
Abstract
Introduction
Major depression is one of the most common mental disorders in the United States. An estimated 7.1% of all US adults, 17.3 million adults, had at least one major depressive episode (National Institute of Mental Health, 2019). The past year prevalence of major depressive episodes has been estimated to be 5.4% among Hispanics, 7.9% among non-Hispanic Whites, and 5.4% among non-Hispanic Blacks (National Institute of Mental Health, 2019). Between 2005 and 2012, data collected from the NHANES indicated that Hispanics and African-Americans were significantly more likely to experience serious depression than Whites (Rodriquez et al., 2018). Overall, depression is a leading cause of disability and is associated with a cost of $210.5 billion per year in the US (Greenberg et al., 2015).
Left untreated, depression can worsen and adversely affect one's quality of life and workplace productivity (Williams et al., 2017). Meta-analyses suggest that depression treatments resulted in reductions in depression (Cuijpers et al., 2011; Linde et al., 2015; Unlu Ince et al., 2014). Specifically, psychotherapy, pharmacotherapy, and the combination of the two were found to be associated with statistically significant reductions in depression scores among those with mild to moderate depression (Cuijpers et al., 2011) and major depression (Linde et al., 2015).
Psychotherapy interventions that were found to be effective across these meta-analyses included cognitive behavior therapy (face-to-face, remote therapist-led, guided self-help, and no/minimal contact), interpersonal psychotherapy, problem solving therapy (both face-to-face and remote therapist-led), non-directive supportive therapy, and behavioral activation therapy (Cuijpers et al., 2011; Linde et al., 2015; Unlu Ince et al., 2014). Improvements in depression were noted across a variety of subgroups including older adults, those with medical conditions, and women with postpartum depression (Cuijpers et al., 2011). One meta-analysis specifically examined these effects among racial-ethnic minority groups and found that psychotherapy was effective specifically among Hispanics (Unlu Ince et al., 2014). This study did note that Hispanics who enroll in psychotherapy are more likely to be well educated and have fewer barriers to seeking care (Unlu Ince et al., 2014), which highlights the importance of examining barriers among a representative community sample.
Approximately 35% of adults with a major depressive episode do not receive treatment (National Institute of Mental Health, 2019). Furthermore, Hispanics are at higher risk than non-Hispanic Whites of having untreated depression in the US (Menselson et al., 2008). A recent comprehensive study of Americans’ attitudes toward access to mental health care revealed mental health services are insufficient for all groups in the United States, and despite demand, the root of the problem is lack of access or the inability to find care (Cohen Veterans Network, 2018). Specifically, 56% of Americans seek or want mental health services but are unable to access them (Cohen Veterans Network, 2018). Barriers may include high cost and insufficient insurance coverage, limited options and long waits, lack of awareness, and social stigma (Cohen Veterans Network, 2018). For example, Hispanics are more likely to come from low socioeconomic backgrounds than non-Hispanic White Americans, which may make it difficult to afford out-of-pocket costs of mental health care (Anastasia & Bridges, 2015; Derr, 2016; Escarce & Goodell, 2007; Horevitz et al., 2015).
Among Hispanics aged 18–74 years living in New York, San Diego, Miami, and Chicago participating in a cohort study, only 5% used antidepressant medications despite a much higher prevalence of major depression (Wassertheil-Smoller et al., 2014). A nationally representative survey found a similar proportion of Hispanic respondents using antidepressants (5%) compared with 16.5% of non-Hispanic White respondents (Pratt et al., 2017). Thus, increasing access to mental health services and treatment might be an effective public health intervention in which to achieve better mental health among Hispanic populations (Falgas et al., 2017).
A variety of reasons for reduced access to mental health care among Latinos exist. According to the Andersen model of health care utilization, there are environmental (i.e., health care system), population (i.e., predisposing, enabling, and need variables), and health behavior (i.e., personal health choices, use of services) determinants of health care utilization (Phillips et al., 1998). Barriers among Hispanics may differ in comparison to those of the general population. For example, health insurance is an enabling characteristic that reduces the cost of care and thus the lack of it is a barrier (Berchick et al., 2019). In 2018, non-Hispanic Whites had higher proportions of any insurance (94.6%) compared with Hispanics (82.2%) who had the lowest of all racial/ethnic groups (Berchick et al., 2019). A much larger percentage of non-Hispanic Whites (74.8%) compared with Hispanics (49.6%) were privately insured while a much larger percentage of Hispanics (17.8%) compared with non-Hispanic Whites (5.4%) were uninsured (Berchick et al., 2019). This pattern was true for adults and children with 8.7% of Hispanic children – a greater proportion than any other racial/ethnic group – lacking health insurance compared with 4.2% of non-Hispanic White children (Berchick et al., 2019). Research shows that having health insurance is associated with access to mental health services (Wang et al., 2005). Like trends found in insurance status, disparities exist between non-Hispanic Whites and Hispanics, specifically with respect to receipt of mental health care and psychotropic medication use (Cook et al., 2017).
To address these challenges, some localities and provider networks are implementing comprehensive mental health policies in an effort to reduce mental illness (Zeiss & Karlin, 2008). New York City's ThriveNYC program, which attempts to address the structural, institutional, and care system challenges, at $850 million, is perhaps the largest such effort (Belkin & McCray, 2019; Eisenberg, 2019; Gratzer & Goldbloom, 2019). Depression is the most prevalent form of mental illness, and is therefore central to these expansion efforts (Gratzer & Goldbloom, 2019). However, there is little direct evidence that such broad policy investments help reduce the incidence of mental illness (Frank & Glied, 2006). Hispanics, having high levels of unmet need, may serve as an ideal population for understanding the relationship between barriers to access and the effectiveness of treatment.
To better understand the relationship between financial barriers to mental health care and depressive symptoms, we draw upon a unique community-level survey that includes data on previously diagnosed depression, a measure of the severity of depressive symptoms (the Patient Health Questionnaire 9 or PHQ-9), and a measure of financial barriers to mental health care, including mental health services. Furthermore, we explore this relationship both in the broader sample and within the sub-population that has previously been diagnosed with clinical depression. Within this sample, previous studies have shown that the estimated prevalence of current depression is 12.7%, while the estimated prevalence of ever having depression was estimated to be 18.6% (Belkin & McCray, 2019). The sample has a 7% rate of undiagnosed depression and a 13.3% rate of depression as diagnosed using the PHQ-9 (Williams et al., 2017). The high rate of undiagnosed depression makes it an ideal survey from which to draw inferences about unmet need. Finally, the Hispanic population under study tends to seek care in a large, high-quality academic medical center. This helps ensure that quality of care is relatively constant in the study.
Methods
Data Sources
We used data from the 2015 Washington Heights Community Survey, a telephone survey administered in both English and Spanish to 2,489 sample households in Washington Heights from March to September 2015 (Williams et al., 2017). Washington Heights is a neighborhood in the northern portion of Manhattan, New York City with a population of 214,040 that is 69% Hispanic with a median household income of $53,995, a value that is close to the poverty line for a family of 3 in New York City (Census Reporter, 2021). The questionnaire measured health care access, neighborhood social and economic conditions, general health, and health conditions. The survey had an American Association for Public Opinion Research (AAPOR) response rate of 16.8%. Sociodemographic data on sex, race, marital status, sexual orientation, nativity, and household income were collected. Ethical approval for all study procedures was obtained by the Columbia University IRB.
Measures
The main exposure of interest was having a financial barrier to mental health care. Respondents were asked, “In the past 12 months, was there ever a time when you needed any of the following things, but didn't get it because you couldn't afford it?” Those who chose Mental health care or counseling, were categorized as having a financial barrier to mental health care.
Our outcome of interest was depression score as measured by the Patient Health Questionnaire-9 (PHQ-9). The PHQ-9 is comprised of nine items that ask respondents, “Over the
To measure mental health history, respondents were asked, “Have you ever been told by a health professional that you have a depressive disorder, including depression, major depression, dysthymia, or minor depression.” As a sensitivity analysis, we ran two models where we first controlled for and then excluded those with a recent diagnosis of depression. Respondents were also asked, “Have you been told that you have a depressive disorder in the past 12 months? For both questions, response options were Yes, No, Don't know, or Refused.
Statistical Analysis
We used traditional multiple regression models and the more novel technique, propensity score matching, to control for confounding (D’Agostino, 1998). Because the exposure was rare, little power to detect small effect sizes using traditional analytical techniques could be an issue. Nonetheless, multiple linear and logistic regression models were used to identify significant correlates of depressive symptoms and the likelihood of being clinically depressed, respectively.
First, deploying the entire survey sample, we ran an unadjusted analysis to determine the association between financial barriers to mental health care and depressive symptoms. Then, we controlled for having been previously diagnosed with depression, diagnosed with depression in the past 12 months, sex, age, race, marital status, sexual orientation, nativity, and household income. Next, to conduct a conditional analysis, we repeated the analyses among those diagnosed with depression. Finally, analyses were conducted among those who had been diagnosed with depression in the past 12 months (n = 202) to determine if the relationship between financial barriers to mental health care and depressive symptoms was more evident among individuals with a more recent diagnosis of depression. All analyses were conducted using Stata 14.0.
Propensity score matching
We used PSM to more fully address confounding (D’Agostino, 1998). Traditionally, observational studies cannot incorporate randomization as a means of allocating participants to exposure groups, as is done in experimental studies to ensure a balance between treatment groups. PSM can approximate randomization by balancing exposure groups on a number of characteristics, ensuring that no substantial differences between groups that may skew the study findings are observed (D’Agostino, 1998).
The goal of the PSM approach in this study was to match those in each group with a similar probability of having financial barriers to mental health services. Every exposed individual was matched up to five unexposed based on previously diagnosed depression, age, ethnicity, marital status, household income, and sexual identity. We used logit regression to calculate a propensity score for each respondent to indicate the probability of having a financial barrier to mental health care or counseling. We used a nearest neighbor propensity matching approach with a caliper width of 0.01. Propensity scores were calculated using the Stata package PSMATCH2.
Following matching, participants were “alike” in all observed characteristics, except for that of the exposure; therefore, any effect on the outcome was attributable to financial barriers to mental health services. Specifically, each respondent with a financial barrier to mental health care or counselling was then exchangeable with a respondent with no financial barriers to mental health care or counseling (i.e., could approximate the counterfactual of the exposed).
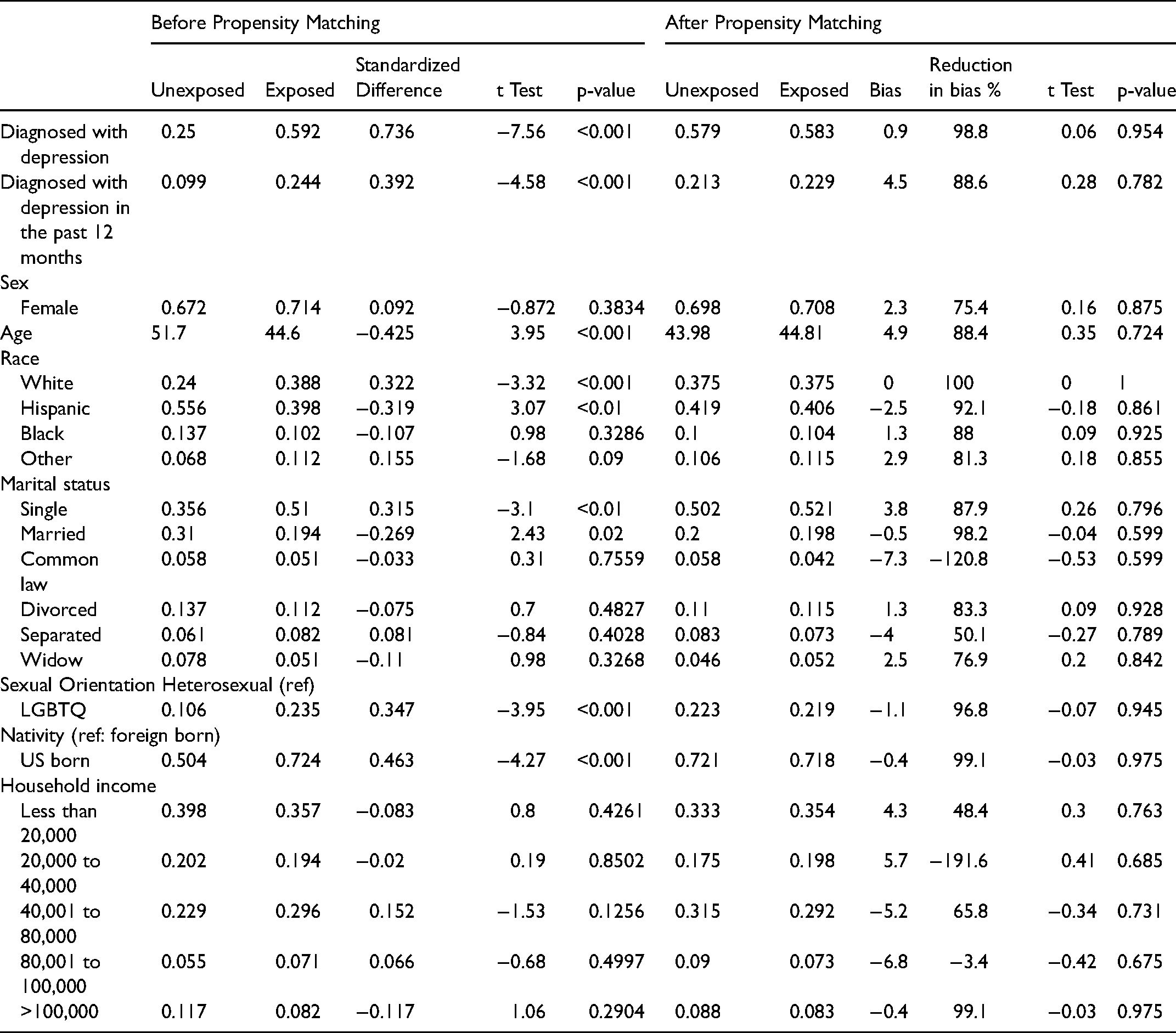
We tested the conditions of the PSM method using the Stata package PSTEST to ensure that the PSM resulted in appropriately matched samples. This method allowed us to compare means between the exposed and unexposed groups (via two-way t-tests), and to determine the reduction in bias post-matching. We used histograms to visualize the distributions of propensity scores for the exposed and unexposed groups (see Figure 1). Based on these tests, we determined that our PSM methods resulted in a well-matched sample.
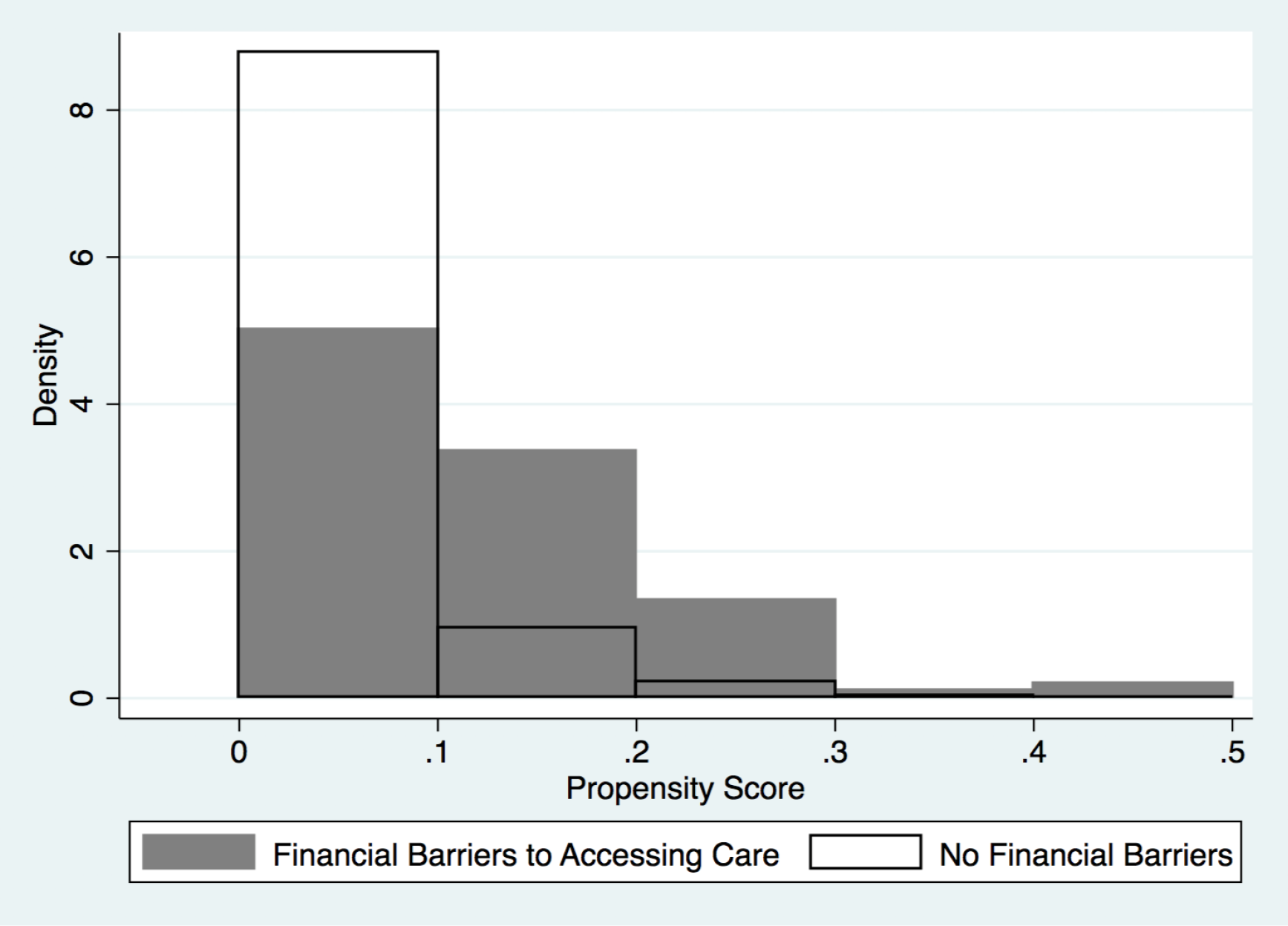
Histogram showing the relationship between the density and propensity score according to whether respondents had access to medical care.
Results
Characteristics of the sample are provided in Table 1. The sample was majority female (69.8%) and Hispanic (59.5%). The proportion of Latinos in this neighborhood is higher than that of Manhattan (25.7%) and New York City (28.2%) in 2015 but is reflective of Washington Heights. The estimated prevalence of clinical depression in this sample was 14.8%.
Characteristics of Participants in the 2015 Washington Heights Community Survey.
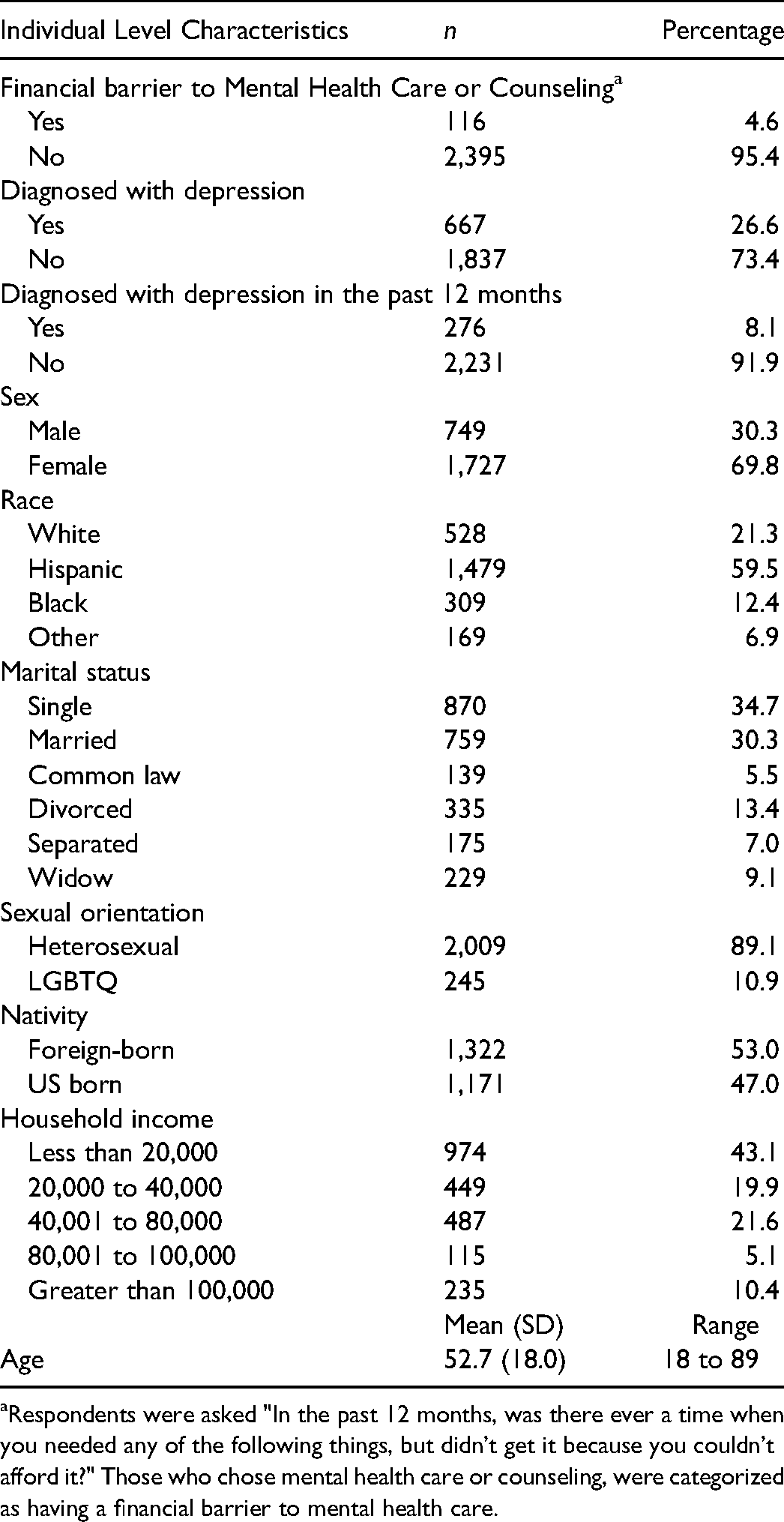
Respondents were asked "In the past 12 months, was there ever a time when you needed any of the following things, but didn't get it because you couldn't afford it?" Those who chose mental health care or counseling, were categorized as having a financial barrier to mental health care.
We also found disparities between sociodemographic groups. For example, those who identified as Hispanic, LGBTQ, foreign-born, and low household income, had higher depressive scores compared to non-Hispanic White, heterosexual, US-born, and higher household income backgrounds, respectively (Table 2). Those who identify as other ethnicities and those from lower household income backgrounds were also more likely to experience clinical depression than non-Hispanic Whites and those from higher household incomes, respectively (Table 3).
Associations between Financial Barriers to Mental Health Care or Counselling and Depressive Symptoms.
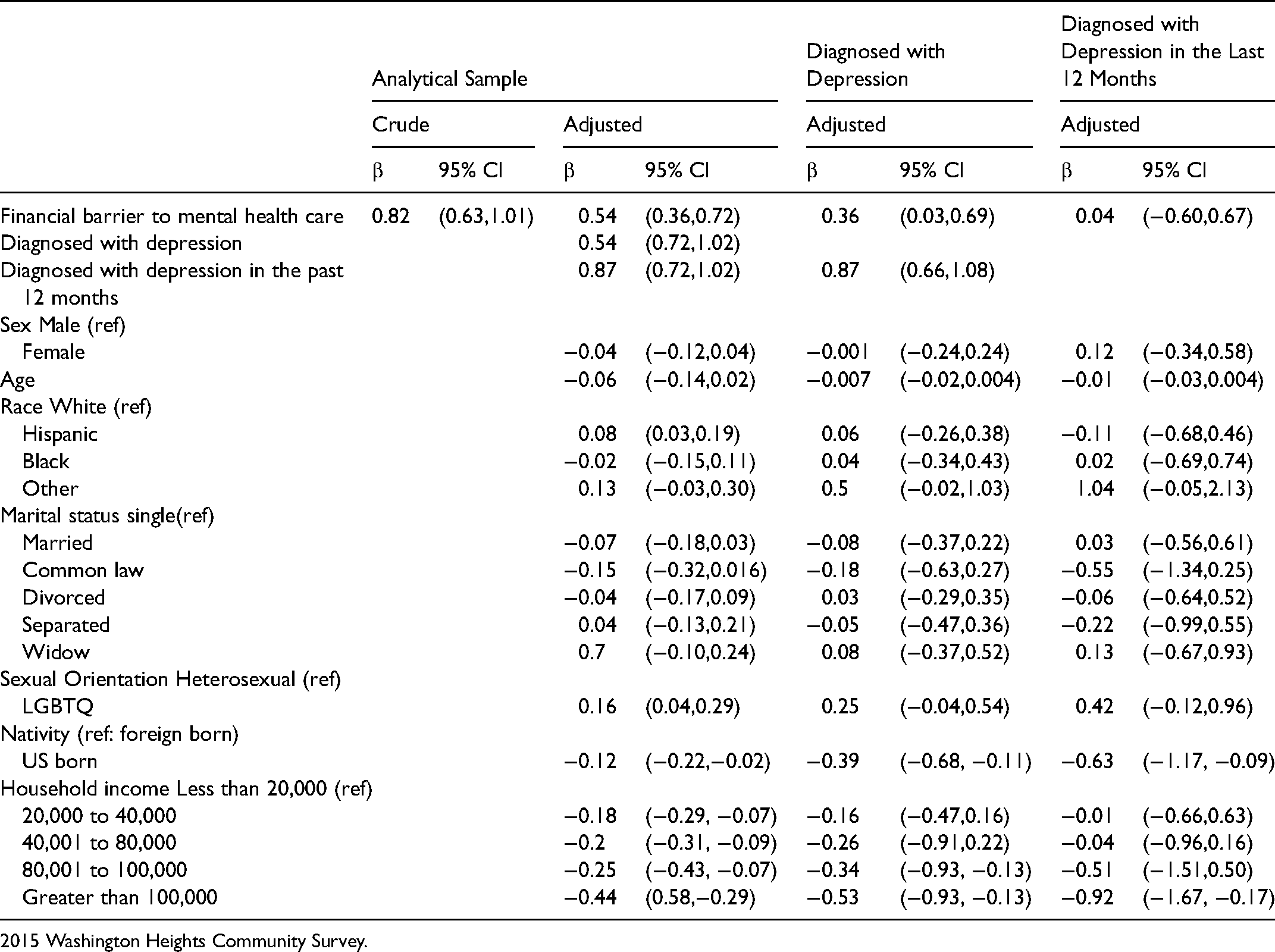
2015 Washington Heights Community Survey.
Associations between Financial Barriers to Mental Health Care or Counselling and the Likelihood for Clinical Depression.
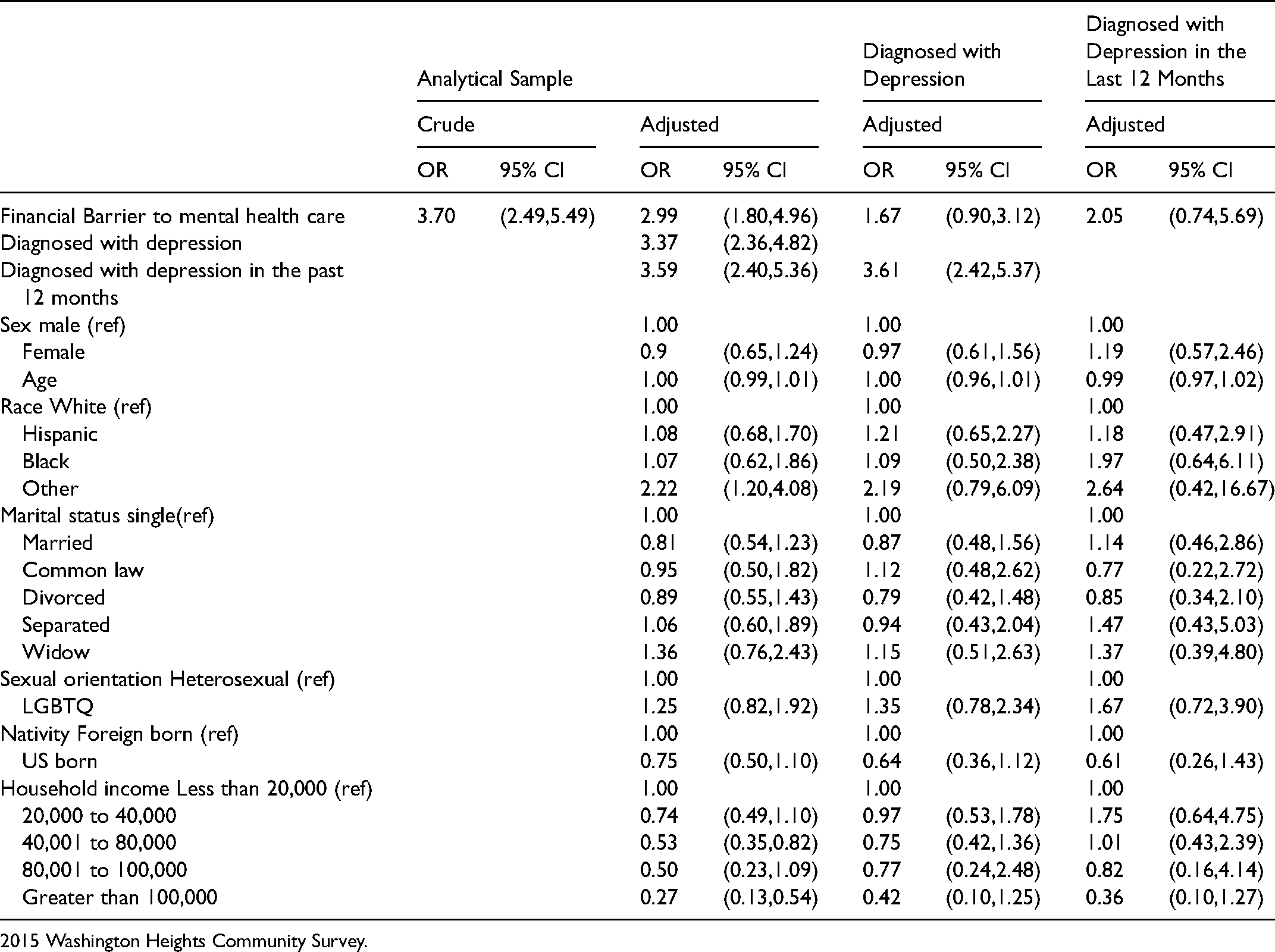
2015 Washington Heights Community Survey.
The results from the multiple linear regression model for depressive symptoms showed that among the whole sample, after controlling for confounders, those who experienced financial barriers to mental health care had significantly higher depressive symptoms in comparison to those who could afford mental health care (β = 0.54, 95% CI = 0.36,0.72) (Table 2). Among those who have been diagnosed with depression, after controlling for confounders, those who experienced financial barriers to mental health care had significantly higher depressive symptoms in comparison with those without such barriers (β = 0.36, 95% CI = 0.03, 0.69) (Table 2). When the analysis was repeated among those diagnosed with depression in the past 12 months, there was no association between having financial barriers to mental health care and depressive symptoms.
When multiple logistic regression was conducted, having a financial barrier to mental health care (OR = 2.99, 95% CI = 1.80, 4.96) was significantly associated with the likelihood for meeting the PHQ-9 cut-off for clinical depression only among the whole sample, while controlling for confounders (Table 3). When restricting the sample to those with a history of depression, those with financial barriers to mental health care or counseling were more likely to experience clinical depression, in comparison to those who had access. However, the association was no significant (OR = 1.67, 95% CI = 0.90, 3.12). Similar insignificant findings were observed when the sample was restricted to those who had been diagnosed with depression in the last 12 months (OR = 2.05, 95% CI = 0.74, 5.69) (Table 3).
We also identified correlates of financial barriers to receiving mental health services. In comparison to non-Hispanic White participants, Hispanic and Black respondents were not significantly more likely to experience financial barriers, but those who identified as “other” were more likely to experience such barriers (Appendix 1).
Results of Propensity Score Analyses
Figure 1 illustrates the distributions of propensity scores by exposure group. As demonstrated in these histograms, there is overlap between the two distributions suggesting a well-matched PSM. Table 4 shows the mean of each covariate in the exposed and unexposed groups of the unmatched cohort. Of the 9 variables, 7 had a significant t-test (p < 0.05), suggesting different means between the exposed and unexposed. Table 4 also presents the mean values of the covariates after matching. After matching, no covariates had a significant t-test (p > 0.05) between the exposed and unexposed groups, which indicates that confounding has been eliminated. Also, as demonstrated in Table 4, we see that matching resulted in a relatively small degree of bias. Therefore, the PSM analysis was deemed valid based on the aforementioned histograms, covariate balance, and degree of bias after matching.
Covariate Imbalance Before and After Propensity Matching.
Among those with depression, when propensity score matching was utilized, experiencing financial barriers to mental health care was significantly associated with higher depressive symptoms (β = 0.63, 95% CI = 0.37,0.89). Also, in comparison to those who had no financial barriers to mental health care, those who did were significantly more likely to be clinically depressed (OR = 2.38, 95% CI = 1.46, 3.89).
Discussion
In this investigation, we used a survey that is uniquely designed to assess unmet medical needs within a predominantly Hispanic community that primarily used a large, high quality academic medical center. We found that financial barriers to mental health care were associated with higher depressive symptoms and a greater likelihood of being clinically depressed. Similar findings were observed when using both multiple regression analysis and propensity score matching. However, associations were more robust in the propensity score matching analysis. Also, within this predominantly Hispanic populated neighborhood within New York City, there was no significant difference in likelihood of experiencing financial barriers to mental health care among Hispanics or Blacks, in comparison to non-Hispanic Whites.
The racial disparity between Hispanics and non-Hispanic Whites for untreated depression in the US is well documented (Anastasia & Bridges, 2015; Derr, 2016; Menselson et al., 2008). Previous research suggests access to treatment is a significant barrier (Derr, 2016; Escarce & Goodell, 2007). This survey is uniquely designed to assess barriers to care and contains a validated measure of depression. The survey was conducted among a representative sample of lower income, predominantly Hispanic respondents. Finally, the community within which the survey was conducted primarily used a large academic medical center for access to mental health services. This adds to the literature on this topic, much of which has not used representative samples, holds quality of care constant, or is targeted to a Hispanic population. In addition, the use of propensity score matching adds to the literature by employing a statistical technique that, to our knowledge, has not previously been used to examine the estimated effect on depressive symptoms and barriers to accessing treatment, which contributes to the evidence base on this topic. Our study examines barriers to depression treatment in a community where a recent initiative, New York City's ThriveNYC program, was implemented to address access barriers (Belkin & McCray, 2019; Eisenberg, 2019; Gratzer & Goldbloom, 2019). While our study is not an evaluation of the ThriveNYC program, it uses a community survey conducted during its implementation to better identify barriers to accessing depression treatment that may be specific to Hispanics in a context where overall access is being addressed.
While the policies employed to improve access to the quality and quantity of mental health services are highly controversial (Frank & Glied, 2006), there is some evidence of a previous linkage between service provision and depressive illness. For example, among people who have been diagnosed with depression, a majority of those who did not receive treatment experienced a recurrence of depression within three years (Bazargan et al., 2005). Our findings suggest that decreasing financial barriers to mental health care or counseling may help mitigate the burden of mental illness. Further research should use quasi-experimental study designs to examine whether these relationships are causal. One potential example is the opportunity to examine differences in clinical outcomes after the rollout of New York City's Thrive initiative using Medicaid or hospitalization data.
While other studies have shown lower rates of depression among the foreign-born than native-born people (Alegria et al., 2017; Huang et al., 2007), our study finds that foreign-born Hispanic in Washington Heights are at higher risk of depression than native-born people. It is unclear why our sample differs from the nation as a whole, but access to health insurance may play one role (Sanchez et al., 2017).
Increasing access to mental health services among Hispanics would require understanding the specific barriers to mental health services experienced by this population group. Earlier work has shed light on the underlying social determinants of health that lead to barriers to accessing mental health services. Specifically, perceptions of stigma, lack of social connection and engagement, vulnerability about sharing the security of their private information, lack of interpreters, cultural differences, and concealing depression symptoms have all been identified as barriers to accessing care (Interian et al., 2007; Uebelacker et al., 2012).
We use quantitative data to show that financial barriers to accessing mental health care are related to the severity of depression. Our findings point to a need to address high medical costs as one step toward mitigating the burden of mental illness. For example, an expansion of the Affordable Care Act (ACA) to populations with an undocumented legal status could potentially benefit Hispanics. When Deferred Action for Childhood Arrivals (DACA) was enacted in 2012, individuals with an undocumented legal status in the United States as a result of being brought to the US as minors became eligible for a work permit, which enables them to obtain employer sponsored health insurance. In a recent study, researchers observed an increase in insurance coverage when DACA was implemented, which was observed when states granted access to Medicaid to those with DACA (Giuntella & Lonsky, 2020).
Researchers also observed an increase in demand for mental health services and a subsequent reduction in depressive symptoms, indicators of stress and anxiety, and hypertension (Giuntella & Lonsky, 2020). Medicaid expansion has been associated with improving access to care and medication while reducing delaying care due to cost among those with depression (Fry & Sommers, 2018). However, while Medicaid expansion has been associated with reductions in uninsurance and increases in having a usual source of care, Hispanic populations have seen the smallest improvements in these areas, which increased disparities (Yue et al., 2018). This may be the result of more ineligible Hispanic subpopulations compared with other groups. Currently, those with undocumented legal status are not eligible to purchase insurance through ACA and the only option is purchasing insurance privately, which is often unaffordable. While the ACA decreased disparities in access to care between non-Hispanic Whites and some Hispanic subgroups, disparities persist based on citizenship status and language (Alcala et al., 2017). Even among citizens who are eligible for insurance coverage, those who are eligible are far less likely to be insured if they are living in a mixed status family (i.e., some members having documentation and others lacking documentation) (Kemmick Pintor & Call, 2019). Some research has found that Hispanics living in states with higher levels of immigrant policy inclusion were more likely to also be insured resulting in smaller disparities between citizen and non-citizen Hispanics (Young et al., 2019) though these results are not universal (Allen & McNeely, 2017) and need to be further examined. Overall, increasing publicly funded mental health services and then targeting Hispanic populations could increase access to and utilization of mental health services among this underserved population.
Limitations
Results should be interpreted in light of several limitations. First, it is important to note that the study response rate is only 16.8%. The target population for this study is unique in that Washington Heights is a low-income neighborhood with higher proportions of racial-ethnic minorities and foreign-born residents than Manhattan and New York City. Therefore, results may not be generalizable to other populations. Also, the relatively rare exposure may result in limited statistical power preventing us from detecting small effect sizes. However, by applying propensity score matching analysis, another way to control for confounding, we obtained similar results leading to our conclusions. Furthermore, the survey did not measure the cultural background of participants and thus did not capture the diversity within the Hispanic population. This diversity likely explains why our results differ from other studies concerning risks among Hispanic relative to non-Hispanic Whites and with respect to native-born versus foreign-born populations.
This survey was cross-sectional in design and therefore causal relationships may not be inferred. This investigation is needed because of the paucity of studies on mental health among Hispanic populations. Trends in mental health among Hispanic Americans have changed since the time of data collection (Bruzelius & Baum, 2019). However, (1) these trends are unlikely to influence the relative differences we observe, and (2) as a community within a “sanctuary city” New York Hispanics may have been less impacted by changes in national immigration laws. Finally, responses were all self-reported and therefore prone to response bias, which may be particularly true for questions regarding mental health. However, this bias was attenuated as respondents were able to respond to mental health questions through an interactive voice response mechanism versus directly through the interviewer.
Conclusion
Eliminating financial barriers to mental health care or counselling among Hispanics may play an important role in mitigating the burden of mental illness in the United States. Further quasi-experimental evaluations can be conducted to confirm these findings. Also, there is a need for researchers to conduct studies among Hispanic populations that capture its diversity.
Footnotes
Acknowledgments
Roman Pabayo is a recipient of a Canada Research Chairs salary award in social and health inequities.
Availability of Data and Material
Data are available by contacting Dr. Peter Muennig, the Principal Investigator of the Washington Heights Survey, pm124@cumc.columbia.edu.
Authors’ Contributors
Roman Pabayo conceptualized and designed the study, conducted the analyses, wrote the manuscript, and reviewed and revised the manuscript. Claire Benny helped conduct analyses, and wrote parts of the manuscript. Sze Yan Liu helped guide the analysis, helped to interpret findings, reviewed and revised the manuscript. Erin Grinshteyn helped to interpret findings, and reviewed and revised the manuscript. Peter Muennig conceptualized and designed the study, reviewed and revised the manuscript, and is a Principal Investigator on the Washington Heights Survey. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
Roman Pabayo is a Tier II Canada Research Chair in Social and Health Inequities Throughout the Lifespan. The authors have no financial relationships relevant to this article to disclose.
Conflicts of Interest
The authors have no conflicts of interest relevant to this article to disclose.
Correlates of experiencing financial barriers to mental health care and counselling among respondents of the 2015 Washington Heights Community Survey.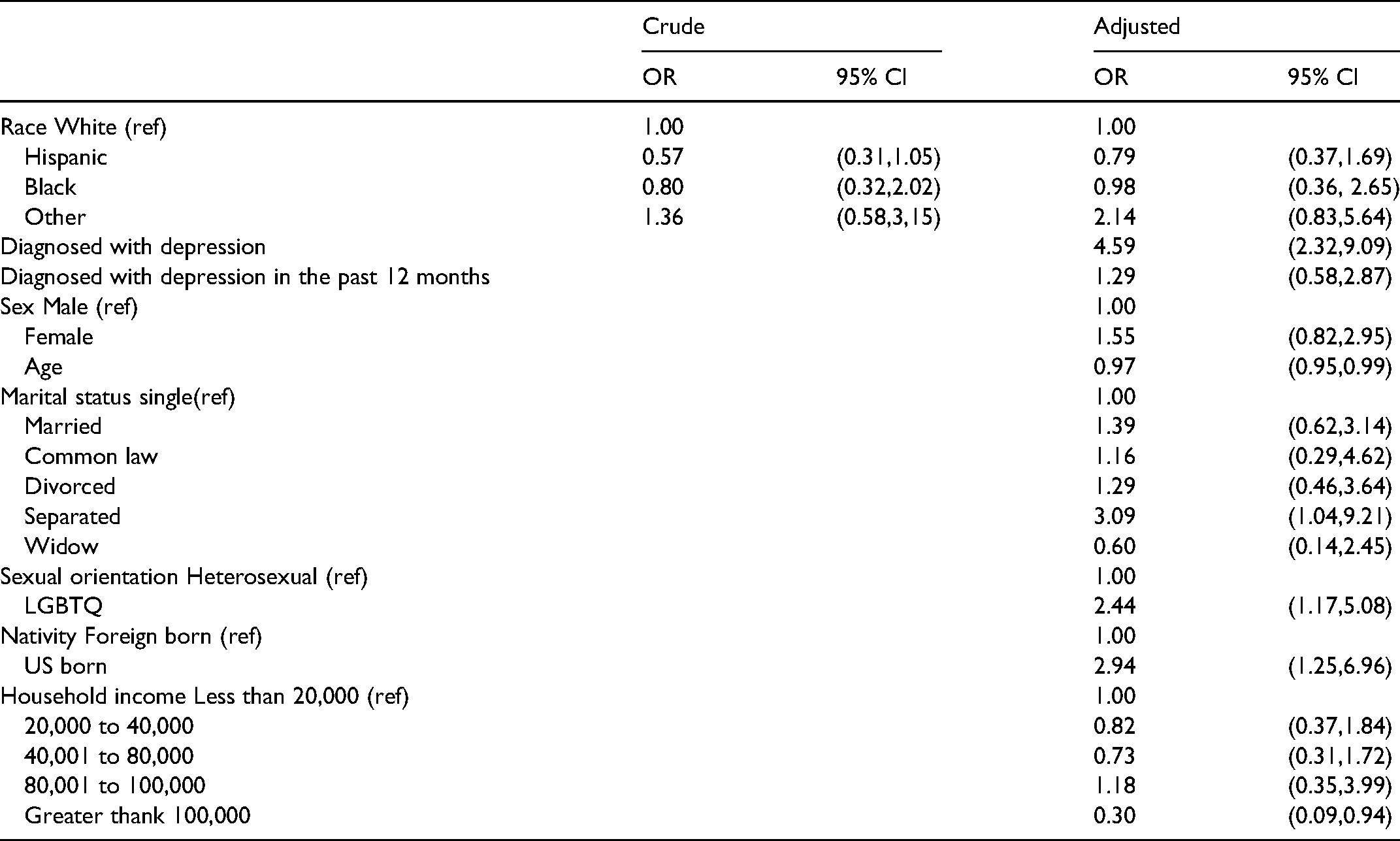
Crude
Adjusted
OR
95% CI
OR
95% CI
Race White (ref)
1.00
1.00
Hispanic
0.57
(0.31,1.05)
0.79
(0.37,1.69)
Black
0.80
(0.32,2.02)
0.98
(0.36, 2.65)
Other
1.36
(0.58,3,15)
2.14
(0.83,5.64)
Diagnosed with depression
4.59
(2.32,9.09)
Diagnosed with depression in the past 12 months
1.29
(0.58,2.87)
Sex Male (ref)
1.00
Female
1.55
(0.82,2.95)
Age
0.97
(0.95,0.99)
Marital status single(ref)
1.00
Married
1.39
(0.62,3.14)
Common law
1.16
(0.29,4.62)
Divorced
1.29
(0.46,3.64)
Separated
3.09
(1.04,9.21)
Widow
0.60
(0.14,2.45)
Sexual orientation Heterosexual (ref)
1.00
LGBTQ
2.44
(1.17,5.08)
Nativity Foreign born (ref)
1.00
US born
2.94
(1.25,6.96)
Household income Less than 20,000 (ref)
1.00
20,000 to 40,000
0.82
(0.37,1.84)
40,001 to 80,000
0.73
(0.31,1.72)
80,001 to 100,000
1.18
(0.35,3.99)
Greater thank 100,000
0.30
(0.09,0.94)