
Abstract
Objective: The aim of this study was to investigate the awareness of palliative care (PC) in a general Swedish population. Design: We developed an e-survey based on a similar study conducted in Northern Ireland, consisting of 10 questions. Closed questions were primarily analyzed using descriptive statistics. Open questions were subject to inductive qualitative analysis. Subjects: The study utilized a population sample of 7684 persons aged 18–66, of which 2020 responded, stratified by gender, age and region. Results: Most participants reported ‘no’ (n = 827, 41%) or ‘some’ (n = 863, 43%) awareness of PC. Being female or older were associated with higher levels of awareness, as was a university-level education, working in a healthcare setting and having a friend or family member receiving PC. Most common sources of knowledge were the media, close friends and relatives receiving PC, as well as working in a healthcare setting. Aims of PC were most frequently identified as ‘care before death’, ‘pain relief’, ‘dignity’ and a ‘peaceful death’. The preferred place of care and death was one’s own home. The main barriers to raising awareness about PC were fear, shame and taboo, along with perceived lack of information and/or personal relevance. The term ‘palliative care’ was said to be unfamiliar by many. A number of strategies to enhance awareness and access to PC were suggested, largely reflecting the previously identified barriers.
Key points
Previous international surveys have identified variable, though less than optimal, levels of public awareness of palliative care.
Public awareness of palliative care in Sweden was found to be low, with 84% reporting ‘some’ or ‘no’ awareness.
Older age and being female were significantly correlated with higher levels of awareness, as was higher educational attainment.
Fear, taboo and shame were the main barriers to raising awareness, along with inadequate information and absence of public debate.
Background
In the upcoming 10 years Sweden’s population is predicted to increase by 1.2 million persons, with the largest percentage increase occurring in the group aged ≥80 [1]. The present mortality rate of ~1% of the population/year is thus also expected to rise. More people are likely to die of non-communicable diseases and to live with complex co-morbidities into old age with increasing frailty. The need for quality care for a longer period towards the end of life (EoL) is thus anticipated to rise significantly [2].
This last decade has indeed seen a rise in the interest and development of palliative and EoL resources within Sweden. A complicating factor with the use of the term ‘palliative care’ (PC), as pointed out by Pastrana et al. [3], for example, nearly 10 years ago but still relevant today, is that it might refer to an approach to care, a specialized knowledge or skill set, a target population or an organizational form [3]. The first Swedish national PC clinical guidelines were published in 2012 [4], and in 2013 new guidelines for the development of PC at the national and local level were presented, aimed primarily at policymakers [5]. Palliative medicine in Sweden was recognized as a sub-specialty for physicians in 2015. These national policy initiatives reflect an increasing international investment in the field; for example, in 2014 the World Health Assembly recognized PC as a core component of health systems [6].
Despite these national and international initiatives, a recent evaluation by the Swedish National Board of Health and Welfare concludes that inequalities and unacceptable deficits in EoL care persist in Sweden [7]. We argue here that issues related to quality and access to EoL care are relevant to a broader group than those directly receiving or providing PC. Although we are unaware of comparable statistics from Sweden, data from Australia indicates that about one third of the population experiences the death of someone close to them in a five-year period [8]; we have no reason to expect that the situation in Sweden would differ notably. EoL care is thus a major public health issue as everyone is affected by the deaths of others close to them, as well as by our own mortality.
Since 2014 the interdisciplinary DöBra research program [9] has been using a public health perspective to influence discussions about PC and EoL to promote constructive change and awareness of the numerous choices which can support better quality of life and death. DöBra is a pun in Swedish, literally meaning ‘Dying Well’, but also an idiom roughly equivalent to ‘awesome’, and the research program consists of several projects, with the overarching goal to work to diminish avoidable suffering related to dying, death and bereavement. In order to effectively promote change and reach out to engage communities, the program began with a joint effort in collaboration with organizers of the 2014 Swedish National Conference in Palliative Care, to map current popular understandings and awareness of PC in the general population in Sweden. In this paper we present results of the survey conducted to this end.
Methods
After perusing the extant literature, we decided to base our survey on one that had been recently conducted in Northern Ireland [10]. As this was the first time a systematic survey on this topic was conducted in Sweden, it was unclear how it would be received by the general public and the extent to which it would be considered ethically sensitive. We therefore chose to work with an established European data collection agency, which had compiled a nationally representative panel of approximately 100,000 adults in Sweden between the ages of 18 and 66 willing to receive Web-based surveys on a variety of topics; the panel had been recruited through a stratified randomization based on official population statistics, and included about 1% of the population. The survey was conducted after approval by the relevant research ethics committee (Karolinska Institutet dnr #2013/1809-31/2).
The invitation to participate in the survey was sent via email to a randomized sample of 7684 persons from the data collection agency’s existing panel in Sweden, stratified by gender, age and region. The goal was to obtain 2000 responses, covering all six healthcare regions in Sweden, which would be generalizable to the national population in the same age range. To ensure this, data were collected until a predetermined number of responses per region were obtained.
The invitation e-letter contained a link to the online survey itself. The first window that opened contained an information letter with an option to continue or decline participation. The e-letter included a short description of the project aim, methods, contact information and the voluntary nature of participation. Continued participation in the survey was deemed an appropriate indication of informed consent by the ethical review board.
The survey contained two sections, and was approximated to take 10 minutes to complete. Section 1 consisted of five multiple-choice questions and two open-ended questions, that aimed to gather specific information on the respondents’ awareness of PC and understandings about existing EoL care. Section 2 contained three open-ended questions to identify perceived barriers to greater familiarity with PC, and strategies to improve access to and engagement with PC.
Translation and pilot testing
We were in contact with the Northern Ireland research team during the translation process, as we aimed for a valid survey that allowed for international comparison but was culturally and linguistically relevant in Swedish. The initial translation was performed by a native Swedish speaker with fluent English, and was commented on and further adapted by a native English speaker fluent in Swedish. After receiving initial comments from our national collaborators, we conducted a series of think-aloud sessions with a convenience sample as they completed the survey, to further revise items which were unclear, in line with the approach used by McGreevy et al. [11].
In the next stage, the online survey was sent to a portion of the sample as a test, in accordance with the data collection agency’s standard procedures. After one day online, 60 persons had answered, and their responses were controlled to ascertain that the survey responses functioned and had reasonable variance. Even open responses were checked for apparent misunderstandings; no further amendments were made at this point and recruitment continued as planned.
Data analysis
Analysis of the multiple-choice questions is presented using descriptive statistics. Differences in proportions to verify differences by gender were analyzed using chi-square tests. Differences in age distribution were analyzed using the Mann–Whitney U-test. The significance level was set at ≤0.05 in all analyses.
The open responses could vary from single words to several sentences and were analyzed qualitatively as follows. All responses were read through repeatedly, and inductively coded based on similarities and differences, by author CW. The responses and initial codes were discussed with authors CT and OL, and adjusted as a result. CT and OL then independently coded 25 responses to each of the open-ended questions in accordance with CW’s coding schemes. The high level of agreement, with only a few differences, led us to continue coding other questions using a process of ‘negotiated consensus’, as previously applied in this research team [12]. After CW completed coding all data individually, these three authors jointly went through the full database, combining similar codes into the larger categories described below. These categories are not mutually exclusive, with the same statement able to relate to more than one relevant category.
Results
A total of 2020 people, between 18 and 66 years of age, responded to the online survey, giving a response rate of 26%, with a mean age of 44.7. Analysis of the 74% non-responders shows that younger people were significantly less likely to complete the survey than older people, but that there was no significant difference in non-response rate between men and women. A lesser number responded to the open questions in Section 2, varying from n = 1450 for the first open-ended question about perceived barriers to n = 596 for the last, requesting any additional comments (data not shown).
Table I presents the demographic features of the respondents. An almost equal number of males (n = 1015) and females participated, both with a generally high educational level.
Demographic background of respondents, in relation to self-assessed awareness of palliative care (n = 2020).
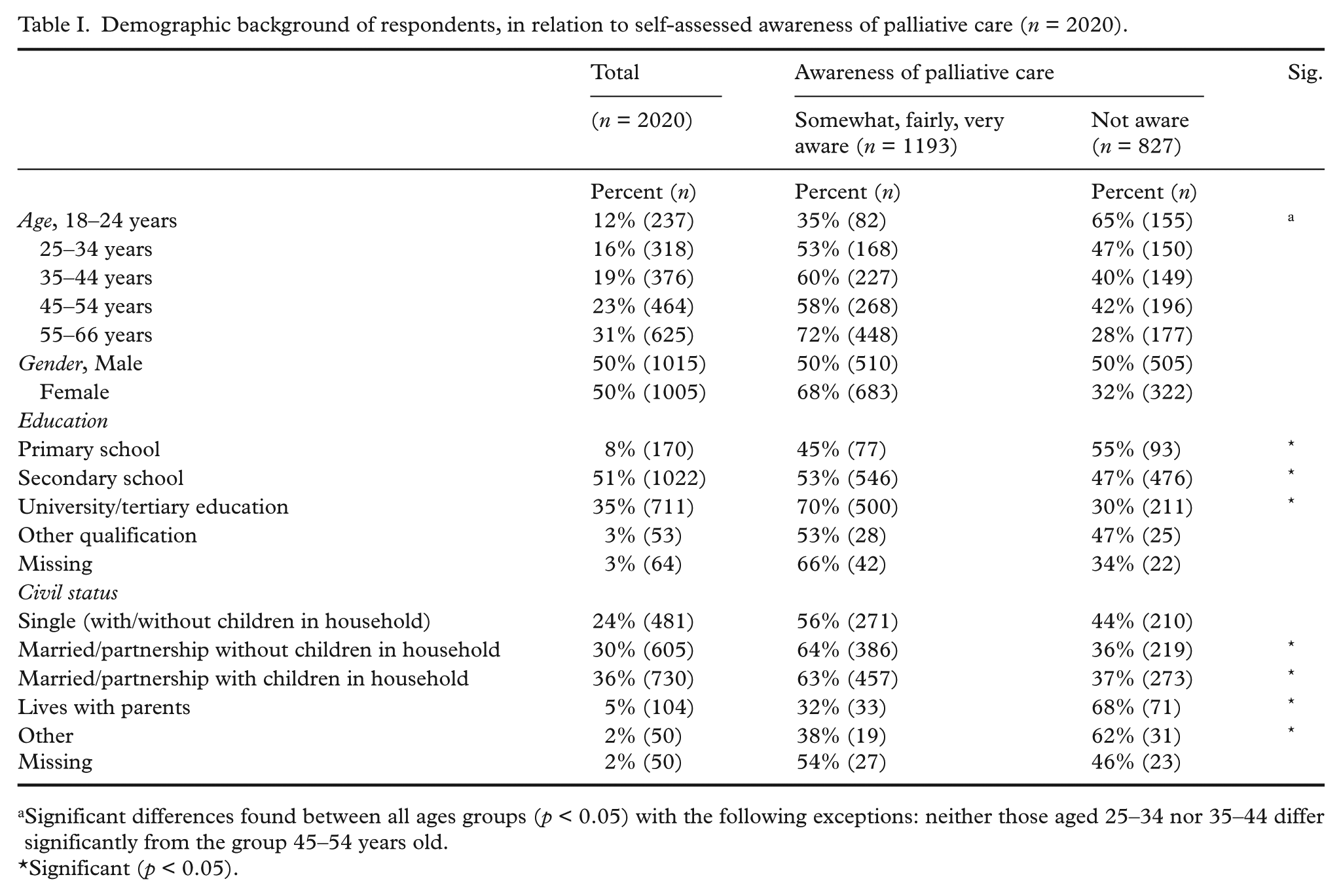
Significant differences found between all ages groups (p < 0.05) with the following exceptions: neither those aged 25–34 nor 35–44 differ significantly from the group 45–54 years old.
Significant (p < 0.05).
Section 1: Awareness and understanding of existing PC
Awareness of PC
Self-assessed awareness of PC was notably limited across all demographics, with a large majority reporting ‘some’ (n = 863, 43%) or ‘no’ awareness (n = 827, 41%), and only 12% reporting ‘quite a bit’ and 4% ‘very much’ awareness of PC. As the group of respondents reporting no awareness of PC was so substantial, we therefore present the results in Table I in relation to that group compared to all other respondents. There was a statistically significant difference between women’s and men’s reported awareness of PC (p = <0.001 chi2), with nearly one third of women and half of men reporting no awareness. There was a statistically significant age difference between groups, with a higher proportion of younger participants responding that they have no awareness of PC. Having a university-level education was also associated with increased awareness of PC.
Source of information
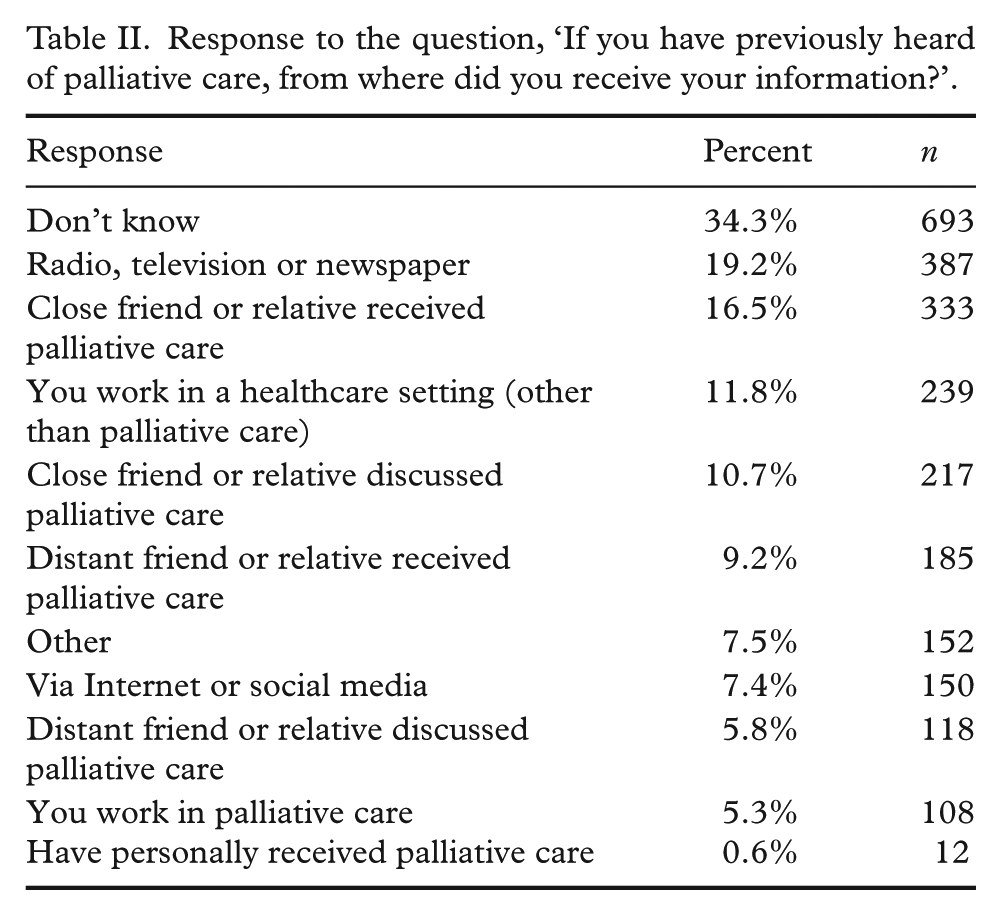
As expected, based on previous responses, a large proportion of participants reported not knowing the source of their information about PC (Table II), with this response provided by 78% of those reporting no awareness of PC (data not shown). The most common sources of information reported were the media, close friends or relatives receiving PC, or working within a healthcare setting.
Response to the question, ‘If you have previously heard of palliative care, from where did you receive your information?’.
Aims of PC
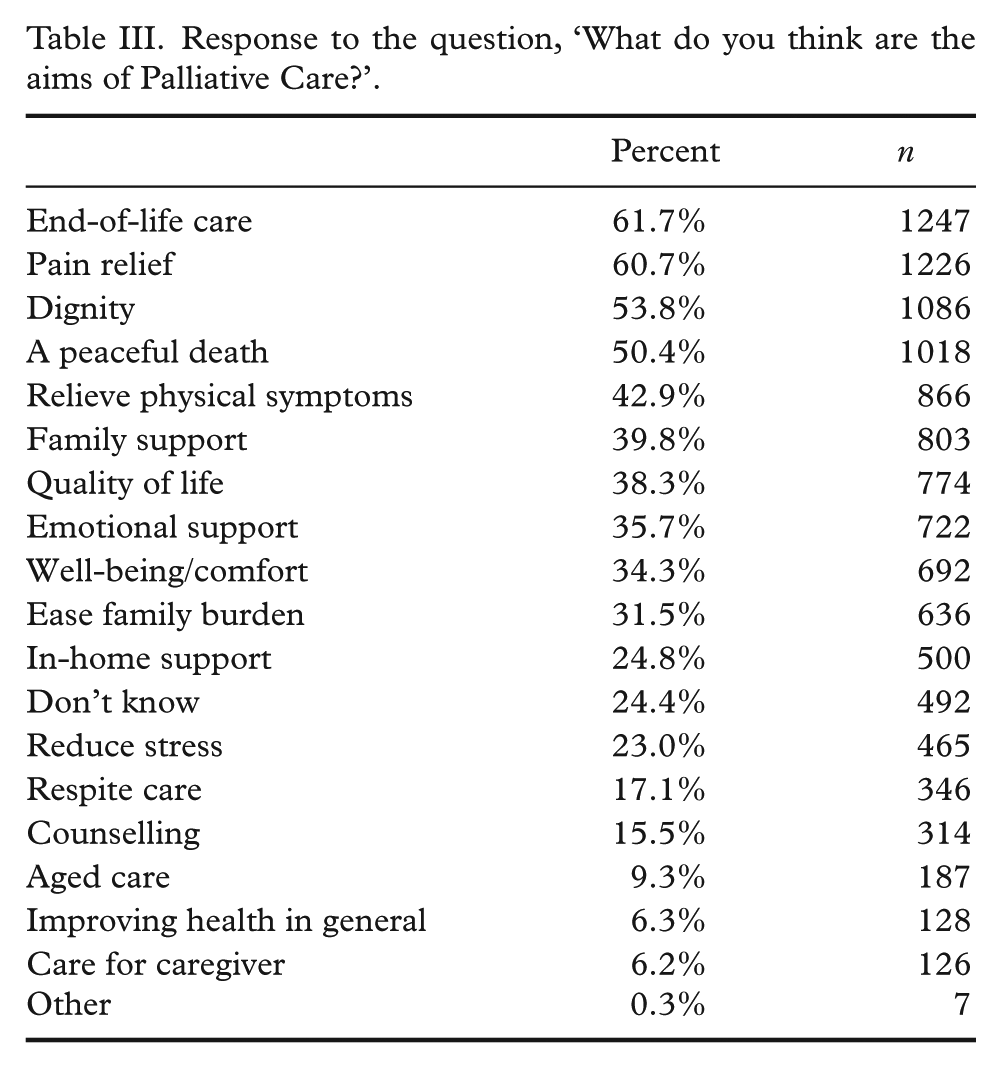
Participants were asked what they considered the aims of PC to be, by choosing all relevant responses from a list of 19 options. As shown in Table III, options chosen by over half of the respondents were: ‘EoL care’, ‘pain relief’, ‘dignity’ and ‘peaceful death’.
Response to the question, ‘What do you think are the aims of Palliative Care?’.
These predetermined descriptions of the aims of PC correspond with answers to the open question preceding it in the survey. Participants were asked to describe in their own words what PC involves, and 1934 statements were provided. The most common responses were coded as referring to the timing of care (EoL or care of persons with a fatal or incurable illness, n = 1117 statements) and the characteristics of care; for example, focus on symptom control, reduction of suffering and quality of life (n = 340), focus on PC as characterized by compassion, empathy and human connection (n = 222) and/or focusing on respect for and dignity of patient and family (n = 166). Only a handful of respondents indicated that PC involved the prolongation of life or delay in disease progression (n = 9) or mentioned euthanasia in some form (n = 6) in their responses.
Preferred place for PC and place of death
When asked to choose from a list of options, a majority, regardless of level of awareness, endorsed the person’s own home as preferred site for receiving PC (68%) or, in the subsequent question, as preferred site for dying (71%). The second most common response to both questions was that it did not matter (11% for care; 9% dying), followed by hospice (10% for care; 8.5% dying). Fewer respondents endorsed a nursing home as preferred place of care (5%) and dying (3.5%), or a hospital (3% for care; 4.4% dying).
Section 2: Open responses related to present barriers and future strategies
Barriers to improving awareness
While not everyone who responded agreed that there were significant barriers to awareness about PC, those statements concerning barriers could be categorized as related to the following four headings.
Fear, taboo and shame (Table IV(a))
A majority of the statements categorized as a barrier to increasing public awareness of PC related to fear of death and social taboos cloaking discussion of the topic.
Barriers to awareness of palliative care.
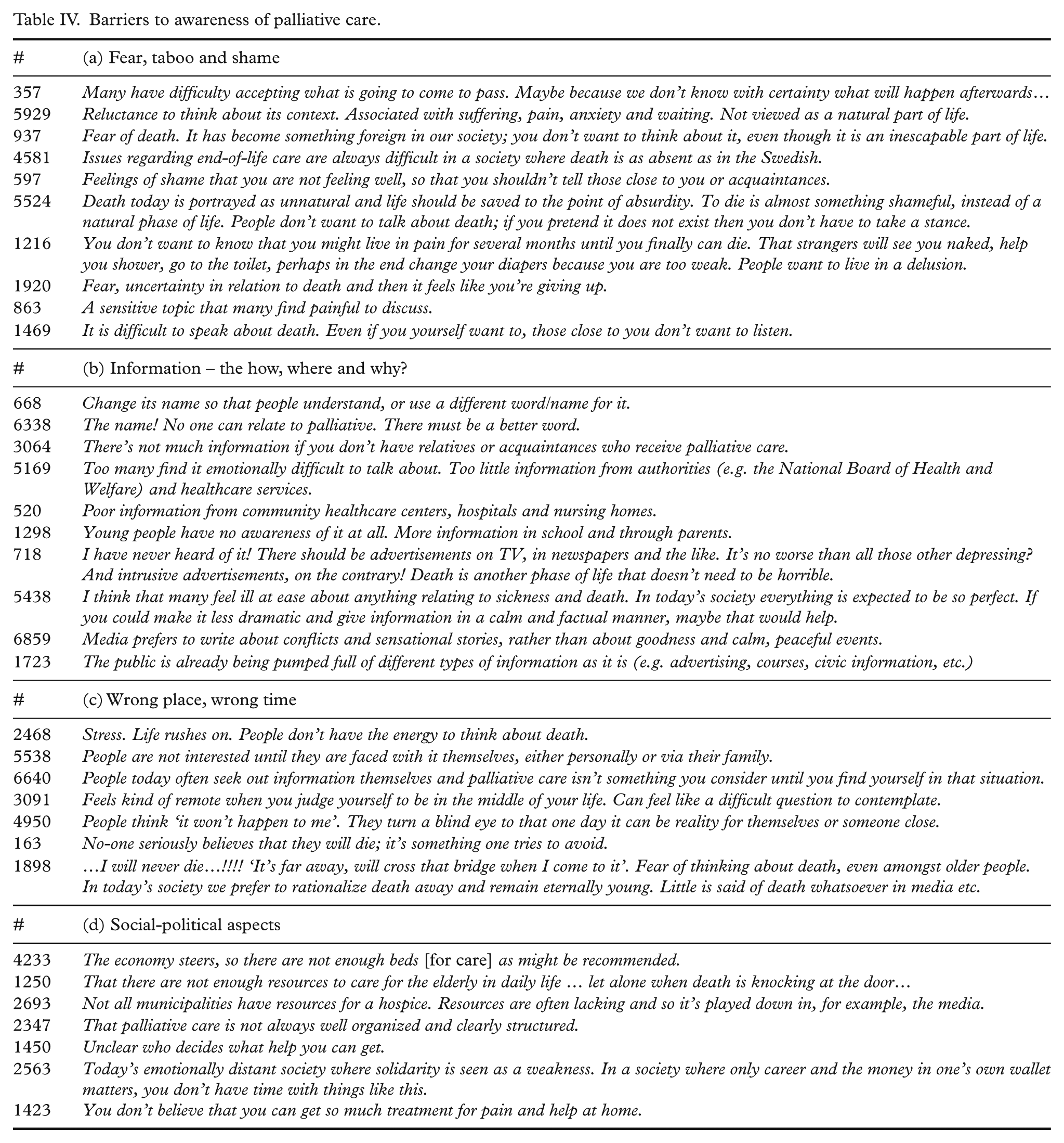
Fear of death was often described in simple and direct language. Intimately connected to fear was a taboo in talking about death, sickness and dying. This could be expressed in single words: for example, fear, silence, taboo and shameful, or longer, more nuanced responses. As illustrated by selected quotes in Table IV(a) (indicated by the respondent code in the text and table), some people elaborated further, bringing focus to the fear of the unknown and inescapable nature of death (#357) and relationship to sickness, pain and mourning (#5929). While responses were often personal, fear and avoidance were also addressed as an issue in Swedish society at large (#937, #4581). Others described a sense of shame at not being in good health and risking loss of autonomy (#597, #5524, #1216) or a sense of giving up and feeling defeated by death (#1920). Another topic directly addressed in responses was difficulties in speaking about death, for oneself and for others (#863, #1469).
Information – the how, where and why (Table IV(b))
Lack of knowledge and inadequate information in areas ranging from personal interactions with healthcare professionals to absence of public debate characterized this second largest category, with nearly one fifth of the statements provided in response to the question categorized here.
Both an individual and a more widespread lack of information about PC were identified. For many, the word ‘palliative’ was problematic and unknown (#668). PC was interpreted as a technical term which was difficult to relate to (#6338) unless one had had direct personal contact with some form of PC (#3064). When commented upon, the responsibility of providing information was placed on all from government agencies and care providers (#5169, #520), to schools and parents (#1298), to a host of various media (#718). Others pointed to fear and taboo as creating difficulties in providing information relating to PC (#5438), including reluctance on the part of media to discuss issues relating to EoL (#6859). In contrast to those respondents referring to a need for further information, others expressed concern over adding to the burden of information already present in today’s society (#1723).
Wrong place, wrong time (Table IV(c))
Rather than fear, taboo or general lack of information raising barriers to a more widespread awareness of PC, this category was shaped by statements indicating that PC was only relevant for those dying, and a reluctance to acknowledge our own mortality.
Key reasons given for this included daily stressors and lack of time (#2468). Statements could also address a lack of interest and feeling of irrelevance that exists unless one has reason to directly confront issues related to death and dying (#5538), in which case some felt information could be sought as needed (#6640). Sickness and death could be seen as in the distant future, making it difficult to relate to in the present (#3091). Other statements ranged from personal avoidance (#4950) of issues related to death, to difficulty conceptualizing one’s own mortality (#163, #1898).
Social-political aspects (Table IV(d))
The final, and smallest, category concerning barriers consists of statements covering a wide range of concerns more structural in nature, from financing, perceived lack of resources, accessibility to services, to mistrust of politicians.
Concise responses included single words such as money, economy, culture, the church, beliefs, politicians and bureaucracy. When respondents elaborated, statements generally addressed financial and political changes within the healthcare system, including general concerns regarding a decrease in beds (#4233) and staffing levels. Some highlighted a lack of resources related to care of the elderly and dying (#1250). There appeared to also be a perceived lack of resources and limited access to specialized PC units (#2693), with some statements indicating a lack of clarity about how PC is organized (#2347) and how decisions are made (#1450). Other statements addressed social barriers to access such as lack of solidarity (#2563) and lack of clarity about what kind of care is possible to receive (#1423).
Strategies to improve awareness, access and engagement
The final substantive question of the survey asked for recommendations for improving knowledge of, access to and engagement in PC. Four categories of suggestions were constructed, with examples of statements from each found in Table V(a)–(d). An additional eight statements argued a need for some form of euthanasia, although not in terms of strategies in response to the questions asked.
Strategies to improve awareness, access and engagement.
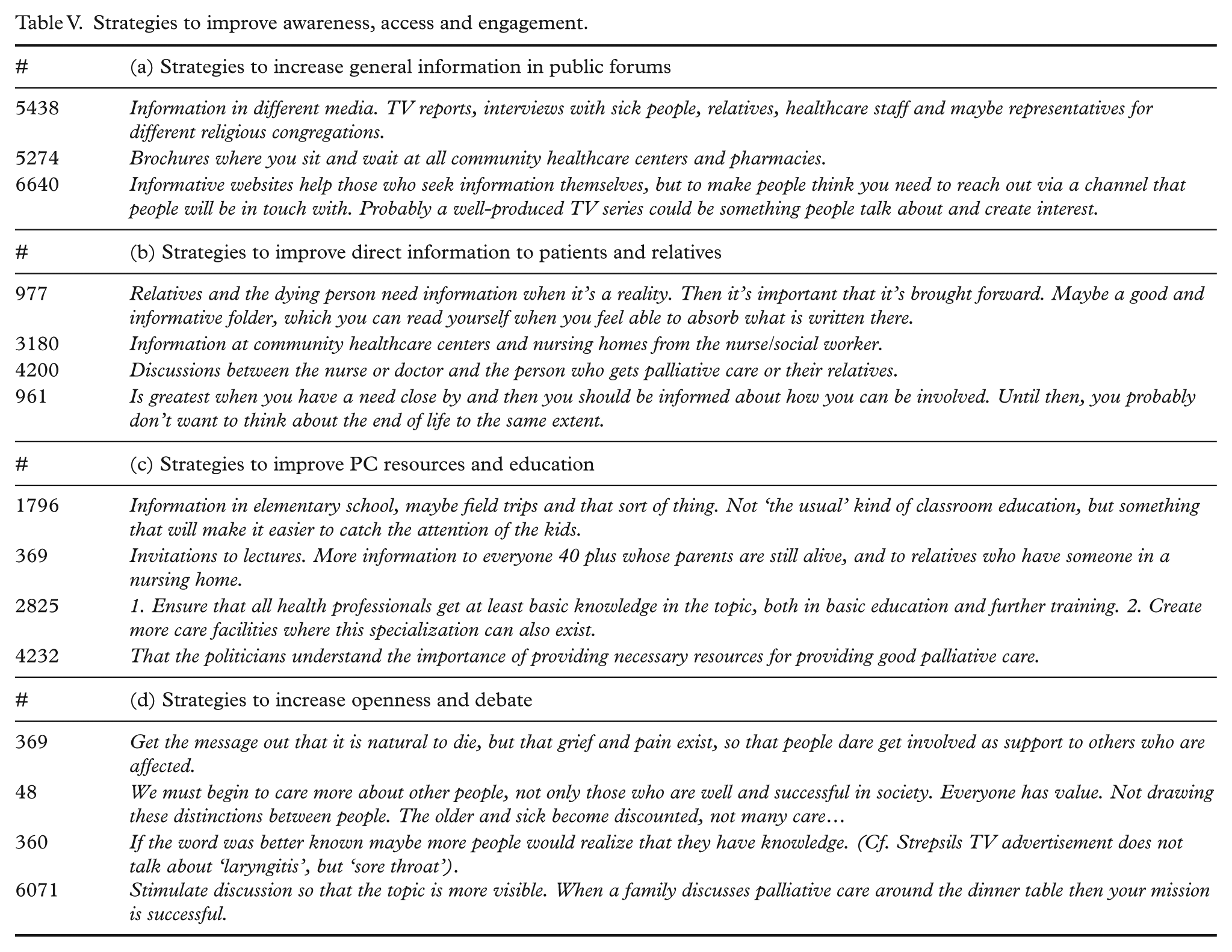
Strategies to increase general information in public forums (Table V(a))
The majority of suggestions are related to easing access to information in all varieties of media (#5438) to increase general knowledge of PC. Suggestions varied from distributing brochures (#5274), to TV programs, to creating Web portals with information (#6640). Relevant information was described as possible to spread via media, advertisements, healthcare providers or easy online availability.
Strategies to improve direct information to patients and relatives (Table V(b))
A smaller group responded that information was necessary only once the need arose (#977), and suggestions related to the improvement of direct information to individuals rather than a general public. Specific contexts for appropriate information and sources of information were identified (#3180, #4200). The need for good information directly to relatives was highlighted (#961).
Strategies to improve resources and education (Table V(c))
Statements related to strategies for improved resources and education included general education in schools (#1796), open lectures for public groups (#369), as well as specialised education, research and training of healthcare professionals (#2825). A general call for increased resources was repeatedly mentioned, with some pointing to the role of politicians in furthering this (#4232).
Strategies to increase openness and debate (Table V(d))
Statements categorized here identified a range of often diffuse strategies to increase openness and willingness to discuss death, dying and PC (#369), including general ideas about a more compassionate society (#48). The need for easily understood terms and concepts was highlighted (#360); that is, the use of everyday terms in everyday life (#6071) rather than ‘professionalized’ and, for many, unfamiliar language.
Discussion
In summary, this population-based survey of the general public in Sweden aged 18–66 years, based on both multiple-choice and open-ended questions, has shown that a majority of participants report having little or no awareness of PC, with most information received via media and experience obtained directly or through family and friends. In this sample, increasing age and being female were related to higher reported levels of awareness of PC, as was university-level education, working in a healthcare setting or having a friend or family member receive PC. Analysis of the open responses indicate that taboos, fear, shame and avoidance of issues related to death and dying, as well as lack of openness and access to information about EoL and PC, were the main barriers to a wider awareness and open discussion of pertinent issues. Recommendations for improving both awareness of EoL issues and access to PC broadly mirrored the barriers identified, including suggestions related to improved resources and education, both in regard to public health issues as well as clinical practice.
Searching scientific databases show no other systematic surveys in Sweden based on public perspectives on EoL or PC, thus limiting comparative data about the Swedish situation. We are, however, aware of a few limited surveys; one conducted over 17 years ago which lacked a systematic sampling strategy, with most of the 1433 responses from attendees at PC conferences [13]. Both that survey and ours share the weakness of underrepresenting older ages, for which these issues may be more relevant. Approximately 25% of the respondents in the prior study [13] stated a desire to be cared for at home. This can be contrasted to the approximately 70% in our survey who chose home as preferred place for EoL care and/or death. Our results are more in line with data based on a 1998 Swedish report of 1200 individuals aged 25–74 [14], indicating that 79%–85% would prefer that they themselves or a close relative be cared for at home, in case of a life-threatening and incurable disease that demanded extensive care. It should be remembered that both this and our survey posed a hypothetical question to people who are not known to be directly dealing with these issues when responding. There is some evidence to show that a preference for home death reduces as death approaches [15] and is also lower among older people [16] – a group who were not represented in this study. The replies to both this 1998 survey and our more recent study differ dramatically from existing data about place of death in Sweden today, with 1.6%–12.5%, dependent on area of residence, of expected deaths taking place at home, according to recent data from the Swedish Register of Palliative Care [17].
On the other hand, there have been multiple international studies looking more specifically at the level of awareness of PC in the general public. Although results vary, these collectively interpret the degree of awareness of PC as suboptimal in various populations [10,18–21]. However, we found the level of awareness of PC in Sweden to be notably lower than the 19% without familiarity of PC in the comparable study from Northern Ireland [10]. In general, the degree of awareness of PC in Sweden was lower than that reported in other western European countries [19,20]. Descriptions of the aims of PC in our survey were strongly profiled to EoL care, as opposed to the more general comfort care highlighted in McIlfatrick et al. [10], with both surveys finding pain relief and dignity to also be highly prioritized.
A number of factors should be considered here. While our response rate of 26% may seem low, the sample is population-based, and this response rate is in line with others conducted by the data collection agency and is higher than other similar surveys on PC [10,20]. However, even if our data is robust compared to similar studies, the limited response rate and the skewed age range in our survey – both due to exclusion of older age groups as well as significant differences in response rates by age – means that results should be interpreted with a degree of caution in terms of generalization to the population of Sweden as a whole.
It should also be remembered that ours was an e-survey, with respondents having the possibility and computer savvy to complement their degree of awareness by searching the Internet for information on PC while responding to the questionnaire. This may explain some participants initially stating no familiarity with PC, but still responding to subsequent open questions in the survey. Being an e-survey may also have compounded a sampling bias by excluding those with less access to digital technology. These sampling factors may be reflected in our somewhat unexpected results, indicating a variety of media as the major source of information, slightly surpassing experience and discussions in personal networks. This differs from international data supporting personal experience as the major source of information and awareness of PC [10,18,20,21] and indicating that media plays a lesser role. This may still be the case in the older population who are also more likely to receive PC, and so our results should also be interpreted with this caveat in mind.
The importance of direct experience was supported, however, by the qualitative data in our survey, highlighting that interest in obtaining information regarding PC increased when issues of dying, death and bereavement become personally relevant. But the qualitative data also includes expressions of difficulty and shame in talking about death and EoL choices, even with close family members. These difficulties and loss of confidence in discussing death can perhaps be traced back to what might be called communities’ loss of ownership in the face of an increased professionalization of death and dying. Communities, including those in Sweden, are viewed as more dissociated and deskilled when it comes to death and dying than in previous times in history [22].
The role of both language and definition become important when interpreting these results. Many commented on the unfamiliarity and perceived foreignness of the term palliative, suggesting that ‘ordinary’ Swedish terms should be used. This may have contributed to an overall lower level of self-assessed awareness of PC, despite our efforts to avoid the use of language relating to specialized knowledge. Although we have unprecedented access to specialized information today via the Internet, the responses to this survey raise the issue of terminology as a hinder in information directed at the public. The regular avoidance of direct reference to terms clearly related to EoL may lead to more confusion than clarity. Data from the UK from 2001 found that people had high levels of awareness of the term hospice, though less familiarity with the term PC [23]; this was confirmed in a later study by Koffman et al. [24] with UK oncology outpatients. These patients, while not well aware of the term PC, were, however, familiar with the term for nurses providing PC, Macmillan nurses, suggesting awareness of available service provision, if not with the professional language used. The results of this and other surveys would suggest the use of more direct communication using non-professional language to better engage the public, rather than professionalizing popular discourse.
A lack of clarity in information about dying and death was again reflected in the recommendations made by respondents to improve awareness of PC. There was variation in the data, with a large proportion of these respondents calling for early and prophylactic information, whereas a minority referred to over-information in society in general, and the need for a personal reason to be willing to engage with issues related to death and dying. The most common recommendations to overcome the lack of openness and taboos that inhibit knowledge of, access to and engagement with PC, were increased information in society at large, and in healthcare contexts. While this call for an increase in public debate and information would perhaps not directly address the difficulty, some respondents identified in talking to family members about death and dying, it may serve as a starting point in more personal discussions. There is inevitably interplay between the public and private, and reducing taboos in one sphere might well affect the other. An assumption that death is taboo has, however, often been critiqued [25,26]; an alternative postulate is that modern problems with death stem primarily from unfamiliarity [22]. The timing and source of information could greatly impact this lack of familiarity, and were indeed recurring concerns in these data. Though many respondents appear to welcome a prophylactic approach which might have potential to reduce taboos and increase advance care planning, others did not invite such discussions before directly needed. A challenge is thus in providing access to societal information that can be incorporated by different individuals to different degrees at their discretion.
This survey can also be considered in light of the findings of the 2015 The Economist Intelligence Unit (EIU) Quality of Death Index [27] in which Sweden ranked notably low in relation to community engagement, based on assessment of volunteerism (30% of score) and public awareness (70% of score). The role of charity and volunteerism in many Anglo-Saxon countries as a mainstay of EoL and PC provision may explain, to some degree, why there is more familiarity and community engagement with PC – but, as noted previously, only with some of its terminology – in these countries. This ranking does, however, appear to be in line with the responses to our Swedish survey, which show an overall low level of awareness and engagement with PC. Our findings are in line with responses to questions recently posed by a large Swedish company arranging funeral services [28], who found that nearly 60% of approximately 1000 interviewees never or less than once/yearly spoke of matters related to one’s own or a family member’s future death, with reasons given for this similar to those seen in our data [28]; for example, fear, sorrow and being unaccustomed to such conversations.
In conclusion, this population-based survey has helped to highlight gaps in awareness among the adult Swedish general public ≤66 years of age, pointing to a widespread disempowerment surrounding EoL issues. This has a number of policy implications, as respondents to our survey do address clinical implications to some extent, although the bulk of responses address public health issues. Dying people and their families are a vulnerable group, and would benefit from improved advocacy; however, one way to improve care for the dying is by strengthening a prophylactic, public health approach focused on increasing preparedness for future encounters with dying, death and bereavement. The post-evaluation recommendations by the Swedish National Board of Health and Welfare [7] address a range of important clinical improvements needed for better direct clinical care of dying individuals and their families. We argue that these need to be complemented with policy initiatives based on increasing public awareness with more equitable access to information, and addressing taboos about death and dying within and beyond the healthcare system. This would be in line with the EIU Quality of Death Index’s conclusions that confronting perceptions of death and cultural taboos is critical to improving EoL outcomes [27], with low levels of public awareness linked to increased invasive procedures at EoL [29] and increased likelihood of dying in hospital. The survey data presented here provides an empirical basis from which we can begin to view death, dying and bereavement through a public health lens, to better stimulate timely discussions and support empowered decision-making, as confronting EoL issues is inevitable for us all.
Footnotes
Acknowledgements
We thank Forte: Swedish Research Council for Health, Working Life and Welfare for their financial support. We also thank the respondents for their generosity in responding, as well as Peter Strehlenert and statistician Sara Runesdotter for their input and engagement in the analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Forte: Swedish Research Council for Health, Working Life and Welfare (2013-1962; 2014-4071).