
Abstract
Aims: The study objectives were to provide a quantitative description of work participation among young adults, and to outline the relations between work participation and social, educational and health-related characteristics throughout the life-course. Methods: We collected data in several national registries for all 318,705 individuals born in Norway 1967–1971 who were national residents on 1 January 1993. The criterion for work was annual occupational income above the boundary which identifies the core workforce. We analysed associations between social, educational and health-related characteristics, and the number of years at work and the risk of never working during 19 years of follow-up (1993–2011; age 22–44 years). Results: The overall work participation was high, with a median of 14 years and a 0.074 risk of never working. Women worked fewer years than men (medians 11 v. 16 years) and had higher risk of never working (0.103 v. 0.047). Combined educational and health problems before 1993 had a strong influence on subsequent work participation. The educational gradient in risks of never working was considerably stronger for women than for men. Diagnostic groups of mental disorders had high risks of never working, ranging from affective (risk 0.150) and stress-related disorders (risk 0.163) to intellectual disability (risk 0.933).
Keywords
Background
Complete participation in working life has been considered to be imperative not only for the sustainability of the welfare state, but also for the prosperity and social fulfilment of the individual [1].
Birth cohorts provide knowledge relating to causes and consequences of marginal work participation. Social, educational and health-related characteristics during the entire life course were closely connected to work participation at ages 47–48 in a Swedish cohort [2]. Similar results were reported in the British National Child Development Study (NCDS), where reduced participation in working life at age 50 was strongly associated with childhood mental-health problems [3]. Work participation at age 30 has also been studied in two birth cohorts using Norwegian register data, showing that social and health-related characteristics in early life may have long-term consequences for employment [4, 5].
More recent observational studies have had a focus on young adults who are not engaged in education, employment or training (NEET) [6]. NEET status is characterized by social problems that can be traced back to childhood [6, 7] as well as negative consequences for later education and work [8]. Self-reported physical and mental-health problems were distinctly more common among NEET youths in OECD countries [6, 9]. A longitudinal Australian study found that depression was not an important predictor or consequence of NEET status [10]. By contrast, a longitudinal study among Dutch youths showed that consistent mental-health problems at ages 11–19 predicted NEET status [11]. These contradicting findings highlight that more research is needed to understand the relationship between mental health and engagement in work, education, or training in young adults. NEET prevalence was lower in Norway than in OECD (9% compared to 14% in 2016) [9]. However, NEET youths in Norway were more selective, with a larger fraction of disability pensioners and lowly educated individuals [9].
Increasing labour force participation has been high on the Norwegian political agenda in recent years. This is illustrated by a co-operation where the Norwegian Government and organisations representing employers and employees have since 2001 co-operated on an Agreement of Intent Regarding a More Inclusive Working Life (the IA Agreement). This is revised for the period 2019–2022. One of the three main objectives of the original IA Agreement was to include more individuals with reduced functional ability, particularly disabled youths, in working life [12]. Results so far indicate that this has been difficult to achieve [12]. The specific objective to increase inclusion of vulnerable groups has been removed from the new agreement, though the general aim is still to organise working life in a manner that secures maximum work participation through preventing and reducing sickness absence and early retirement [13].
Study aim
Our aim was to carry out a descriptive study on factors that affect work participation by using a registry-based birth cohort, which covers more extensive time and age periods than similar research we have earlier conducted [5, 14–19]. We studied work participation over 19 years (1993–2011) in a cohort of all who were born in Norway 1967–1971 and who were aged between 22 and 44 years during follow-up. We had two objectives:
to quantitatively examine associations between earlier social, educational and health-related characteristics (before 1993), and work participation during follow-up; and
to quantitatively examine relations between social, educational, and health-related characteristics, and work participation during follow-up 1993–2011.
Methods
Study population and data sources
The study was based upon all 331,884 live-born individuals in Norway who were registered in the Medical Birth Registry of Norway (MBRN), 1967–1971. We excluded 4984 who emigrated and 8195 who died before 1993. Thus, the study population constituted 318,705 residents as of 1 January 1993. The project was approved by the regional ethical committee (REC South East A, reference number S-06028a).
Data for all individuals were collected from several national registries: the National Registry [20]; the event database FD-Trygd [21]; the National Education Database [22]; medical benefit registries in the Norwegian Labour and Welfare Administration; and three central health registries [23] – Registry of the Norwegian Armed Forces Medical Services, Norwegian Patient Registry (NPR) and MBRN. Register data were individually linked by means of the unique national identity number and de-identified by Statistics Norway before delivery.
Work participation
Work participation between 1993 and 2011 was the study outcome; thus, participant ages during follow-up were 26–44 years for the 1967 cohort and 22–40 years for the 1971 cohort. Labour market attachment was determined using annual employment income (earned income plus net income from self-employment minus unemployment benefit) [21], which was measured as Consumer Price Index-harmonised G units, determined annually by the Government. One G unit was equal to NOK 37,300 in 1993 and NOK 79,216 in 2011. We used an annual income of at least 3.5 G units as the criterion for work participation as this limit identifies the core workforce [7]. Two outcome measures were applied: ‘Years at work’ 1993–2011 (range 0–19), and ‘Never working’ during follow-up (dichotomous). Participants were followed up from 1 January 1993, until death, emigration, or end of follow-up (31 December 2011).
Social, educational and health-related variables before 1993 and during follow-up (1993–2011)
Definitions and categorisations of background and follow-up study variables are provided in Table I and Table II, respectively. In addition to sex, year of birth and characteristics according to place of residence, variables were by nature social, educational or health-related.
Distribution of selected background variables (before 1993) and their relation to work participation during 19 years of follow-up.
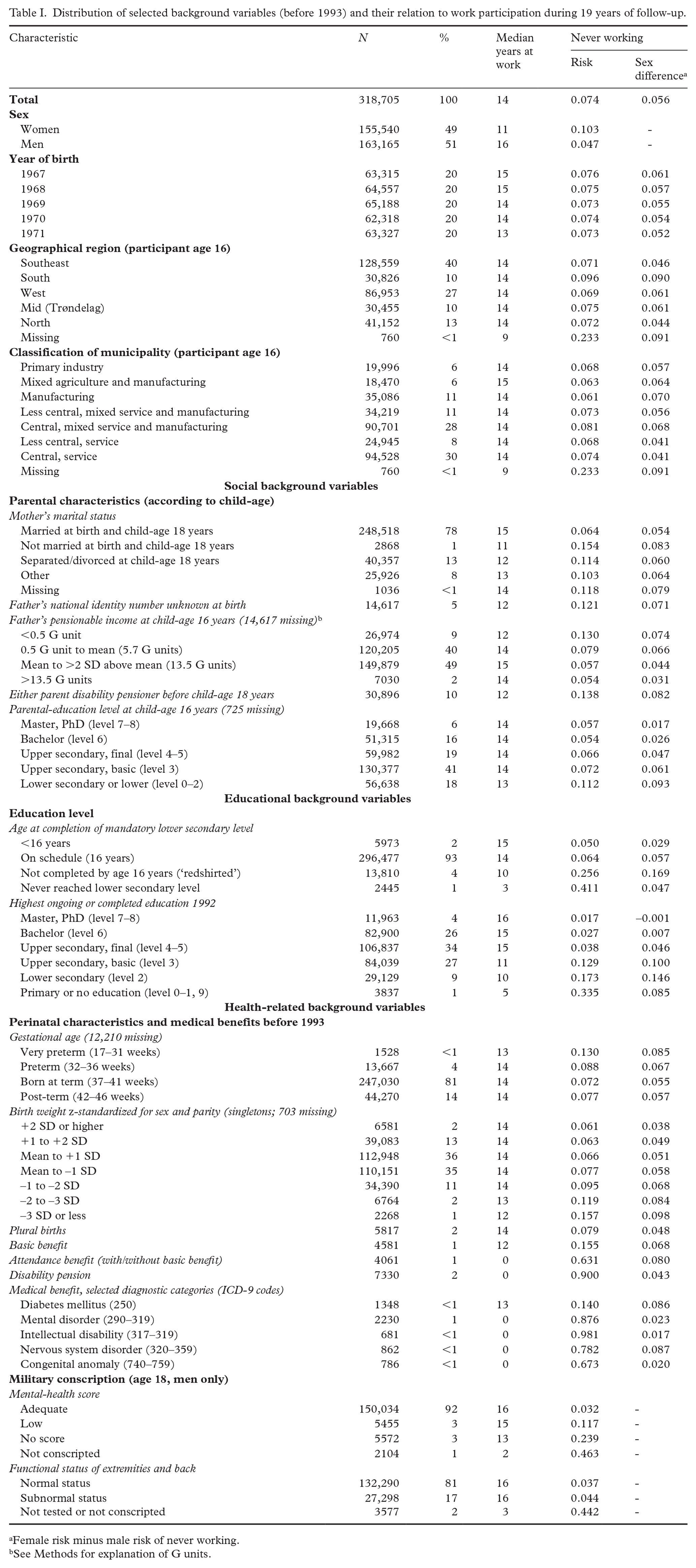
Female risk minus male risk of never working.
See Methods for explanation of G units.
Distribution of selected follow-up variables (1993–2011) and their relation to work participation during 19 years of follow-up.
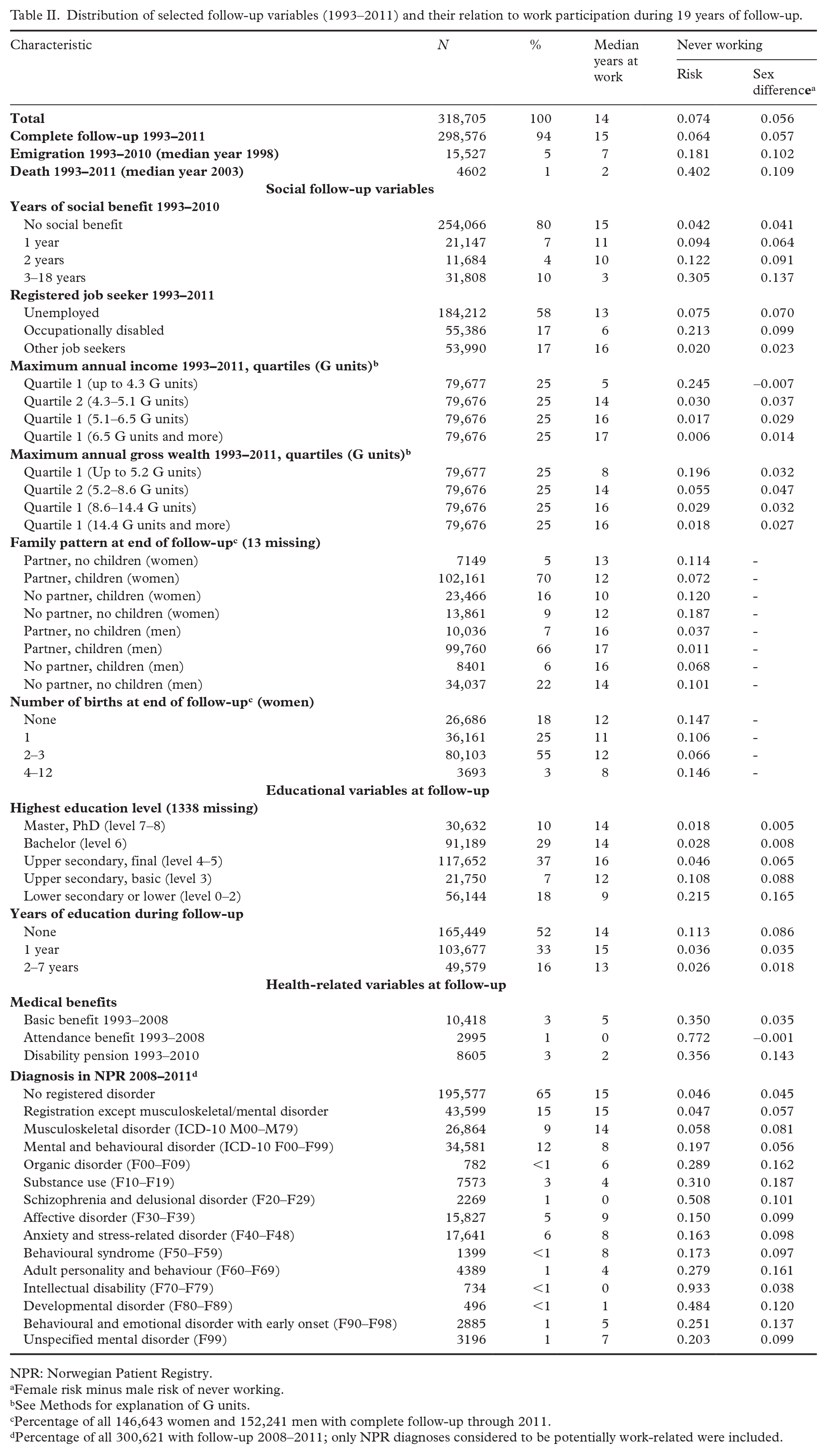
NPR: Norwegian Patient Registry.
Female risk minus male risk of never working.
See Methods for explanation of G units.
Percentage of all 146,643 women and 152,241 men with complete follow-up through 2011.
Percentage of all 300,621 with follow-up 2008–2011; only NPR diagnoses considered to be potentially work-related were included.
Background variables (Table I)
Background variables included: geographical region (five categories); municipality type according to industry and centrality (seven categories) [24]; mother’s marital status (four categories); father’s national identity number unknown at birth (dichotomous); father’s pensionable income (four categories); either parent disability pensioner (dichotomous); parental-education level (five categories); participant age at completion of lower secondary education (three categories); highest ongoing or completed education level 1992 (six levels); gestational age (four categories); birth weight z-standardised for sex and parity (seven categories); plural birth (dichotomous); medical benefits before 1993 (basic benefit, attendance benefit, disability pension, all dichotomous); selected diagnostic categories that qualify for medical benefits (diabetes mellitus, mental disorder, intellectual disability, nervous system disorder, congenital anomaly); dichotomous mental-health score, and functional status of extremities and back at military conscription (men only).
We constructed an integrated variable of early social, educational and health problems based upon earlier studies of early life conditions and work participation [2–5], termed ‘Background problems’. Social problems included two or more of the indicators: parental-education level lower secondary or less, parental disability pension, mother unmarried, father’s income <0.5 G unit, or father’s identity unknown. Educational problems included at least one of the indicators: education level in 1992 lower secondary or lower, or age at completion of lower secondary >16 years (‘redshirted’). Health problems included at least one of the indicators: medical benefits before 1993, birth weight ⩾2 SD below the mean, or preterm birth (gestational age <37 weeks). Background problems had eight (23) categories, where each of the three dichotomous social, educational and health elements were included either as absent (no problem) or present (problem). In a secular trend analysis, we dichotomized the background problem variable (no problem, problem(s)).
Follow-up variables (Table II)
Follow-up variables included: years of social benefit (four categories), registered job seeker (three categories), maximum annual income (quartiles), maximum annual gross wealth (quartiles), sex-specific family pattern at end of follow-up (four categories each), number of births at end of follow-up (four categories, women only), highest education level (five categories), years of education during follow-up (three categories), medical benefits during follow-up (as above; all dichotomous), and NPR diagnoses (four categories plus 11 subcategories of ICD-10 Mental and behavioural disorders, Block F00–F99).
Analysis
Analyses were carried out in Stata SE v14.2 software (Stata Corp, TX, USA). We computed number of years at work according to categories of background and follow-up variables. In order to provide central location as well as distributional variability, we presented seven percentiles (5, 10, 25, median, 75, 90, 95) in boxplots. We had a particular interest in both the left tail of the distribution and sex differences, and thus computed the risk (probability) of never working as well as the association between sex and never working as the additive risk difference (female risk minus male risk) for background and follow-up variables. We computed secular unemployment trends across strata of sex and dichotomous background problems in order to assess the trend of relations between background problems and unemployment during follow-up.
Welfare problems including poverty, low education, health problems and unemployment tend to be clustered [25]. We assessed clustering by computing additive differences in risks of never working according to categories of background problems. This analysis was performed by estimating additive risk differences and corresponding standard errors using binomial regression, and clustering was determined by computing departure from additivity as outlined by Altman and Bland [26].
Results
Population characteristics, as well as stratum-specific median years of work and risk of never working according to the explanatory variables are provided in Table I and Table II.
The 318,705 participants had a total follow-up of 5,832,164 person years (mean 18.3 years), of which 3,871,948 (66%) were years at work. Median years at work in the total population was 14 years; 23,707 (risk 0.074) never worked. Women participated less at work than men: median years at work were 11 and 16 years, respectively; the risk of never working was 0.103 and 0.047, respectively; and cumulative years at work constituted 55 and 77% of all years of follow-up, respectively.
Work participation according to background variables (before 1993)
Number of years at work according to background problems is depicted in Figure 1. The majority (74%) had no background problems; quartiles at work were 10, 15 and 18 years. The groups with social, educational, or health background problems alone had fewer years at work (medians 11–13 years). Those with combined background problems (5% of population) had 0–8 median years.
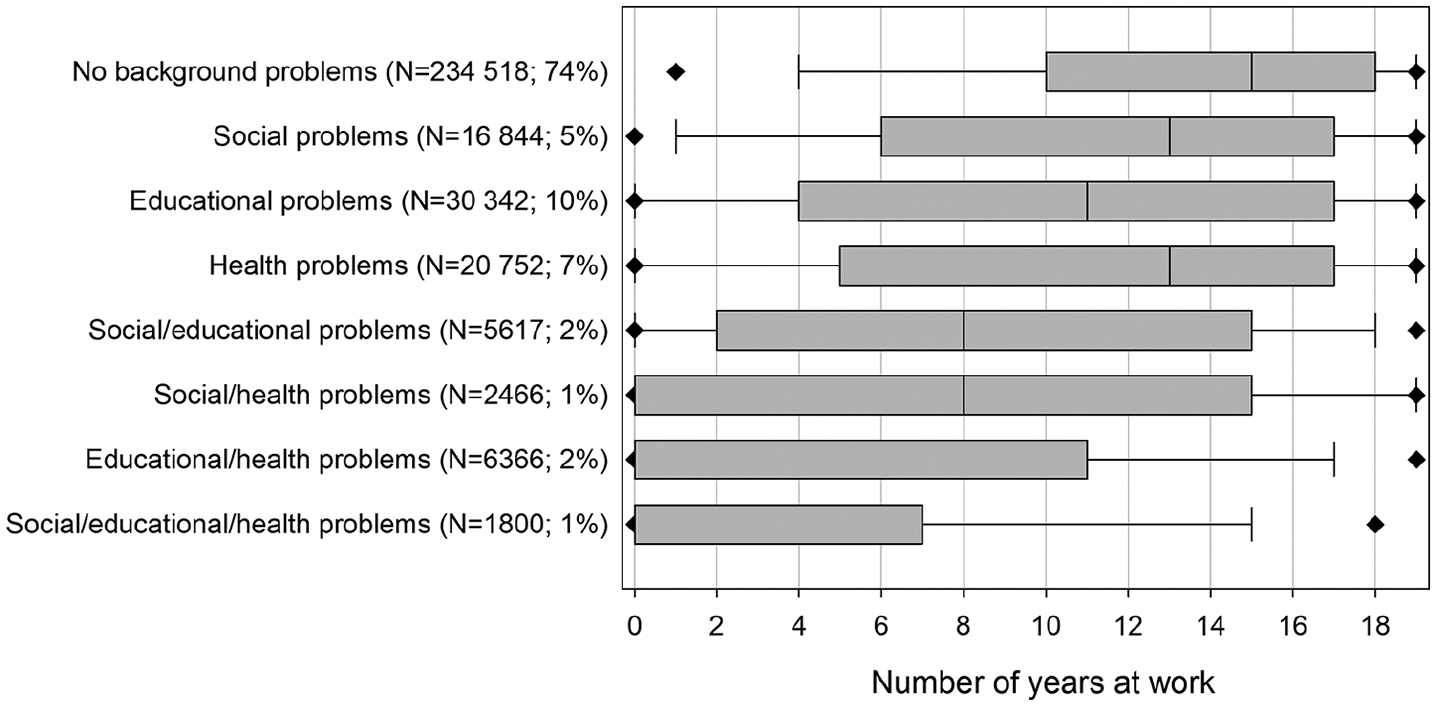
Number of years at work according to background problems.
Table III shows the pattern for risk of never working according to background problems with risks ranging from a low 0.040 for the ‘no background problem’ category to above 0.5 for the two categories including both health and educational problems. All problem combinations showed risk departures from additivity, and distinctively strongest for educational/health problems (departure 0.292) and social/educational/health problems (departure 0.329).
Crude additive associations for never working according to social, educational and health-related background problems.
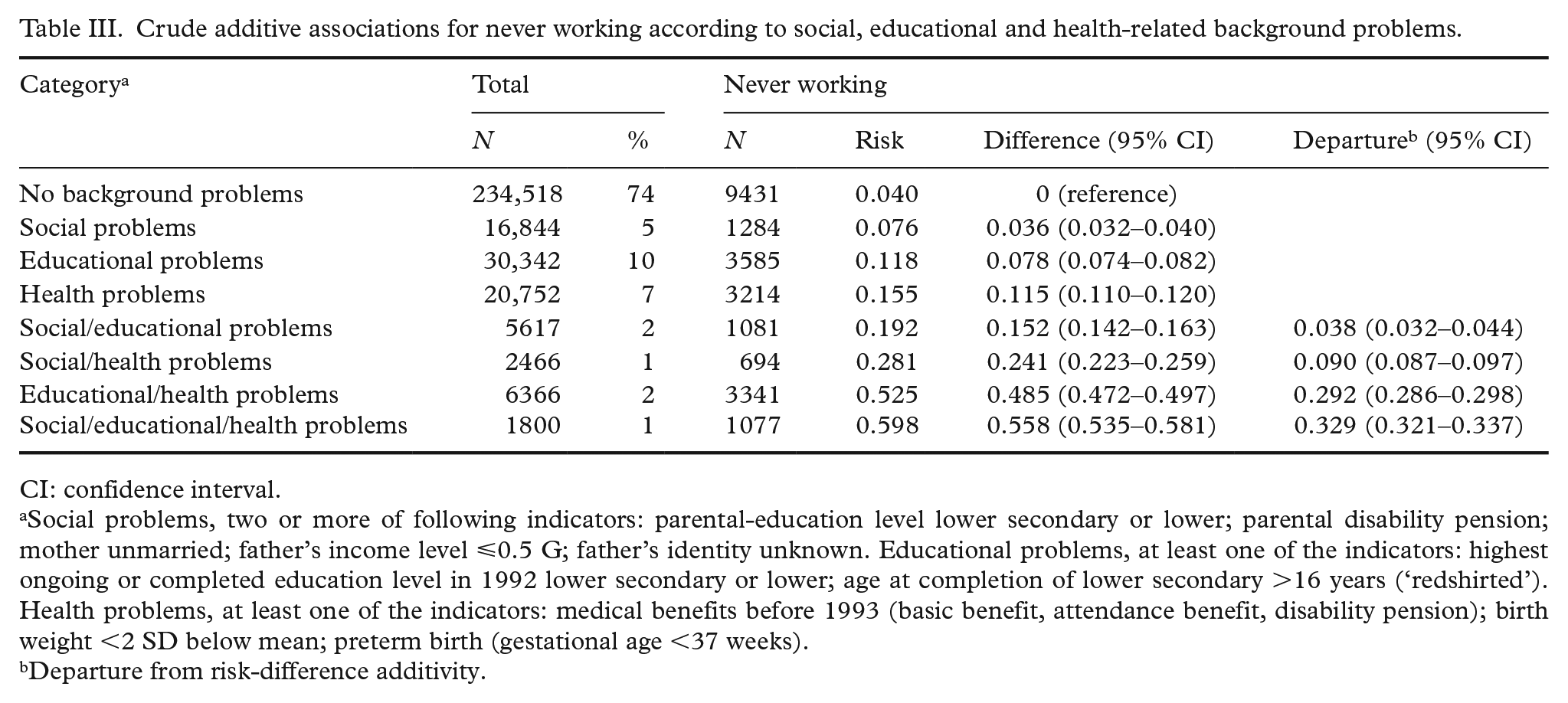
CI: confidence interval.
Social problems, two or more of following indicators: parental-education level lower secondary or lower; parental disability pension; mother unmarried; father’s income level ⩽0.5 G; father’s identity unknown. Educational problems, at least one of the indicators: highest ongoing or completed education level in 1992 lower secondary or lower; age at completion of lower secondary >16 years (‘redshirted’). Health problems, at least one of the indicators: medical benefits before 1993 (basic benefit, attendance benefit, disability pension); birth weight <2 SD below mean; preterm birth (gestational age <37 weeks).
Departure from risk-difference additivity.
Table I shows more detailed work participation results for the specific background factors. Work participation was moderately affected by unfavourable social conditions whereas problems affecting own education before 1993 had larger negative impact. This was particularly the case for those who had not completed lower secondary education by age 16 (‘redshirted’) and those in the three lowest education levels in 1992. Very preterm birth and birth weight ⩾2 SD below mean were associated with moderately increased risks of never working. The majority of medical benefit recipients (except basic benefit) and diagnostic groups (except diabetes) never worked. Men with low mental-health score at military conscription had a nearly fourfold higher risk of never working (0.117) compared to those with adequate score (0.032).
Work participation according to follow-up variables (1993–2011)
Emigration and death during follow-up constituted 5 and 1% of the total population, respectively. The risk of never working was more than seven-fold higher among those with social benefit ⩾3 years (0.305) compared to the ones without social benefit (0.042), and nine-fold higher for men without a partner or children (0.101) as compared to men with both a partner and children (0.011). For women, the lowest risk of never working was found for 2–3 childbirths during follow-up (Table II).
Education level had a strong influence on work participation. Figure 2(a) depicts different patterns for women and men. Women showed strong and consistent reductions in work participation for each decrement in level of education. Men in the final upper secondary level had optimum work participation, and the differences in lower education levels were more moderate than in corresponding female categories. The lower work participation in the two highest education levels for men could be due to a high prevalence (80%) of education during follow-up in these categories compared to lower education levels (40%).
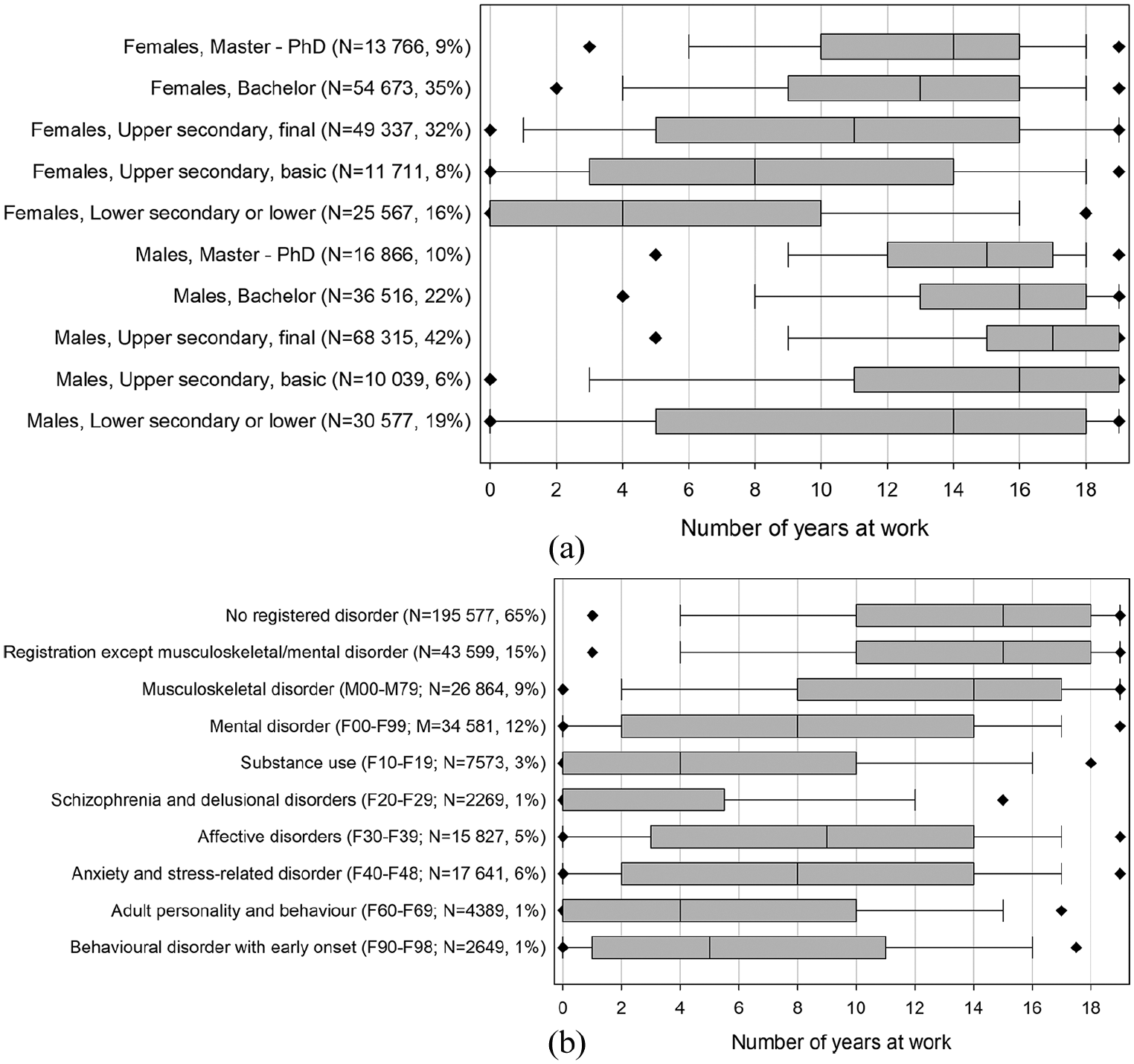
Number of years at work according to selected follow-up factors: Sex-specific education level.
Figure 2(b) and Table II show that mental disorders in NPR 2008–2011 were associated with fewer years at work and several-fold higher risks of never working compared to individuals with musculoskeletal or other NPR registrations. Diagnostic subgroup risks of never working ranged from 0.150 to 0.163 for affective (F30–F39) and anxiety and stress-related (F40–F48) disorders; 0.508 for schizophrenia and delusional disorders (F20–F29); and 0.933 for intellectual disability (F70–F79). Similar patterns were present for distributions of years at work (Figure 2(b)).
Secular unemployment trends seemed to follow the business cycle for both sexes. The groups with and without background problems followed the same unemployment trends during follow-up (Figure 3).
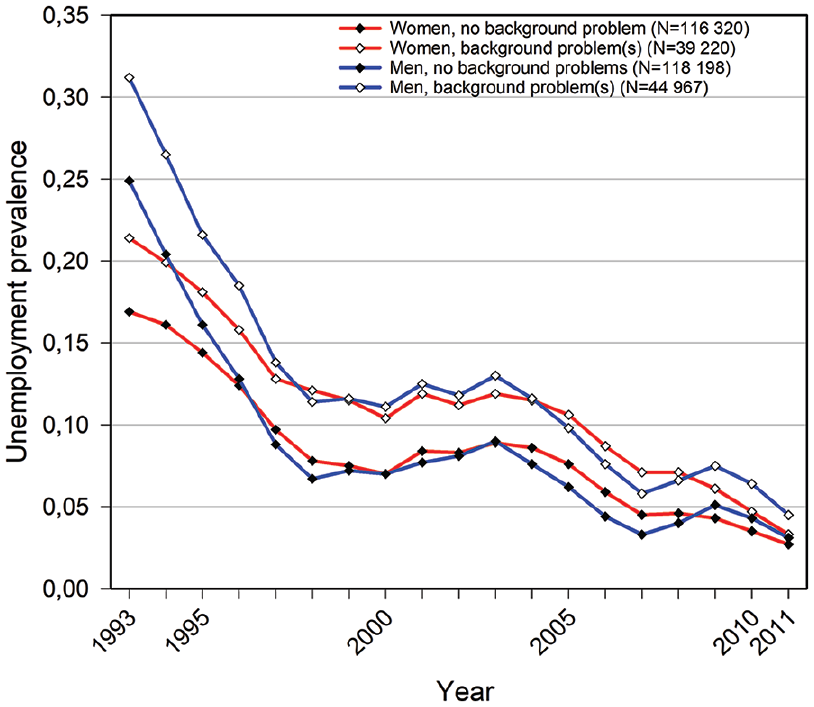
Annual unemployment prevalence 1993–2011 according to sex and background problems before 1993.
Additive sex differences in risk of never working across strata of background and follow-up variables are provided in the right-hand column of Table I and Table II. Parental and all other indicators of education show strong risk difference gradients from approximately equal risks for master level to female risks more than 0.1 higher than male risks in the lowest education levels. For most other variables, sex differences in risks of never working tended to be unevenly distributed and particularly higher for categories indicating problems of social or health-related nature compared to no-problem categories. Geographical region and type of municipality had little overall influence on work participation, but sex differences in risk were moderately higher in South Norway and manufacturing municipalities.
Discussion
In this registry-based cohort study, we have described how work participation between the ages of 22 and 44 was associated with individual conditions throughout the life course, providing a quantification of number of years at work and the risk of never working during follow-up. Work participation during 19 years of follow-up was high, and clearly higher among men than women. Problems relating to social background, education and health in childhood and adolescence, and particularly clustering of educational and health-related problems, were associated with low work participation. The same applied to low education and mental disorders during follow-up. The sex differences in risks of never working were highly dependent on parental and own education levels and demonstrated a socioeconomic gradient that was steeper and more consistent for women than for men.
The work attendance patterns in the present study are largely in agreement with findings in other life-course studies [2, 3], in earlier results from studies using this cohort [5] and in NEET studies [6–11]. Childhood mental-health problems had more severe consequences for subsequent work than somatic health problems in the British NCDS cohort [3], and a recent Danish study shows associations between self-reported somatic health in adolescence and work participation in young adult age [27]. Mental disorders have repeatedly been linked with unemployment [28–30]. Table I illustrates that both mental and somatic childhood disorders had adverse consequences for later work in our study. The conscript and NPR results suggest that mental disorders in young adult age are more strongly associated with low work participation than musculoskeletal and other somatic disorders. The sex-specific educational inequalities (Figure 2(a)) show that the female underrepresentation in work participation mainly affects lower education levels. This pattern is in agreement with Dutch working life expectancy data (Supplemental material S2) [31].
We aimed at describing individual characteristics in the study population and have therefore not conducted causally oriented analyses. It is plausible that background variables are in some way on the causal pathway towards workforce entry. We can also assume that the strong association between low education level and low work participation is to some degree due to poor opportunity to enter or stay in the workforce. However, analyses of such pathways are beyond the scope of this study. Prior studies suggest that strong associations between work participation and mental disorders are explained by more complex causal pathways [30]. We can assume that mental disorders that are likely to appear in youth (e.g. ICD-10 codes F60–F98) could have detrimental effects on a later work career. The more common affective and stress-related disorders (ICD-10 F30–F48) could, however, be caused by unemployment and work-related factors. Thus, the strong associations between work participation and mental disorder could therefore partly be explained by health selection and partly by social causation.
The strengths of this registry-based study are that it is population-based with complete coverage and nearly complete follow-up over the life course. Study variables were collected in a prospective and independent manner. Nevertheless, there are some potential validity problems.
Registry-based studies are dependent on available data that are often collected for administrative and not research purposes. Data are usually less tailored, for example, compared to the British NCDS cohort [3]. Not all follow-up variables covered the entire study period (see Table II). We did not have access to certain variables included in other birth cohorts [2, 3], such as personality traits, achievements at school, social relations outside the family and law offences. The study scarcely covered contextual and macro-level conditions and did not take potential confounding into consideration. There is also a possibility that the results are hampered by ill choices of variable contents and analyses. They are also likely to be influenced by our definition of work participation. Those not officially registered with an annual income of at least 3.5 G are a heterogeneous group: people earning less than 3.5 G, unpaid voluntary or domestic work, undeclared work and moonlighting, and illicit work and criminal activity.
In the majority of analyses, we did not take into account loss of working years due to lack of opportunity or possibility to work. This is evident for the 6% who emigrated or died during follow-up. Comparison between the total study population and those with complete follow-up (Table II) indicates that this had only restricted impact. The results are nevertheless not suited to assess relations between emigration or mortality and work. Nor did we take into account reduction in work participation due to childbirth, infant care and education during follow-up. If we assume that one birth (women only) and one year of education during follow-up each results in a one-year absence from work, these activities would have only moderate impact, occupying approximately 12 and 4% of total follow-up time for women and for men, respectively.
There are some limitations concerning external validity. The study was based on individuals born in Norway 1967–1971, in a period where very few immigrant mothers gave birth. Accordingly, the vast majority of participants are ethnic Norwegians. Our results may also overestimate the importance of early life health adversities due to considerable improvement in perinatal health care over the last decades. The results for women and particularly mothers might not apply in countries with less generous social benefits related to maternity.
The topic of the present study is closely related to the second main objective of the former IA Agreement: to include more individuals with reduced functional ability and particularly young disabled people in working life [12]. This objective is removed from the present IA Agreement [13], but the failure in achieving this objective in prior agreements [12] suggest that it should be prioritised. Unemployment trends in Figure 3 suggest that problems early in life have adverse consequences for work participation that last the entire follow-up period.
Even though this study is of a descriptive nature, the complexity and clustering early in life of social, educational and health problems with poor work participation suggest that preventive measures should be implemented in high-risk groups. Our results suggest that vulnerable groups are characterised by more than just health problems and should also include groups with early social and educational issues. One measure could involve prioritising improved education among young disabled people. This suggestion is in accord with recommendations from OECD for young NEETs in Norway [9] as well as from a governmental established expert panel [32].
Conclusion
Norwegians with problematic working careers in young adult life were characterised by complex social, educational and health problems early in life. Furthermore, low educational attainment and mental disorders in adult life added to these problems. The socioeconomic gradient in low work participation was stronger for women than for men. The results have public-health relevance and suggest that preventive measures should be implemented early in life. Policy implications for mental disorders and work could be more complex, including partly early-life measures and partly measures aimed at unemployment and adverse conditions at work. Disentangling these issues warrants further study using causally-oriented methods.
Footnotes
Acknowledgements
The late Professor Emeritus Tor Bjerkedal (1926–2015) had the initial idea for and took part in establishing this registry-based cohort in 2002. The present study carries on work that Bjerkedal started that never reached completion.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by grants from The Research Council of Norway (Grant Number 237831).