
Abstract
Background
Providing meaningful activities to persons living with Alzheimer's disease or other dementias in home settings is challenging because it typically involves the expense of professionals instructing the caregivers. Enhanced group activity kits (EGAKs) have been shown to enhance the wellbeing of persons living with dementia (PLwD) in group settings.
Objective
To investigate the feasibility and potential benefits of EGAKs in one-on-one settings without the expense of visiting professionals.
Methods
Recruitment started with 75 referrals, from nursing agencies, family caregivers’ support groups, a health services organization for older persons and their families, and an occupational therapists WhatsApp group, resulting in 34 family caregivers from greater Tel Aviv and Jerusalem metropolitans, Israel, completing a baseline interview. From those who completed the baseline interview, 16 PLwD experienced EGAKs with facilitators (family members, formal caregivers, or friends). Facilitators completed EGAKs-related questionnaires and a post-EGAKs-use interview. This mixed methods study includes a quantitative analysis of the EGAKs’ facilitators’ perceptions of the extent of success and an inductive content analysis to identify EGAKs’ benefits and potential outcomes.
Results
For most PLwD, one-on-one EGAKs were perceived as successful, making PLwDs’ and facilitators’ shared time more interesting and enjoyable. Four EGAKs’ use benefits emerged: Affecting mood, feelings, and emotions; Affecting cognition and behavior; Shifts in perceptions; and improving communication and relationship between the PLwD and facilitators.
Conclusions
When used in a home setting, EGAKs are often feasible and are often perceived to increase PLwDs’ engagement in activities and improve their wellbeing.
Keywords
Introduction
Most persons living with dementia (PLwD) live at home, 1 and frequently experience loneliness.2,3 Boredom and the absence of engaging activities represent common challenges for both PLwD4,5 and their caregivers. Apathy in PLwD often manifests as difficulty initiating activities, and finding pursuits that sustain their interest. 6 A related challenge faced by family caregivers is the difficulty communicating with PLwD.7–10 These phenomena along with caregivers’ difficulties to meaningfully occupy PLwD have driven the development of targeted interventions.
Several interventions aimed to provide tailored activity programs to PLwD in their homes11–13 or to understand how family caregivers can promote PLwDs’ engagement with activities. 14 Most such studies involved a professional (often an occupational therapist) conducting multiple home sessions 15 and developing personalized activities for PLwD.12,16,17 Study objectives varied and included reducing behavioral and psychological symptoms of dementia, or improved quality of life for PLwD and caregivers.
Various studies reported significant reduction in psychological symptoms,12,16–18 usually through tailored activity programs, while other interventions such as Reality Orientation, 19 individual cognitive stimulation therapy20,21 or cognitive rehabilitation 22 did not achieve similar outcomes. Some studies demonstrated significant improvements in quality of life for the PLwD, 15 though others did not.12,18,20,21,23,24 While one intervention providing activities for PLwD 16 resulted in reduced family caregiver burden or distress, a Reality Orientation intervention showed no such reduction. 19
To summarize these findings, home-based activity interventions for PLwD demonstrate inconsistent outcomes and require substantial time and resources that many family caregivers cannot provide. Moreover, many family caregivers lack the necessary skills to engage PLwD in activities or develop meaningful programming. These limitations significantly hinder the implementation of such interventions in real-world settings. The challenge of developing meaningful activities extends beyond family caregivers to activity leaders in long-term-care facilities. Most group activities provided to PLwD in long-term-care settings fail to optimize participants’ potential because staff often lack the resources, knowledge, or time to prepare activities that maximize PLwDs’ engagement and mood. 25 Enhanced Group Activity Kits (EGAKs) were designed to tackle this challenge.
EGAKs were developed based on the following principles:
Dignity. PLwD's dignity is achieved by providing activities involving age-appropriate topics that respect personhood and offer opportunities for successful participation. Success is achieved by (1) utilizing procedural memory of over-learned skills like reading or speaking, which are often maintained until later stages of dementia, (2) incorporating topics that draw upon long-term memory, (3) asking error-free questions, and (4) adapting activity materials to compensate for cognitive and sensory deficits, through large-print, high-contrast booklets with pictures and materials accessible to multiple senses. Active engagement of PLwD is achieved through activity leaders who facilitate participation and encourage reading, singing, drawing, responding to questions, and social interaction. Utilizing retained skills is considered preventive of further decline.
The 47 EGAKs utilized in this study encompass nine activity categories: physical activity, reading, creative arts, art history, cognitive training, singing, travel around the world, Jewish texts, and miscellaneous activities. Each EGAK included all materials necessary to conduct the activity: guidance booklets for facilitators (containing suggested instructions and relevant background information, as facilitators were not expected to have prior subject matter knowledge), participant booklets, PowerPoint presentations, pictures, coloring templates, craft supplies, and other materials. The EGAKs were designed as ready-to-use resources.
Two prior studies have successfully utilized this approach. The first study, conducted in Canada, 26 included nine geriatric units: seven from a nursing home, one from a community adult day program, and one from an independent living facility. The second study, conducted in Israel, 27 included ten geriatric units: six residential nursing care units from five facilities and four senior day center units from three facilities.
Given the documented success of EGAKs in engaging PLwD and improving mood and general wellbeing in senior day centers and geriatric care units26–28 we examined EGAK implementation in home settings. Thus, this study explores the ways EGAKs contribute to PLwD and facilitators at home. EGAKs introduce activities and communication between facilitators, who may be family caregivers, friends, or paid caregivers, and PLwD on neutral topics, potentially enhancing engagement and fostering communication. No other studies have examined the use of activity kits with PLwD in home environments. We hypothesized that facilitators would find selected EGAKs feasible to implement with PLwD in home settings and would perceive the experience as contributing to both parties.
Methods
Ethics
The study was approved by the institutional review board of Tel Aviv University on May 23, 2022 and was conducted from July 2022 to November 2023. The initial screening was conducted via phone. Informed consent was obtained in one-on-one online meetings with the study staff from the PLwDs’ main family caregiver, even if the caregiver was not the EGAKs’ facilitator. Facilitators who were not family caregivers also gave their consent to participate in the study in personal online meetings with the study staff.
Recruitment
We approached nursing agencies, family caregivers support groups, an organization that provides health services for older persons and their families, and an occupational therapists WhatsApp group in the greater Tel-Aviv and Jerusalem metropolitan areas in Israel. Some recruitment involved snowballing.
Facilitators in this study were defined as family caregivers, friends or formal caregivers of PLwD who agreed to facilitate the EGAKs. For family caregivers and facilitators, inclusion criteria were being over 18 years of age; being a family caregiver/formal caregiver/friend of a community-dwelling PLwD; high proficiency in Hebrew (speaking, reading and writing); having a computer with internet access; and good computer-use skills.
For PLwD, inclusion criteria were age 65 or older with dementia or cognitive decline; able to use fine motor skills; no diagnosis of schizophrenia or bipolar disorder; adequate visual and auditory capacities to view text and pictures and to hear music.
We received contact information for 75 family caregivers (Figure 1 is a flow chart of the recruitment process). The main reasons for exclusion were:
Caregiver unavailability (n = 7); Caregiver without time to participate (n = 14); PLwD or caregiver refused (n = 3); Caregiver did not complete baseline information (n = 6). Total = 30. Poor health (n = 6), death prior to starting EGAKs’ use (n = 3), PLwDs’ or family caregivers’ functional/sensory limitation (n = 5). Total = 14. Caregiver/PLwD could not be reached or geographic distance: Total = 10. Caregiver without access to computer (n = 3); Caregiver without computer competence (n = 1). Total = 4. Prior participation in a study of EGAKs: Total = 1.
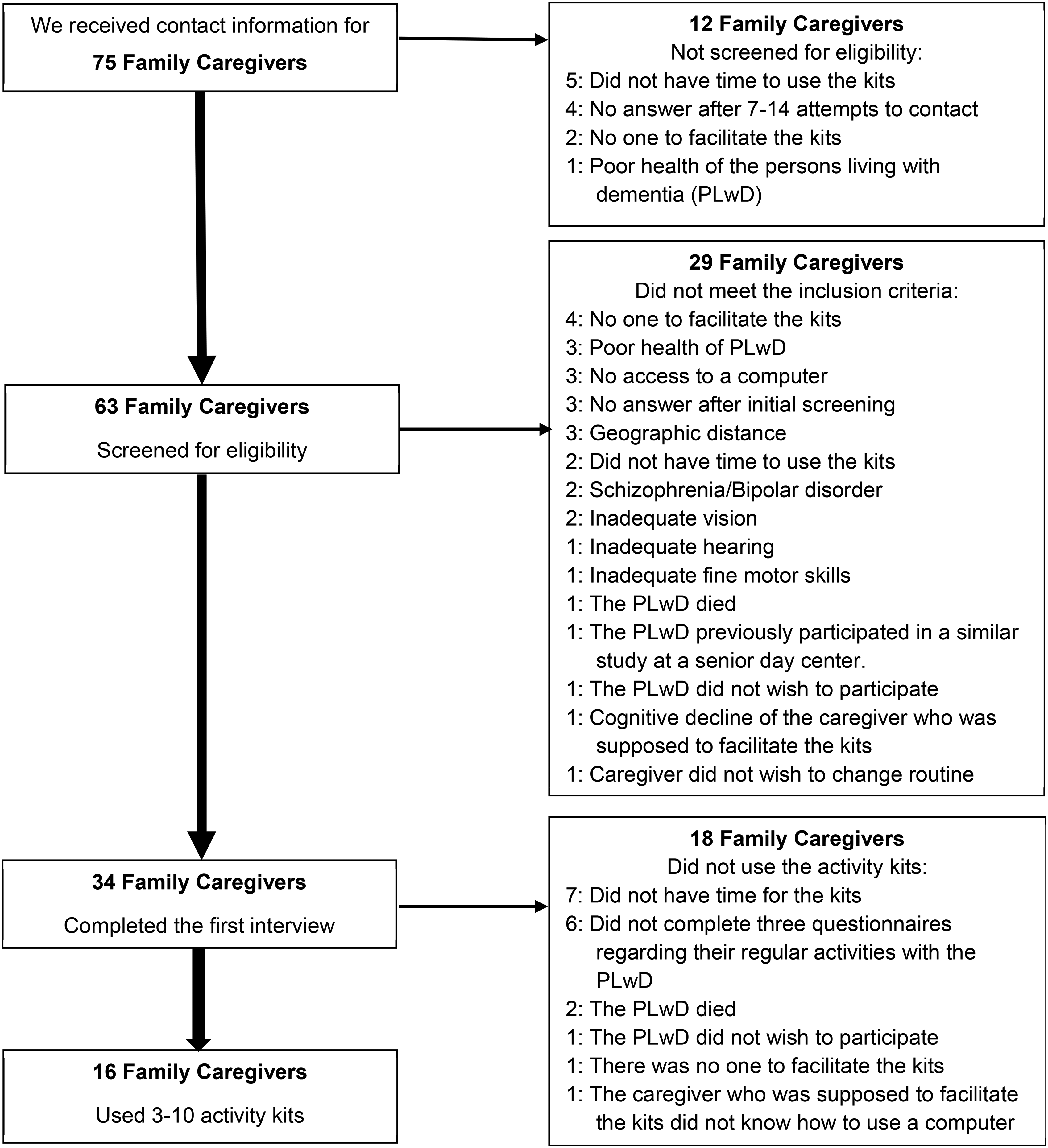
Recruitment flow. PLwD: Persons Living with Dementia. Nine family caregivers stated multiple reasons for not participating in the study. The figure states only the first reason given. The reasons beyond the first one included: No one to facilitate the kits (n = 4); No access to a computer (n = 2); Not having time to use the kits (n = 2); Inadequate vision (n = 1); Inadequate hearing (n = 1); Inadequate dexterity (n = 1); and poor health of PLwD (n = 1).
Procedure
Prior to the start of the study, we had adapted the EGAKs to be used in a one-on-one setting.
Thirty-four family caregivers of PLwD completed a baseline interview (1–2 h), of whom 16 used EGAKs and completed an additional EGAKs-related questionnaire and a post-EGAKs-use interview (50 min-1.5 h). A detailed description of the recruitment flow is presented in Figure 1.
A baseline interview was administered to family caregivers and designated EGAKs’ facilitators, during which interviewers presented all 47 EGAKs and assisted in selecting 10 EGAKs tailored to the PLwDs’ preferences. Subsequently, facilitators completed an online questionnaire concerning three pre-EGAK usual activities they conducted with the PLwD (e.g., talking, playing games, watching TV, eating, traveling outside, and cooking or baking). After receiving the responses, we sent the selected EGAKs to the facilitators.
Facilitators were asked to use the EGAKs at least once per week over a period of approximately three months. In practice, due to everyday life challenges (e.g., illness, doctor appointment, travel, etc.) usage varied with a median duration of 12.1 weeks (range: one week to 8.2 months). Among facilitators who used at least five EGAKs (n = 9), the median duration use was 15.1 weeks (range: 3.9 weeks to 8.2 months). Based on facilitators’ reports, the median length of each EGAK session was 40 min (range: 15–180 min).
The facilitators were requested to complete an online questionnaire after each activity they had with the EGAKs. In addition, we contacted facilitators at least once or twice monthly during the EGAKs-use stage to receive their feedback, provide additional mentorship, answer questions and remind facilitators to complete a questionnaire regarding each EGAK they used. Those conversations were transcribed verbatim. At the end of the period of EGAKs’ use, a post-EGAKs interview was conducted with facilitators. Personal interviews were conducted via Zoom by one or two of three trained interviewers (two with a PhD and one with a bachelor's degree). Facilitators’ answers were transcribed verbatim during the interview.
Assessments
All PLwD-related baseline questionnaires were completed by the family caregivers of the PLwD. Facilitators who were not family caregivers also completed the questionnaires except for information regarding the PLwD. The Baseline interview included a questionnaire concerning background information of facilitators and PLwD. Sociodemographic information concerning the facilitators included: relation to the PLwD, gender, age, marital status, and years of education. As for the PLwD, the questionnaire asked for age, gender, years of education, and whether there was a diagnosis of dementia (all types).
Family caregivers completed the Cognitive Performance Scale (CPS; 0 = ‘intact’ to 6 = ‘very severe impairment’) 29 to assess PLwDs’ cognitive status. The ability to perform activities of daily living (ADL) was calculated as the mean of four domains: dressing, eating, bathroom use, and hygiene (0 = ‘independence’ to 4 = ‘total dependence’). 30
Hearing and visual abilities
Hearing and vision were assessed by two questions from the minimum data set (MDS): hearing (with hearing appliance, if used) with the scale ranging from 0 = ‘hears adequately—normal talk, TV, phone’ to 3 = ‘highly impaired/absence of useful hearing’; vision (ability to see in adequate light and with glasses, if used), 0 = ‘adequate—sees fine details, including regular print in newspapers/books’ to 4 = ‘severely impaired—no vision or sees only light, colors or shapes, eyes do not appear to follow objects.’
Measurement of success
The extent of the EGAKs’ success was measured during the final interview with the facilitators after they fully or partially completed their use of the EGAKs. It included a question: “To what extent was the activity successful?” Responses were rated separately for each EGAK they used on a 7-point scale (0 = not at all′, 1 = to a very small extent′, 2 = to a small extent′, 3 = to a moderate extent′, 4 = to a large extent′, 5 = to a very large extent′, and 6 = excellent′).
Measurement of benefits
The benefits of EGAKs were also measured during the final interview. The questionnaire asked facilitators about the EGAKs’ benefits to the PLwD and to the facilitator concerning four domains: (1) changes in usual activities, (2) enhanced quality of the time spent together, (3) deepening facilitators’ understanding of the PLwD, and (4) facilitators’ understanding of the PLwDs’ condition. The questions are stated in Table 2.
Analytic approach
This study utilized a mixed methods analysis. For the quantitative analysis, we used IBM SPSS 29 for descriptive statistics (frequencies, mean, standard deviations and range) to (1) describe the PLwD and facilitators, (2) compare those who used the EGAKs with those who did not, (3) describe facilitator ratings of EGAKs’ success and benefits. For the qualitative analysis, we applied an inductive content analysis31,32 to the verbal descriptions of the degree of success of the EGAKs and to the verbal answers to the questions in Table 2 in oreder to identify the EGAKs’ specific benefits and potential outcomes. To establish trustworthiness and reduce bias in the analysis, the second author and a research assistant read all the data, conducted the categorization process, and analyzed the data independently. The categorization process was conducted iteratively, involving repeated readings of the data and the development of theme, category, and subcategory labels. These labels were revised as needed to reflect new insights emerging from the data. Upon completion, they produced an independent list of themes, categories, and subcategories. The lists were subsequently compared until a mutually agreed-upon version was reached. Both authors further discussed and refined the categorization and a consensual version was established. Trustworthiness was enhanced through prolonged engagement with the data over six months, ongoing interactions with participants, immediate interview transcription, inclusion of direct participant quotes, triangulation with quantitative analysis, and examination of negative cases. 33
Results
In the initial interview we obtained background information for 34 potential participants (PLwD, family caregivers of those who did not use EGAKs, and facilitators for those who did). See Table 1. The 16 PLwD who used the EGAKs used an average of 7.1 (S.D. = 2.2) kits (range: 3–10). EGAKs’ facilitators included 10 children, three grandchildren, two formal caregivers, and one friend of the PLwD. Most facilitators (87.5%) were women (Table 1). The majority (62.5%) were children of the PLwD. Facilitators had a mean age of 51.1 years (S.D. = 10.4, range: 25–69), and 18 (S.D. = 3.8) years of education (range: 12–24). The mean age of the PLwD was 82 years (S.D. = 9.5; range: 63–101) with most being women (87.5%) and widowed (72.5%). All PLwD were reported by family caregivers to have cognitive impairment, with a mean CPS score of 3.4 (S.D. = 1.3). The mean MDS ADL score was 1.4 (S.D. = 1.1). Slightly more than half of the PLwD (56.3%) were reported to have adequate hearing, but less than half (43.8%) were reported to have adequate vision.
Characteristics of the main caregiver/facilitator and persons living with dementia (N = 34).
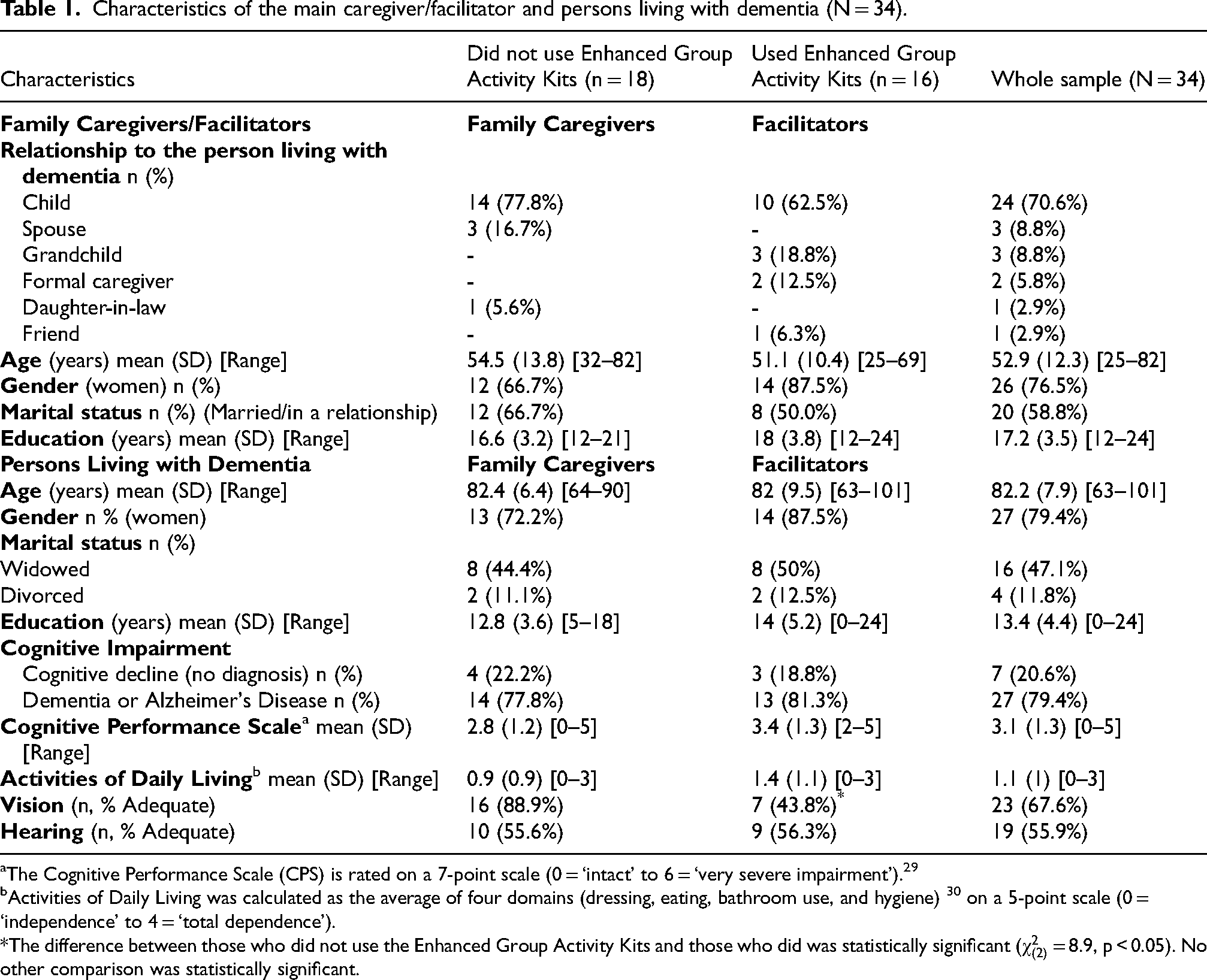
The Cognitive Performance Scale (CPS) is rated on a 7-point scale (0 = ‘intact’ to 6 = ‘very severe impairment’). 29
Activities of Daily Living was calculated as the average of four domains (dressing, eating, bathroom use, and hygiene) 30 on a 5-point scale (0 = ‘independence’ to 4 = ‘total dependence’).
The difference between those who did not use the Enhanced Group Activity Kits and those who did was statistically significant (
When comparing the background of PLwD who experienced EGAKs with that of those who did not, there was only one statistically significant difference (
Quantitative analysis
EGAKs’ success
We evaluated the facilitators’ ratings of the success of the EGAKs for the PLwD in two ways:
We calculated the average level of reported success—for each PLwD, over all the EGAKs used. The mean success level was 5.2 (S.D. = 1.1). Considering that the goal of the study was to explore whether EGAKs could help detect successful ways of engaging the PLwD on a one-on-one basis, rather than to evaluate the specific EGAKs used, we also examined the ratings for the three most successful EGAKs for each PLwD. For 12 PLwD, this average was between 5 and 6. For two PLwD, it was 4, and for another two it was 3.
EGAKs’ benefits
Facilitators reported improvements in all four domains: (a) changes in usual activities, (b) enhanced quality of the time spent together, (c) deepening facilitators’ understanding of the PLwD, and (d) facilitators’ understanding of the PLwDs’ condition. See Table 2. The most often reported benefits were regarding the EGAKs’ adding interest to the usual activities (93.7%), the extent to which the facilitator thought the PLwD enjoyed the activities (93.7%), the extent to which the facilitator enjoyed the activities (87.5%), and the extent to which the EGAKs provided opportunities for positive experiences (81.3%).
Effects of enhanced group activity kits′ use based on facilitators’ reports during final interview (n = 16).
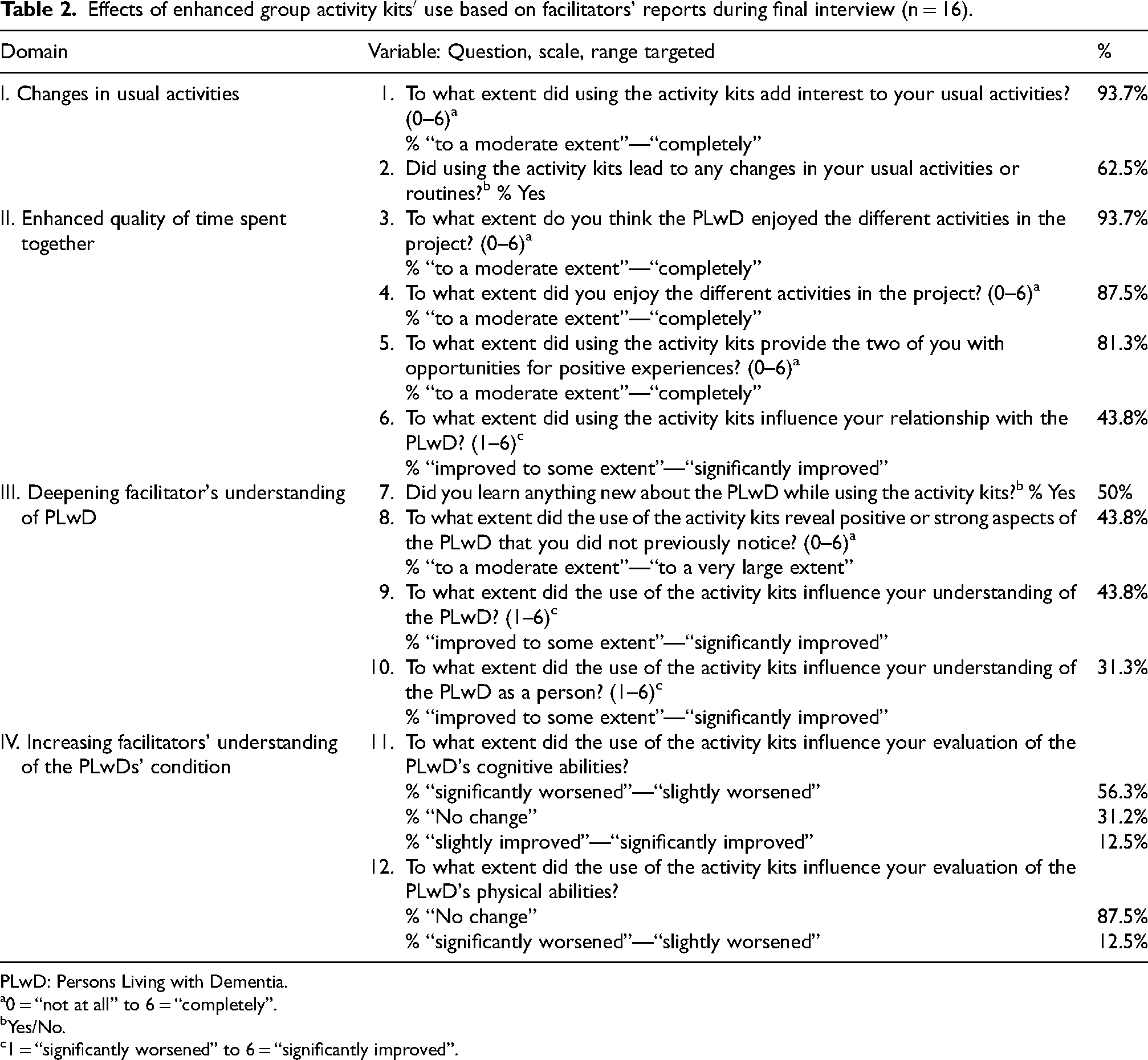
PLwD: Persons Living with Dementia.
0 = “not at all” to 6 = “completely”.
Yes/No.
1 = “significantly worsened” to 6 = “significantly improved”.
Most facilitators were close relatives of the PLwD or were well acquainted with them, yet 50% of the facilitators reported learning new things about the PLwD, and 43.8% reported becoming more aware of the capabilities of the PLwD, while the same percentage reported gaining improved insight into the PLwD. More than half of the facilitators (56.3%) stated that due to their use of EGAKs they realized that the cognitive functioning of the PLwD was worse than they had originally thought. However, two facilitators (12.5%) were surprised by better cognitive functioning (e.g., reading) than they had expected.
Qualitative analysis
Four themes emerged in the qualitative analysis: Affecting mood, feelings and emotions; Affecting cognition and behavior; Shifts in perceptions; and Improving communication and relationship between the PLwD and facilitators. See Table 3. Each excerpt is followed by the facilitator's study number and relationship to the PLwD. All excerpts were translated from Hebrew into English by ChatGPT-4 and then were checked by both authors who are bi-lingual.
Outcomes of enhanced group activity kits.
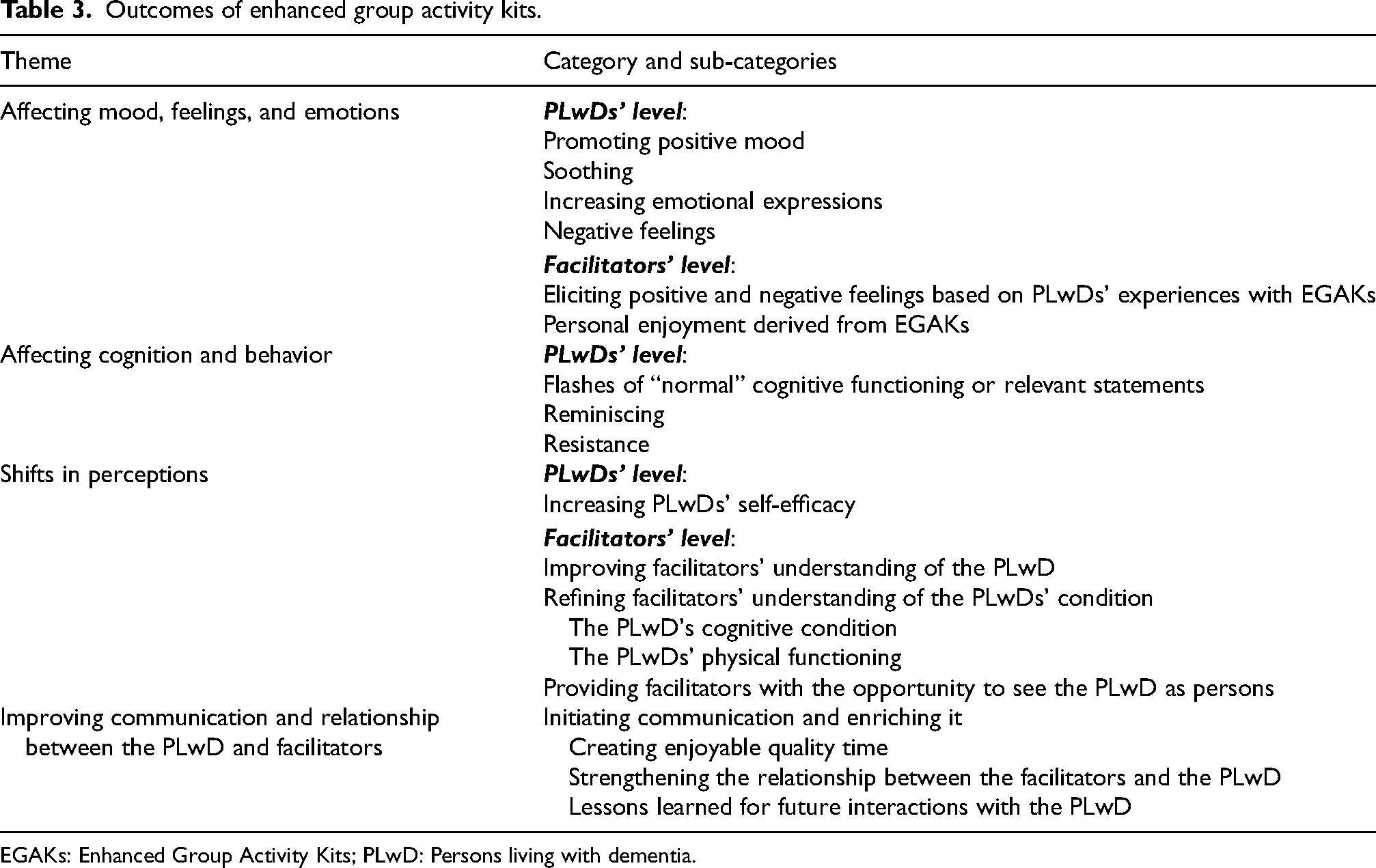
EGAKs: Enhanced Group Activity Kits; PLwD: Persons living with dementia.
Affecting mood, feelings, and emotions
PLwDs’ level
Promoting positive mood
Many EGAKs were perceived as facilitating positive affect as in, “She was really excited throughout the entire activity. The level of her enthusiasm surprised me” (102, Son, Reading). Some of these emotions were manifested also through the PLwDs’ facial expressions and reflected joy: “Her excitement about the things she saw, from the stories she told” (104, Granddaughter, Miscellaneous).
Soothing
The act of singing was perceived as soothing: “She enjoys singing. It does her good, it calms her down” (110, Daughter).
Enhancing emotional expression
EGAKs’ use enhanced emotional engagement of PLwD: “I was surprised by her facial expressions in the more emotional parts of the story [about poverty, anger…]” (112, Granddaughter, Reading).
Evoking negative feelings
When the activity confronted the PLwD with her/his weaknesses, it generated negative affect. For instance, asking a too abstract open-ended question (“What activities of life were important to you”) embarrassed the PLwD: I felt that she was embarrassed when she did not know how to answer questions… It was nice to sit and talk, but it was less comfortable to feel Mom's embarrassment and have to try to move forward and ‘skip’ over it… I skipped many questions that were not relevant to Mom. (106, Daughter, Reading).
Facilitators’ level
Eliciting positive and negative feelings based on PLwDs’ experiences with EGAKs. Facing the PLwDs’ cognitive and physical condition was difficult for facilitators, as in, “It was frustrating to see her struggling to remember and not succeeding, but I could still understand what she meant” (113, Daughter, Miscellaneous). Other facilitators spoke of their pleasure when they observed the PLwDs’ enjoying an activity, as in, “It gives me joy and makes me happy to see her vibrant. She complains a lot about pain, and suddenly seeing her laughing and active is a good thing” (109, Granddaughter, Physical activity), or “I am happy when she is happy” (101, Daughter, Creative arts). Some facilitators reported that they found the activities to be
Affecting cognition and behavior
PLwDs’ level
Flashes of “normal” cognitive functioning or relevant statements
One facilitator stated she was surprised when “She called me by my name, and I was excited” (115, Formal caregiver, Travel). Another facilitator spoke of different situations (for different activities) when her mother acted “normally” as before the dementia, as in, “When she accompanied me to the door, she asked me to call and let her know I arrived home. It is a saying that perfectly fits the situation, and I have not heard it in a long time” (106, Daughter, Singing). This facilitator also pointed out the sharpening impact of the singing activity on her mother: “After we sang, she spoke more to the point” (106, Daughter).
Reminiscing
The activities evoked many memories from the past, as in, “The conversation with Mom about Tel Aviv brought up many memories from her youth” (103, Daughter, Travel).
Resistance
Some PLwD refused to participate in activities. In one case, this was due to the PLwD considering the activity childish: “She slightly opposed it because she thought it was appropriate for children” (102, Son, Reading), or due to a general resistance to the activities, as in, “It is difficult, because I have to push her, persuade her, even put on a show just to get her to agree to do something. She shows resistance, and I wonder if she feels that there is a loss of dignity involved” (116, Friend).
Shifts in perceptions
PLwDs’ level
Increasing PLwDs’ self-efficacy
Hands-on activities made PLwD feel valuable, as in, “She felt that she was doing something, that she could show us something she had made. The flowerpot she created stood proudly in the kitchen for a long time” (101, Daughter, Creative arts), or “It makes her feel that she is capable of doing things” (111, Daughter). EGAKs also enhanced the PLwDs’ self-efficacy by sometimes providing them with a teaching role rather than a learning role, as in, ‘Things from yesteryear': Very interesting. It allowed her to teach me. I played along a bit too, and she told me stories non-stop. She said the soap [seen in the PowerPoint presentation] used to stink; Explained what one does with the [old] items, how one pronounces the words. She taught me, and it empowered her. She explained the objects to me, and when I asked how they were made, she had to teach me a complete lesson. (114, Formal caregiver, Miscellaneous)
Facilitators’ level
Improving facilitators’ understanding of the PLwD. Some facilitators observed retained abilities, as in, For me, as a daughter of a mother going through the process of forgetting, it was a pleasure to see her reading. It was moving to see that she still remembered Tel Aviv and Umm Kulthum. We even talked about Picasso, which is not really her field. I saw that she is still someone who reads, understands. She is still with us. It does not matter that a few days later, when I asked if she remembered we talked about Umm Kulthum, she did not remember. (103, Daughter, Reading)
Refining the facilitators’ understanding of the PLwDs’ condition
Use of EGAKs revealed the PLwDs’ condition: “The activity kits did not change my understanding of him, but they made me see what remains of what was, and that is not much” (108, Daughter).
The PLwDs’ cognitive condition
One facilitator was surprised by his mother's retained reading ability: “I was surprised that she managed to read about 65% of the text by herself” (102, Son, Reading). Yet another facilitator was shocked by the inability to read, as in, The kit that caught us by surprise. We had seen her reading signs before, but during this activity, we discovered that it was not relevant. She could not keep up; she could not read. The amount of text in this kit overwhelmed her (110, Daughter, Reading). As a person, she was a very intelligent woman, but now she does not remember and speaks off-topic. Here, her answers pleasantly surprised me. As for songs—I realized she knows so many songs and can sing them with the correct melody. Even if in the past it was embarrassing to hear her sing, today she sings really beautifully. (111, Daughter)
Yet sometimes the PLwD did not remember the songs’ lyrics: “I was sure she would remember the words, but she did not” (104, Granddaughter, Singing), or personal information: “There were questions I was surprised to discover she did not know the answer to, meaning that her condition has worsened” (112, Granddaughter, Miscellaneous).
The PLwDs’ physical functioning
One facilitator referred to her amazement at her grandmother's ability to complete physical tasks: “She is a bit overweight and has some difficulty seeing, so it was hard for me to imagine her doing it, but she did it great” (109, Granddaughter, Physical activity). Facilitators reported reconsidering the PLwDs’ condition in physical tasks, as in, “I wanted to do a sports activity, but I realized she was unstable and swaying, so I did not do it” (112, Granddaughter). Working with the kits revealed problems with fine motor skills, of which the facilitators were unaware: “During the drawing activity, we suddenly realized how much she is unable to use her hands – it was a bit new and frustrating” (101, Daughter).
Providing facilitators with the opportunity to see the PLwD as persons
The activity was also an opportunity to get to know the PLwDs’ perspective, “It is nice. It is interesting to see their worldview, the way they look at things” (104, Granddaughter, Miscellaneous). It also enabled them to learn about the PLwDs’ preferences “I understand more now what she likes and does not like, what frustrates her” (111, Daughter).
Improving communication and relationship between the PLwD and facilitators
Initiating communication and enriching it
The EGAKs assisted in initiating conversations and provided the PLwD with opportunities to talk, “It definitely created conversation and interest and gave her a platform to speak” (112, Granddaughter, Miscellaneous). The experience enriched the communication, “She would always talk about certain things, and the visits revolved around those same topics. The kits opened the door to other subjects” (109, Granddaughter), and deepened it, “It took me to places I would not have encountered like this… It took us to subjects we do not touch on in daily life. It connected us to memories. It was good. In daily life, the conversation is very concrete” (106, Daughter).
Creating enjoyable quality time
EGAKs fostered quality time between the facilitators and the PLwD: “It created quality time with her, one-on-one and in a purposeful way. It filled my time with her. Quality time that was focused on doing. It worked great for me” (112, Granddaughter). The EGAKs’ setting facilitated the meaningful time together, “The whole aspect of attention, sitting one-on-one and not just listening to her but doing something else, really contributed here” (103, Daughter).
Strengthening the relationship between the facilitators and the PLwD
Some facilitators reported that the mutual and equal dynamics strengthened their relationship with the PLwD, as in, “It had a very positive impact [on our relationship] because it created a shared area of interest. We would sit together and do things together” (103, Daughter). The shared learning deepened their relationship and acquaintance: The relationship strengthened, and we learned together… It allowed us to bond, learn about each other, and learn together. It made the time pass in a good way… It created more personal conversations. I learned about her. I knew her before, but very superficially. Today, I can tell stories about her. Now, during her Shiva [time of mourning after a death], I shared stories about her with her grandchildren. (114, Formal caregiver).
Lessons learned for future interactions with the PLwD
A facilitator who previously recounted the complex nature of her relationship with her mother, described the meaning of EGAKs for their interactions, “The kits provide a solution for moments when you arrive and do not know what to do” (107, Daughter). EGAKs’ experience provided the facilitators with an opportunity to learn how to tailor future activities to the PLwD, “I learned how to create an activity that would suit her” (103, Daughter), and how to get the PLwD engaged, “I need to focus more on activities that involve more doing, singing or physical activity, and less on intellectual conversation. It is hopeless” (106, Daughter, Travel). One facilitator referred to the broader effect of EGAKs’ use on his overall interaction with his mother: Getting acquainted - Great kit… It is a great tool to develop a conversation and keep it going. It focuses you on simple things… We, as a family, are also dealing with how to make visits enjoyable and pleasant for both sides… This kit opened my mind in terms of just going with the flow… The kits helped me realize that I need to live in the moment with her… I saw this as a lifesaver kit. Something to turn to if I lose my way and do not know where it is going… I think it is good to have a variety of topics and activities through which you can figure out what to do. (102, Son).
Discussion
The hypotheses that facilitators would find it feasible to implement selected EGAKs with PLwD in home settings and that they would perceive the experience as successful were generally supported. However, the full meaning of this experience proved more complex. While most facilitators were able to use the EGAKs effectively, others encountered difficulties. Moreover, the success of the experience extended beyond mere implementation to include facilitators’ enhanced understanding of the PLwD and improved recognition of which specific EGAKs were most suitable for individual participants.
The goal of this study was to test the feasibility and the benefits of EGAKs tailored for one-on-one use by facilitators from close familial or social circles with community-dwelling PLwD. The results show that the adapted EGAKs were successful or very successful for most PLwD, according to the facilitators who used them. Most facilitators reported that the EGAKs increased the enjoyment experienced by the PLwD, and improved their interactions with the PLwD, while also enhancing the caregiving experience. The precise ways in which the activities were successful varied depending on PLwD and type of activity. In some cases, it was the topic of the kit that was enjoyable for the PLwD, such as music, or the activity appeared to give the PLwD a sense of success, or it brought about meaningful conversation. In some instances, an important benefit was the facilitator's improved understanding of the PLwD regarding retained skills of which the facilitator was not aware, such as reading, while in other cases the experience brought to light limitations unbeknownst to the facilitator. In either case, there was value to the revelations because they created an opportunity to tailor future activities and overall care to the true abilities of the PLwD. The enhanced engagement arising from the use of the activity materials often improved the quality of the relationship and the wellbeing of facilitators and PLwD. One of the most important lessons for some of the facilitators was that positive conversation was still possible, and that the fostering of a positive atmosphere within a conversation was the true goal. Facilitators credited the EGAKs for this accomplishment.
The results of this study echo the findings of prior studies with EGAKs in that they demonstrate success, as perceived by the facilitators, in using EGAKs with PLwD even in the home setting. Yet, using EGAKs in a one-on-one context poses unique challenges compared to group settings. In group activities, some participants are likely to respond early and create an atmosphere of engagement that encourages broader participation. While one-on-one encounters provide more personalized attention, success depends entirely on the individual participant's abilities and responsiveness. Consistent with these characteristics of home-based EGAK implementation, this pilot study found that individual encounters provided opportunities to better understand both the abilities and the limitations of PLwD. This enhanced understanding can inform adaptations of EGAKs to match participants’ functional levels, thereby fostering more positive experiences.
Though the facilitators availed themselves of the opportunity to decide which EGAKs to use, not all kits achieved their intended benefits. Some were too difficult, and, in a minority of cases, some of the EGAKs were perceived as inappropriate by the PLwD. However, at the discretion of facilitators, EGAKs can be modified, such as by decreasing the amount of text to be presented or by limiting or changing the EGAKs’ optional questions. In addition, if one EGAK does not seem to be going well, another can be tried. Future research is needed concerning whether certain levels of cognitive function or verbal fluency are needed for certain activities to be beneficial.
The main strength of the EGAKs’ approach as compared to other at-home interventions for PLwD as referred to in the introduction, 16 is (before any direct comparison has taken place) the elimination of the expense of employing professionals to come to the home to determine recommended activities and instruct the facilitator how to apply them with the PLwD. A professional can explain via telephone the general approach of EGAKs and the guidelines in the facilitator's booklet clarify how the EGAK is to be used.
This is not to say that the EGAKs approach is without costs. The costs involve development of the EGAKs, their refinement, and the production of EGAKs′ components, including booklets for the facilitators and PLwD, memory sticks with PowerPoint presentations, as well as specific materials (especially for creative art EGAKs). However, these costs are lower than hiring professionals for multiple home visits with PLwD and their family or formal caregivers.
One limitation of this study is that it is a pilot study of feasibility and exploration of perceived effects on PLwD and facilitators that does not allow for effective comparison with published controlled intervention studies. 17 A larger controlled study is needed to better assess the efficacy of the EGAK-based intervention, and to determine the functional level of PLwD who can benefit from EGAKs.
A second limitation is the small proportion of PLwD at home referred to the study who were able to participate in it. We intend to further investigate this issue, but our results suggest that the absence of facilitators willing and able to devote time and effort in trying a new intervention with PLwD was an important contributor to this limitation. Given that burden is common among caregivers of PLwD 34 and that not all PLwD have caregivers, interventions requiring a caregiver to implement them pose a significant barrier to overcome. Yet, as shown in this study, while the intervention places demand on facilitators, it can also alleviate some of their stress by reducing PLwD and caregiver boredom and loneliness, and increasing their level of positive interaction. Even if caregiver-dependent interventions were to be introduced only to a small proportion of PLwD in the community, the initiative may well improve the wellbeing of many people given the enormous size of this population.
This study explored an innovative approach to providing one-on-one activities to PLwD in their homes based on initial success reported in the use of EGAKs in senior day centers and geriatric care units. The findings indicate that EGAKs adapted for one-on-one use can be successful for most PLwD and facilitators. Our results show promise for further development, dissemination, and evaluation of one-on-one EGAKs.
Footnotes
Acknowledgements
The authors would like to thank the dyads who used the activity kits and especially the facilitators who provided valuable feedback and thoughtful insights regarding their use.
Ethical considerations
The study was approved by the institutional review board of Tel Aviv University on May 23, 2022.
Consent to participate
Informed consent was obtained from the main family caregivers of the persons living with dementia and from the facilitators.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Minerva Foundation grant number 3158329500.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Numerical data used for this study are available from the corresponding author in anonymized form upon reasonable request after approval for sharing the data has been obtained from the institutional review board. The open-ended data are not publicly available due to privacy and ethical concerns.