
Abstract
Keywords
Introduction
Measles is a highly contagious disease that is still a major cause of childhood death and severe disability [1,2]. Although an inexpensive and efficacious vaccine has been available since the 1960s, measles caused approximately 140,000 deaths globally in 2010, with the highest burden in Sub-Saharan Africa [2]. In the World Health Organization (WHO) European region, a significant decline in reported measles cases was seen in the last 2 decades, with cases decreasing from 304,184 in 1991, to 67,759 in 2001 and 8617 cases in 2009 [3]. Despite this substantial reduction, the initial goal of eliminating measles in the WHO European region by 2010 (defined as the absence of endemic measles or rubella cases in a defined geographical area for a period of at least 12 months in the presence of a well-performing surveillance system [4]), was not met, and the number of measles cases in recent years has started to increase [3]. In 2012, there were 33,602 measles cases reported by the countries of the WHO European Region, with 10,271 cases reported by European Union (EU)/European Economic Area (EEA) member states [3]. Measles was targeted for elimination by 2015 [5], but this goal will not be achieved. Progress towards measles elimination has been hindered, as some children are either not immunized on time or are never immunized (the recommended age for immunization varies from 6–15 months, with a second dose required, as 2–5% of children over 12 months of age do not respond to the first dose). Sub-optimal coverage rates often occur in at-risk groups, such as the Roma, Irish travellers and orthodox religious communities; this results in clusters of unvaccinated individuals that reduce overall population coverage below the 95% minimum that is needed for eradication [6] and contributes to dissemination of the disease to other sections of the population.
A further group that is thought to be at increased risk of measles due to insufficient vaccination coverage is migrants. Although migrants are often comparatively healthy, a phenomenon known as the ‘healthy migrant effect’ [7], some studies suggest that certain groups of migrants in Europe are more vulnerable to infectious diseases, such as measles, than the majority population [8–10]; however, current information on the extent to which migrants in the EU/EEA are affected by measles is limited, due to a lack of data.
First, comparisons of migrant health across Europe are challenging, due to varied definitions of who constitutes a migrant. Definitions and classifications are determined by national legislative, administrative and policy factors [11]; therefore, migrants may be classified by their country of birth, nationality, residency or duration of stay [12,13]. Secondly, the quality and type of surveillance data collected still vary greatly between countries. In Europe, measles is a notifiable disease in all 53 member states of the WHO European region; surveillance data for EU/EEA member states are collected by the European Centre for Disease Prevention and Control (ECDC), shared with the WHO European Region Office and then published routinely on the ECDC website [3,14]. However, although efforts have been made in recent years to harmonize national surveillance data collected on migrant-specific variables, such as ‘country of birth’ or whether a case is ‘imported or endemic’, this information is inadequately reported for measles in the majority of member states.
Understanding and meeting the health needs of migrants affected by infectious diseases is becoming increasingly important, in part due to increasing migration flow to and within Europe [15]. In 1990, 6.9% of the total EU population was foreign-born, a figure that has increased to 9.7% of the total population in 2011 [16]. There were an estimated 48.9 million foreign-born residents in the 27 EU member states in 2011, with 32.4 million having been born outside the EU and 16.5 million having been born in a different EU country [16].
The increasing diversity of European populations is inevitably creating new challenges for health systems, which need to adapt in order to accommodate disparate health needs [17,18]. If the goal of eliminating measles is to be met, it is necessary to target the groups at risk of remaining unvaccinated with specific health information and disease prevention campaigns [19]. At present, the lack of data makes it difficult to determine if migrant populations are at higher risk of contracting measles. In light of these gaps in evidence, this paper aims to provide an overview of the burden of measles in migrants in the EU/EEA and to give an assessment of the quality, completeness and comparability of data. Evidence was collected through a comprehensive literature review, expert opinion from infectious disease specialists and a survey of national key informants.
Methods
Comprehensive literature review
A comprehensive literature review was conducted to critically appraise and summarize the available evidence on both the burden of measles and measles, mumps and rubella (MMR) vaccination coverage rates in migrant populations in the EU/EEA. We identified the studies to be included in the comprehensive literature review by searching electronic databases and relevant websites, scanning reference lists of papers and by asking infectious disease experts to identify key publications. We conducted the literature search between July and September 2012, and updated it in April 2015, using three electronic databases and 18 websites of key organizations. The databases and the websites searched for the literature review were:
Databases (last date searched: 07 April 2015): PubMed/Medline, Web of Science and Cochrane Library.
Key websites (last date searched: 07 April 2015): Central European Forum for Migration and Population Research (Poland); Center for Health and Migration (Austria); Danish Research Centre for Migration, Ethnicity and Health (MESU); ECDC; Eugate; European Research Centre on Migration and Ethnic Relations (ERCOMER); EU-Level Consultation on Migration Health; Health Protection Agency (HPA); Global Forum on Migration and Development (GFMD); Global migration group, International Organization for Migration (IOM); Migrant and Ethnic Health Observatory, National Health Service (NHS); United Nations Population Fund (UNFPA); the European health Association UPHA; the WHO; and the World Health Organization, Regional Office for Europe (WHO-EURO).
Our database search strategy was built using a combination of keywords related to measles, migrants and the study setting (EU/EEA):
Measles;
AND Migration, immigration, emigration, migrant, immigrant, emigrant, foreign-born, foreign born, foreigner, asylum seeker, refugee, irregular, citizen, citizenship and nationality;
AND Austria, Belgium, Bulgaria, Cyprus, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Italy, Latvia, Liechtenstein, Lithuania, Luxembourg, Malta, Netherlands, Norway, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden, UK, Great Britain, England, Wales, Scotland, EU, EU/EEA and Europe.
Articles were included if they were descriptive and analytic observational studies, experimental studies, reviews, systematic reviews and meta-analyses; were published in English; and included data on measles in the EU/EEA. Data from non-EU/EEA publications were considered for inclusion to provide background information only.
Eligibility assessment for inclusion was performed independently by two reviewers, initially by screening titles and abstracts, followed by a full-text review to determine final eligibility. Disagreements between reviewers were resolved by discussion. Data relevant to the study questions were retrieved, with high priority given to recent nationally-representative studies and large population-based studies. No minimum sample size was selected, but small hospital-based studies were only included if no other data were available and they reported their limitations in terms of generalizability.
Expert meeting
In October 2012, the ECDC and the Portuguese National Health Institute in Lisbon co-hosted an expert meeting on infectious diseases and migration. The meeting enabled experts to present feedback on the survey to their member states, and allowed member states to share examples of best practice on surveillance, prevention and control targeted toward migrant populations in various infectious disease areas. We include evidence presented at this meeting to provide additional information on the patterns and reasons for measles outbreaks in individual member states.
Survey of EU/EEA member states
A survey of key informants in EU/EEA member states was conducted to collect migrant-relevant measles data not reported to the ECDC’s ‘The European Surveillance System’ (TESSy) database. In May 2012 through July 2012 we developed questionnaires for the survey, which contained open-ended questions on the occurrence of measles among migrants, how migrants are defined for the purpose of measles surveillance and if any specific data are available. A table was also constructed to collect data on the incidence and mortality rates for 2007–2010. The questionnaires were sent out electronically to the ECDC disease focal points in all EU/EEA member states in July through August 2012, requesting a response within 4 weeks. We also considered using data from the TESSy database, but the only potentially relevant variables were ‘importation status’ and ‘probable country of infection’, with no information collected on ‘country of birth’, significantly limiting any conclusions that might be drawn on measles in migrants. Therefore, this data source was not included.
Results
Comprehensive literature review
The literature search identified 195 papers for evaluation. After screening abstracts and titles, 37 articles were selected for full-text screening. Of these articles, 20 were found to meet the inclusion criteria and were included in the final review. The literature review revealed very few papers that studied measles among migrants in Europe; those that mentioned migrants frequently conflated them with indigenous religious or ethnic minorities. Many studies did differentiate ‘imported’ from other cases, but did not ascertain whether the imported cases were in the indigenous population whom had travelled abroad and returned infected. Thus, these studies did not provide meaningful information on the burden of disease among migrant populations.
One of the largest studies using surveillance data illustrates these difficulties. It used national data from 32 European countries from 2006–2007, covering a total of 12,132 reported cases of measles, of which 210 (1.7% ) were reported as ‘imported’, 117 (56%) of which were from another European country, and 43 (20%) of which were from Asia [20] . The study provided little information specifically on migrant populations; it merely noted the presence of measles outbreaks in 2005–2009 among certain indigenous populations, such as the Roma and Sinti, Travellers, anthroposophic (a particular philosophical-spiritual community) and ultra-orthodox Jewish communities [20] .
There were similar problems with the case studies of measles outbreaks, many of which discuss ethnic minorities, but do not specify whether these include recent migrants or not. Thus, a report on an Irish measles outbreak in 2009–2010 mentioned that two-thirds of the cases were in unvaccinated subjects, and that the majority of them were from the Traveller community, or “others from Eastern Europe” [21]. In France, an outbreak in 2008–2010 was reported to have particularly affected Roma and “gens du voyage” (nomadic populations) [22]. Yet, it was again unclear whether these were migrant populations, non-migrant itinerant groups, or both. Another epidemiological study on a 2008 measles outbreak in Germany reported that a new strain of measles virus (D4-Hamburg) was imported from London to Hamburg and then to Bulgaria, with the spread of the virus being predominantly associated with travel by the Roma individuals [23]. Additional information was provided in a report on a Greek measles outbreak in 2010, which highlighted the Roma communities as bearing a disproportionately high case load, noting that they came from both Greece and Bulgaria [24]. Similarly, two measles outbreaks in Lazio, Italy in 2006 and 2007 were noted as having disproportionately affected the Roma/Sinti community, with index cases identified as unvaccinated Roma/Sinti children of Romanian nationality[25]. One study that did identify cases in migrants reported that 8 of 10 measles cases in an outbreak in Oslo in 2011 were from the Somali immigrant community, with two cases in Norwegian children [26].
Immunization is key to the elimination of measles, yet outbreaks and fatalities continue in Europe because vaccination rates remain below the recommended coverage level of at least 95%, leaving pockets of vulnerable groups unprotected [27]. In some EU/EEA countries, these outbreaks have been linked to migrant populations with low or sub-optimum coverage [28]; however, as with incidence data, data on immunization rates in migrant populations is limited. In many EU/EEA countries, these data are not routinely collected [28]. Moreover, migrants may not be registered with a national health system. It is also necessary to place any data in a national context, with far lower immunization rates typically in Western than in Eastern Europe [29]; however, data on the determinants of non-immunization matter: most of the reported measles infections in Europe during 2005–2009 were in unvaccinated or previously uninfected individuals, with recent outbreaks concentrated in remaining pockets of susceptible individuals [20,30].
There are a few studies from individual countries on immunization rates in those persons explicitly identified as migrants by country of birth, often finding that they are less likely to be vaccinated against measles than their peers. One German study, using data from the representative German Health Interview and Examination Survey for Children and Adolescents, found that children who were foreign-born had a 3-fold higher risk of being unvaccinated [31,32]. Another analysis of the same data found that among vaccinated children, migrant status was associated with being more susceptible to measles [33]. An Italian study reports that children born outside of Italy, or whose parents were born outside Italy, had lower immunization rates than native children (89.6% versus 87.3%, respectively), although it was not stated if this difference was statistically significant [34]. A Spanish study found a statistically significant difference in immunization rates between indigenous and immigrant children, for both primary coverage (96.5% and 85% coverage, respectively) and the primary vaccination plus booster dose (88.6% and 78.3%, respectively) [35].
Other studies in Spain also report that immigrant children have lower vaccination rates [36]. The authors point to the need for better vaccination coverage, including among adults and those seeking work or visiting, whom may not come into contact with the health system [29,35,36]. One Belgian study that defines migrant status as having one or more parents or grandparents born abroad, rather than the country of birth of a case, found that there were lower coverage rates in both adolescents with a non-European background and in primary schoolchildren with a European, but non-Belgian background [37].
A major factor in the failure to achieve comparable immunization rates among migrant populations is their poor access to health services. Barriers to accessing health services include: cultural and linguistic barriers, socioeconomic exclusion and discrimination [20,38]. In many countries, ethnic minority children and children in socioeconomically disadvantaged families (both of which might include migrants) are less likely to be immunized [29]. Having parents who do not speak the local language is another risk factor for low vaccination coverage among children [39,40].
A meeting of experts
A number of reasons for measles outbreaks in EU/EEA member states were presented at the infectious disease and migration expert meeting. Outbreaks were generally linked to low vaccination coverage in Roma communities or particular religious groups, such as Orthodox Jews, and were infrequently linked with migrants.
Reasons for measles outbreaks vary between countries, but they do not often correlate to migration. These can include:
Anthroposophic objectors (Steiner groups) (Germany)
Religious groups (Netherlands)
Low vaccination coverage, possibly unvaccinated migrant groups (France)
Autism scare (UK)
Roma minorities (Romania, Bulgaria and Balkan states)
Death after vaccination that was unrelated to vaccine: Vaccination hype (Ukraine)
Decentralized surveillance (Switzerland)
Low political support (Austria)
Orthodox Jewish communities (Belgium)
Anti-vaccination movements and low support among medical personnel (EU-wide)
Survey of EU/EEA member states
Of the 30 countries surveyed, 22 returned the questionnaire on measles and rubella. There were 13 countries that reported that they had collected information on the migrant status of measles cases, using the criterion of ‘country of birth’. Only Greece and Spain reported that tourists or visitors were excluded from their ‘migrant’ category.
Within the 13 countries that collected information on the migrant status of measles cases, 72 of 909 (7.92%) reported measles cases in 2010 were in migrants. By comparison, the total foreign-born population in these 13 countries in 2010 was 9.8%, as shown in Table I [41] .
Foreign-born population in surveyed countries, 2010.
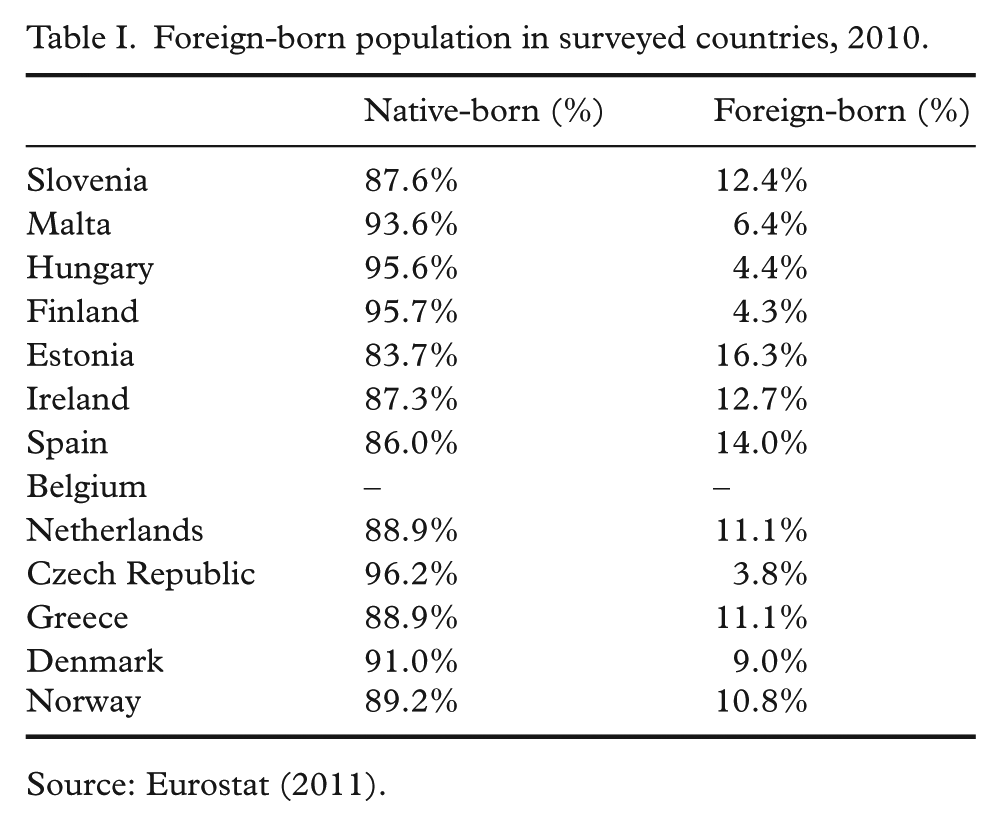
Source: Eurostat (2011).
Overall, in the period 2007–2010, 142 out of 1995 (7.12%) measles cases in these countries occurred among migrants (Figure 1). There was wide variation between countries, with no cases reported in migrants in Slovenia, Malta, Hungary, Finland and Estonia, but 25.5% of cases reported in migrants in Greece and 75.9% of cases reported in migrants in Norway. Out of 13 countries, only three (Greece, the Netherlands and Norway) reported the vaccination status of measles cases in their responses to the survey, with only the Netherlands and Norway reporting vaccination coverage for migrants. In the Netherlands, none of the 28 measles cases reported in migrants from 2007–2010 had been vaccinated. In Norway, vaccination coverage was marginally higher, with two out of 22 measles cases (9%) in migrants from 2007–2010 being reported as having been vaccinated.
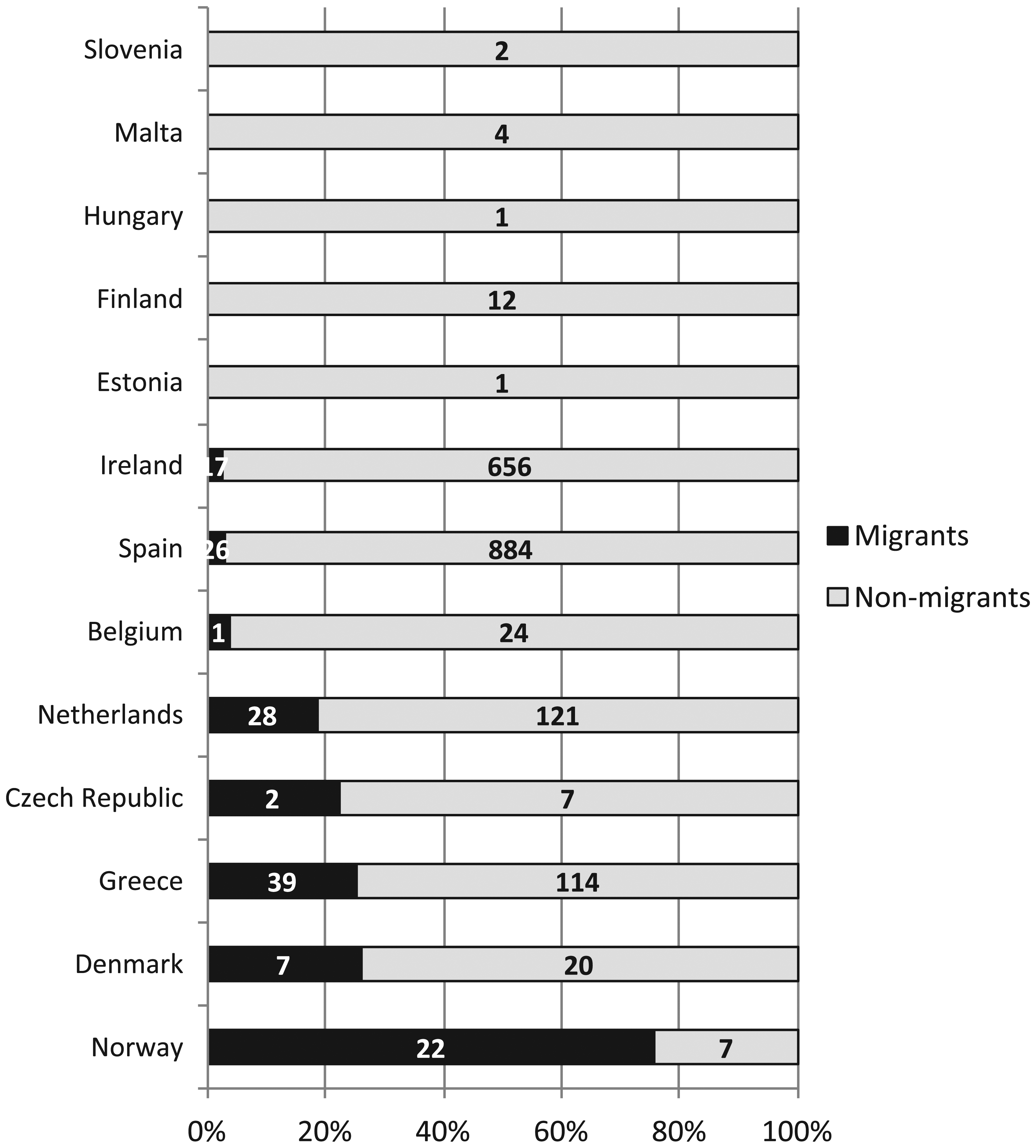
Migrant status of measles cases in 2007–2010, using the country of birth variable.a
When asked whether data for migrants were subject to any significant biases and/or inadequacies (e.g. incompleteness of data or inaccuracy of diagnoses), respondents from three countries (Czech Republic, Denmark and Spain) reported that there were no biases. In Belgium, the data on measles were limited to the Flemish community. Incompleteness of data was also noted by other national focal points. In Ireland, it was reported that information on the country of birth was only available for 18% of those with measles cases in 2007–2010. Potential data incompleteness as a result of migrants not seeking health care was mentioned by key informants in Greece, Malta and Slovenia. Finally, incompleteness of information on the vaccination status of migrants was mentioned by the respondents from the Netherlands and Norway.
Limitations
This study inevitably has some limitations. We included only papers published in English, which may have limited the number of studies included from EU/EEA member states that do not routinely publish in English. It should also be noted that the opinions provided for some questions in the country survey and at the Lisbon meeting may be subject to biases, as they reflect the views of a limited number of measles experts.
Discussion
There is little information available on the occurrence of measles among migrants in Europe. Although national surveillance systems for measles are in place and regular reporting occurs, surveillance is incomplete in relation to migrant health. As noted, routine national surveillance data, as reported to the ECDC, do not record migrant-specific information such as country of birth, but rather record the importation status of cases, which are classified as ‘imported’, ‘endemic’, ‘import-related’ or as being of ‘unknown’ origin. This variable is not an optimal proxy for migration, but rather indicates travelling in the days before disease onset. Our literature review identified few studies that assessed measles among the migrant populations, with the literature instead focused on specific minorities at risk of measles, such as the Roma, Traveller, anthroposophic and ultra-orthodox Jewish communities.
Despite these limitations, this study revealed important findings in relation to measles in migrant populations. Several studies did conclude that some measles outbreaks were linked to sub-optimal vaccination coverage in migrant populations, with migrant children being less likely to be vaccinated than their native counterparts [28,31,36,42]. Furthermore, a number of respondents to the member state survey noted that the potential data incompleteness on measles cases and the vaccination status as a result of migrants not seeking health care was an issue of concern. The limited access of undocumented migrants to health care services is another area of concern that is emerging from the literature [43,44].
The survey of member states provided important additional information on measles in migrant populations, with 13 countries reporting information based on the ‘country of birth’ variable. In these 13 countries, migrants accounted for 7.1% of the measles cases in 2007–2010; however, there are widespread differences in reporting between countries, with some, such as Slovenia, Malta, Hungary, Finland and Estonia reporting no cases in migrants in 2010, but Greece and Norway 25.5% and 75.9% of their cases being in migrants, respectively.
The varying patterns of measles in migrant populations in different countries makes it essential that, even if measles is not a particular problem in their migrant communities now, all countries undertake routine surveillance of migrant-specific variables for measles cases to ensure that policy responses can be tailored to emerging developments in individual member states. In particular, surveillance systems should be strengthened to routinely capture migrant-specific variables for measles cases and for MMR vaccination rates. These data can help inform the provision of preventive services, which may need to reach out to vulnerable migrant populations that currently face barriers in accessing routine immunization and health services [27,45]; however, it will be important to think carefully about how to do this, to ensure that the rationale for doing so and the methods used are accepted by migrant communities, some of whom may be concerned about interactions with statutory authorities. This may be mitigated by recruitment of community and health workers from migrant groups [46], and by policies that take advantage of research from other areas of health policy that highlight the need to take full account of the legal and cultural issues pertaining to each country, including the entitlement to health care and the levels of racism and xenophobia [47,48].
Finally, it is important to note that these figures do not support the view that migrants overall have a higher burden of measles, contrary to perceptions that are widespread in some quarters. Indeed, a greater challenge in achieving measles elimination may well be the indigenous communities, who, for whatever reason, have longstanding objections to the concept of immunization [49,50].
Footnotes
Acknowledgements
The authors are grateful for the advice received on this article from: Pierluigi Lopalco, Marta Busana and Lucia Pastore Celentano.
Conflict of interest
The authors declare that there are no conflicts of interest.
Funding statement
This work was supported by the European Centre for Disease Prevention and Control (ECDC).