
Abstract
To arrest the spread of COVID-19 infection, strict adherence to frequent hand washing and respiratory hygiene protocols have been recommended. While these measures involve private effort, they provide health gains along with collective community benefits and hence are likely to be driven by pro-social motives like altruism and reciprocity. Using data from 934 respondents collected from April till May 2020 across India, we assess if changes in perceived community compliance can predict changes in individual compliance behaviour. We observe statistically significant and positive relationship between the two, even after accounting for observable and omitted variable bias allowing us to view the results from a plausible causal lens. Further, we find subsequent lockdowns having a detrimental effect on individual compliance though the gains from higher perceived community compliance seem to offset this loss. We also find positive perceptions about community can be particularly effective for people with pre-existing co-morbidities. Our findings underscore the need for multi-level behavioural interventions involving local actors and community institutions to sustain private compliance during the pandemic. We suggest these interventions need to be specially targeted for individuals with chronic ailments and emphasize on community behavioural practices in public messaging.
Introduction
The novel coronavirus (COVID-19) pandemic has spread globally claiming close to two million lives across the world. In the initial phase when vaccine research was at the nascent stage, Non-Pharmaceutical Interventions (NPI) like social distancing and wearing mask were recommended as protective measures to reduce infection spread. Currently, though COVID-19 vaccines are being administered, infection spread continues to remain a potent threat especially as the virus is mutating into newer strain with higher infectivity. 1 Over time as deterrence measures like lockdown are loosened, increasing mobility is observed along with frequent non-adherence of the compliance protocols. In the backdrop of increasing human interactions and limited evidence on vaccine effectiveness as opposed to efficacy 2 stricter adherence to social distancing measures, if not less, continues to impress itself as a crucial pandemic management strategy. In particular, as individuals with pre-existing disease conditions are found to be more susceptible to COVID infection, promoting NPI on a long-term basis remains an important health policy agenda for restricting virus incidence. Past experiences on health interventions have shown that preventive health behaviour is responsive to social contacts (Centola, 2011) and individual actions are often anchored to the high prevalence behaviour (Rimal & Real, 2003). In this article, we study individual compliance levels and examine the implications of perception about community compliance on adherence of the COVID protocols. In the process, our work also allows us to study the factors that sustain the compliance behaviour over time as well as encourage the co-morbid individuals to follow them.
Theoretically, one major driver for individual compliance efforts would be to ensure better health and avoid the possibility of getting infected. The other driver that confers collective benefits, stems from moral motivation to protect others. Variants of moral motivation like pure altruism (Andreoni, 1988, 1989) and improved self-image (Brekke et al., 2003) have been used to explain voluntary contribution in public good contexts (Chorus, 2015). In this strand of literature, individual adherence to pro-social behaviour occurs because a positive utility is derived from matching actions that are considered ideal. In fact, studies have argued how individual behaviour are often driven by norms, social expectations and first order beliefs about whether her community follows a particular behaviour (Bicchieri, 2017; Cialdini & Goldstein, 2004; Lyon, 2000). In the context of disease outbreaks like COVID-19 there is a possibility that abidance to the compliance protocols might be motivated by such pro-social concerns.
On the other hand, economic incentives often interact with moral incentive such that collective behaviour may impose a decision externality on private action (Collier & Venables, 2014). Better community preparedness that poses lesser chances of infection may induce individuals to reduce her preventive efforts. Thus, the net effect of community compliance level on individual action is ambiguous. Moreover, government reliance on lockdowns may intensify economic hardship, which could weaken the community ties that motivates compliance. In this article, we use self-reported data collected from 934 respondents across India during the lockdown period till May, 2020 to assess if positive perception about community compliance behaviour can encourage higher levels of individual compliance of the preventive measures.
Individual compliance efforts involve positive externality in that it reduces the infection potential for others besides self-protection. Although adherence to COVID-19 protocols confers collective benefits, there are associated private costs such as limiting work time, or poorer wellbeing due to social isolation and consequent disruption of livelihood (Ahmed et al., 2020; Lancet, 2020). As a result, voluntary compliance effort might fall short of the optimum over time. Indeed, studies have documented that individual compliance might be inversely related with the duration of social distancing measures (Briscese et al., 2020; Moraes, 2020). In developing countries, with deeper economic inequality and lack of awareness, the gaps in preventive effort are likely to be even higher. Moreover, ‘vaccine optimism’ might induce people to drop their guards if there is reduction in perceived risk in anticipation of vaccine arrival (Andersson et al., 2020).
Besides increasing health risk in general, laxity in social distancing is more likely to have adverse effect on individuals with pre-existing disease conditions like hypertension and elevated blood sugar levels (Singh et al., 2021). 3 Those with co-morbidities would have higher expected health cost from infection but the effort cost of compliance over time might also outweigh the perceived health gain. The fatigue effect, in already sick patients could significantly demotivate compliance. Antecedents of such non-complying behaviour can be found in studies documenting the discontinuation of long-term therapy among majority of the patients suffering from chronic illness (Horne et al., 2013; Munro et al., 2007). Understanding how people with different health endowments respond to compliance guidelines might provide important insights into sustenance of preventive behaviour. Our article allows us to examine the changes in compliance behaviour over the subsequent lockdowns implemented after the outbreak and assess the implications of better perceived community compliance with time. Since individuals with chronic co-morbidities are more susceptible to serious illness, we further assess its implications over these set of individuals as well. A mathematical exposition of the framework along with an example with an appropriate functional form is given in Appendices A and B.
The findings from the article indicate a statistically significant, robust and positive relationship between perceived community compliance and individual compliance levels. Notably, these positive relationships hold even after accounting for the potential unobservable that include strategies developed by Altonji et al. (2005) and Oster (2019) indicate that our findings might be viewed through the causal lens though concerns about reverse causality remain. We also find compliance for co-morbid respondents to increase systematically with higher levels of perceived community compliance. Interestingly we find a significant decline in compliance levels with subsequent lockdowns but the gains through higher community compliance seems to offset this loss. Given this evidence, we propose a set of recommendations that can increase adoption of preventative measures to curb COVID-19 transmission. Among others, we propose behavioural interventions and outreach programmes through active local community institutions that makes community compliance visible and salient among its members. Further underestimation of the actual community compliance can be corrected since it can reinforce positive norms.
The structure of the article is as follows. The second section gives a brief overview of the situation pertaining to COVID-19 in India. The third section presents a theoretical framework and the fourth section discusses the data and the variables included in our analysis. The fifth section reports the results while the associated discussions are presented in the sixth section. A brief conclusion is provided in the seventh section.
COVID-19 in India
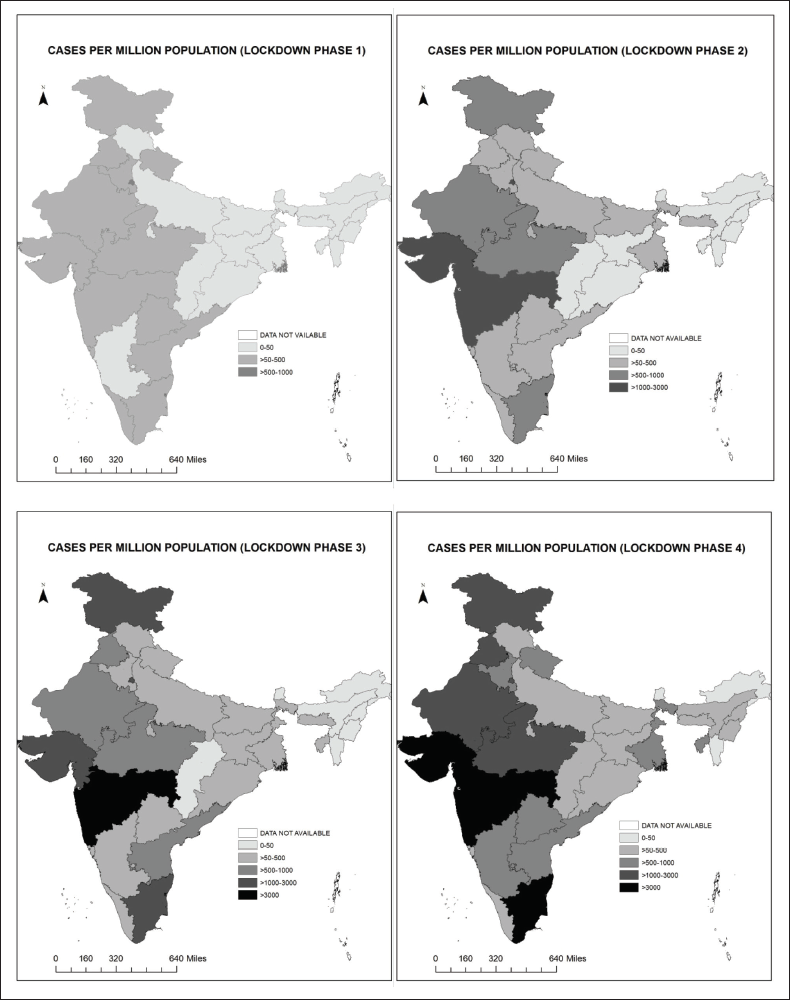
In this article, we study India, which remains among the most affected countries in the world. Currently (31-August-21), close to 33 million infected cases have been reported with a death toll of close to 440,000 individuals. As a preventive measure, the government had ordered a nationwide massive lockdown in four phases as follows: Phase 1: March 24 to April 14; Phase 2: April 15 to May 3; Phase 3: May 4 to May 17 and Phase 4: May 18 till May 31. In all these phases, India imposed the strictest lockdown rules curbing individual movements for non-essential purpose, mandating facemasks and allowing no social gatherings. Despite this we find a substantial increase in the number of infection cases over these four lockdowns (Figure 1). Notably, the economic loss during this period was substantial as India recorded a slump by about –23.9 per cent (year-on-year) in the quarter of April to June, 2020. Studies have documented the huge economic disruptions among different section in the economy in India (Ceballos et al., 2020; Kumar et al., 2020). In addition, the incidence of COVID fatality has been disproportionately higher among co-morbid individuals particularly for the elderly people in India. As per recent figures in the age group of 60 years and above, the case fatality rate for people with and without co-morbidities is 24.6 per cent and 4.8 per cent, respectively, while the country average for the two groups stands at 17.9 per cent and 1.2 per cent, respectively. Accordingly understanding the health seeking behaviour of the individual in the background of economic downturn and infection fatality becomes important as the infection rate is projected to increase in the coming period.
Conceptual Framework
Consider a society with N individuals and the utility function of individual, i is given by

Here x is the consumption of private goods h denotes the health status and I is the measure of individual’s self-image. We assume that the utility function is continuous and strictly quasi-concave. We suppose further that the health stock of the individual depends on his compliance level, c,say that is given by the amount of time, she distances herself from the society and/or the amount of time that she engages in protective activities like wearing mask and hand washing among others. However, private health stock would also depend on the extent to which community in his neighbourhood follows the health norm. Given the infectious nature of the COVID-19, we presume community behaviour would have an impact upon individual health through contagion dynamics. For simplicity, we assume that the individual interacts only within her own neighbourhood, which, given the extended lockdown period and high neighbourhood interaction, seems plausible in the Indian context. Let the perception about community health norm be given as

Thus, health is a concave function of individual compliance.
A growing strand of literature has examined the relation between social capital and pro-social behaviour. For instance, analysing the waste disposal behaviour of households in United States, Videras et al. (2012) find that higher recycling is driven by intensity of social ties and pro-environmental community norms. In their review of social capital and well-being, Helliwell et al. (2017) note that collective nature of social capital in the form of community connections can induce pro-social behaviour. In fact, personal identity via social capital can form the basis of reciprocal behaviour. Thus, individuals are more prone to give or receive support from those who they perceive to share the same social identity (Levine et al., 2002). In particular positive social identities are seen to be associated with better health status (Haslam et al., 2008).
The other role that community compliance has is through its moral appeal. We assume that individual converge to behavioural conformity by attempting to adopt the community level compliance. In the literature such pro-social moves have been modelled as one emanating from stigma from not following socially prescribed action (Akerlof & Kranton, 2000; Brekke et al., 2003) or individual might want to do what the others are doing in order to signal themselves as desirable social types (Bernheim, 1994; Bigenho & Martinez, 2019). Following these literature works, we assume that the representative individual would attempt to bolster his self-image by following the compliance behaviour of the community.
Accordingly, we define the self-image function as follows:

as in Brekke et al. (2003). The function is concave in c, I is increasing if
The time constraint of each individual is as follows:

Where l is the time allocated for work. Assuming that hourly wage rate is w we can replace x = w (T – c) in the utility function, that is x is the numeraire good. The individual maximizes (1) subject to his health production function, self-image function and time constraint in (2) to (4). The first-order condition gives the following:

Equation (5) defines the relation between c and
Data, Variables and Estimation
Data
The data used in the article is obtained from an online survey of 934 respondents across India from April 27 to May 31, 2020 mainly through snowball sampling. Since this survey was conducted during the lockdown face to face interviews or even phone call interviews could not be conducted in absence of a representative set of phone numbers. The survey was distributed via online platforms like the WhatsApp, Facebook and Twitter among others.
The survey was administered in four main languages: Bengali, Hindi, English and Tamil and hence our survey has majority of the respondents from West Bengal, Tamil Nadu and parts of the Hindi speaking belt that includes the Northern India. The questionnaire form was administered in Google form. Research assistants who were native speakers of these languages pretested the questionnaires. Suggestions to improve comprehension and flow of the survey were incorporated. We used several channels of distribution to ensure variation in our sample with respect education, occupation, age and gender. This study was approved by the Institutional Review Board at the University of Pennsylvania (Protocol No.: 843016).
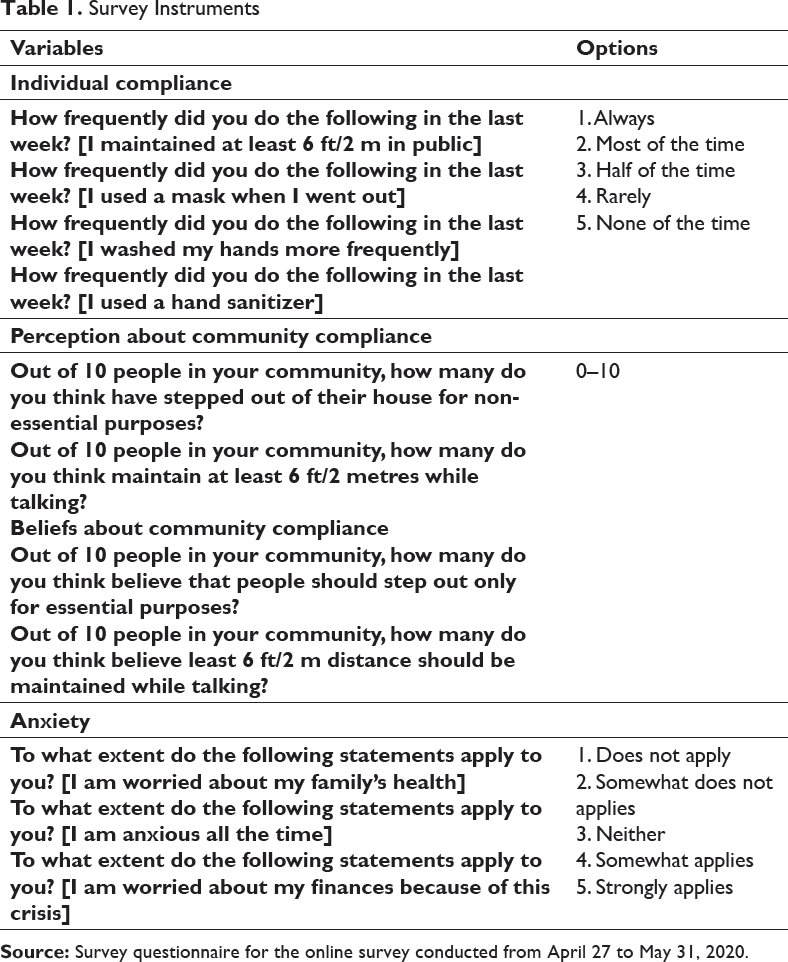
Survey Instruments
Variables and Estimation
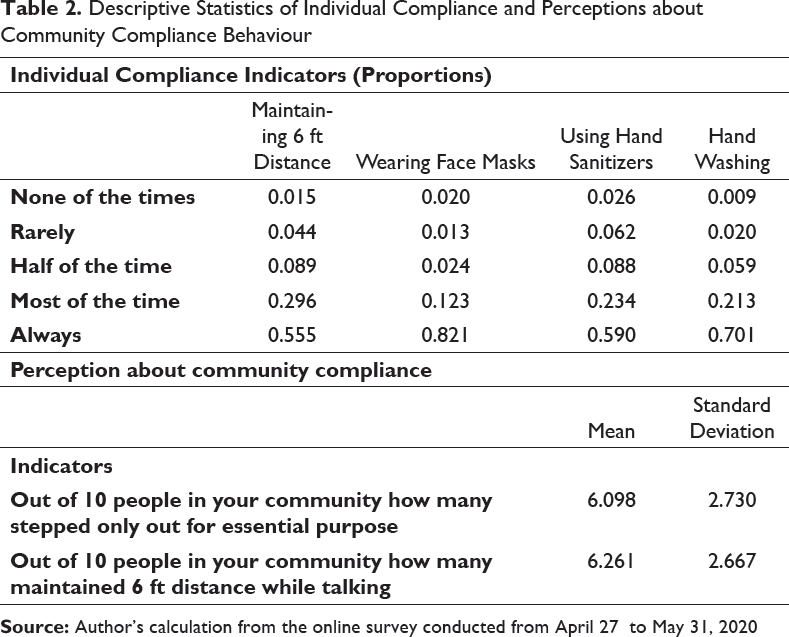
We use the first two indicators related to stepping outside for non-essential purpose and maintaining 6 ft distance while interacting with others for calculating the perception about community compliance. We left out the third indicator pertaining to hand washing since this behaviour about the others in the community is not observable for the respondents. We standardized these variables and use that to calculate perception about community compliance. Our dependent variable is individual level compliance, which is calculated by standardizing the four protocol adherence variables that we mentioned. We use Ordinary Least Squares (OLS) to regress the individual level compliance score on the perception about community compliance scores controlling for the potential confounders. The list of confounders and the associated variable construction are given in Table A1.
Results
Descriptive Statistics
Descriptive Statistics of Individual Compliance and Perceptions about Community Compliance Behaviour
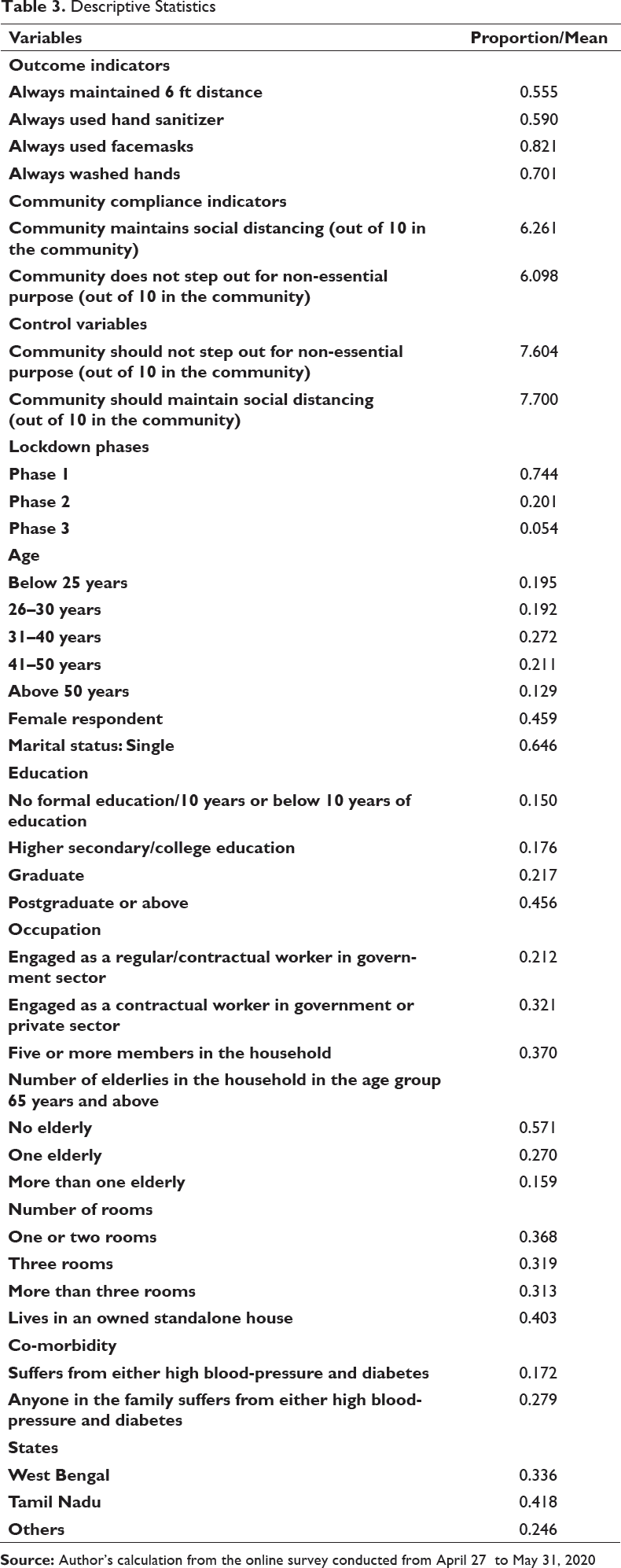
Descriptive Statistics
Regression Results
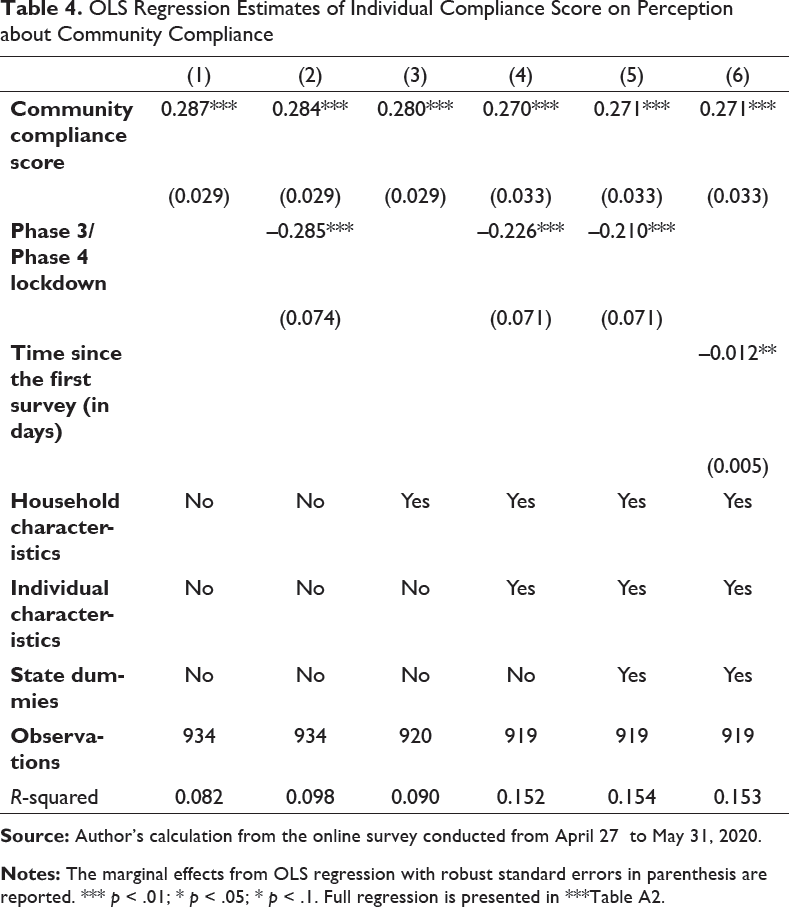
First, we examine the relationship between the standardized individual compliance score and the perception about community compliance scores. Table 4 presents the regression results. We sequentially introduce different groups of covariates to confirm if the marginal effects of the community compliance remain stable with increasing explanatory power of the model. In the first specification, only the community compliance scores are incorporated in the model and in the second model, the lockdown dummy is included. In the next specifications, the household characteristics and then individual characteristics are included along with the lockdown dummy (a dummy to indicate Phase 3 and Phase 4 lockdown). In the final preferred specification, we put all the controls together with the state fixed effects (West Bengal, Tamil Nadu and others). Importantly, we have controlled for perception about community beliefs about the compliance protocols, which would control for any systematic bias that the respondent may have about the community. The findings indicate that the community compliance scores, in all the specification are statistically significant at 1 per cent level. Notably, the effect size does not alter across specifications as we find one standard deviation increase in perception about community compliance abidance is associated with about 0.27–0.29 standard deviation increase in private compliance.
OLS Regression Estimates of Individual Compliance Score on Perception about Community Compliance
Even though the marginal effects of community compliance remain largely stable in all the specifications, endogeneity from omitted variable bias (OVB) and reverse causality remains a concern that prevents us from interpreting these results from the causal lens. With respect to OVB, there might be other unobservable factors correlated with community level compliance as well as his/her own abidance that we did not account for. With respect to reverse causation, existing literature indicates that high association of bias in prevalence perception with one’s own personal behaviour. In particular, it found that people tend to perceive that their own behaviour to be more common in the community than it actually is, often called the ‘false consensus effect’ (Kuang et al., 2020; Ross et al., 1977). Therefore, because of the potential OVB and reverse causation, we may not be able to say higher community compliance is causally related to better abidance of the compliance protocols.
Accounting for Omitted Variable Bias (OVB)
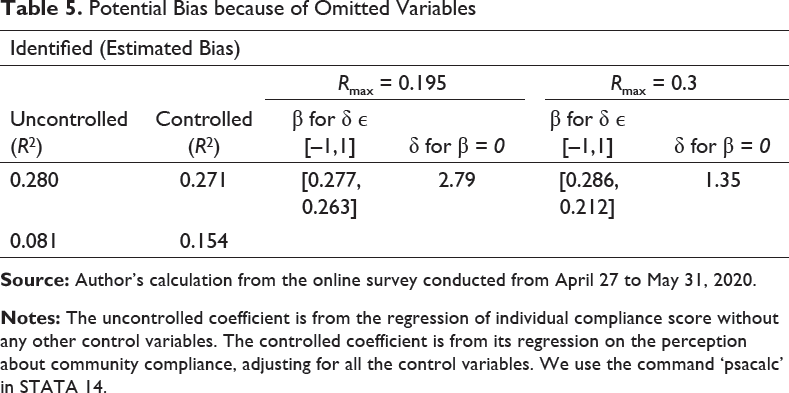
To assess the potential changes in the coefficients after accounting for OVB, we use a strategy developed by Oster (2019) based on Altonji et al. (2005), based on the assumption that selection on unobservable variables can be gauged by the extent of selection on observables. For further elaboration, we consider the following regression equation:

Here, Y is the outcome variable, Z is the primary variable of interest, X is the vector of observable controls and U is the set of all unobserved components. If U is substantially high, our aim is to examine the corresponding changes in β. Here the primary assumption is as follows:
Potential Bias because of Omitted Variables
Robustness Checks
Further, we apply other robustness checks as well to ensure that the relationship is robust and do not get alter with changes in specification, methods or the formulation of the dependent and independent variable. These are as follows:
Individual compliance protocols: We examine the relationship between abidance of the compliance protocol indicators separately with perception about community compliance for each the two protocol indicators we consider through a probit regression. The findings indicate positive relationship for most of these compliance indicators signifying that our results are robust (Table A3). With sub-samples: Since most of the responses were from the states of West Bengal and Tamil Nadu, we ran the same regressions with respondents only from these two states. In a separate exercise, because majority of our respondents came from the bigger cities, we also run the same regressions separately for respondents from only the six biggest cities of India: New Delhi, Mumbai, Kolkata, Chennai, Hyderabad and Bangalore. In these regressions, we incorporate city level fixed effects that would control for city specific observables that include deaths, number of tests and administrative efforts among others that may be correlated with compliance protocol abidance. The inference from the regressions is qualitatively similar to what we observed with the full sample (Table A4). Falsification tests: For falsification test, we replace the outcome variable with a non-equivalent variable that is not expected to change in response to changes in the treatment. After the outbreak of the pandemic, because of the sudden enforcement of the lockdown, there has been a mass exodus of migrant labourers from the cities to the villages leaving them starved and a number of deaths have been reported from across the country (Lancet, 2020). Accordingly, in our survey, we collect information on satisfaction about government measures taken on distribution of food ration to the poor and dealing with the internal migrant crisis that the country faced with the lockdown. Since these variables are views on government actions which are not related to compliance or even COVID protocol awareness, they are unlikely to be related to the respondent’s perception about community compliance. This is indeed found to be the case as we observe the coefficient of community compliance score is statistically indistinguishable from zero (Table A5).
Relationship with Lockdown and Health Conditions
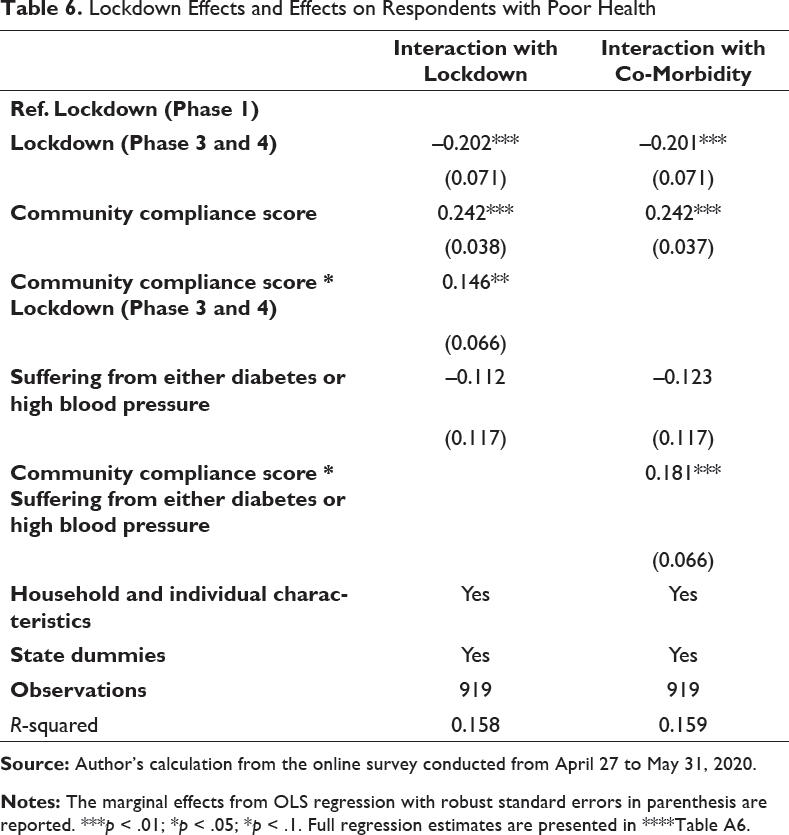
In the first part of the analysis, we find the lockdown (Phase 3 and 4) dummy is found to be negatively associated with individual compliance. Can higher perception about community compliance offset this decline in compliance over time? To answer this, we introduce an interaction of the community compliance variable and the lockdown dummy in the regression model and study the estimations (Table 4). We observe that the marginal effect of this interaction term to be positive implying an overtime increase in the potential effect of the respondent’s perception about community compliance on her own compliance behaviour. Hence, individual compliance which can potentially decline over time because of fatigue and economic conditions, enhancing perception on community level compliance can have a positive effect.
Studies have indicated individual with pre-existing chronic conditions like diabetes and high blood pressure have higher health risks (Fang et al., 2020; Klonoff & Umpierrez, 2020). Despite this, our regression results seem to indicate respondents with co-morbidities do not have significantly higher compliance (Table 6). Accordingly, we assess the heterogeneous effects of community compliance with individual compliance among these respondents (Table 4). The findings indicate that the community compliance is positively related and, statistically significant at 5 per cent level.
Lockdown Effects and Effects on Respondents with Poor Health
Discussion and Policy Implications
The main finding of the article underscores that positive perceptions regarding community behaviour can encourage individual COVID-19 compliance protocols. Additionally, affirmative perceptions regarding community are seen to sustain private compliance effort over time even with a potential fatigue effect and mobility restrictions that pose binding constraints on the income earning ability in general. Our work thus reaffirms the importance of social beliefs and norms on individual health focused behaviour that literature has often focused on (Bicchieri, 2017; Cialdini & Goldstein, 2004; Van Bavel et al., 2020). Notably, literature on Ebola epidemics and even non-contagious ailments like HIV/AIDS that documents outreach interventions facilitated through local community organizations led to increased awareness, contained the spread of the virus and lowered stigma (Abramowitz et al., 2015; Gregson et al., 2013; Pronyk et al., 2016). Community focused measures were recommended in other studies that have highlighted the role of norms in collectivistic cultures in predicting SARS-preventive behaviours (Cheng & Ng, 2006). Our findings also exhibit stronger ties with the literature that links pro-social behaviour with descriptive or provincial norms (Goldstein et al., 2008; Yoeli et al., 2013). Even in the COVID context a study from Japan revealed that in adhering to compliance activities like wearing mask people are most likely to do what others around him are doing (Nakayachi et al., 2020).
The underlying implication of our results highlights the need for behavioural change interventions that use influential individuals from the local community to exert social pressure or incentives to sustain compliance. Social distancing measures and wearing masks are positive behaviours that should be made visible and salient so that it can stabilize a norm through visual cues. In this context, social media platforms can be used to engage peers and broadcast the use of masks and safety measures. If more people see their neighbours in their community wear masks and talk about staying at home during the pandemic, it might increase one’s willingness to do the same. Such community level interventions may be more cost effective compared to individual level monitoring and vigilance and also less likely to raise mistrust and antagonism against the implementing authorities.
Importantly, our findings also signify the effectiveness of sensitization through community especially for individuals with pre-existing co-morbidities. As COVID infection propensity and mortality are known to be higher among people with co-morbidities (Ejaz et al., 2020) community-based interventions, in the light of our result, can be useful in reducing the fatality rate. Hence, such interventions should be targeted more in the local public health centres or hospitals or even medicine shops where the likelihood of the co-morbid individuals visiting remains higher. Focused interventions related to community compliance through posters or periodic announcements in these places can be a good way to reinforce these motivations. While our article identifies the significance of community interventions, it must be noted the design of such programs are largely contextual and constitutes an important future research agenda.
Along with these interventions that raise perception about community, targeted educational and communication messages that periodically stress the need to sustain respiratory hygiene and pandemic protocols should be clearly stated (Bennett et al., 2015). For longer term benefits, stronger institutions and policies that promote harmony and cooperation among the community members becomes pertinent. This becomes especially important in urban areas where community ties are relatively weaker. Further because our empirical assessment reveals that subsequent lockdown has reduced private compliance, imposing mobility restrictions that impede community interactions can potentially constrain individual compliance. While gauging the impact of deterrence measures like lockdowns on enhancing compliance and comparing that with other government measures is beyond the scope of the article, we note that as a policy tool, lockdown may not serve to propagate voluntary protection effort and might even dampen it.
The findings should be interpreted with certain caveats and limitations. First, without exogenous variation in community compliance, we are unable to view the relationship between individual abidance of protocols and perception about community compliance from the causal lens. Though we account for the potential OVB, concerns about reverse causation remain valid. Secondly, snowball sampling and usage of social platforms raise concerns regarding the representativeness of the sample particularly if sections of the populations without smart phones are systematically excluded from the sample. Therefore, the inferences from the regressions are not externally valid, which opens up space for further research using representative data. Further, self-reported data on compliance, might also be associated with substantial upward bias. Nevertheless, given unprecedented nature of the outbreak and subsequent lockdowns, we feel these findings provide insight on an importance issue regarding compliance.
Conclusion
This article examines the relationship between perceived community compliance and individual abidance to the COVID-19 compliance protocols. We find that community influence reinforcing individual compliance in data collected across India from April to May, 2020 during the lockdown. The heterogeneous effects indicate higher effects of the community over time and also on individuals with co-morbidities.
Our work underscores the importance of community behaviour in persuading people to engage in those protocols which are beneficial for society. Some of the compliance activities are also difficult to monitor and thus, imposing penalties or sanctions for partially observable compliance behaviour, may not guarantee best outcomes particularly if violation of COVID-19 related norm can take place in the private domain. With the NPIs becoming essential for arresting the growth in infection, our research tends to show that when others in the community engage in pro-social behaviour, individuals are more likely to do so. This is in line with other research that shows motivation for compliance behaviours are pro-social, and can be driven by multiple social motives such as, social norms, reciprocity, cooperation and social learning (Batson & Powell, 2003; Dovidio et al., 2017; Nguyen et al., 2018; Rand et al., 2014). Importantly, the findings complement other studies on COVID-19 (Bicchieri et al., 2020; Nakayachi et al., 2020). Further, experimental studies in other contexts have indicated that perception about community behaviour influences one’s own behaviour. For example, Goldstein et al. (2008) emphasized the impact of descriptive norms, by using messages broadcasting that majority of the hotel guests reused their towels to increase the likelihood of guests to do that same and engage in pro-environmental efforts. Accordingly, we argue similar norm centric messages can be utilized by the decentralized communities to increase adherence to COVID-19 protocols.
Based on these findings of the article, we highlight a number of policy recommendations based on using community networks to foster collective action that can raise compliance and arrest the growth of the infection. Apart from these policy implications, the article assumes contextual importance as India is currently among those countries with the highest number of new infection and deaths.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for Love Thy Neighbour? Perceived Community Abidance and Private Compliance to COVID-19 Norms in India by Upasak Das, Prasenjit Sarkhel and Sania Ashraf, in South Asia Economic Journal
Footnotes
Acknowledgements
The authors acknowledge the help received from Rajesh Kanna, Jeyaganesh, Sushmita Chakraborty and Aishmita Biswas for setting up the data collection process with the google forms, dissemination in the rural areas, cleaning the data and creating the maps. We are thankful to all the respondents for filling up the forms. We also acknowledge the comments received from the conference participants of the SANEM International Development Conference (SIDC) 2020 along with Sukanta Bhattacharya, Ritika Jain and Shreya Biswas.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no external funding. This study is approved by the Institutional Review Board at the University of Pennsylvania (Protocol No.: 843016).
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.