
Abstract
Background
The COVID-19 pandemic disrupted healthcare systems worldwide, forcing adaptations in care pathways. A particularly vulnerable patient group are those with Alzheimer's disease and other forms of dementia who experienced unique challenges during this period.
Objective
This study aims to examine shifts in healthcare utilization, focusing on inpatient and outpatient services.
Methods
We retrospectively analyzed 27,240 dementia cases from 86 German hospitals, comparing inpatient and outpatient care between March 1, 2020, and December 31, 2022 to cases from 2019. Admission rates, length of stay, disease severity (case mix, comorbidities) and complications (i.e., intensive care admission, mortality) were assessed using (generalized) mixed models.
Results
Outpatient care utilization for dementia increased during the pandemic (+33%, from 11.3 before to 15.1 daily admissions during the pandemic, p < 0.001), with three outpatient admissions accompanying each lacking inpatient admission (−20%, from 6.3 before to 5.0 daily admissions during the pandemic, p < 0.001). Morbidity indicators were generally lower during the pandemic for inpatient cases, while the proportion of comorbid depression was higher.
Conclusions
The pandemic triggered a substantial redistribution of dementia care favoring outpatient over inpatients services. The shift reflects an increased need for dementia-related medical interventions during the pandemic. This was likely due to social isolation aggravating dementia symptoms as evidenced by the increased rate of depression. At the same time, fear of COVID-19 exposure in hospitals likely discouraged inpatient admissions. We conclude that flexible and integrated care pathways are essential to ensure continuity and quality of care for dementia patients, especially during public health crises.
Keywords
Introduction
The COVID-19 pandemic disrupted healthcare systems worldwide, forcing adaptation in care pathways. In particular, hospitals in Germany were subject to public health regulations including the suspension of elective admissions, redistribution of wards and triage. 1 These measures strongly disrupted routine care pathways, especially for vulnerable groups such as those with dementia, since they have specific healthcare needs due to the chronic and progressive nature of their disease. Cognitive impairments render these individuals highly dependent on caregivers and healthcare systems for routine management. Dementia patients, significantly affected by social isolation during the pandemic, likely experienced an increased need for medical interventions.2–5
During the COVID-19 pandemic a reduction of inpatient admissions of roughly −20% has been documented in Germany.6,7 Specifically, our previous analyses have shown a decrease of hospital admissions for all neurological conditions by on average −18% during the COVID-19 pandemic with outpatient services failing to fully compensate for this decline. 8 Decreases in admission rates for inpatient dementia cases in another German (psychiatric) hospital network are equally reported at −20%, 9 while data for outpatient cases are not available.
Due to the ban on elective admissions a higher proportion of emergency admissions was a common phenomenon in hospitals. 10 How this affected dementia patients, is unknown in Germany.
Data on changes in length of stay are also not available for dementia inpatient cases in Germany during the pandemic.
While overall admissions for neurological cases declined, morbidity indices for those admitted patients were higher during the pandemic, implying that there was a treatment gap for less severely affected patients. 8 Mortality rates for neurological inpatient cases were not increased in the first waves,8,11 but increased during the omicron waves and the total span of the first three years of the pandemic from 2020 to 2022. 8 Unfortunately, specific data on changes in mortality or morbidity during the pandemic for the group of inpatient dementia cases are not available in Germany.
In summary, although the pandemic clearly affected dementia care utilization, comprehensive analyses in large, real-world cohorts remain elusive. Understanding these changes is critical to both addressing care gaps and building resilient healthcare systems for future public health crises.
Therefore, we address the following research questions:
Were inpatient admissions due to dementia reduced during the COVID-19 pandemic?
Did outpatient services compensate for any observed declines in inpatient care?
Were there significant changes in length of hospital stay, morbidity, or mortality for dementia inpatients during the pandemic?
Methods
Helios hospital structure
This study analyzed anonymized retrospective data from routine claims of 86 hospitals in Germany from the Helios hospital group. Individual structural information on participating hospitals (e.g., size, location, level of care) were not available due to data protection regulations. The Helios hospital network encompasses all care levels from primary care to maximum care, from non-academic to university hospitals all over Germany.
Data extraction
All data were collected for the purpose of clinical care and billing of services to health insurance companies. The analyzed cohort was part of a larger study cohort in a previous publication. 8 Data were extracted via QlikView (QlikTech, Radnor, PA, USA).
Definition of time periods and control periods
The total study period was March 1, 2020 through December 31, 2022 compared to the control period January 1, 2019 through December 31, 2019. Data were segmented into different virus predominance periods as defined before
12
:
Wildtype: March 1, 2020–March 7, 2021 (372 days) Alpha: March 8, 2021–June 25, 2021 (110 days) Delta: June 26, 2021–January 2, 2022 (191 days) Omicron: January 3, 2022–December 31, 2022 (362 days)
The different virus predominance periods were compared with the corresponding control periods of 2019 on the same dates. For instance, the alpha predominance period from March 8, 2021, to June 25, 2021, was compared to March 8, 2019, through June 25, 2019. As the study period for the wildtype predominance period was more than 365 days, seven days from 2019 were included twice (March 2, 2019 through March 8, 2019).
Diagnostic coding system
Diagnoses were made according to the International Statistical Classification of Diseases and Related Health Problems German Modification (ICD-10-GM) with the main diagnosis being the primary reason for hospital stay. Secondary diagnoses existed at the time of hospital stay or occurred during the hospital stay and complicated treatment.
Inclusion criteria
Included were all dementia cases with one of the following main discharge diagnoses: G30 Alzheimer disease, G31 Other degenerative disease of the brain, F00 Dementia in Alzheimer disease, F01 Vascular dementia, F02 Other dementia, F03 Unspecified dementia, F06.7 Mild cognitive impairment, G91.2 Normal-pressure hydrocephalus. We extracted the frequency and proportion of each main discharge diagnosis for each time point in the inpatient and outpatient cohorts.
Demographic information
We extracted age and sex to characterize cohorts.
Definition of inpatient and outpatient cases
Inpatient cases received full inpatient hospital care. Outpatient cases in this study refer to hospital-based day-care treatments documented within the same administrative and billing system as inpatient cases. Only services coded and reimbursed through the hospital sector were included; primary care or community-based outpatient treatments were not captured, as they fall under a separate reimbursement framework in the German healthcare system.
Mode of admission
We extracted the mode of admission, meaning “elective” was a scheduled admission and “urgent” was either due to an unscheduled emergency or a hospital transfer.
Length of stay
We extracted the length of stay defined by the number of nights in treatment.
Factors and variables for comorbidities and complications
All variables for comorbidity and complications were analyzed for the inpatient cohort only, since they were not available for outpatient cases due to the nature of German DRG data.
The following list contains all variables concerning comorbidities and complications and their operationalization (where applicable):
Case mix values were calculated and provided by each hospital for inpatient cases as part of routine DRG-based billing data; weights are standardized according to national reimbursement regulations and reflected the relative expected resource use of each hospital case based on diagnoses, procedures, and other factors Elixhauser comorbidity index (ECI) as a measure of the overall severity of comorbidities was extracted as explained in more detail previously.13,14 The AHRQ algorithm was applied to the weighted ECI.15,16 Furthermore, the frequency and proportion of each secondary diagnosis contained in the ECI was extracted. Total number of coded secondary diagnoses Mechanical ventilation (through codes of operations and procedures (OPS): OPS 8-70x, 8-71x, or duration of ventilation > 0) Intensive care admission (through OPS codes 8-980, 8-98d, 8-98f, or duration of intensive-care stay > 0) In-hospital mortality
Furthermore, we analyzed the occurrence of specific secondary diagnoses selected because of their clinical relevance as typical complications in geriatric patients and mentioning in scientific literature17,18: N17 Acute kidney failure, F05 Delirium, not induced by alcohol or other psychotropic substances, E86 Volume depletion (exsiccosis), N30 Cystitis, I26 Pulmonary embolism, J09-J18 Influenza and pneumonia, J69.0 aspiration pneumonia, I80 Thrombosis, phlebitis, and thrombophlebitis.
Statistical analyses
General remarks
Inferential statistics were based on generalized linear mixed models (GLMM), specifying hospitals as random factors. 19 The effects were estimated using the lme4 package (version 1.1-26) in R environment for statistical computing (version 4.0.2, 64-bit build).20,21 In all mixed models, we specified varying intercepts for the random factor. We computed intra-class correlation coefficients (ICCs) for all hierarchical models to quantify between-hospital variation. 22
Level of significance
For all tests, we applied a two-tailed 5% error criterion for significance. For linear mixed models, we computed p-values based on the Satterthwaite Approximation for the degrees of freedom. We generally report results for p < 0.05. To address multiple testing, we additionally applied the following thresholds: p < 0.01 for calculations in Table 1 (6 variables), p < 0.005 for calculations in Table 2 (10 variables), p < 0.005 for secondary diagnoses from ECI (31 variables).
Patient characteristics and case severity for cases with inpatient treatment.
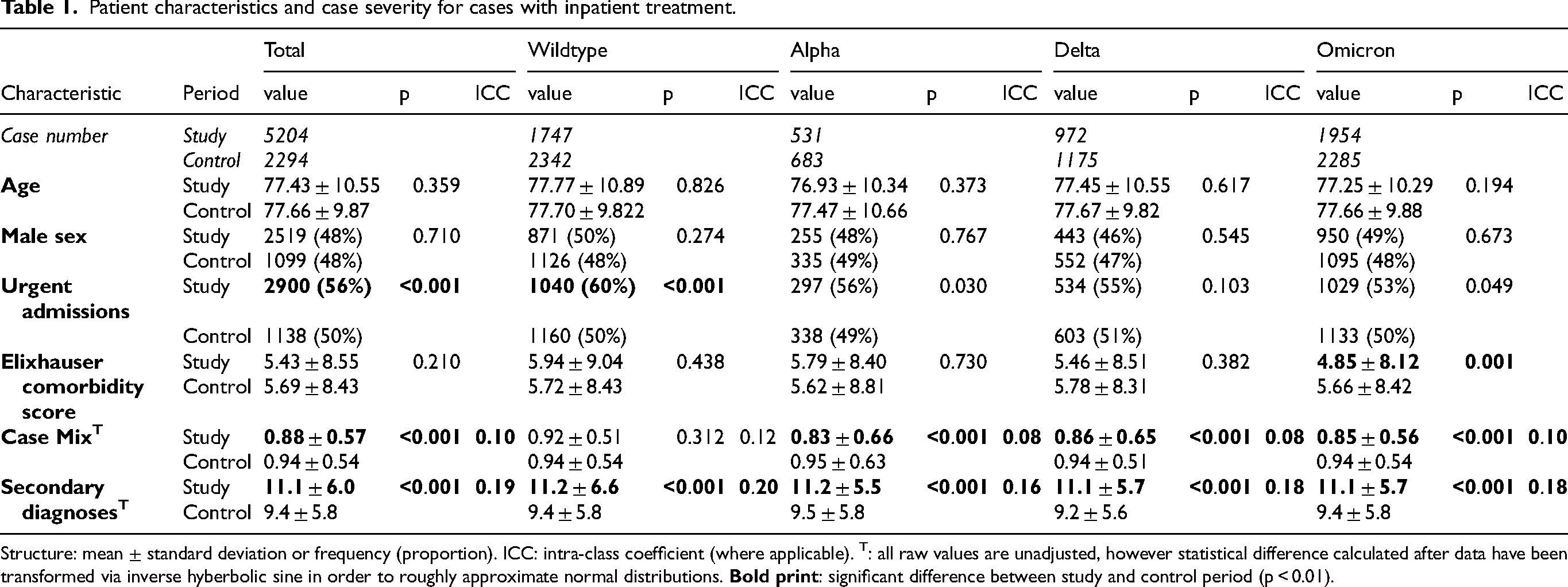
Structure: mean ± standard deviation or frequency (proportion). ICC: intra-class coefficient (where applicable). T: all raw values are unadjusted, however statistical difference calculated after data have been transformed via inverse hyberbolic sine in order to roughly approximate normal distributions.
Frequency and proportions of complications for inpatient cases.
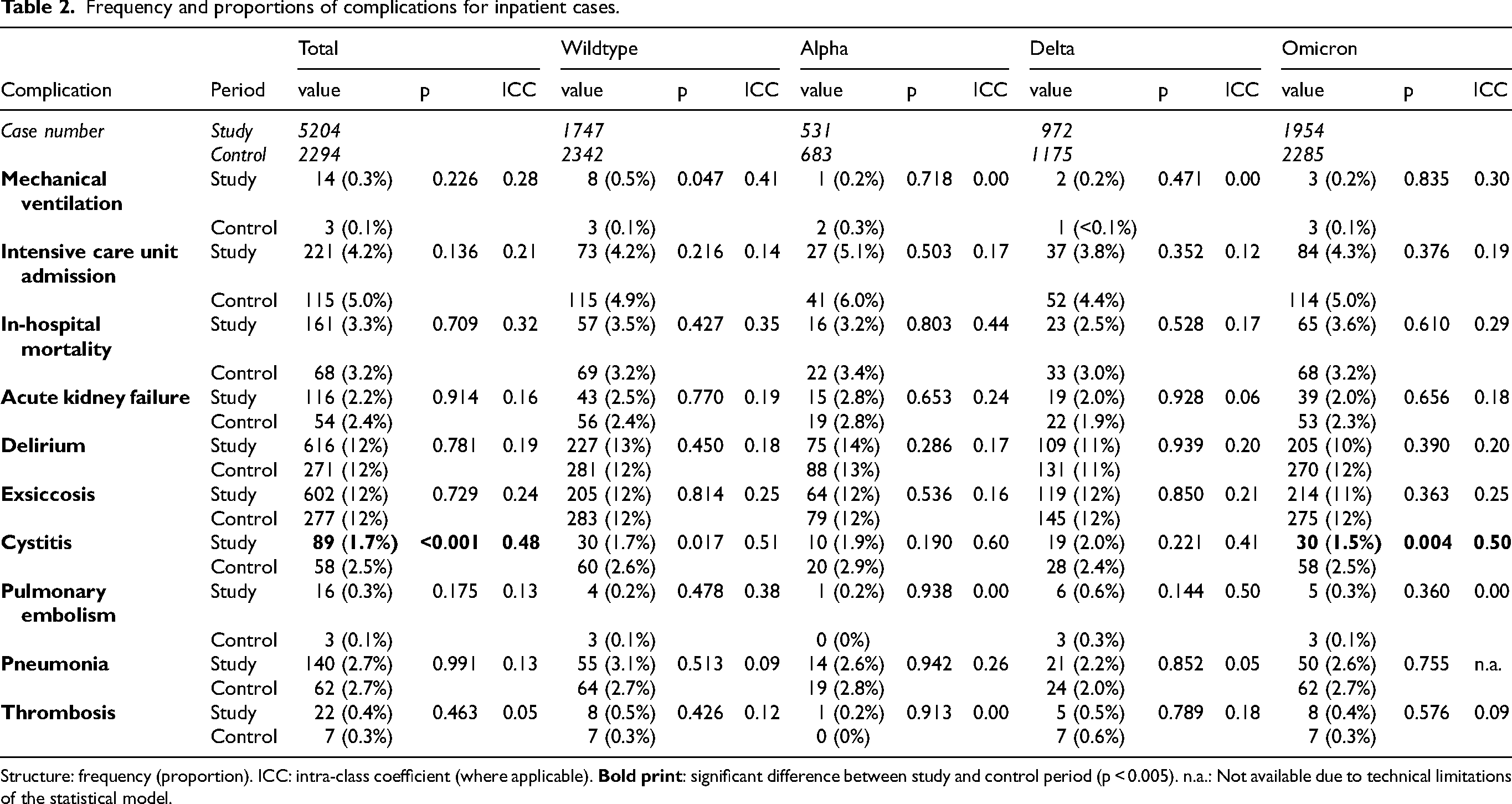
Structure: frequency (proportion). ICC: intra-class coefficient (where applicable).
Cohort description
To describe the patient characteristics of the cohorts and comorbidities, we employed χ2-tests for categorical variables (sex) and a two-sample t-test for numerical variables (age). We reported the proportions, means, standard deviations, and p values.
Admission patterns
Admission rates were modeled using negative binomial GLMMs with a log link function. We reported daily admissions, incidence rate ratios (IRRs), a 95% confidence interval (CI) and p values.
The admission mode was modeled using logistic GLMMs to compare proportions of urgent versus elective admissions between time periods. We reported proportions and p values.
Length of stay was modeled using linear mixed models. Due to a positively skewed distribution, we applied inverse hyperbolic sine transformation. We reported means, standard deviations, and p values.
Outpatient cases
Outpatient admission counts were analyzed with the same negative binomial GLMM approach as inpatient rates. No multivariable modeling was applied to outpatient morbidity or mortality due to lack of comparable data.
Cumulative hospitalization deficit
The cumulative hospitalization deficit was computed as the difference between the expected and observed cumulative admission numbers in the study period, expressed as incidence rate ratio (IRR) of the cumulative expected number. The expected number of admissions was defined as the daily average during the 2019 control period.
Comorbidities and complications (inpatient cases)
Case mix, ECI, and number of secondary diagnoses were modeled using linear mixed models. The presence of selected complications and individual ECI items were modeled using logistic GLMMs. We reported means, standard deviations and p values. Because the variables Case mix and number of secondary diagnoses were positively skewed, we transformed them using an inverse hyperbolic sine to approximate normal distributions.
Mechanical ventilation, intensive care admission, and in-hospital mortality were analyzed as binary outcomes using logistic GLMMs with hospital as a random effect. We reported proportions and p values.
Timing of publication statement
Data analysis for this subgroup of dementia was conducted in July 2023 following ethics approval. The manuscript was finalized and submitted in March 2025 after prioritizing publication of broader analyses from the same dataset. This sequencing was a strategic decision which allowed integration of feedback from prior publications to improve subgroup analyses.
Declaration of ai-assisted writing
The authors used ChatGPT-4 from OpenAI (chat.openai.com) to assist with language refinement, structuring passages, and translations from German to English. Its use was strictly limited to improving fluency and clarity. The first draft, all scientific content, data interpretation and conclusions were exclusively authored by the researchers. The final responsibility for the manuscript's content remains entirely with the authors.
Results
Cohort description
Case numbers
The overall number of included cases was 27,240 cases, of which 7498 were inpatient cases and 19,742 outpatient cases. Hospitals contributed the following inpatient dementia cases: 99.7 cases on average, 34.5 median number of cases, minimum 1 case and maximum 650 cases. Hospitals contributed the following outpatient dementia cases: 282.0 cases on average, 23 median number of cases, minimum 1 case and maximum 5891 cases.
Cohort demographics
Overall, patients from inpatient cases were 77.43 years old in the study cohort and 77.66 years old in the control cohort. 48% of inpatient cases were male. Throughout all the examined COVID-19 periods, age and sex were not different compared to the pre-pandemic period for the inpatient cases. More detailed data are presented in Table 1. Supplemental Table 1 shows demographic data for outpatient cases.
Proportion of dementia diagnoses over time
All proportions of different dementia diagnoses can be found in Supplemental Tables 2 and 3. Overall, the proportion of dementia diagnoses remained relatively stable over time. For inpatient cases the number of “F03 Unspecified dementia” increased during the pandemic from 14% to 18%, while the proportion decreased from 25% to 22% in outpatient settings. The proportion of “F06.7 mild cognitive impairment” increased during the pandemic in inpatient settings from 7.2% to 8.3% and in outpatient settings even more so from 10% to 14%. The majority (80%) of patients with mild cognitive impairment were treated in outpatient settings.
Admission patterns
Inpatient admission patterns
The number of inpatient cases for the study periods are listed in Table 1. The case numbers of outpatients for the study versus the control periods were: total 15,617 versus 4125, wildtype 5948 versus 4154, alpha 1594 versus 1224, delta 2714 versus 1983, 5361 versus 4063.
Daily admissions of inpatient cases were significantly reduced in the total pandemic period and in each of the four virus predominance periods. The data are visualized in Figures 1 and 2. In the total period, daily inpatient admissions were 5.0 ± 3.5 versus 6.3 ± 4.1 (p < 0.001), resulting in an IRR of 0.80 (95% CI 0.73–0.87). In the wildtype predominance period daily inpatient admissions were 4.7 ± 3.3 versus 6.3 ± 4.1 (p < 0.001), resulting in an IRR of 0.75 (95% CI 0.67–0.83). In the alpha predominance period daily inpatient admissions were 4.8 ± 3.2 versus 6.2 ± 4.2 (p < 0.009), resulting in an IRR of 0.78 (95% CI 0.64–0.94). In the delta predominance period daily inpatient admissions were 5.1 ± 3.6 versus 6.2 ± 4.0 (p < 0.009), resulting in an IRR of 0.83 (95% CI 0.72–0.95). In the omicron predominance period, daily inpatient admissions were 5.4 ± 3.7 versus 6.3 ± 4.2 (p < 0.003), resulting in an IRR of 0.86 (95% CI 0.77–0.95).
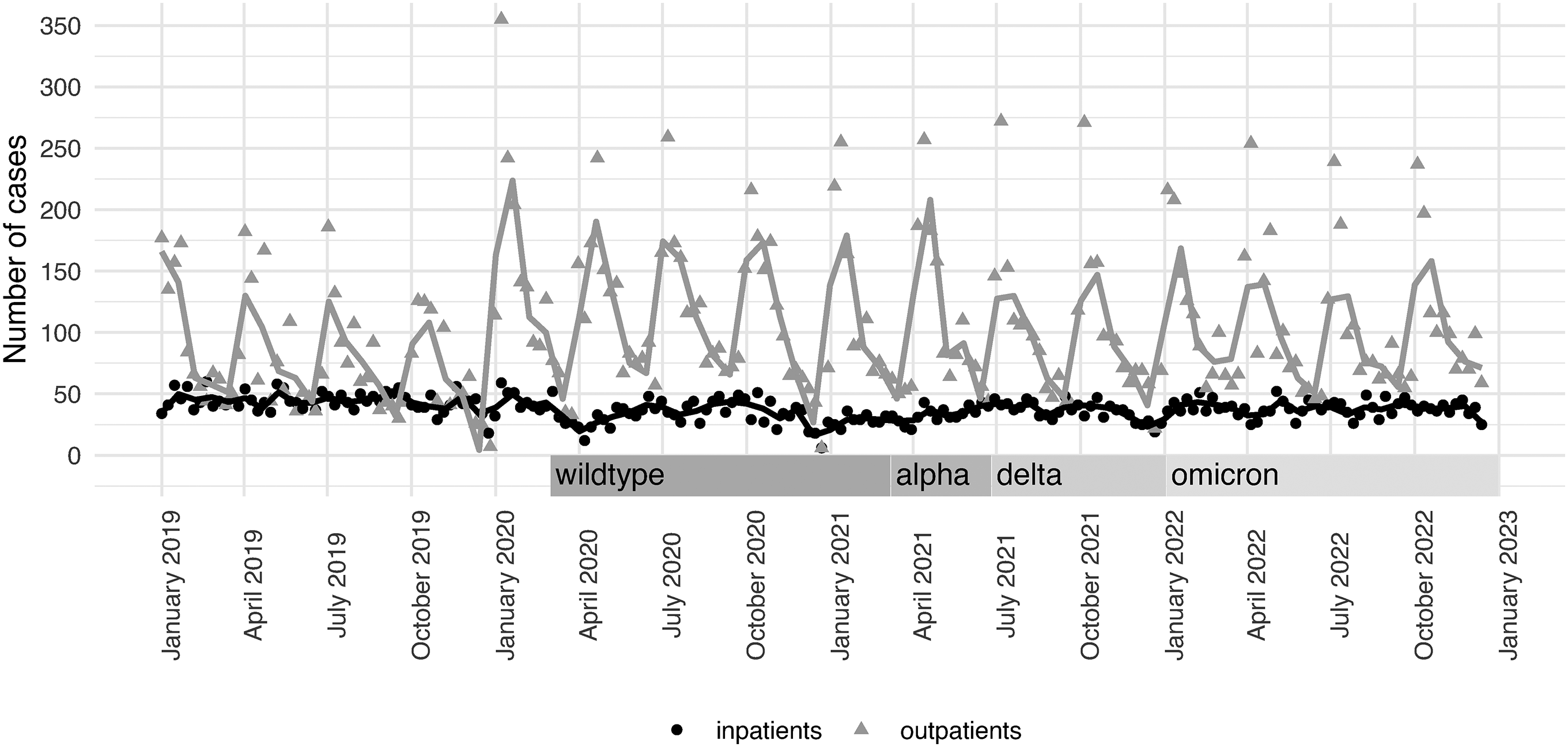
Changes in treatment frequency for dementia patients during the COVID-19 pandemic. The graph depicts the temporal development of dementia patient treatments in outpatient (gray triangles) and inpatient (black dots) settings from January 2019 to December 2022. During the COVID-19 pandemic, especially throughout the wildtype, alpha, delta, and omicron predominance periods, outpatient treatments increased significantly, while inpatient treatments decreased to a lesser extent (cf. Figure 2).
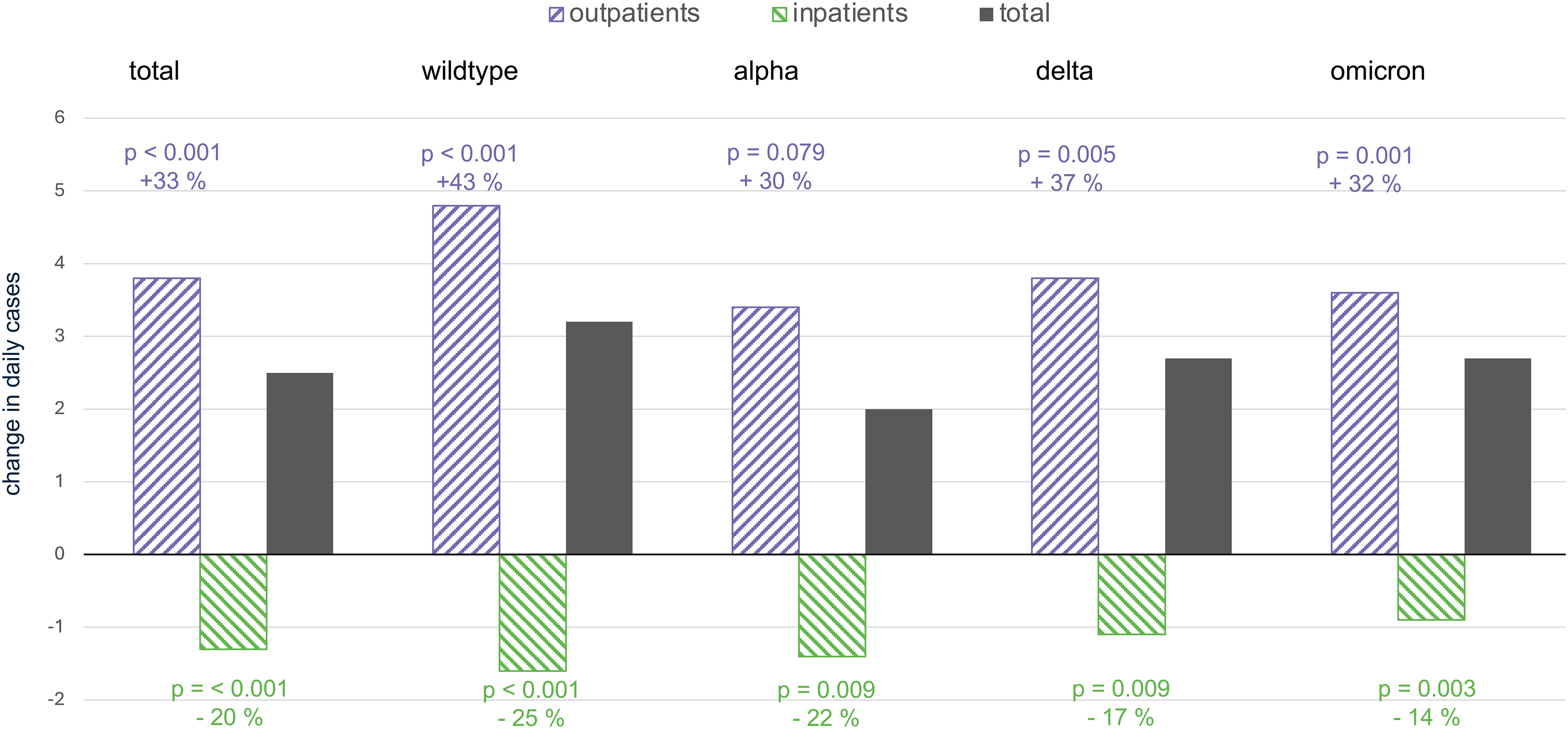
Shift during pandemic: outpatient admissions compensated three times for reduced inpatient admissions. This bar chart illustrates the change in daily dementia patient cases for outpatient (purple, diagonal up), inpatient (green, diagonal down), and total (black) settings during different COVID-19 virus predominance periods: total time, wildtype, alpha, delta, and omicron. Outpatient care increased significantly during most phases, with the largest spike during the wildtype (+43%, p < 0.001) and delta (+37%, p = 0.005) predominance periods. In contrast, inpatient care consistently declined, particularly during the wildtype (−25%, p < 0.001) and alpha (−22%, p = 0.009) predominance periods. The total number of cases (inpatient + outpatient) were thus higher than prior to the pandemic.
Outpatient admission patterns
While inpatient admissions for dementia cases declined, the outpatient admission rates increased across all pandemic phases. In the total period, daily outpatient admissions were 15.1 ± 15.5 versus 11.3 ± 13.0 (p < 0.001), resulting in an IRR of 1.33 (95% CI 1.17–1.53). In the wildtype predominance period, daily outpatient admissions were 16.0 ± 15.7 versus 11.2 ± 12.9 (p < 0.001), resulting in an IRR of 1.43 (95% CI 1.21–1.69). In the alpha predominance period, daily outpatient admissions were 11.1 ± 12.9, resulting in an IRR of 1.30 (95% CI 0.97–1.75), which was only a trend (p = 0.079). In the delta predominance period, daily outpatient admissions were 14.2 ± 15.4 versus 10.4 ± 12.1 (p = 0.005), resulting in an IRR of 1.37 (95% CI 1.10–1.70). In the omicron predominance period, daily outpatient admissions were 14.8 ± 15.2 versus 11.2 ± 12.9 (p = 0.001), resulting in an IRR of 1.32 (95% CI 1.12–1.55).
Admission mode
Compared to pre-pandemic times, the percentage of urgent admissions was significantly higher in the total pandemic period, as well as in the wildtype predominance period (Table 1).
Length of stay
The length of stay was shorter during the study period compared to the control period (p < 0.001; 10.6 ± 13.2 days versus 10.7 ± 12.8 days). The length of stay was shorter during the alpha predominance period (p = 0.004; with 10.2 versus 10.5 days, the delta predominance period (p = 0.009; 10.6 versus 11.2 days) and the omicron predominance period (p < 0.001; 10.3 versus 10.7 days).
Disease burden (for inpatient cases)
Comorbidity
ECI was lower (p = 0.001) during the omicron predominance period (Table 1). Case mix was higher (all p < 0.001) during the pandemic in the total time period, as well as in the alpha, delta and omicron predominance periods (Table 1). The average number of secondary diagnoses was higher (all p < 0.001) in the total pandemic period, as well as in the wildtype, alpha, delta and omicron periods (Table 1).
Higher proportions of secondary diagnoses were found only for depression (delta predominance period: 12.0% versus 7.9%, p = 0.001). Lower proportions of diagnoses were found for obesity (alpha predominance period: 3.8% versus 7.9%, p = 0.004) and renal failure (total period: 24% versus 29%, p < 0.001; omicron predominance period: 21% versus. 29%, p < 0.001).
Complications
There were no significant changes for mechanical ventilation, intensive care admission, or in-hospital mortality (cf. Table 2). The proportion of cystitis as a secondary diagnosis was lower in the total (p < 0.001) pandemic period, as well as during the omicron period (p = .0.004) (Table 2). The latter finding might be biased because of regional differences between hospitals as indicated by the high ICCs of 0.41 to 0.60.
Discussion
The main results are a marked shift in dementia care with greatly increased outpatient services while inpatient admissions decreased in the pandemic. This resulted in three outpatient admissions for every “missed” inpatient admission. Inpatient dementia cases were characterized by higher urgency, shorter lengths of stay, and lower overall disease severity. Notably, the proportion of depression as a comorbidity of dementia was higher in inpatient cases during the pandemic.
Increased healthcare utilization by dementia patients with a preference for outpatient services
Previous studies have shown that patients with dementia had a significantly higher risk of mortality and complications due to hospitalization during the COVID-19 pandemic compared to before, and, compared to people without cognitive impairment. The main drivers of this were an increased susceptibility to contract COVID-19 and an increased risk of developing severe symptoms of COVID-19. 23 However, our study took a novel approach by examining admissions due to dementia and thus independent of SARS-CoV-2 infection. Using this approach, we found reductions of hospital inpatient admissions during the first two years of the pandemic by −20% which match previous literature.6–9 However, taking inpatient and outpatient care together, there was an increased utilization of healthcare facilities of dementia patients in this study. A previous study in Germany showed a compensation of outpatient facilities for decreased hospital admissions in psychiatric patients 7 and no compensation of outpatient facilities for decreased hospital admissions in neurology. 8 The COVID-19 pandemic affected dementia patients in a particular way increasing their need for medical interventions. Symptoms of depression, anxiety and cognitive decline were significantly aggravated by social isolation during the pandemic in the elderly population and in patients with dementia.2–5 This is also mirrored in our data by the increased prevalence of depression as a comorbidity in dementia patients in hospitals. Furthermore, cognitive decline and functional deterioration were particularly challenging for caregivers of dementia patients.2,4 Caregivers themselves reportedly felt more overwhelmed, anxious and irritable.3,4 The increased utilization of healthcare services by dementia patients during the pandemic reflects on the one hand the impact of social isolation on this vulnerable patient group, and on the other hand the resilience of the outpatient facilities to address their medical needs. Furthermore, patients with “F06.7 mild cognitive impairment”—a risk factor for developing dementia and often a prodromal stage—were increasingly admitted to inpatient and outpatient services. Four out of five cases were treated in outpatient facilities. This group apparently had a higher diagnostic and therapeutic demand during the pandemic compared to pre-pandemic times.
Taken together, these findings are vastly expanding knowledge from previous studies about altered and increased healthcare utilization for dementia during the pandemic.
Natural prioritization: postponing elective hospital admissions for dementia
The prioritization of urgent cases during the COVID-19 pandemic was in line with previous data.8,10,24 This represents further evidence of how hospitals naturally prioritized patients and shifted their resources towards patients with immediate and life-threatening needs. 1 The increased proportion of “Unspecified dementia” in inpatient cases during the pandemic, is supporting this finding, since it indicates a lack of diagnostic specificity in hospitals for dementia during the pandemic. Elective and non-urgent cases, or procedures such as lumbar punctures or neuroimaging, were routinely postponed as part of broader efforts to conserve healthcare resources and reduce patient exposure to the virus. This reprioritization had an immediate impact on the care pathways of dementia patients. Other studies report rather disrupted outpatient care pathways for dementia patients.25–27 However, data from this study do not support this for dementia care, at least in the Helios day clinic network in Germany. Opposite to the inpatient cohort, our outpatient data showed a reduced proportion of “F03 unspecified dementia” indicating a higher diagnostic specificity for day care clinics compared to pre-pandemic times. There are good logistical reasons why outpatient care was well-suited for dementia care during the pandemic. Unlike acute conditions requiring urgent diagnostic workflows and urgent treatments, these needs could often be met in outpatient settings for dementia patients. Careful planning and coordination of neuroimaging, cognitive assessments, laboratory tests could easily have been conducted in outpatient facilities.
To our knowledge, this is the first study to report increased outpatient utilization specifically in patients with mild cognitive impairment and dementia during the pandemic. According to our data, day care services seem to have been offering healthcare according to this cohort's needs during the disruptions caused by the pandemic.
Avoidance of inpatient admission by more morbid dementia patients
Contrary to our previous data in a neurological cohort 8 and other independent data from all hospital cases, 28 morbidity indices were lower in the dementia cohort during the pandemic compared to pre-pandemic times. Lower morbidity indices may indicate that multimorbid dementia patients specifically avoided inpatient admissions. Another fact supporting the observation of patients avoiding hospital stay was the significantly shorter length of stay, representing reduced direct contact with hospital facilities.
One of the main reasons of reduced inpatient admissions may have been a fear of hospital-associated COVID-19 exposure.8,29 This is backed by the fact that the proportion of comorbidities of specific chronic conditions with high risk of contracting severe COVID-19 was significantly lower in this cohort. The less prevalent risk factors in this inpatient dementia cohort during the pandemic were kidney failure and obesity—both are known risk factors for contracting severe COVID-19. 30 Whether patients were aware of their specific risk factors for contracting severe COVID-19, or whether their referring physician specifically filtered high-risk patients, remains unclear. Possibly, a perceived risk of complications in general by hospitalization added to this hesitancy toward inpatient care for dementia patients. Hospitalization of multimorbid dementia patients is generally known to also increase the risk for delirium, pressure areas and other complications.17,18,31 These increased risks for dementia patients may have increased the threshold for inpatient admission on the side of patients, caregivers and also referring physicians. Furthermore, physicians were particularly concerned with the limited availability of inpatient capacities and keen to improve outpatient care where possible. 32 Lastly, reduced inpatient admissions were probably also driven by the patients’ needs and their caregivers’ perspectives. The specific care needs of dementia patients were very difficult to meet by the overstrained staff together with visitor restrictions during the pandemic.33,34 Patients with cognitive disorders are strongly reliant on their caregivers. Thus, they were particularly vulnerable in this time of visitor restrictions and social distancing.2–5
Overall, the shift toward outpatient care by dementia patients during the pandemic appears to be a result of both structural constraints and conscious decisions by patients, caregivers, and referring physicians.
Limitations
In addition to its retrospective design, certain limitations of this study need to be addressed. First, the use of administrative claims has previously been implied with coding inaccuracies or misclassification of diagnoses. Second, the data are extracted from the German healthcare system limiting generalizability. Third, the study does not analyze specific details of inpatient- and outpatient care and thus cannot evaluate whether the increased quantity of healthcare utilization offered an adequate care in terms of delivery of medical care and improvement of quality of life for patients and caregivers. The main strength of this study was the large set of real-world data.35,36
Conclusions
During the COVID-19 pandemic, dementia patients probably avoided hospital care in fear of COVID-19 contraction and other dementia-specific complications, such as delirium. Overall, the increased reliance on outpatient services for dementia patients reflects a well-adapted response by the German healthcare system to the constraints of the pandemic. Outpatient facilities were thus an available and safer alternative for dementia patients to meet their medical needs that have been aggravated through the pandemic.
Implications
The observed shift toward outpatient care in dementia medicine underscores the need to strengthen decentralized, flexible healthcare structures for our large population of people with cognitive impairment. Outpatient clinics have proven effective in addressing medical needs during the pandemic. In future public health crises, outpatient and day-clinic services must be equipped to assume core responsibilities for vulnerable patient groups. The lessons learned from this pandemic may also be relevant beyond crisis settings. Therefore, we encourage research to systematically assess the effectiveness of outpatient dementia care in ongoing routine practice. Strengthening outpatient services could improve care quality, reduce the financial burden of full inpatient admissions, and prevent hospitalization-related complications in patients with cognitive impairments.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251386368 - Supplemental material for Dementia care shifted towards outpatient services during the COVID-19 pandemic in Germany
Supplemental material, sj-docx-1-alz-10.1177_13872877251386368 for Dementia care shifted towards outpatient services during the COVID-19 pandemic in Germany by Nils Diogo Nellessen, Mohamad Samehni, Sven Hohenstein, Andreas Bollmann, Julius Dengler, Frederick Palm and Juraj Kukolja in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
This study was approved by the Ethics Committee of the Medical Faculty of Leipzig University (#490/20-ek). Helios Health and Helios Hospitals have strict rules regarding data-sharing and detailed restrictions to preserve data privacy. This study was conducted according to the declaration of Helsinki in its most recent form. 37
Consent to participate
Owing to the retrospective nature of the data and anonymized data extraction, informed consent was not obtained.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Helios Kliniken GmbH, [Grant-ID: 2023-0110]. The funder had no role in the design, data collection, data analysis, or reporting of the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during the current study are not publicly available due to patient confidentiality but are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.