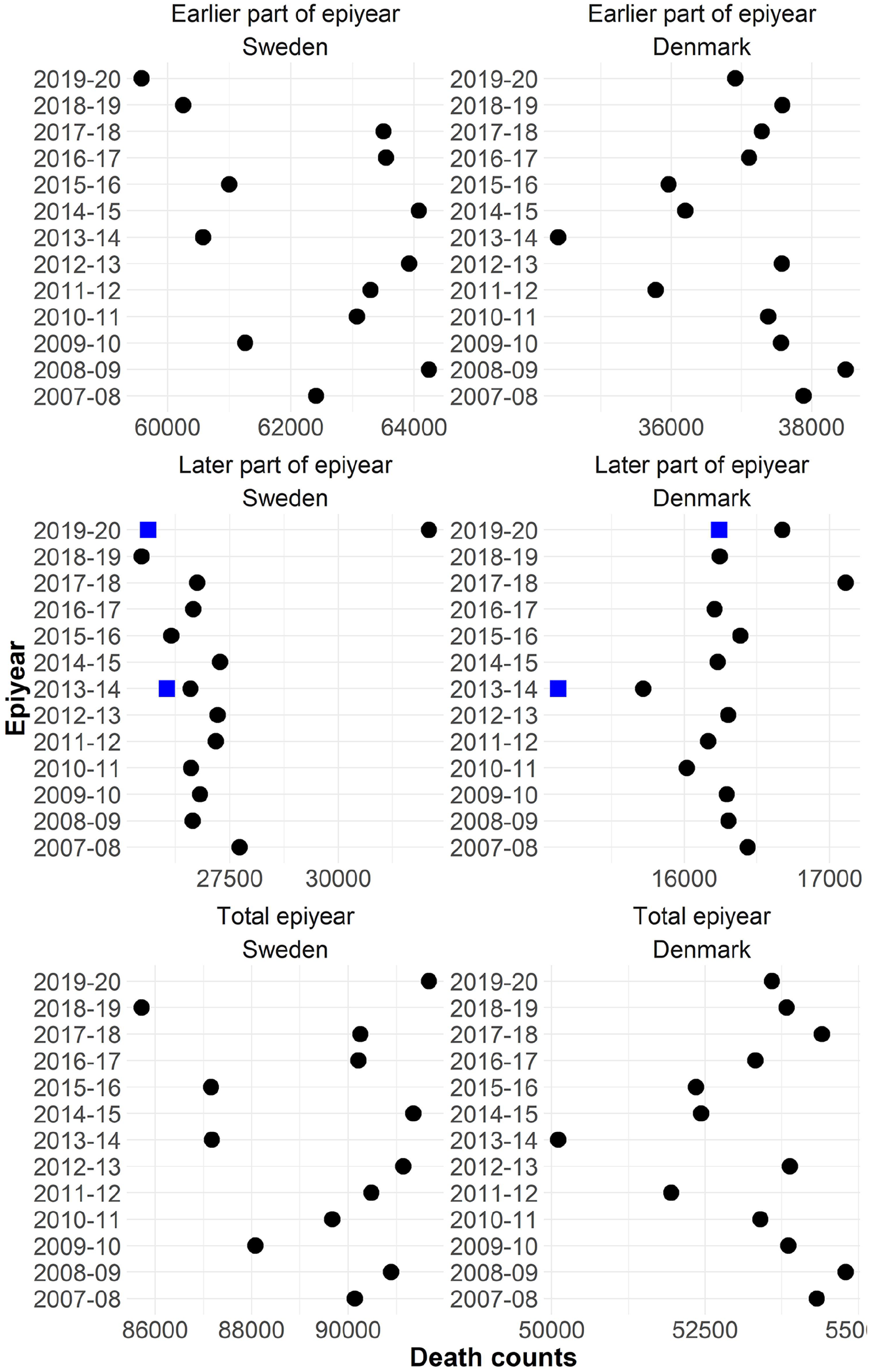
Observed death counts (dots) in the earlier part of epiyears (July to early March), later part of epiyears (March to June) and total epiyears (July to June) from 2007–2008 to 2019–2020 for Sweden and Denmark. The squares in 2019–2020 and 2013–2014 give the expected number of deaths in the later part of the epiyear.
‘Dry tinder’ refers to a hypothetical stock of individuals who are at risk of dying soon. In epidemiology and demography, the similar hypothesis of ‘harvesting’ [9,10] predicts that short-term shocks such as extreme air pollution or heatwaves tend to kill the weakest. The number of deaths temporarily increases and then decreases after the shock. Epiyears characterised by relatively low levels of deaths in an earlier segment would show a larger number of deaths than expected in the later segment [11].
Sweden experienced low mortality in the first period of 2019–2020. If mortality had been as high as in the seven worst years since 2007–2008, around 4000 more people would have died in the first period of 2019–2020 (Figure 2). If all these potential deaths were, highly unlikely, displaced to the second part of the epiyear due to the COVID-19 shock, the ‘dry tinder’ hypothesis would explain two thirds of the observed excess deaths.
For both Sweden and Denmark, the epiyear 2013–2014 was characterised by a mild earlier period (Figure 2). Compared to the harsh earlier period of epiyear 2008–2009, about 3600 fewer lives were lost in Sweden and about 4000 in Denmark. If the ‘dry tinder’ hypothesis were correct, in the later part of the epiyear 2013–2014, mortality should be substantially higher than predicted by the later/earlier approach. This occurs, but modestly. estimates for both Sweden and Denmark are about 600 deaths lower than observed deaths (Figure 2). This excess mortality is only a modest fraction of the deaths hypothetically averted in the first part of the epiyear.
If ‘dry tinder’ can survive a year, then epiyears with low mortality should be followed by epiyears with correspondingly high mortality and vice versa. Figure 2 shows that low mortality years are followed, with one exception, by years with higher mortality and that years of high mortality are followed, with several exceptions, by years with lower mortality. The increase or decrease in mortality from one epiyear to the next, however, is only weakly related to how low or high mortality is in the epiyear. Rypdal et al. [12] studied this.
The most striking jump from low to high death counts occurred in Sweden from 2018–2019 to 2019–2020 (Figure 2). Low mortality in the first period of 2018–2019 was, however, followed by low mortality rather than high mortality in the second period. The low mortality for 2018–2019 was followed by low rather than high mortality in the first part of 2019–2020. An explanation is needed regarding how the purported ‘dry tinder’ of 2018–2019 survived to the spring of 2020. If the very frail who survived through June 2019 faced a 50% hazard of mortality, then almost a third of them (1–exp(–0.50×37/50)=31%) would have died over the 37 weeks before week 11 in 2020. If during the first wave their hazard of mortality increased by a factor of 1.5, raising their annual risk of death to 75%, only a fraction would have died in the 15 weeks from 11 March to June: 1–exp(–0.75×15/52)=19%.
Half of all excess deaths in Sweden and 60% of female excess deaths struck people aged >85 years. This concentration of mortality at the highest ages lends some plausibility to the ‘dry tinder’ hypothesis, but the data and calculations above suggest that ‘dry tinder’ can only account for a fraction of excess Swedish mortality. Furthermore, the risk of death during the first COVID-19 wave rose 29% for Swedish women aged >85 years but only 5% for Danish women aged >85 years [8]. Why there was so much more purported dry tinder in Sweden requires explanation. The risk discrepancy seems more likely to result from differences between Sweden and Denmark in how care and housing for the elderly are organised, coupled with a less successful Swedish strategy of shielding the elderly [13]. This interacts with the dry tinder hypothesis: if Sweden had a lot of dry tinder, perhaps Sweden should have made special efforts to protect those >85 years of age.
After the pandemic years, mortality in Sweden might be modified in two opposite directions. If the dry tinder hypothesis were true, mortality should decrease. Causes of deaths neglected by delay of treatment might increase.
Conclusions
Some of the excess deaths in Sweden during the first COVID-19 wave were among people whose deaths were averted in previous months. This dry tinder hypothesis probably explains a fraction of high Swedish mortality compared to the much lower Danish levels. Further research is needed to estimate the magnitude of the effect. It seems clear, however, that most of the Swedish disadvantage was due to policy differences between Sweden and Denmark.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research is supported in part by the ROCKWOOL Foundation Excess Deaths grant and the AXA Research Fund.