
Abstract
Chronic pain imposes substantial individual, occupational, and societal burdens. This study explores the prevalence, severity, and associated burden of chronic back pain and headaches—defined as pain experienced repeatedly or persisting for at least 3 months within the past 12 months—in a nationwide sample of the working population in Germany (N = 4,751). It also examines how demographic and psychosocial factors are associated with chronic pain. Among participants, 34.4% experienced mild, 25.1% moderate, and 13% (very) severe chronic back pain symptoms; 35.6% experienced mild, 20.1% moderate, and 10.8% (very) severe chronic headaches. Gender, age, sleep problems, and burnout were identified as key correlates of chronic back pain and headaches. These findings indicate that chronic pain may be more prevalent and burdensome than previously believed, underscoring the need for comprehensive prevention and management strategies that integrate both biological and psychosocial perspectives. Further research should investigate the underlying mechanisms and inform targeted interventions.
Introduction
Headaches and back pain are among the most prevalent pain conditions worldwide. According to the Global Burden of Disease (GBD) studies, almost 3 billion people suffered from migraine or tension-type headaches in 2016 alone (GBD Headache Collaborators, 2018). In a 2020 GBD study, 203 million people were estimated to have neck pain while 619 million experienced lower back pain (GBD Low Back Pain Collaborators, 2023; Wu et al., 2024). These conditions, particularly when chronic, are debilitating, and negatively affect well-being, quality of life, ability to work, and the ability to participate in leisure activities (Fine, 2011; Raffaeli and Arnaudo, 2017).
In Germany, the country in which the current study was conducted, headaches and back pain are common. A nationwide study from 2020 on the burden of disease (N = 5,009; representative of the German-speaking population aged 18 and older) reported that 57.5% of women and 44.4% of men experienced at least one headache in the past year (Porst et al., 2020). Comorbidities and social factors were also investigated, showing that headache disorders, especially migraines, are often accompanied by depression and anxiety symptoms, as well as other pain conditions such as neck and lower back pain. Notably, gender emerged as a factor strongly associated with chronic conditions, with women being 4.7 times more likely to experience migraines and 2.7 times more likely to experience tension-type headaches than men. Education, unemployment, and partnership were not significantly associated with the prevalence of headache disorders, while social support emerged as a protective factor. Data from the same sample published in another article (von der Lippe et al., 2021), indicated that 61.3% of the respondents experienced back pain at least once in the past year, with a higher prevalence among women, as similarly found for headaches. In both studies, age was statistically significantly associated with chronic pain. However, while the prevalence of chronic headaches decreased with age, the opposite was true for back pain. Further psychosocial correlates of chronic pain were not investigated in these studies. However, the role of various psychosocial factors in the development and persistence of chronic pain, including psychological characteristics (e.g. optimism, self-efficacy, coping strategies, and catastrophizing), psychological disorders (e.g. anxiety and depression), social environment (e.g. social interactions, social support, and family), and socio-economic status (e.g. education and income) has long been recognized (see reviews Driscoll et al., 2021; Edwards et al., 2016; Meints and Edwards, 2018; Wilson et al., 2025). Still, most studies have focused on a subset of factors, while comprehensive studies investigating a wide range of psychosocial factors in the same population are lacking. Such studies would offer the opportunity of comparing the effects of different factors in order to identify the most relevant ones for preventing and managing chronic pain.
The aim of this study is twofold. First, we describe the prevalence, severity, and associated burden of headaches and back pain symptoms in a representative sample of the working population in Germany. We chose to focus on the working population because employed individuals encounter specific stressors, working conditions, and psychosocial dynamics that can influence the prevalence, severity, and burden of pain conditions. For example, people in lower occupational classes (e.g. unskilled workers) are more likely to report pain symptoms than people in higher occupational classes (e.g. skilled workers, Mehlum et al., 2008; Toivanen, 2011). Moreover, sedentary behavior, which is common among white-collar workers, has been associated with back pain, especially among older individuals (Baradaran Mahdavi et al., 2021; de Freitas Cardoso et al., 2022). However, associations between blue-collar jobs and pain symptoms (e.g. shoulder, lower back, and foot pain) have also been reported, and these symptoms are more prevalent among blue-collar workers (<50 years old) than among their white-collar counterparts of the same age (de Freitas Cardoso et al., 2022; Yang et al., 2016). Second, we explore associations between these pain indicators and a wide range of socio-demographic variables (e.g. gender, age, socio-economic status, and education) together with other important psychosocial factors that have been linked to pain, such as sleep, stress, and social support (Bernier Carney et al., 2021; Edwards et al., 2016; Meints and Edwards, 2018; Porst et al., 2020; Whibley et al., 2019). The identification of relevant socio-demographic and psychosocial factors is critical for developing targeted prevention strategies that could ultimately reduce the individual burden of these conditions and their broader health and societal costs.
Methods
Sample
We conducted a web-based study with a nationwide offline-recruited sample of German-speaking residents in Germany aged 18 or older. Recruitment occurred via forsa.omninet, which provides a panel of the population in Germany that is representative of sex, age, education, and federal state for the adult residential population with internet access (applying to 92% of the households in Germany; Statista, 2024). The forsa.omninet panel uses a multi-stage random sampling process, which is based on the telephone master sample of the Association of German Market and Social Research Institutes (ADM, 2012; Häder and Gabler, 1998). It uses a sampling frame to representatively select samples of the population living in private households. Thereby, every household in Germany had the same statistical chance of being selected. Thus, infrequent internet users could be included, and self-selection into the panel was avoided. The initial sample included 47,406 individuals (first wave). We used data from the fourth wave, which consists of previous participants and refreshment samples to compensate for demographic imbalances that occurred over time due to selective participation by hard-to-reach participants. In wave 4, 28,567 individuals were invited, including individuals who declined to participate in waves 2 and/or 3. In total, 13,452 individuals agreed to participate, and 12,168 completed the survey. Due to time constraints, the pain questions were asked in a random sample of 7,402 respondents (only in wave 4). For our analysis, we use 4,751 employed individuals (i.e. full-time, part-time, minimally employed, partially retired, and other types of employment). Participants with missing information on one or more measures or who selected “no response” on single-item measures were removed from the analyses (see more details in Table 1 and information on the rowmean function, below, for how missing data/“no response” answers in multi-measure items were handled).
Descriptive statistics.
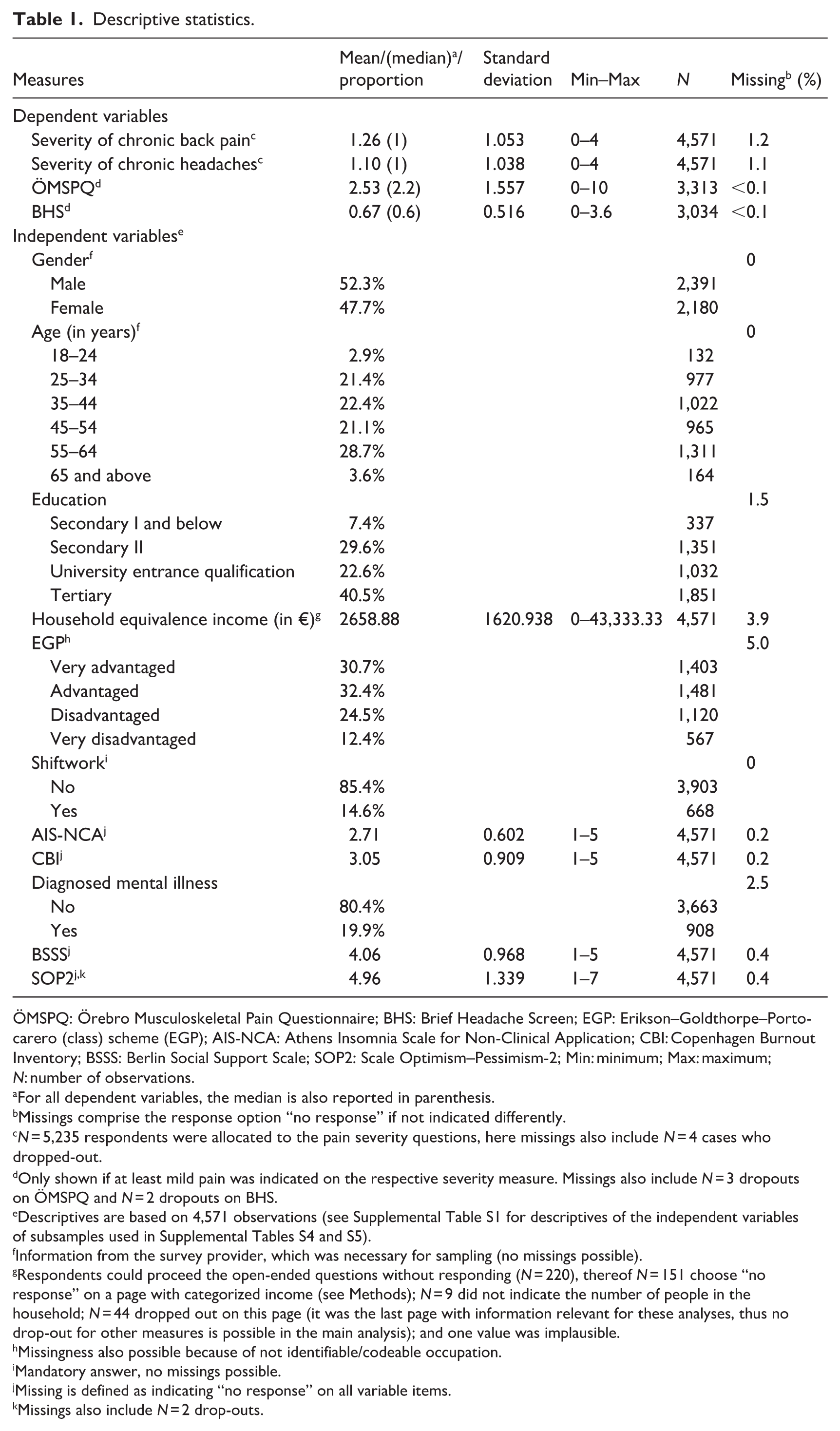
ÖMSPQ: Örebro Musculoskeletal Pain Questionnaire; BHS: Brief Headache Screen; EGP: Erikson–Goldthorpe–Portocarero (class) scheme (EGP); AIS-NCA: Athens Insomnia Scale for Non-Clinical Application; CBI: Copenhagen Burnout Inventory; BSSS: Berlin Social Support Scale; SOP2: Scale Optimism–Pessimism-2; Min: minimum; Max: maximum; N: number of observations.
For all dependent variables, the median is also reported in parenthesis.
Missings comprise the response option “no response” if not indicated differently.
N = 5,235 respondents were allocated to the pain severity questions, here missings also include N = 4 cases who dropped-out.
Only shown if at least mild pain was indicated on the respective severity measure. Missings also include N = 3 dropouts on ÖMSPQ and N = 2 dropouts on BHS.
Descriptives are based on 4,571 observations (see Supplemental Table S1 for descriptives of the independent variables of subsamples used in Supplemental Tables S4 and S5).
Information from the survey provider, which was necessary for sampling (no missings possible).
Respondents could proceed the open-ended questions without responding (N = 220), thereof N = 151 choose “no response” on a page with categorized income (see Methods); N = 9 did not indicate the number of people in the household; N = 44 dropped out on this page (it was the last page with information relevant for these analyses, thus no drop-out for other measures is possible in the main analysis); and one value was implausible.
Missingness also possible because of not identifiable/codeable occupation.
Mandatory answer, no missings possible.
Missing is defined as indicating “no response” on all variable items.
Missings also include N = 2 drop-outs.
All data analyzed here come from the fourth wave, with few exceptions (see more details in the description of the instruments). In the analytical sample, 47.7% were female and the mean age was 46.01 years (standard deviation = 12.223). Participation was voluntary and data were pseudonymized. Upon completion, respondents received bonus points (worth ~$3.00) which could be exchanged into vouchers, charity lottery tickets, or donations to UNICEF. Ethics approval was received from the Ethics Committee of the University of Erfurt (reference number: EV-20220830) and informed consent was obtained from all participants.
Instruments
Severity of pain symptoms: Respondents indicated whether they had been repeatedly and/or for a prolonged period (at least 3 months) experiencing back pain and/or headaches in the past 12 months (following the ICD-11 classification criteria for chronic pain; Treede et al., 2015). Response options indicated the intensity of the experienced pain (“never” [value 0], “mild pain” [1], “moderate pain” [2], “severe pain” [3], and “very severe pain” [4]), while “no response” was also possible.
Örebro Musculoskeletal Pain Questionnaire (ÖMSPQ): Respondents indicating at least mild chronic back pain received nine items of the ÖMSPQ (Linton et al., 2011; Schmidt et al., 2016, 2023). The ÖMSPQ assesses pain severity in the past 4 weeks (one item on an 11-point scale ranging from “no pain–0” to “strongest imaginable pain–10”) and associated burden; impact of pain on respondents’ ability to function normally in their lives (four items with response options ranging from “possible without any adverse effect–0” to “absolutely impossible due to pain–10”), emotional state (two items assessing feeling sad and tense/worried, with response options on a 11-point scale ranging from “not at all–0” to “extremely–10” and “completely calm and relaxed–0” to “completely tense and worried–10”), and the impact of physical activity on pain symptoms (two items with response options on a 11-point scale ranging from “not true at all–0” to “completely true–10”). Internal consistency was 0.81 (calculated from item responses with a sample size ranging from 3,227 to 3,313, considering pairwise item covariances). Unweighted mean scores (higher scores indicate more pain severity and associated burden) were calculated using Stata’s rowmean function for this and all other multi-item measures. This function excludes respondents only if they did not provide answers to all items, therefore allowing to keep higher case numbers compared to listwise deletion. However, it assumes that unanswered items do not substantially differ.
Brief Headache Screen (BHS): Respondents indicating at least mild chronic headaches, received five questions of the BHS (Maizels and Burchette, 2003) asking about the pain frequency of severe headaches (that impact day-time functioning) and mild or less severe headaches, while the other items covered the impact of headaches on work and leisure as well as medication overuse (frequency of pain relief or other medication use to alleviate headache symptoms, and prescription medication use to prevent headaches). Response options were “almost never” [0], “1 day a month or less” [1], “2 days a week to 2 days a month” [2], “3–4 days a week” [3], and “daily or almost daily” [4]. An unweighted mean score was computed (higher scores indicate more pain severity and associated burden). Internal consistency was 0.75 (N = 3,001–3,034).
Household equivalence income: Respondents estimated their household monthly net income using an open-ended question (cf. Beckmann et al., 2016). If no answer was provided, income categories were shown. The mean value for income categories was used, while for the last open-ended category (“20,000 and more”), the value 20,000 was used (Celeste and Bastos, 2013). The equivalence income considers the number of household members with the OECD-modified scale (Hagenaars et al., 1994). The first adult received a weight of 1, each additional adult had a weight of 0.5, and each child (under 14 years) had a weight of 0.3. Income was divided by this weight.
Erikson–Goldthorpe–Portocarero (Class) Scheme (EGP): Based on an open-ended question on jobs and using the classification of occupations, which refers to the International Standard Classification of Occupations (ISCO), the EGP was created to describe the class situation of respondents by assigning occupations to classes based on their employment relations (Brauns et al., 2000; Goldthorpe, 2016; Goldthorpe and McKnight, 2006). While the scheme consists of up to 10 categories, the classification can be also used to divide individuals into four main categories: “very advantaged” (i.e. high-status professional and managerial occupations, often associated with significant wealth and influence; EGP I) [1], “advantaged” (i.e. middle-class occupations with a relatively high level of autonomy and income, but not at the top of the social hierarchy; EGP II) [2], “disadvantaged” (i.e. lower-level, non-manual jobs with limited autonomy and lower incomes; EGP IIIab, IVab) [3], and “very disadvantaged” (i.e. low-status, manual labor occupations with low income and minimal job security; EGP IVc, V, VI, VIIab) [4] (cf. Hoven et al., 2015).
Shiftwork: Respondents indicated whether they had no shiftwork [0] or had worked in shifts (e.g. nightshift) during the past 12 months [1].
Athens Insomnia Scale for Non-Clinical Application (AIS-NCA): We used the seven-item AIS-NCA to assess problems with sleep and daytime functioning (Sattler et al., 2022, 2023). Responses were assessed on a five-point scale. Items were averaged to calculate a total score. Higher scores indicate more problems with sleep and daytime functioning. Internal consistency was 0.80 (N = 4,563–4,569).
Copenhagen Burnout Inventory (CBI): The CBI uses three items of the Copenhagen Psychological Questionnaire (COPSOQ II; Pejtersen et al., 2010) to assess feelings of burnout in the past 12 months. A mean score was computed (higher scores indicate more frequent burnout). Internal consistency was 0.87 (N = 4,565–4,569).
Diagnosed mental illness: Respondents’ lifetime diagnosis of mental illnesses, such as depression, Attention Deficit Disorder (ADD), Attention Deficit Hyperactivity Disorder (ADHD), phobias, or dementia, was assessed upon entry in the study by asking about the presence of a lifetime diagnosis. Potential new diagnoses in the past 12 months were assessed in the subsequent waves. Responses were coded into a binary indicator for “no mental illness” [0] and “at least one mental illness diagnosis” [1].
Berlin Social Support Scale (BSSS): Instrumental and emotional social support were assessed with four items of the BSSS (Schwarzer et al., 2003). A mean score was computed (higher scores indicate more support). Internal consistency was 0.94 (N = 4,542–4,565).
Optimism–Pessimism Scale (SOP2): The SOP2 assesses generalized and relatively stable expectations of future events (Kemper et al., 2013). It uses only two items to assess how optimistic and pessimistic someone generally is. For some respondents, it was measured in wave 1, for others in waves 3 or 4. A mean score was computed after reverse-coding the pessimism item (higher scores indicate more optimism). Internal consistency was 0.88 (N = 4,571).
Statistical analysis
We employed partial proportional odds models, commonly referred to as generalized ordered logit models, using the Stata command gologit2 (Williams, 2006, 2016). The gologit2 model offers several advantages for analyses involving ordinal outcomes. It provides diagnostics to test the proportional odds assumption (also known as the parallel lines assumption) and can selectively relax this assumption for specific explanatory variables when necessary. This flexibility is more advantageous than traditional ordinal logistic regression models, which universally impose the proportional odds assumption while being more parsimonious than, for example, multinomial models.
Partial proportional odds models are particularly suitable for analyzing the relationship between the ordinal variables “severity of back pain” and “severity of headaches” with various sociodemographic and psychosocial factors. The model estimates the effects of independent variables on the odds of being in higher categories of the ordinal outcome variable, accommodating potentially varying effects across the outcome categories (when the parallel lines assumption is not met). Odds ratios (ORs) greater than 1 indicate that higher values on the explanatory variable increase the likelihood of reporting a higher pain severity category than the current one, reflecting positive effects. ORs less than 1 indicate an increase of the likelihood of being in the current or lower pain severity category, reflecting negative effects. An OR equal to 1 suggests no effect. We utilized Gamma parametrization (Lall et al., 2002; Peterson and Harrell, 1990), which presents coefficients for the first test (“no pain” vs “mild pain,” “moderate pain,” “severe pain” and “very severe pain”) and then quantifies the extent (magnitude and direction) to which the proportional odds assumption is violated for certain explanatory variables in other tests (e.g. “no pain” and “mild pain” vs “moderate pain,” “severe pain” and “very severe pain”).
For ÖMSPQ and BHS, generalized linear models (GLM) with the log link function were used to account for the right-skewed distribution of these variables and the presence of heteroscedastic residuals. We present exponentiated log link coefficients (eβ) representing rate ratios (RRs). RRs indicate the multiplicative effect of a coefficient. RRs greater than 1 indicate that higher values on the explanatory variable are associated with higher values of the dependent variable (ÖMSPQ and BHS scales); RRs less than 1 indicate that higher values on the explanatory variable are associated with lower values of the dependent variable. RRs equal to 1 suggest no effect. For ease of interpretation and to allow for a comparison of the strength of effects, all multi-item scales and household equivalence incomes were normalized to the interval [0;1], wherein “0” represents the empirically lowest level of the respective measure and “1” represents the highest level. In the Results section, ORs and RRs of the full models (which are adjusted for all other independent variables) are displayed in Figures 2 and 3 with 95% confidence intervals (relying on robust standard errors). Thereby, we highlight all statistically significant associations based on a significance level set at α < 0.05, while we put the results into perspective based on effect sizes in the Discussion section. We additionally report the ORs and RRs in the Supplemental Information (SI; Supplemental Tables S2–S5), which include two additional models, one with only sociodemographic and one with only psychosocial variables.
Results
Almost three-quarters of the respondents (72.5%) reported having at least mild back pain and two-thirds (66.5%) reported having at least mild headaches repeatedly or for at least 3 months in the past 12 months (Table 1; Figure 1, Panels A–B). Respondents most frequently reported mild symptoms (34.4% back pain and 35.6% headaches) and least frequently very severe symptoms (2.7% back pain and 2.7% headaches). While 57.1% reported both back pain and headache symptoms being at least mild, only 3.3% reported that both pain symptoms were (very) severe. According to the ÖMPSQ scores distribution, the back pain’s associated burden during the past 4 weeks was low for about one out of six of the respondents (16.2%, Panel C). Similarly, the majority of respondents reported a lower associated burden concerning headaches (BHS scores distribution; Panel D).
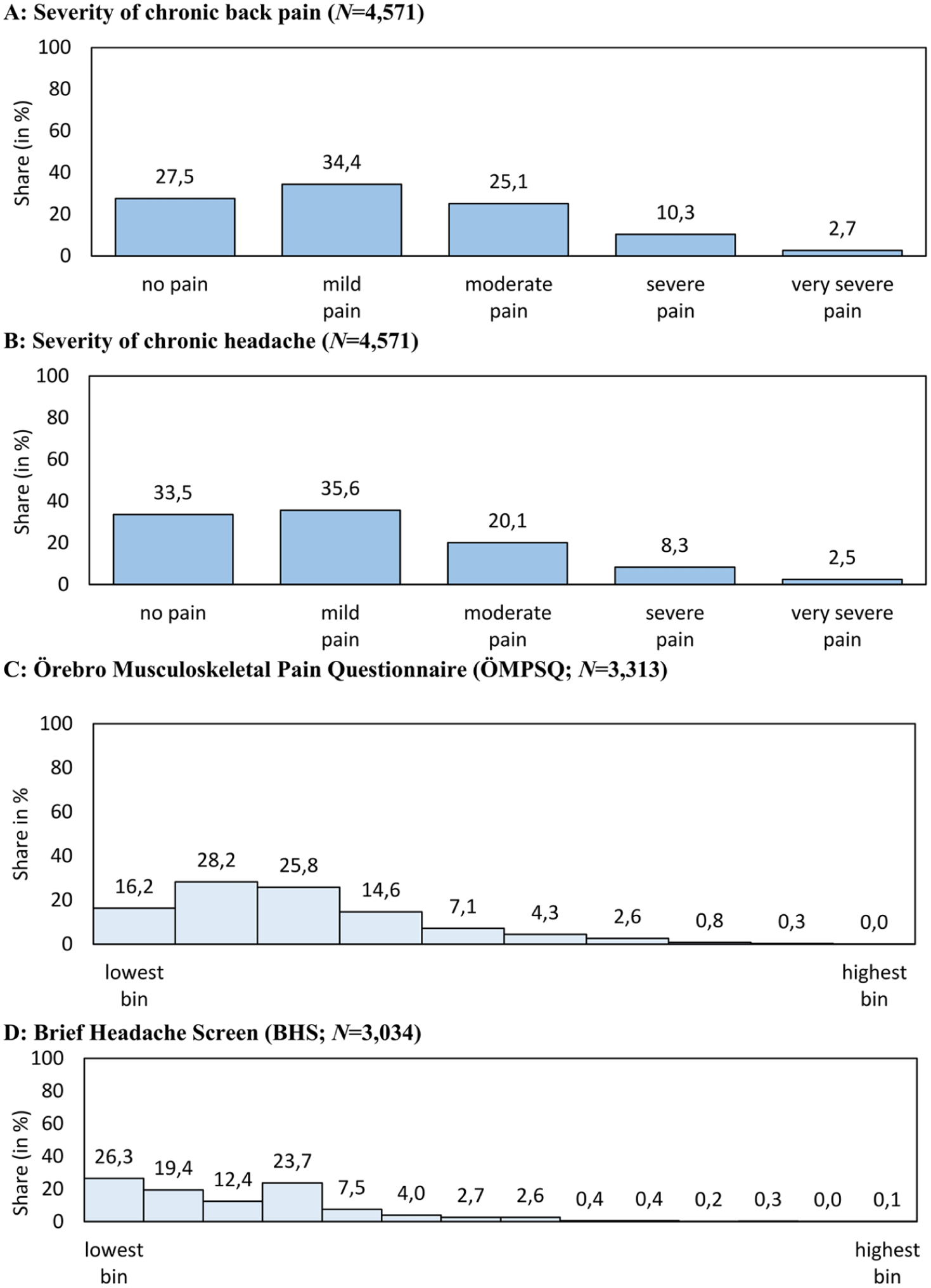
Share of respondents (in %) with no pain and different severities of pain symptoms that were experienced repeatedly and/or for prolonged periods (at least 3 months) in the past 12 months (Panels A and B), as well as relative frequency histograms for the associated pain burden (Panel C with a bin size of 1 and Panel D with a bin size of 0.25).
Panel A in Figure 2 (see also Supplemental Table S2) shows that females were 17.1% more likely than males to report having experienced any chronic back pain (indicated by an OR of 1.171). The proportional odds assumption was not met for gender (pPO = 0.033), indicating that the effect varied across pain severity levels. The gender effect was only statistically significant when comparing “no pain” to any level of pain, and it was not statistically significant for greater symptom severity. The Gamma parametrization indicates that the OR of 1.171 was statistically significantly (pGamma = 0.006) different from the OR of 0.869 for “no pain,” “mild pain,” and “moderate pain” versus any higher pain severity level, while it was not statistically significantly different from the other two ORs (pGamma > 0.05).
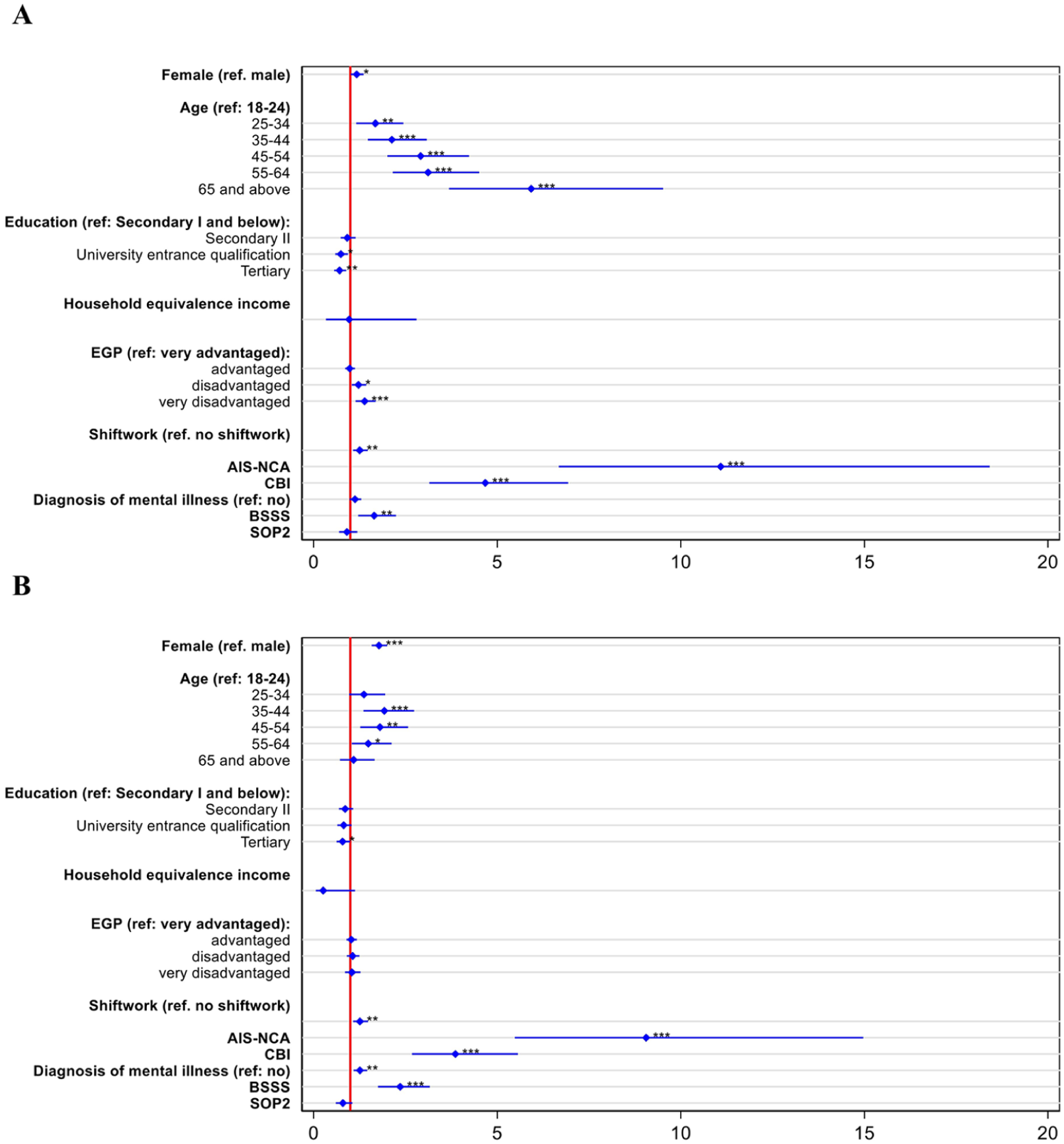
Multivariate associations between severity of chronic back pain (Panel A, N = 4,571) and chronic headaches (Panel B, N = 4,571) with demographic and psychosocial variables.
Age was also associated with chronic back pain severity, with individuals in the oldest age group (65 and above) most likely to report higher levels of pain compared to the reference group (18–24 years old). For this variable (and for the following variables except for burnout and social support) the proportional odds assumption was not violated, indicating a similar effect of age across the different levels of pain severity. Moreover, individuals with university entrance qualifications and with tertiary education were less likely to report higher levels of chronic back pain severity compared to the lowest education group. Similarly, individuals in very advantaged job classes were less likely to report higher levels of chronic back pain severity compared to individuals in (very) disadvantaged job classes. Regarding the psychosocial variables, sleep problems and burnout were positively associated with increased odds of having higher levels of chronic back pain severity. While the effect of sleep problems was similar across pain levels, the proportional odds assumption was not met for burnout (pPO = 0.039). Higher levels of burnout were statistically significantly associated with increased ORs of reporting pain for all levels of symptom severity. However, the OR for “no pain” versus any level of pain was only statistically significantly different from the OR for the highest pain severity level, that is, any pain versus “very severe pain” (pGamma < 0.05). Individuals who received more social support were more likely to report any chronic back pain. However, the odds of the effect are not proportional (pPO = 0.012) but rather appear to decrease, although the difference is not statistically significant in the final cumulative logit. Household equivalence income, shiftwork, diagnosis of mental illness, and optimism were not statistically significantly associated with chronic back pain severity.
Reporting chronic headaches and greater pain severity (Panel B in Figure 2 and Supplemental Table S3) was more likely among females than males as well as for those in the middle-aged groups (35–64 years old) compared to the youngest age group (18–24 years old). The proportional odds assumption was met for gender and all age groups except for the 55–64 age group (pPO < 0.001). The effect for this age group statistically significantly decreases with increasing pain symptom severity (except for the comparison between the first effect and the final cumulative logit). Individuals with a tertiary education had lower odds of reporting higher levels of chronic headaches compared to the lowest educational group. Shiftwork was also associated with chronic headache severity, with those working in shifts reporting higher odds compared to those not working in shifts. This likelihood was also elevated for individuals reporting more sleep problems, burnout, and social support. Like for back pain, the proportional odds assumption was not met for burnout (pPO = 0.013) and social support (pPO = 0.012). The effect of burnout tends to increase (although the difference is not statistically significant when comparing the first effect to “no pain” and “mild pain” vs higher levels), while the effect of social support tends to decrease (although the difference is not statistically significant when comparing the first effect with the final cumulative logit). Further factors were not significantly associated with the likelihood of reporting headaches.
Panel A in Figure 3 (see also Supplemental Table S4) shows elevated ÖMPSQ scores for females compared to males (RR = 1.058, indicating that the ÖMPSQ scores for females are about 5.8% higher compared to males) and for individuals in very disadvantaged job classes (RR = 1.123, indicating that the ÖMPSQ scores for individuals in very disadvantaged job classes are approximately 12.3% higher compared to individuals in very advantaged job classes). Individuals with higher education had lower scores than those with the lowest education. Individuals with higher household equivalence income, greater social support and higher optimism had also lower ÖMPSQ scores. In contrast, sleep problems, burnout, and having a mental illness diagnosis were positively associated with the ÖMPSQ. Other factors were not significantly associated with the ÖMPSQ.
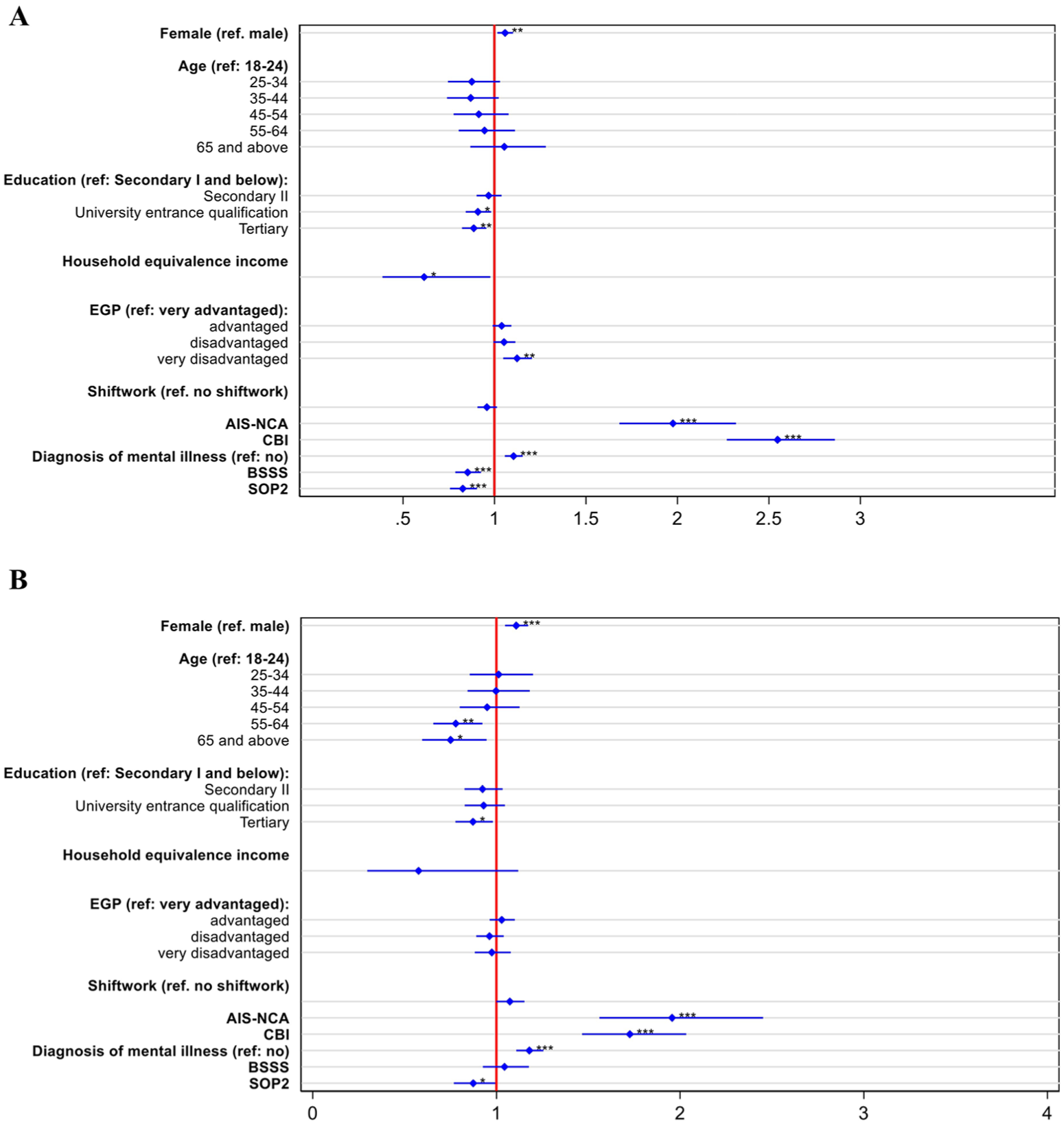
Multivariate associations between ÖMSPQ (Panel A, N = 3,313) and BHS (Panel B, N = 3,034) with demographic and psychosocial variables.
Panel B in Figure 3 (see also Supplemental Table S5) shows that BHS scores were higher among females, individuals reporting more sleep problems, those with higher levels of burnout, and in individuals with a diagnosed mental illness. BHS scores were lower in the age groups 55–64 and 65–74 compared to the youngest age group, as well as among individuals with tertiary education compared to the lowest educational group. Moreover, optimism was negatively associated with BHS. Further factors were not significantly associated with the BHS scale.
Discussion
The aim of this study was to investigate demographic and psychosocial factors associated with chronic back pain and headaches in a nationwide sample of the working population in Germany. We collected and analyzed data on back pain, headaches, the associated burden, and a wide range of demographic and psychosocial variables including gender, age, occupation classification, social support, sleep problems, and burnout.
Our results indicate that 72.5% of respondents reported having at least mild back pain and 66.5% reported having at least mild headaches repeatedly or for at least 3 months during the past 12 months. Chronic back pain and headache symptoms also showed a high comorbidity rate of 57.1%. A high comorbidity of these two pain conditions was also found in the 2020 German Burden of Disease study (Porst et al., 2020) and deserves particular attention because of the potential higher burden experienced by these individuals. The prevalence rates of chronic symptoms for both types of pain in our study are higher than in previous studies involving different samples, including the general population (Breivik et al., 2006; Cimas et al., 2018). For instance, the 2020 German Burden of Disease study reported that 61.3% of respondents experienced back pain at least once in the past 12 months, but only 15.5% were classified as having chronic back pain (Porst et al., 2020; von der Lippe et al., 2021).
The variability in prevalence estimates across studies may be due to differences in how chronic pain is defined (e.g. continuous/daily vs intermittent/recurrent pain and which diagnostic criteria are applied), which time interval is considered (e.g. the last 3 or 6 months), what type of assessment tool is used (e.g. prevalences gleaned from questionnaires are usually higher than those from clinical interviews), and which population is sampled (working vs general population; Ospina and Christa, 2002; Rometsch et al., 2025). We classified participants as having chronic pain based on self-report measures, which might lead to higher prevalences than when using data derived from official medical records (i.e. medical diagnosis). Also in our study, the frequency of pain was described as “repeatedly” for at least 3 months rather than “daily” as was done in the 2020 German Burden of Disease study. Moreover, instead of a simple yes/no response option, we used a scale ranging from “never” to “very severe pain,” which might have prompted some respondents to answer “mild,” whereas if they would need to choose between “yes” or “no,” they might have answered “no.” Thus, our measure was likely more sensitive to detecting the presence of pain whereas dichotomous measures could be prone to overlooking the presence of milder, but still relevant, chronic pain. The symptom severity most frequently mentioned was “mild” (34.4% for back pain and 35.6% for headaches), but still 13% and 10.8% of the respondents reported severe-to-very-severe pain symptoms for back pain and headaches, respectively. Such prevalences align more closely with previous studies (Breivik et al., 2006; Cimas et al., 2018; Rometsch et al., 2025). Even with this more conservative approach, the prevalences are concerning and, given the high health and financial costs associated with chronic pain, they should be considered by health policymakers (GBD Low Back Pain Collaborators, 2023; Vos et al., 2020).
Our findings also reveal that gender and age are associated with pain symptoms, consistent with several previous studies (GBD Low Back Pain Collaborators, 2023; Grol-Prokopczyk, 2017; Porst et al., 2020; von der Lippe et al., 2021). Females were about 17% more likely to report chronic back pain and 78% more likely to report headaches than males. For chronic back pain the effect of gender varied across symptom severity and tended to be lower with increasing symptom severity (albeit not for every pain severity category). Associated burden was also about 6% higher among females for both chronic back pain (ÖMPSQ score) and 10% higher for headaches (BHS scale). Increasing age was linked to higher odds of reporting higher levels of back pain and headaches. For instance, the odds of reporting any level of back pain versus “no pain” were five times higher for respondents older than 65, and those between 35 and 64 had about double the odds of reporting any level of headaches versus “no pain” compared to the youngest group. Age was not statistically significantly associated with back-pain-related burden, while older respondents reported reduced headache-pain-related burden compared to younger respondents.
We found that higher education was associated with lower reported pain severity concerning back pain and headache as well as associated burden. This aligns with previous studies linking low education to a higher risk for chronic pain (Landmark et al., 2013; Neville et al., 2008) and high education to better overall health (Eide and Showalter, 2011). One explanation for such a protective role of education might rely in better health literacy among individuals with a higher education (van der Heide et al., 2013), leading to healthier behaviors that can protect against developing chronic pain or reduce its frequency (Kim et al., 2022; Mackey et al., 2019).
While higher income or better job class might also be associated with better health and lower chronic pain prevalences for similar reasons (Lazar and Davenport, 2018; Prego-Domínguez et al., 2021; Stormacq et al., 2019), and likely due to better access to higher quality medical care (e.g. shorter waiting time, access to preventive health care programs; McMaughan et al., 2020; Stormacq et al., 2019), our findings revealed a more nuanced picture. Household equivalence income was not associated with most of the outcome variables once all covariates were included (but see statistically significant associations in the model with only socio-demographic factors in Supplemental Tables S2–S5), except for a negative association with back pain-related burden. This isolated effect suggests that economic resources may help buffer the functional or psychological consequences of back pain, even when overall pain prevalence remains unaffected. The absence of more consistent associations between income and chronic pain in our sample might be explained by the inclusion of covariates and by country-specific health care systems, such as Germany’s mandatory health insurance, which ensures comprehensive coverage for all residents. In contrast, job class emerged as a significant factor associated with chronic back pain, with individuals in very disadvantaged job classes being 40% more likely to report any level of back pain versus “no pain” compared to those in very advantaged job classes. Burden associated with back pain was also higher for individuals in very disadvantaged job classes. Two other European studies using the EGP scheme found similar results (higher prevalence of musculoskeletal pain symptoms in lower occupational classes; Mehlum et al., 2008; Toivanen, 2011). While job class is correlated with income, it additionally captures occupation types, including the type of work done, and it relates to social stratification. Very disadvantaged job classes comprise, for example, manual labor occupations, which might explain the higher odds of back pain and more severe back pain symptoms (Herrero Babiloni et al., 2020). Future research should further investigate the role of the physics of work behavior, such as physical strain, sedentary behaviors, or screen time, as potential predictors of chronic pain. In line with previous studies on the relationship between shiftwork and health problems (Teófila Vicente-Herrero et al., 2019; Vogel et al., 2012), we found shift workers to have about 26% higher odds of reporting any and more severe levels of back pain or headache compared to non-shift workers.
The analysis of the psychosocial variables that have been previously directly or indirectly linked to pain (Bernier Carney et al., 2021; Porst et al., 2020; Whibley et al., 2019) revealed that sleep problems and burnout were systematically associated with increased odds of reporting any and partially more severe levels of back pain and headaches, as well as higher associated burden. Our results suggest that these associations were overall stronger than other factors. For instance, individuals with the highest sleep problem and burnout scores had 11-times and 5-times greater odds, respectively, of reporting any level of back pain compared to those with the lowest scores. Similar strong associations were found for chronic headache. While the effect of sleep problems was similar across symptom severity (proportional odds assumption not violated), the ORs for burnout tended to be higher with increasing symptom severity (especially for headaches). Associated burden was also elevated among individuals with more sleep problems and higher burnout levels. Studies show that sleep problems and stress can increase pain sensitivity, exacerbate existing pain conditions, and drive the emergence of chronic pain (Abdallah and Geha, 2017; Andersen et al., 2018; Vachon-Presseau, 2018). For instance, sleep disturbances have been identified as potential headache triggers, especially for chronic conditions like migraines (Sullivan and Martin, 2017, 2020). Sleep quality is also proposed as a mediator between stress and pain (Vieira et al., 2023). Our findings support the link between sleep, stress, and pain and highlight their crucial role in chronic pain. However, chronic pain has also been found to influence sleep and stress, suggesting a complex, likely bidirectional relationship (Alsaadi et al., 2014; Koffel et al., 2016; Mák et al., 2021).
Our findings also indicate that respondents with a lifetime mental illness diagnosis were more likely to experience any and more severe levels of headache symptoms and they also reported more associated burden for both back pain and headaches. This is in line with previous studies showing how depression, anxiety, and substance abuse are common comorbidities in patients with chronic pain (Hooten, 2016). While sleep problems, burnout, and psychological disorders are risk factors for developing chronic pain, social support and optimism are often considered protective factors for physical and psychological health (Mulkana and Hailey, 2001; Rasmussen et al., 2009). For instance, studies have shown that individuals with chronic headaches report less social support (Porst et al., 2020; Westergaard et al., 2021), while higher levels of social support have been linked to less pain and decreased disability (Jensen et al., 2011). A similar pattern emerged in our study, where greater social support was linked to a lower burden related to back pain. Notably, social support can also have the opposite effect and contribute to the pain symptoms becoming chronic (Nees et al., 2022; Weiß et al., 2024). Operant conditioning principles suggest that pain behavior and associated symptoms are more likely to recur and become chronic if social support systems (e.g. family and friends) display sympathy and commiseration for the person who is experiencing pain (Fordyce, 1976; Fordyce et al., 1973). In line with this theory, we found that higher social support was associated with increased odds of reporting any level of chronic back pain and headaches. The effect of social support varied depending on the severity of symptoms and tended to be smaller with greater symptom severity.
Regarding optimism, studies have investigated its protective role for chronic pain. While optimism appears to have beneficial effects on pain symptoms (Basten-Günther et al., 2019; Shanahan et al., 2021), these effects are often small and sometimes statistically non-significant (Martinez-Calderon et al., 2018). In our study, optimism was not statistically significantly associated with the experience of pain itself, but it showed statistically significant negative associations with the burden related to back pain and headache symptomatology. These associations may reflect the role of optimism in shaping cognitive appraisal, stress regulation, and coping responses. Such effects likely operate through psychosocial mechanisms rather than through direct reductions in pain severity.
Limitations and directions for future research
While this study aimed to recruit a representative sample of the German population, some groups are slightly underrepresented (i.e. the 18–30 age group) and others are slightly overrepresented (i.e. respondents with higher formal education). This limits the interpretation of the results. Moreover, we cannot rule out the possibility that underlying pain symptoms might have influenced survey participation (e.g. not participating due to headache). We focused our analyses on a nationwide sample of the working population in Germany; future studies may elect to target the general population or subsamples thereof. For example, given the rapidly increasing aging world population, more studies on older, retired individuals are needed. Moreover, we only investigated back pain and headaches; we acknowledge that nationwide and labor market-related investigations of the prevalence, severity, and associated factors of other types of chronic pain, such as fibromyalgia (Pinto et al., 2023) or neuropathic pain (Cruccu et al., 2017), deserve further attention. Another limitation of this study is the cross-sectional nature of the data, which does not allow us to infer causality from the associations found. Thus, we encourage prospective and longitudinal studies to better identify causal explanations for the emergence of chronic pain symptoms. Finally, cross-national studies could give interesting insights into whether protective and risk factors are similar across different countries and whether biological or socio-cultural factors explain the emergence of chronic pain.
Conclusions
In this study of the working population in Germany, chronic back pain and headaches were highly prevalent. The majority of the respondents experienced only mild symptoms. The high prevalences are worrisome and should be carefully considered by health policymakers. Several demographic and psychosocial factors were significantly associated with symptom severity, and/or associated burden of chronic pain. However, several variables, such as education, household income, job class, shiftwork, optimism, and social support, were statistically significantly associated only with specific pain indicators. In contrast, gender, sleep problems, and burnout symptoms emerged as the strongest correlates, consistently associated with all pain indicators. Age was also statistically significantly associated with the severity of both chronic back and headache symptoms, but not with the associated burden (with exceptions for certain age categories). These findings underscore the need for future prospective or interventional studies to further explore sleep and burnout as potential targets for preventing and mitigating chronic pain, as both are potentially modifiable. A more nuanced understanding of the factors that drive or alleviate chronic pain could guide the development of targeted preventive health programs, ultimately reducing the prevalence of chronic pain and its associated health and societal burdens.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261437575 – Supplemental material for Chronic back pain and headaches in a nationwide study of the working population in Germany: Prevalence, symptom severity, associated burden, and related demographic and psychosocial factors
Supplemental material, sj-docx-1-hpq-10.1177_13591053261437575 for Chronic back pain and headaches in a nationwide study of the working population in Germany: Prevalence, symptom severity, associated burden, and related demographic and psychosocial factors by Sebastian Sattler, Nadine Baumann and Giulia Zerbini in Journal of Health Psychology
Footnotes
Acknowledgements
We thank those who helped conduct this study, especially Floris van Veen, Fabian Hasselhorn, Dana Pietralla, Saskia Huber, the forsa-team, and Alexander Neuhaus and Nina Hänel for supporting the analysis, as well as Kelsey Hernandez for language editing.
Ethical considerations
Ethics approval was received from the Ethics Committee of the University of Erfurt (reference number: EV-20220830).
Consent to participate
Informed consent was obtained from all study participants.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
Conceptualization: S.S. and G.Z. Methodology: S.S. and G.Z. Investigation: S.S. and G.Z. Data curation: S.S. Formal analysis: S.S. Validation: S.S., G.Z. and N.B. Visualization: S.S. Writing—original draft: S.S and G.Z. Writing—review and editing: S.S., G.Z. and N.B. All authors reviewed and approved the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Research Foundation (grant numbers: SA 2992/2-1, SA 2992/2-2 to Sebastian Sattler; ME 2082/8-1 and ME 2082/8-2 to Guido Mehlkop).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are openly available in the publication repository (PUB) of Bielefeld University (Sattler et al., 2026).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.