
Abstract
Aim: Mental diseases and pain are serious public health problems and are a leading cause of disability worldwide. The aim of this study is to describe how pain and psychological distress separately and in combination are associated with four income trajectories over nine years in a cohort of long-term social assistance recipients (LTRs). Methods: A cohort of 456 LTRs from 14 municipalities in Norway were divided into four groups based on the presence or absence of pain and/or psychological distress. These were surveyed in 2005, and later linked by personal identification numbers to high-quality longitudinal administrative data covering the period 2005–2013. Methods include calculation of income statuses based on main sources of income, and multinomial logistic regression analysis. Results: In the group without pain and psychological distress, earnings from work as main source of income (14.6–38.0%) and disability benefits (2.9–16.1%) increased over the period. In the ‘double burden’ group the proportions who had social assistance as main income decreased (68.2–21.5%) and the proportions with disability benefits increased over time (5.6–36.6%). Only 27.2% of the total sample had earnings from work as their main income in 2013.
Keywords
Introduction
The global impacts of mental diseases and chronic pain are serious public health problems. While lower back pain in 2017 was reported as the leading cause of disability worldwide [1], depressive disorders ranked number three. Mental illness accounted in 2016 for 32.4% of years lived with disability (YLD) [2], and psychological distress is one of the prime mediators of the relationship between chronic pain and disability [3]. These facts provide good reasons to study how pain and psychological distress influence the income trajectories of long-term social assistance recipients (LTRs).
Evidence indicates that LTRs belong to the lowest layers in the socioeconomic hierarchy [4, 5] where their life opportunities are affected by worse health, more prevalent illness and higher mortality. Research on social inequalities in health, also in relatively egalitarian countries, demonstrates marked social gradients in health, and the pattern is documented in all age groups for both genders [6, 7]. LTRs experience multiple disadvantages over their life course, and previous research has found that psychological distress and chronic pain is prevalent among LTRs [8, 9]. Findings from numerous studies suggest that chronic pain and psychological distress co-occur. Not every individual with psychological distress has chronic pain or vice versa. However, many LTRs have had a troubled childhood, have a low sense of coping and self-esteem, have less social capital and report that they often are lonely [10]. Many LTRs have experienced long-term bullying and problems with alcohol and drug use [11]. A recent study shows that experience of economic disadvantage during childhood is a major predictor of a variety of negative outcomes during early adulthood, as for example mental disorders [12]. It is reasonable to assume that these factors affect LTRs’ affiliation to the labour market.
Welfare programmes are expected to reduce the socioeconomic gap because they decrease the impact of social stratification [13]. In this study, we investigate the relative risk of having social assistance as main source of income in 2013 versus disability benefits, earnings from work or work assessment allowance for those reporting to have pain and/or experiencing psychological distress in 2005.
Economic social assistance provides money for subsistence intended for short-term use. However, previous studies of social assistance dynamics show that many, who successfully exit social assistance, re-enter later [14–17]. These studies provide important, yet limited insights, both theoretically and practically. This is often caused by a lack of information on personal, social and health-related resources. In theory, these factors are likely to affect the exiting of social assistance benefits and the likelihood of entering and exiting a job [18]. Key predictors of this phenomena are both structural and individual circumstances such as a weak labour market, high age, immigrant status, low education, weak professional ties, being single, weak labour market attachment, low employability, substance abuse and poor physical and mental health [5, 14, 9, 20]. Studies combining health and social variables with the duration of social assistance benefits are hard to find, but in one previous study, no statistically significant association was found between health problems and the probability of receiving social assistance [21]. However, a large study from Australia, based on nationally representative longitudinal data, found that multiple risk factors and mental health problems were associated with increased risk of entry and re-entry to disability, unemployment, and single parenting payments for women, and disability and unemployment payments for men [22].
Given the paucity of research on health variables and income trajectories, in this study we extend our previous research in a cohort of LTRs identified in 2005. The aim of this study is to describe and investigate whether pain and psychological distress separately and in combination, are associated with the four income trajectories – ‘earnings from work’, ‘work assessment allowance’, ‘disability benefits’ and ‘social assistance’ – over a period of nine years from 2005–2013.
Methods
Design
The current study combines data from a descriptive cross-sectional survey conducted in 2005 with longitudinal administrative data obtained from different registries in Norway for the period 2005–2013.
Survey data from 2005
Participants were recruited from 14 of the 433 municipalities in Norway, providing geographic variability including both rural and urban municipalities in different parts of the country. LTRs were included if they had received social assistance as their main source of income for at least six of the last 12 months, were between 18 and 60 years of age, and were able to complete the study questionnaire. A detail description of methods is reported elsewhere [8].
Registry data
In March 2016, Statistics Norway (who had stored the code key from the survey study) sent out an information letter to the LTRs who were included in the study from 2005. The letter provided information about the variables we wanted to obtain, and the individuals were asked if they wanted to reserve themselves from the follow-up registry study. Figure 1 shows that 1291 individuals met the initial inclusion criteria in 2005, and 1266 of these were found in the registers in 2017. The response rate in 2005 was 52.7%. Since the present study links data from the LTRs who answered the questionnaire in 2005, with follow up data from Norwegian registers, the sample in this study comprises 456 individuals. No significant differences in age, gender and previous receipt of social assistance or social security benefits were found between the survey and registry samples (See Table I).
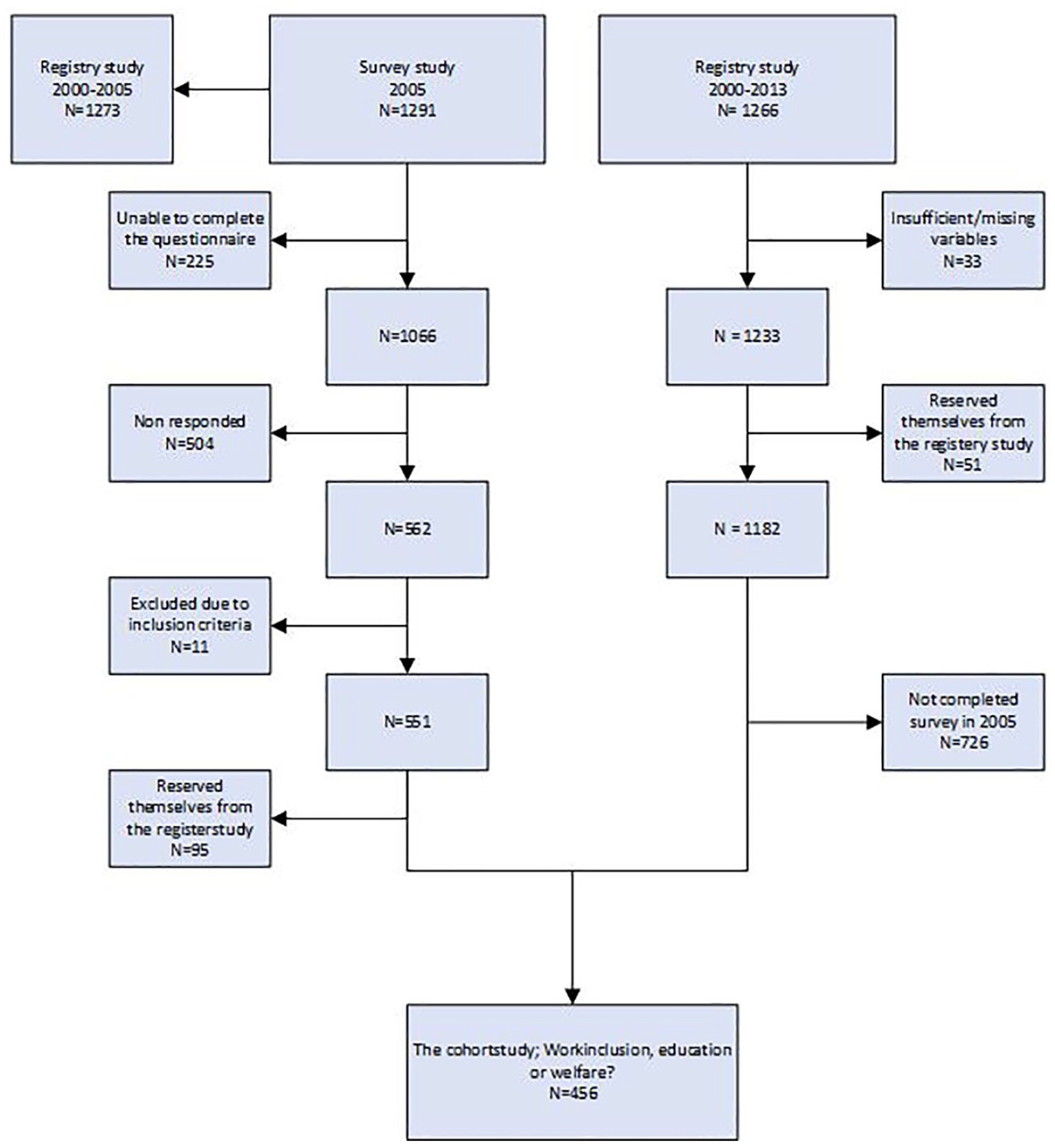
Flowchart.
Comparison of registry selection (n = 1182) and survey selection (n = 456) on background and income variables in 2005 and 2013.
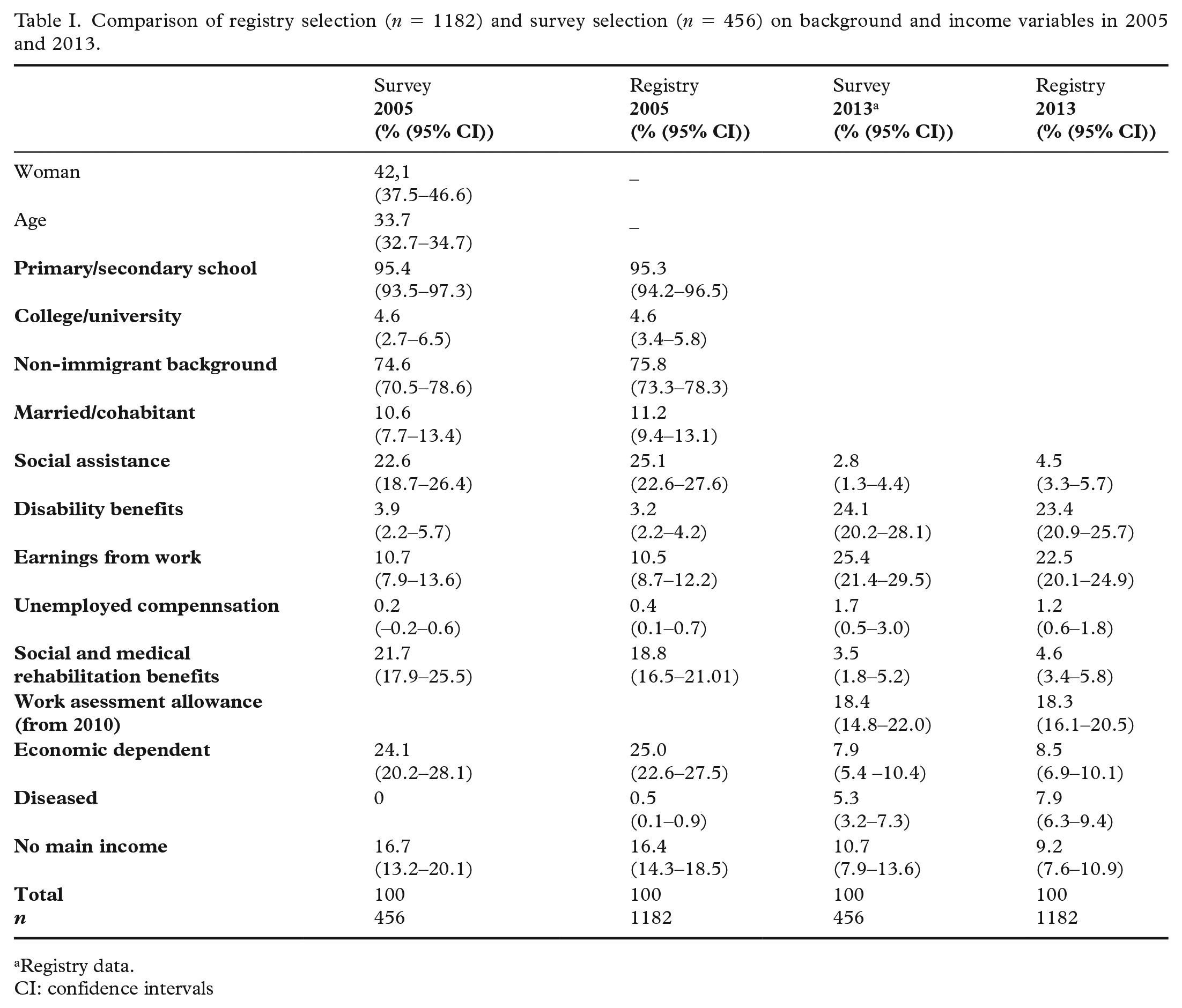
Registry data.
CI: confidence intervals
Instruments/variables
Pain
LTRs were categorized into pain groups based on their responses to a screening question about whether or not they were generally in pain.
Psychological distress
The 10-item Hopkins symptom checklist (HSCL-10) was used to evaluate psychological distress. A total HSCL-10 score was calculated as the mean of the 10 individual items. Each item is rated on a 4-point Likert scale that ranges from 1 (not at all) to 4 (extremely). HSCL-10 has a cut point of 1.85, which is recommended as a valid predictor of mental disorders as assessed independently by a clinical interview [23]. In this paper we measure pain and psycological distress based on the 2005 survey. Thus, we are only measuring pain and psycological distress cross-sectionally.
The registry data
The registry data from 2005–2013 is obtained from Statistics Norway (SSB), The Directorate of Labour and Welfare, and The Causes of Death registry. The variables were age, marital status, refugee status, type of household, child and child age, education, social assistance, unemployment, participation in labour marked programmes, occupational activity, granted disability insurance, or other benefits and the cause/diagnosis of disability benefit and death.
Data construction and analyses
Eight different statuses were defined based on income data retrieved from the income register of SSB. SSB’s definition of what constitutes a main source of income has been applied and the person’s income has to fulfill two criteria: (a) to have an income equal to, or more than 1.5G, and (b) this income must represent the highest amount of the income sources. G is the basic amount, directly linked to in the National Insurance scheme. The eight income statuses were ‘social assistance’, ‘disability benefits’, ‘earnings from work’, ‘work assessment allowance/time-related disability benefit/social and medical rehabilitation’ and ‘unemployed compensation’. Furthermore, we defined one status called ‘no main income’. This means that the total income was 1.5G or more, but none of the income components was more than 1.5G. The two remaining statuses were ‘economically dependent’, that is the total income was below 1.5G, and ‘death’. These eight statuses were collapsed into four groups: ‘social assistance’ (included also ‘no main income’ and ‘economically dependent’), ‘disability benefits’, ‘work assessment allowance’ (included ‘social and medical rehabilitation’ and ‘time-related disability benefits’) and ‘earnings from work’, a status with a main income above 1.5G from work. All analyses were performed using Stata, version 12. Given that the dependent variable is categorical, multinomial logistic regression has been employed in the analysis and relative risk ratios are reported.
Ethical permissions
This study is approved by The Norwegian Data Protection Authority, the National Committee of Research Ethics in Social Sciences and Humanities, The Norwegian Directorate of Labour and Welfare, The Regional Committees for Medical and Health Research Ethics, The Causes of Death registry and SSB.
Results
As shown in Table II, the LTRs were divided into four groups based on the presence or absence of pain and/or psychological distress. One group had neither pain nor psychological distress (n = 137). One group reported having only pain (n = 61), one group reported having only psychological distress but not pain (n = 98), and one group reported having both pain and psychological distress (n = 160). Sample characteristics about sociodemographic status and general health in 2005 and 2013 are shown in Table II.
Differences in sociodemographic characteristics between the four groups with and without pain and psychological distress – reported in 2005 (n = 456).
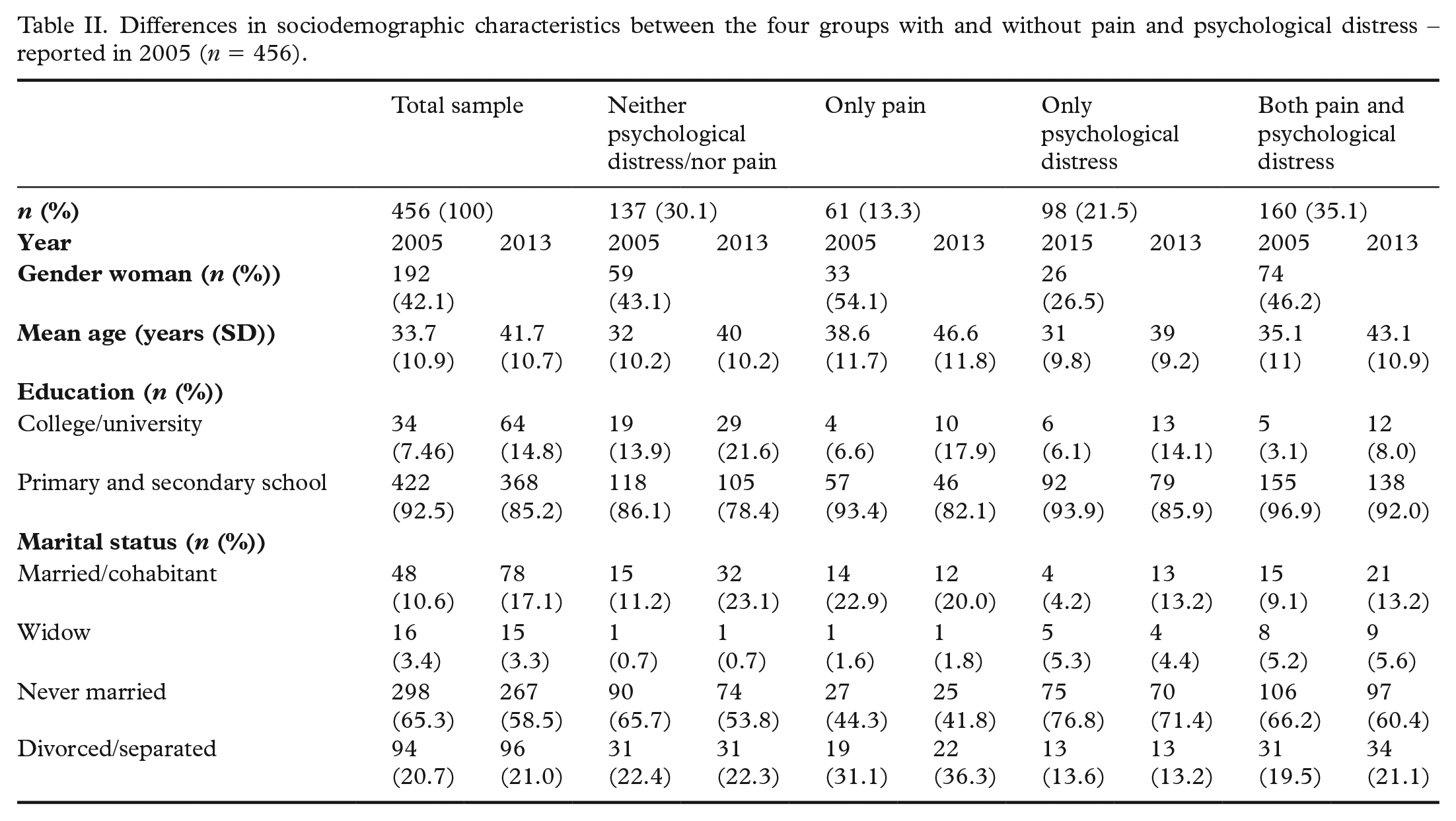
The mean age of the LTRs in 2005 was 33.7 years and 42% were woman. There were more women in the group ‘only pain’ than in the other three groups. LTRs who reported neither pain nor psychological distress and LTRs with only psychological distress were younger than the LTRs with only pain and LTRs with both pain and psychological distress.
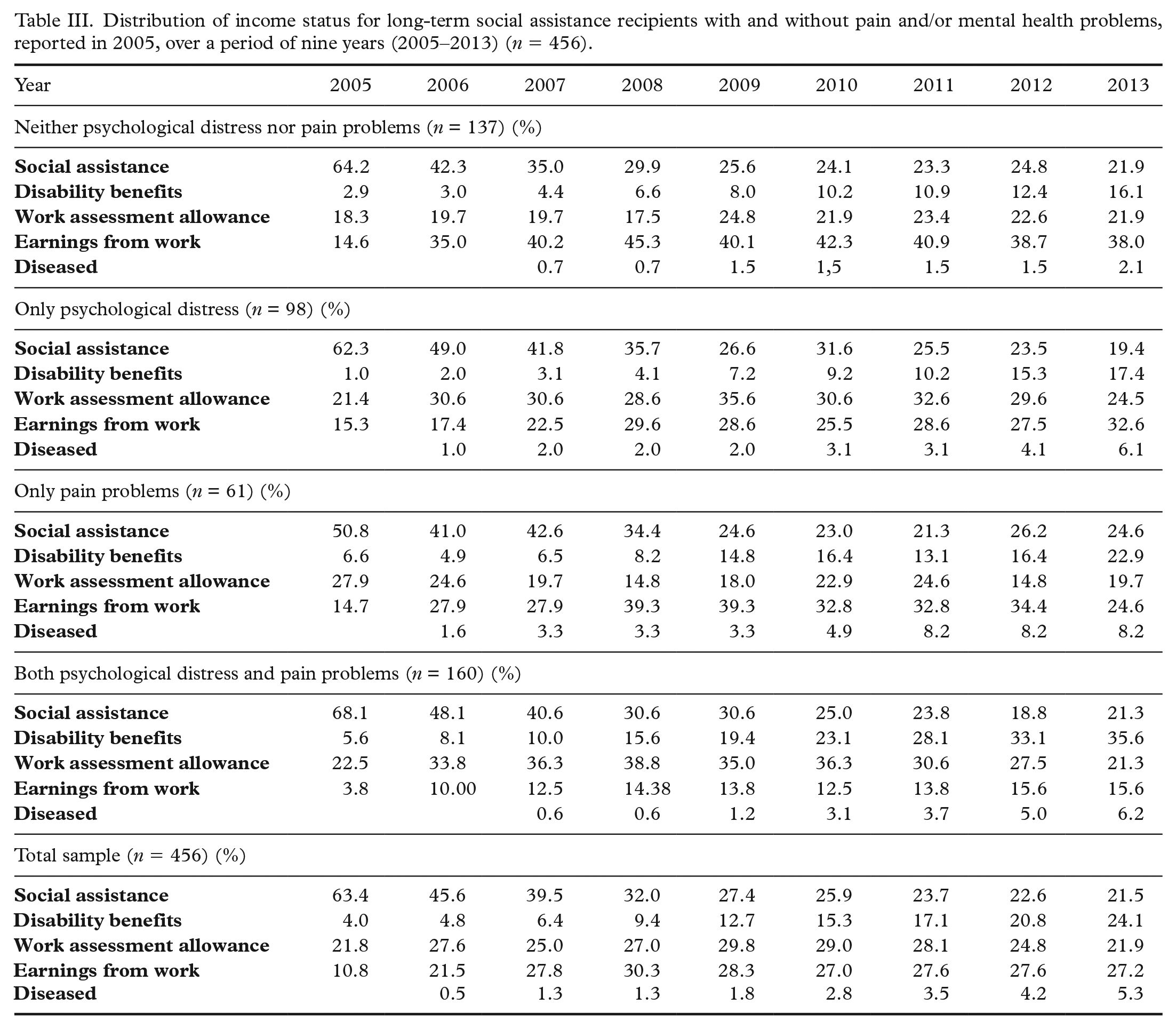
Distribution of income sources for LTRs with and without pain and/or psychological distress for each year in the period of nine years (2005–2013) are shown in Table III and Figure 2.
Distribution of income status for long-term social assistance recipients with and without pain and/or mental health problems, reported in 2005, over a period of nine years (2005–2013) (n = 456).
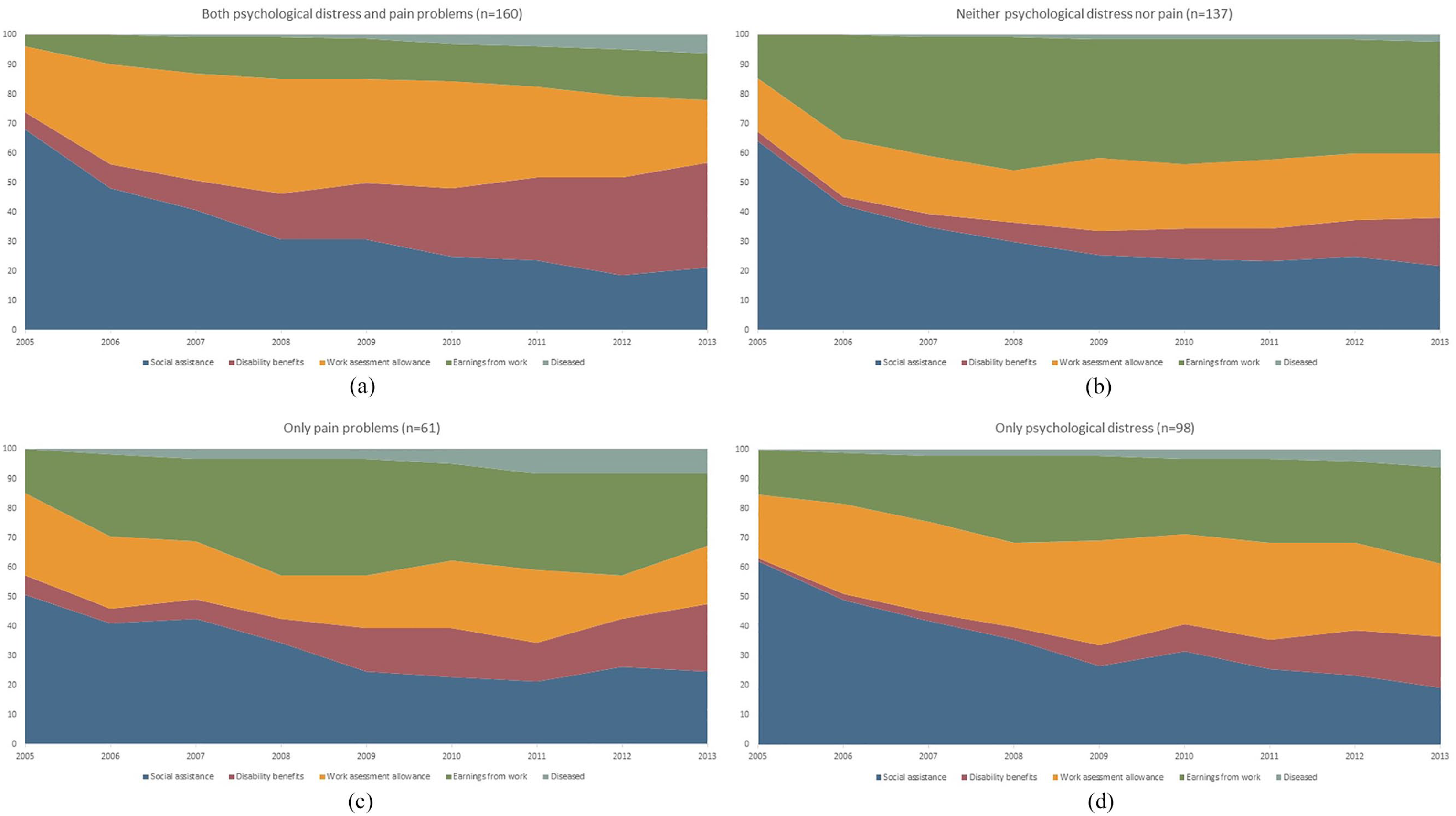
Patterns of main income over nine years in groups with and without psychological distress and pain problems reported in 2005: (a) both psychological distress and pain (n = 160); neither psychological distress nor pain (n = 137); (c) only pain (n = 61); (d) only psychological distress (n = 98).
In the group reporting neither psychological distress nor pain problems, the percent with earnings from work as main source of income (14.6–38.0%) and disability benefits (2.9–16.1%) increased over the period and the percent with social assistance status decreased (64.2–21.9%). The proportion with work assessment allowance stays almost the same during the nine-year period. The same pattern is shown in the group with only psychological distress. In the group reporting pain problems, the proportion with earnings from work (14.8–25.0%) and disability benefits (6.7–23.0%) as their main income sources showed an increase. The proportion with social assistance as their main source of income decreased over the period (62.2–19.4%), and the proportion of those who had work assessment allowance as main income source (27.9–19.7%) also decreased. In the group with both psychological distress and pain problems, the proportions who had social assistance decreased (68.2–21.5%) and the proportions with disability benefits as main income sources increased over time (5.6–36.6%).
The multiple multinomial logistic regression analysis (Table IV) shows that having both psychological distress and pain in 2005 is significantly associated with having disability benefits as main source of income in 2013, compared to those LTRs with neither psychological distress nor pain (relative risk ratio (RRR) 2.32, p = 0.03). Higher age and having worked more than 6 months is associated with earnings from work as main source of income and disability benefits. Also, higher age is associated with having work assessment allowance as main source of income in 2013.
Multinomial Logistic Regression showing the relative risk ratios (RRRs) between social assistance as main source of income in 2013 versus disability benefits, earnings from work or work assessment allowance according to health status in 2005 (n = 456).
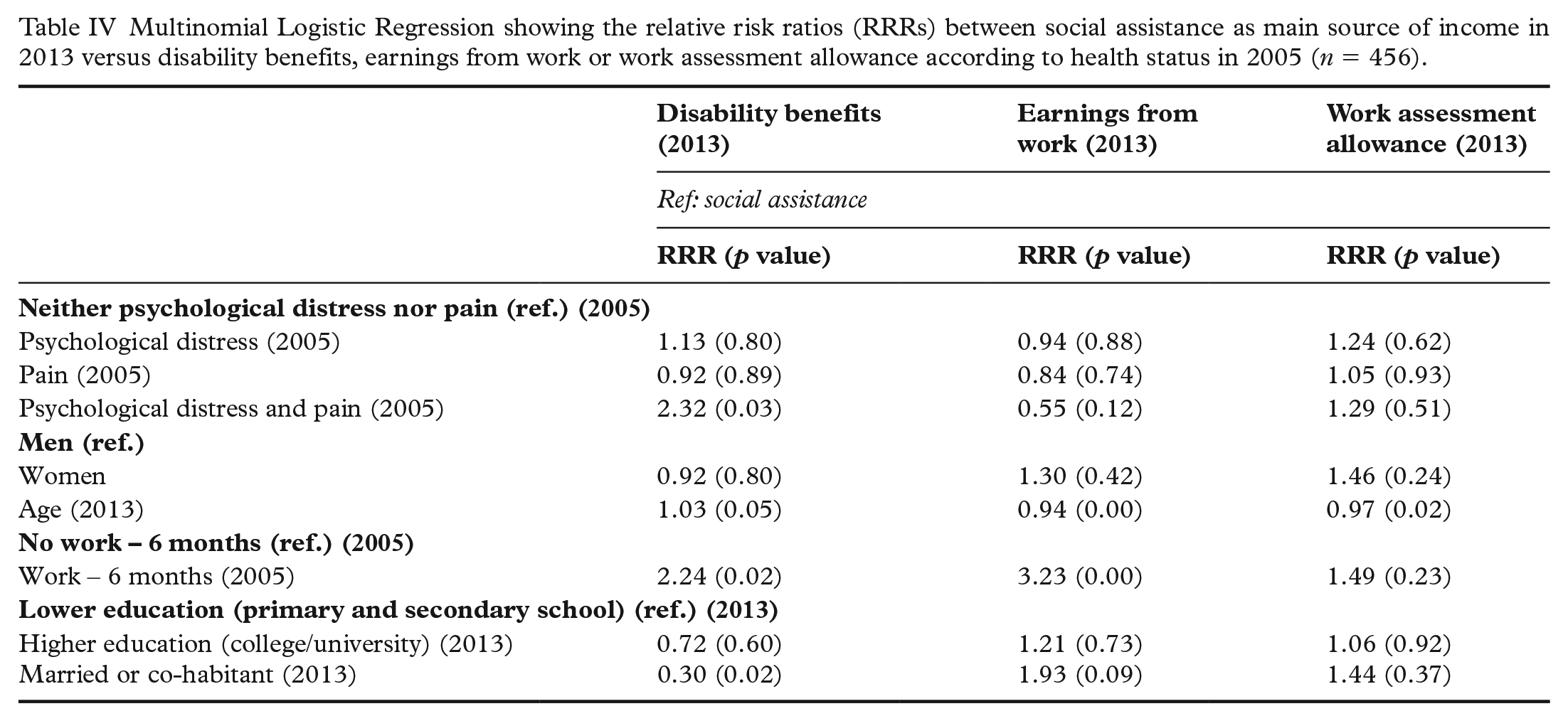
Being married or cohabitants in 2005 is associated with earnings from work (RRR 3.23, p = 0.00) and disability benefits (RRR 1.93, p = 0.09). Of the LTR who were granted disability benefits during the nine-year period (n = 151), the largest primary diagnosis group for receiving disability benefits (n = 110) were those with mental disorders. Of these, 41 individuals had substance abuse related diagnoses. Those in the second largest group (n = 21) had a muscle skeleton disease as their primary diagnosis. Heart, coronary and lung diseases were the reasons for receiving disability benefits for six individuals, with only two being diagnosed with a cancer disease.
Discussion
To our knowledge, this study is the first to investigate how pain and psychological distress, separately and in combination, are associated with income trajectories over nine years in a cohort of LTRs identified and surveyed in 2005. In this study, 70% of the LTRs report either pain, psychological distress or both, and this reflects the findings from ‘The Global Burden of Disease Study’. In other words, pain and depression disorders are two of the dominant causes of the global ‘disease burden’ [1]. A main finding in this study is that 38% of LTRs with neither pain nor psychological distress in 2005, have earnings from work as their main income in 2013. On the other side, only 16% of the LTRs who reported both pain and psychological distress in 2005 have earnings from work as their main income. A finding of income trajectories over nine years, was that those who suffered from both pain and psychological distress (35%), a ‘double burden’ of illness, over time gradually had disability benefit as their main income, as well as work assessment allowance. ‘The double burden’ in 2005 is associated with disability benefits in 2013, compared to social assistance benefits. In 2013, 36% of the LTRs with the ‘a double burden’ of illness have disability benefit as their main income. LTRs who report only pain or only psychological distress seem to have a less of a burden. The proportion that had social assistance as their main income source diminished over time, but yet the percentage exceeded 20% in 2013. This indicates that the primary goal of the social assistance system – to make the clients self-sufficient – is hard to achieve for LTRs.
This finding is consistent with what we initially assumed: LTRs are extra burdened by pain and psychological distress, and this has consequences for their life opportunities and income trajectories. Findings from a Swedish study show that psychological distress and musculoskeletal pain were associated with being poor at least once in life [24].
In one way, the results from this study could be seen as a great success for the welfare state as it seems that the sick do indeed get long-term financial aid, which they probably need. On the other side, you can ask why these persons still have mental health problems after nine years? Previous studies from different countries have documented that rates of health problems were high among social assistance or welfare recipients and especially the burden of mental health problems [22, 25–27]. In this study it is noteworthy that 72% (n = 110) of the total who begin receiving disability benefits during the nine-year period have mental disorders as the primary diagnosis for disability and 27% (n = 41) of these diagnoses were related to alcohol and substance abuse. The last finding reflects another important point in the Global burden of disease report: deaths from illicit drug use are high in Norway compared to other countries [28]. However, consistent with a previous study [29], this study shows that mental illness may be a contributing factor to later receipt of different types of welfare payments. The present study confirms that poor mental health may limit welfare recipients’ opportunities to work [22], and confirm a report from The Organization for Economic Co-operation and Development (OECD) [30], that mental illness seems to cause many people to leave the labour market and to take up social benefits. Further research must document and explain how mental illness can lead to disability and other types of social benefits. Undocumented ‘explanations/circumstances’ may draw attention to underlying personal characteristics and social factors that may predispose individuals to experience an increase in both poor mental health and the need to claim welfare benefits. Other factors may be related to stigma, different symptoms of mental health disorders, or other life events. It is also important to evaluate what services the healthcare system provides to people with psychological distress and mental disorders, and the quality of these various services.
The fact that only 27.0% of the total sample had earnings from work as their main source of income in 2013 implies that 70.0% had anyone (or a combination) of the three other income statuses as their main income source. This low overall proportion that had earnings from work as their main income after nine years shows that self-sufficiency is far from being achieved for this cohort. This finding portrays LTRs as people who, over a longer period of time, are in need of social benefits, either from the municipality (i.e. social assistance) or from the state (i.e. social security). Given the prevalence of health problems and lack of resources that they have, this is not too surprising, but it does provide a challenge for the healthcare services and the social policy. A previous Swedish study concluded that it is difficult to be self-sufficient after extended periods of social assistance recipiency [19]. Findings from this study confirms the explanation seen in previous studies, that this group is more vulnerable, with more mental illness and/or drug and alcohol abuse. However, having both pain and psychological distress seems to give the worst prospects for economic self-sufficiency.
A strength of the present study is the linking of health variables obtained in a survey from 2005 to registry information on income trajectories from 2005–2013. Another strength is that used instruments are valid and reliable. Further, the use of administrative registry data avoids bias. A limitation, however, is that there is no information available as to whether individuals in poor mental health were less likely to respond to the survey and, therefore, the estimates may underestimate the longitudinal association. Another limitation is that the distribution of the four groups resulted in there being relatively small sample sizes in the pain only group and in the psychological distress only group. The small sample, resulting in low statistical power, is especially evident in Table IV, were only few coefficients are significant. A third potential limitation is the fact that all information on illness is based on self-reporting and thus subject to socio-economic or work-related bias, or bias related to economic incentives to over report ill health. However, one should not overstate this possibility, since objective health outcomes – such as mortality and disability rates related to poor mental health – are high among the LTRs.
Conclusion
The income source trajectories over nine years and the distribution of main income sources at the end of the observation period varied according to which illness group the long-term recipients of social assistance benefits belonged to. The group that had a ‘double burden’ of disease, both pain and psychological distress, differed significantly from the group without any of these two health problems. Increasing percentages of the doubly burdened group had disability benefit as their main income source, whereas, in the ‘unburdened’ group, relatively many had earnings from work as their main income source. These contrasts were also statistically significant at the end of the observation period, nine years on. This study indicates that the primary goal of the social assistance system, to make the clients self-sufficient, is hard to achieve for long-term social assistance recipients. The large percentage with a ‘double burden of disease’ and the low level of self-sufficiency in this group illustrate the need for health services as well as for work-related services and for smooth and seamless co-operation between healthcare institutions and the Labour and Welfare Administration (NAV).
Footnotes
Acknowledgements
Many thanks to our colleagues in the team, Kjetil A. van der Wel, Magne Bråthen and Ivar Lødemel for important comments and support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Norwegian Directorate of Labour and Welfare.