
Abstract
Introduction
Research has established solid evidence on the impact of socioeconomic positions on health. People in lower socioeconomic positions have a higher likelihood of having poor health and of dying younger than those in higher positions [1–3]. In view of population ageing throughout European societies, and because of the high economic burden of health care expenditures for older people, interest in determinants of health inequalities for older men and women has increased considerably and has been a major area of interest within the field of social epidemiology. Taken together, findings of previous research indicate that social inequalities in health, although diminishing, persist into late life [4–6].
Scientific debate, however, continues about the best strategies for measuring social inequalities in late life [7,8]. Alongside studies linking current income after retirement to health outcomes [9], the majority of research recognises the importance of socioeconomic conditions at earlier stages of the life course, and identifies life-course characteristics that set the pathways for later health inequalities. These studies rely predominantly on indicators measuring social inequalities prior and during working life, including education and occupational position [10,11]. A growing body of research additionally identifies characteristics of employment histories that may be linked to poor health beyond working life [12,13]. More specifically, studies investigate associations between measures of discontinuous (e.g. unemployment periods, weak labour market attachment) or disadvantaged (e.g. continuously low occupational positions) careers and later health [14].The present study aims to extend this research by exploring if precarious working conditions are linked to later depressive symptomology. More specifically, we use the lack of continuously contributing to pension schemes throughout entire working careers as an indicator for precarious employment conditions and analyse its associations with elevated depressive symptoms after exiting the labour market. One reason why the lack of pension contributions may lead to lower levels of depressive symptoms is the long-lasting uncertainty about financial protection in old age. Additionally, working without pension contributions may generally be linked to less favourable jobs with health-adverse working environments and a low quality of work. Importantly, pension contributions are assessed for entire working careers, and thus imply more than only the level of pension benefits after retirement. To sum up, our aim is to investigate associations between working without contributing to pension schemes during entire employment histories and elevated depressive symptoms thereafter, independent of retiree’s income.
Methods
Data
This study relies on data from the Survey of Health, Ageing and Retirement in Europe (SHARE 6.1.1.) [15]. SHARE is an ongoing project collecting data on a variety of sociological, economic and health-related topics. SHARE started in 2004, and consists of nationally representative samples of older adults (50+) in 11 European countries. Since then, data have been collected at 2-year intervals. In this study, we use SHARE waves 1 and 2, which we combine with retrospectively assessed life history data from wave 3. Wave 3 is commonly called SHARELIFE and includes a distinct retrospective survey collecting life history data using computer assisted personal interviews (CAPI) [16]. All three waves rely on the same sample, while subsequent waves include large refresher samples and new countries that cannot be combined with retrospective data from SHARELIFE. Among other information, SHARELIFE includes retrospective information on entire employment histories among men and women who have already left the labour market. Data is available for 14 countries (Sweden, Denmark, Ireland, Germany, the Netherlands, Belgium, France, Switzerland, Austria, Italy, Spain, Greece, Poland and the Czech Republic). At study onset, the household response rate was 61.6% for the total sample, ranging from 81% in France to 39% in Switzerland. All in all, this is above average compared with other European Surveys [17]. Recall and timing of the retrospective information on entire employment histories in SHARELIFE is supported by a graphical representation of a respondent’s life, which is filled during the interview – a method that has been shown to improve the accuracy of self-reported life history information [18,19]. More details on SHARE and SHARELIFE can be assessed online (www.share-project.org).
Sample
In total, 28,495 respondents participated in SHARELIFE. For the aim of our study, we apply the following sample restrictions. Firstly, we restrict our sample to respondents aged 60 to 85 years at the time of the retrospective interview, as this allows us to study previous employment histories between the age of 25 and 60 (n = 18,850). Secondly, we restrict the sample to retired men and women at the time of the assessment of depressive symptoms (n = 12,251). Thirdly, to reduce the risk of reverse causality when testing associations between employment history characteristics and elevated depressive symptoms, we excluded respondents with retrospectively self-reported poor mental health prior to and during working life (n = 11,934). Then, we restrict the sample to respondents who have worked at least 5 years between age 25 and 60 (n = 10,958). Finally, we restrict the sample to respondents with full available data on all variables (n = 10,248). These restrictions result in a final sample of 5969 men and 4279 women.
Measures
Depressive symptoms
For our analyses, we use data from wave 2 (2006–2007) to measure elevated depressive symptoms. When data is missing, we use respective information from wave 1 and thus rely on the most recent available information on depressive symptoms to wave 3. In SHARE, depressive symptoms are assessed by the 12-item EURO-D depression scale [20]. A scale score of 4 or higher is interpreted as elevated depressive symptoms, a cut-point that has been validated against standardised clinical interviews [21].
Pension contributions
Respondents provide detailed retrospective information on past employment histories as part of the life history interview in SHARELIFE. This includes details on the starting and ending date of each job during their working career and a detailed description of respondents’ jobs, including the employment status (employed or self-employed work) and whether they contributed to public, occupational or private pension schemes during each particular job. To measure pension contributions, we combine the information on these different pension schemes and ascertain for each year between the ages of 25 and 60 whether respondents contributed to any pension scheme or not (covering 35 years of labour market participation). We furthermore differentiate between pension contributions in self-employed and employed work. This is instrumental because there is a higher likelihood of social adversity and poor health among employed than self-employed workers [22], whereas working without pension contributions is more common among self-employed than employed workers (see below). Specifically, we ascertain a measure counting the years that respondents worked in each of the following employment situations: (a) employed work without contributing to pension schemes, (b) employed work with contributing to pension schemes, (c) self-employed work without contributing to pension schemes and (d) self-employed work with contributing to pension schemes. We categorize workers as contributing to pension schemes if they contributed to at least one pension scheme (either public, private or occupational pension schemes). Next, we specify respondents’ main employment situation by identifying the modal situation within the ages of 25 and 60.
Additional variables
Besides gender, age and country affiliation (broken into country dummies in multivariable analyses), we include information on education, partnership history and current income into the analyses. Education is measured according to the International Standard Classification of Educational Degrees (ISCED-97), regrouped into ‘low education’ (pre-primary, primary or lower secondary education), ‘medium education’ (secondary or post-secondary education) and ‘high education’ (first and second stage of tertiary education) [23]. Missing information on education is captured using an additional category for missing information. Partnership history is defined as the years living with a spouse (regardless of the marital status). We regrouped partnership history into a binary indicator of being mainly in a partnership (more than 75% of the time) or not. Current income is measured at the time of the health assessment. We use the OECD equivalence scale to account for household composition and we classify respondents’ income into high, medium and low, according to distribution-based tertiles [24].
Analytical strategy
After a sample description (Table I), we present the results of sequence analyses and report the proportions of those workers who mainly contributed to pension schemes between the age of 25 and 60 and those who have not (Table II). Pension contributions are shown separately for employed and self-employed workers and for men and women. Next, we estimate a series of Poisson regression models for binary outcomes to investigate the associations between contributing to pension schemes and elevated depressive symptoms later on. Poisson regressions enable us to estimate relative risks, which are easier to interpret than, for example, odds ratios [25].In total, we estimate three models. In model 1, we show crude estimates of an unadjusted model. Next, we show a model (model 2) adjusted for age, education and partnership history to determine if potential confounders have an effect on the associations between mainly working without pension contributions and depressive symptoms. In a final model (model 3), we additionally adjusted for current household income. In doing so, we investigate whether continuously contributing to pension schemes impacts on later health independently from later pension benefits. If confirmed, this would indicate effects of the psychosocial component of continuously contributing to pension benefits independently of current equivalent household income. For all models, we present relative risks (RR) and corresponding 95% confidence intervals (95 % C.I.).
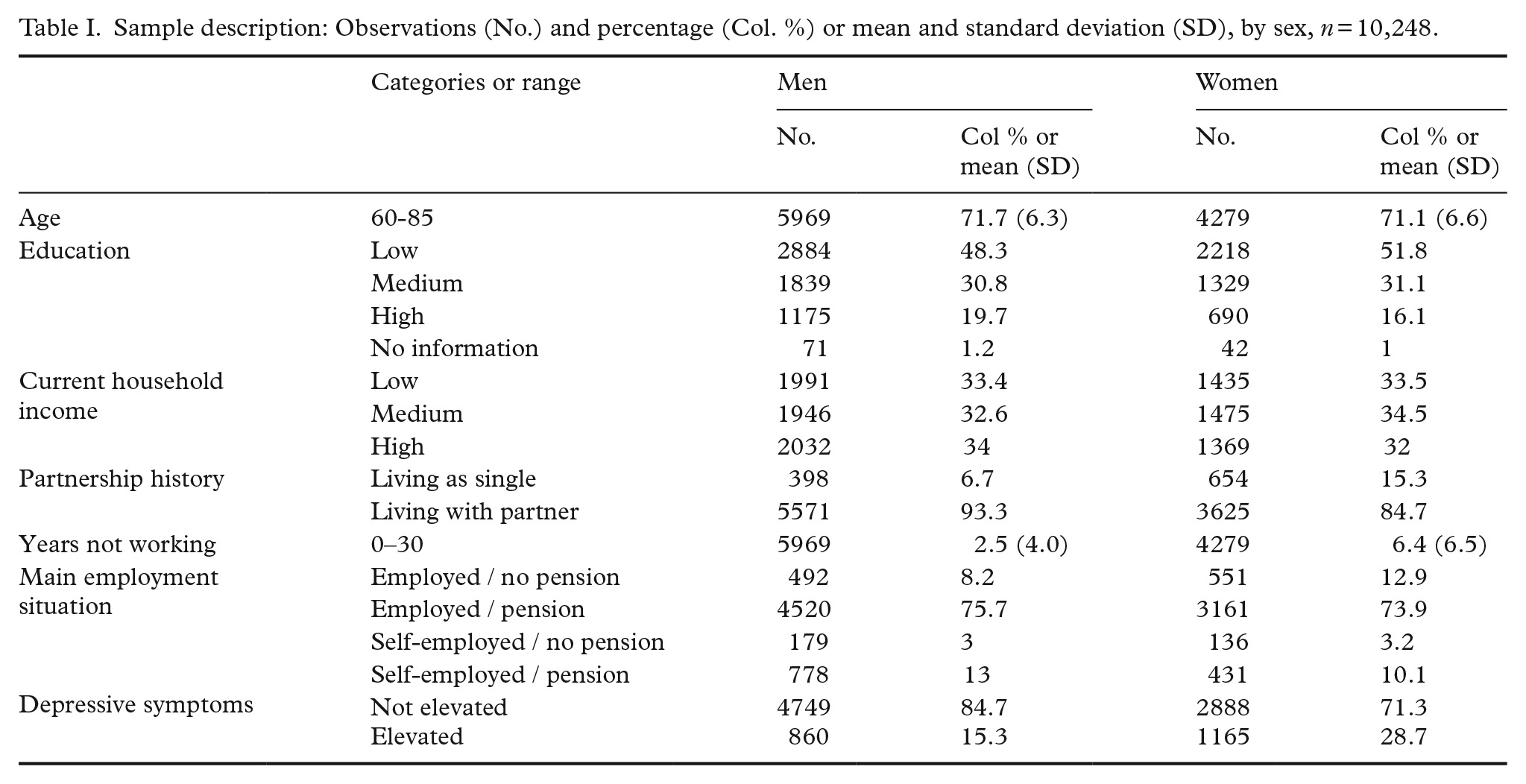
Sample description: Observations (No.) and percentage (Col. %) or mean and standard deviation (SD), by sex, n = 10,248.
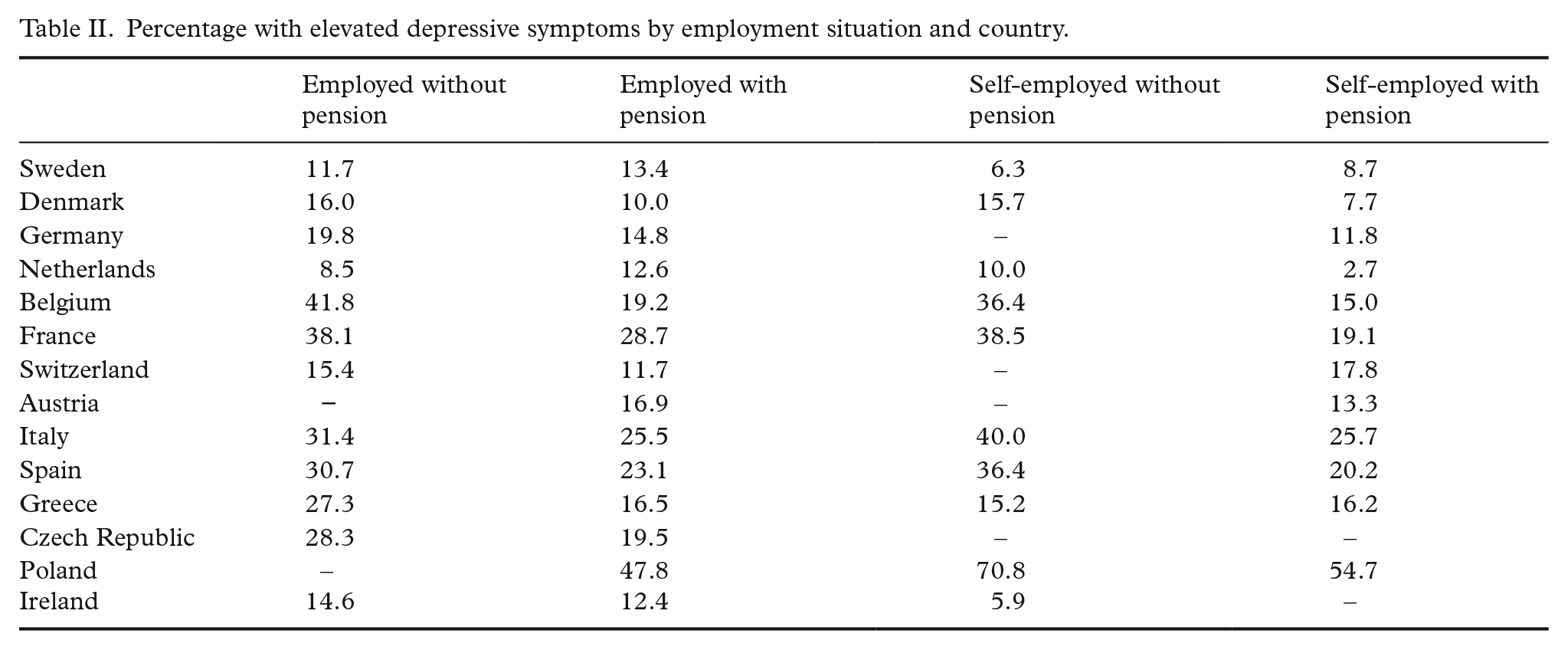
Percentage with elevated depressive symptoms by employment situation and country.
Results
Our sample consists of slightly more men (5969) than women (4279), each with a mean age of 71 years at the time of the retrospective life history interview. Most respondents contributed to pension schemes, either in employed (approximately 75% of both genders) or self-employed (13% of the men and 10% of the women) work. In all, 8% of the men and 13% of the women were mainly employed without contributing to pension schemes and 3% of both genders were self-employed without pension contributions. In total, women were more likely than men to have an employment history where they have mainly not contributed to pension schemes. Regarding the distribution of depressive symptoms, our results clearly indicate that women are more likely to report elevated depressive symptoms than men (29% vs. 15%). More details of sample characteristics are given in Table I.
In Table II, we show, for each pension scheme, the proportions of elevated depressive symptoms separately for each country. The proportions differ by country, and one can see that the prevalence of elevated depressive symptoms is higher for respondents mainly working without contributing to pension schemes than for those who mainly contributed for most countries. However, for the Netherlands and Greece, findings from Table II are mixed, and for Sweden the proportion of depressive symptoms is consistently higher for those contributing to pension schemes. Importantly, we can note that – although the distribution varies – each category of our key variable “pension contribution history” is represented in each country.
Table III presents associations between contributing to pension schemes and elevated depressive symptoms, separately for men and women. Here, four findings deserve attention. The first finding is that employed work without contributing to pension schemes is consistently associated with later depressive symptoms for women only. If adjusting for current household income (Model 3), the association remains statistically significant for women. For men on the contrary, mainly working without pension contributions is not associated with elevated depressive symptoms if considering the current income. The second finding shows that self-employed work without pension contributions is linked to an increased risk of depressive symptoms for men only, but not for women. Thirdly, estimates for self-employed men are somewhat higher than for employed women, indicating a more stable relationship between pension contributions and elevated depressive symptoms for this group. The fourth finding is that all estimates diminish at least slightly after adjusting for potential confounders (age, education, partnership history and years not working in Model 2) and for equivalent household income (as a potential mediator) in Model 3. The latter finding is important as it indicates that associations between the history of contributing to pension schemes and elevated depressive symptoms are independent from current income (with the exception of employed work without contributing to pension schemes for men).
Association between contributing to pension schemes and elevated depressive symptoms: relative risks, confidence intervals and p values.
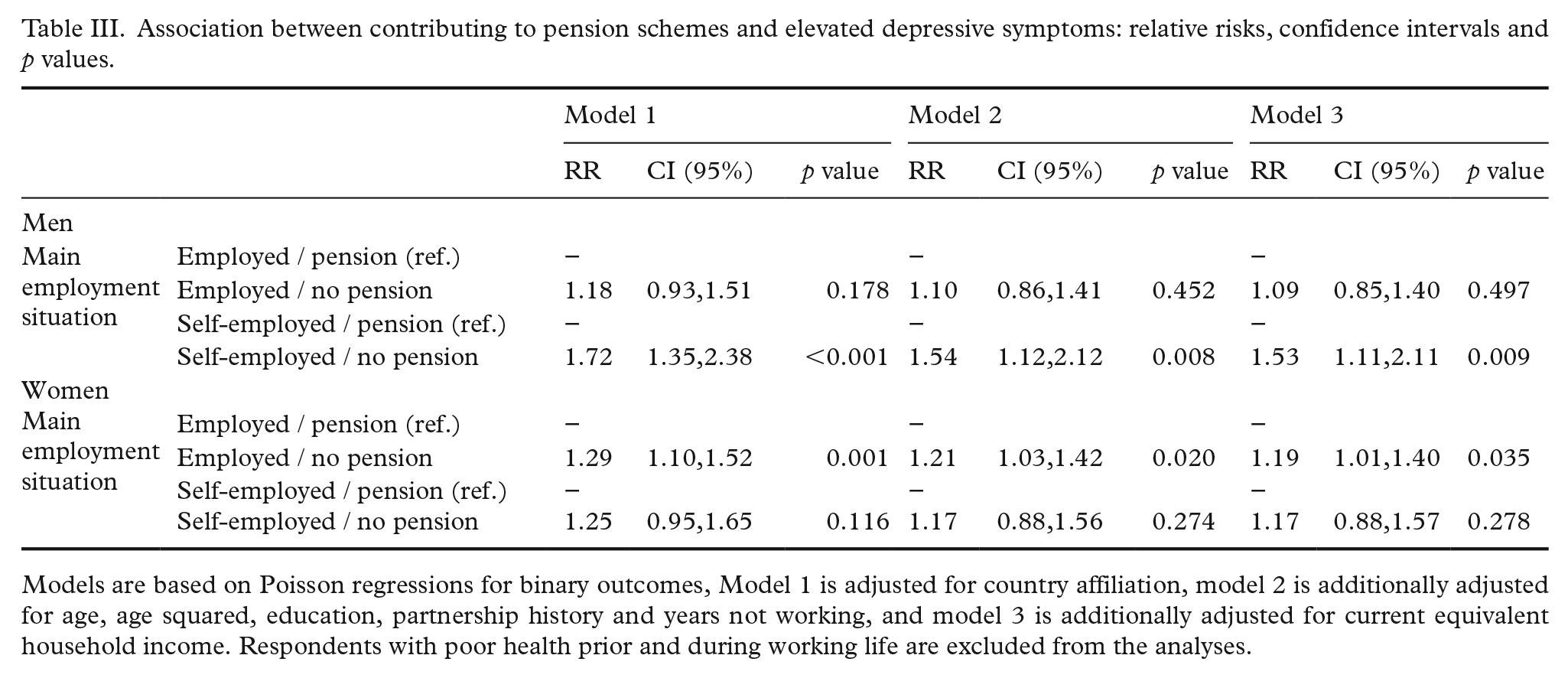
Models are based on Poisson regressions for binary outcomes, Model 1 is adjusted for country affiliation, model 2 is additionally adjusted for age, age squared, education, partnership history and years not working, and model 3 is additionally adjusted for current equivalent household income. Respondents with poor health prior and during working life are excluded from the analyses.
Discussion
The present paper relies on life history data from SHARE with detailed information on entire employment histories between the ages of 25 and 60 in Europe. These histories are linked to elevated depressive symptoms after labour market exit for 6931 men and 5735 women aged 60 or older. Our analyses indicate that working continuously without contributing to pension schemes is linked to elevated depressive symptoms for self-employed men and employed women, but not for employed men and self-employed women. Importantly, these associations are independent of the retiree’s current income. Overall, our findings are in line with previous research linking characteristics of individual employment histories with poor health later on in life [12–14]. Yet, by investigating details of labour market involvement, we add to existing research in several ways.
Our results revealed that research aiming at identifying links between previous labour market participation and health in older populations should be complemented by an investigation of individual job descriptions. Our findings indicate that it is not only important to study whether men and women have a job or not. Instead, studies need to consider details of each job of individual employment histories – including the question of whether workers continuously contribute to pension schemes or not. In fact, employed or self-employed workers who are not contributing to pension schemes are exposed to uncertainty about their financial protection in old age. Similar approaches include information on life course occupational positions, working hours or employment contracts (e.g. whether workers have permanent or temporary contracts) [26,27]. Previous studies have shown that those men and women who are strongly attached to the labour market are generally in better health than those who are not [28,29]. Here, our study points to interesting gender differences, where pension contributions matter for men in self-employed work and women in employed work. These findings support previous research on gender differences in self-employment, indicating that men are more likely than women to be in self-employed work for economic reasons, whereas women are often motivated by family-related advantages [30].
On a further note, the present paper adds to research investigating social inequalities in health after retirement. Conventional measures of socioeconomic positions after labour market exit rely on retirees’ education or their last social position. In line with previous research, our findings support measuring indicators of social position throughout entire life course [8,9,31], and we introduce the history of pension contribution as an alternative indicator of social position. As such, contributing to pension schemes may be an important mechanism for the social gradient in health and is directly linked to material circumstances. Research on social inequalities in health after retirement may thus be supplemented by investigations of previous employment histories that set at least parts of the pathway from social disadvantages to health [7]. Our findings additionally illustrate that continuously working without contributing to pension schemes is associated with elevated depressive symptoms, independent of retirees’ incomes. This lends support to a psychosocial component behind the relationship of material circumstances after retirement and health, with cumulating disadvantages throughout individual life course.
This study profits from several strengths. Notably, detailed life history data from a large study sample and the use of sequence analysis to summarise entire histories of contributing to pension schemes enabled us to gain further insight into links between previous employment histories and later depressive symptoms. Nevertheless, we have to consider several limitations. First, we focus on individual determinants of poor health and we do not consider details of country-specific pension schemes. Country-specific pension systems may be important factors in explaining health inequalities after retirement, and we could therefore have included details on pension schemes into analyses, e.g. net pension replacement rates or state pension age, and investigate how these are related to poor health [32]. We adjusted for country-specific affiliation in multivariable regression analyses, however, and furthermore investigated the distribution of individual pension contributions for each country separately in sensitivity analyses. Importantly, we find that all categories of our key variable are represented in each country participating in SHARE, and findings are similar after excluding Denmark and Ireland – the two countries with the most diverging distribution of pension contributions. However, further research needs to examine in more detail how pension contributions vary by country, or if national pension policies moderate the associations between contributing to pension schemes and depressive symptoms, e.g. by affecting average pension levels. Secondly, we have to consider limitations that are due to our decision to include only retirees with an employment history (either employed or self-employed) of at least 5 years. In doing so, we have excluded workers with a very weak attachment to the labour market (those who have been in paid work for less than 5 years) but included workers with a discontinuous attachment (5 or more years in paid work). However, pension contributions may be less important for retirees who have been not in paid work most of their working lives, for example because of other disadvantages, such as unemployment periods [22].Future investigations may consider including information on unemployment or family work into their analyses for a more comprehensive investigation of entire employment trajectories. In this study, we have adjusted for the number of years that respondents have worked during their career to address this limitation. Thirdly, our measure of contributing to pension schemes is collected retrospectively. Respondents may have remembered details on their employment history inaccurately, and potential recall bias needs to be considered. Yet, there is increasing support that retrospective life history data provides reliable and valid information [33]. Fourth, although we minimize the risk of reverse causation by excluding workers with poor mental health prior to and during their working careers, we cannot sufficiently control for potential health selection. Finally, the measurement of pension contribution is based on simple binary indicators of whether respondents contributed to public, occupational, or private pension schemes. Clearly, this does not adequately represent the variety of different pension schemes, and – importantly – their monetary value. Additionally, we do not consider other possibilities of retirement arrangements, such as housing and wealth accumulation. However, although the question of whether respondents contributed to any pension schemes is undoubtedly unspecific, this measure has at least two advantages. First of all, it enables us to identify highly disadvantaged workers with precarious employment relations that do not contribute to any pension schemes at all. Plus, our indicator may be less biased by incorrect recalls of individual employment histories than more detailed descriptions would have possibly been.
In conclusion, our study shows that elevated depressive symptoms are linked to discontinuities in contributing to pension schemes, independently from current income. Our findings are consistent for employed women (but not for employed men), and self-employed men (but not for self-employed women). On a more general note, our study suggests that it may be fruitful to investigate details of individual employment histories to assess social inequalities in health in old age. In view of aging societies in Europe and persisting health inequalities in later life, an understanding of the roots of these health inequalities in individual employment histories may contribute to health policies specifically designed to reduce social inequalities in health.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted in the frame of the German initiative “Labor market participation at older ages” which is financed by the “Fund for the Future” of the Ministry of Innovation, Science and Research, North-Rhine Westphalia from 2016-2019. HH and MW were supported by funding from the German Research Foundation (DFG, project number: WA 3065/3-1). This paper uses release 6.1.0 data from SHARE Waves 2 and 3 (SHARELIFE; DOIs: 10.6103/SHARE.w2.500 and 10.6103/SHARE.w3.500), for methodological details see [15]. The SHARE data collection has been funded primarily by the European Commission through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812) and FP7 (SHARE-PREP: N°211909, SHARE-LEAP: N°227822, SHARE M4: N°261982). Additional funding from the German Ministry of Education and Research, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064) and from various national funding sources is gratefully acknowledged (see ![]() ).
).