
Abstract
Background
Dementia is a significant public health issue globally. People with dementia (PWD) exhibit symptoms in multiple domains (e.g., cognition, emotion, motor, speech/language) that can vary in their impact on the caregiver and the PWD-caregiver relationship.
Objective
We assessed the relative impact of various dementia symptoms on caregiver health and well-being and on the PWD-caregiver relationship using a broad sampling of PWD symptoms and caregiver/relationship outcome measures.
Methods
Data were analyzed from 54 primary caregivers of PWDs who completed seven questionnaires assessing caregiver health and well-being and PWD-caregiver relationship quality. An exploratory factor analysis of these questionnaires revealed two primary factors: (a) General Distress (anxiety, burden, depression, general health, loneliness), and (b) Relationship Quality (interpersonal closeness, relationship satisfaction). Caregivers also rated nine categories of PWD symptoms (memory, executive functions, speech/language, visual/spatial, motor, changes in behavior, sleep, medical/sensory, activities of daily living).
Results
Greater caregiver General Distress was associated with greater PWD speech/language and sleep symptoms. Lower caregiver Relationship Quality was associated (at trend, p < 0.10, levels) with greater PWD speech/language and activities of daily living symptoms. Correlations with the seven individual caregiver outcome measures revealed that speech/language symptoms were the most robust predictors (correlated with five measures), followed by sleep and activities of daily living symptoms (correlated with two measures), and memory, visual/spatial, and motor symptoms (correlated with one measure).
Conclusions
Findings highlight the profound adverse effects that PWD speech and language deficits may have on caregivers and underscore the importance of addressing these deficits in dementia care.
Introduction
Dementia has become one of the major public health problems faced in countries across the world. In the United States alone there are an estimated 6.9 million people aged 65 and older living with Alzheimer's disease (AD). 1 Although AD often presents with memory problems, people with dementia (PWD) can experience a wide range of symptomatology in realms that span cognition, behavior, personality, emotion, motor functions, speech, and language. Loss of function in any of these areas can increase the overall burden placed on those providing care for PWDs, but the nature and amount of that burden, as well as strategies for management, can differ depending on the specific symptoms.2–4 Thus, a caregiver for a PWD with declining memory may need to be increasingly vigilant for failures to turn off appliances, whereas a caregiver for a PWD with increasing impulsivity and disinhibition in social situations may need to engage in compensatory actions to smooth over interpersonal miscues. Similarly, motor deficits can engender additional demand for physical assistance for activities of daily living, whereas problems with speech and language may require additional efforts in scaffolding communication between the PWD and others. 5 As dementia and caregiver research expands to incorporate other kinds of dementia in addition to AD (e.g., behavioral and language variants of frontotemporal dementia [FTD]), it becomes increasingly important that assessments incorporate the full range of dementia symptoms.
Impact on caregiver health and well-being
Given the aging population and the rising prevalence of dementia, caregiving has become an increasingly common part of family life. In 2022, there were more than 11 million family and other caregivers who provided an estimated 18 billion hours of informal (i.e., unpaid) caregiving valued at $339.5 billion. 1 While there are many positive aspects of caregiving, including a great deal of meaning and fulfillment,6,7 a large body of research shows that, compared to non-caregivers, family caregivers for PWDs suffer higher rates of burden, strain, depression, anxiety, loneliness, loss, and isolation.8–10 In addition, caregivers’ physical health can be adversely affected, with family caregivers for PWD having worse overall health,11,12 increased risk of mortality 13 and higher incidence of cardiovascular disease 14 and hypertension 15 compared to non-caregiving adults.
Efforts to understand the factors that influence the adverse effects of dementia caregiving have focused largely on the construct of “caregiver burden”, which is an umbrella term that encompasses the strain and stress involved in being a caregiver. 16 To achieve greater specificity in our understanding of the contributors to caregiver burden, research has examined the relative impact of different broad classes of PWD symptoms, with most studies17–21 finding that socially-inappropriate behavioral symptoms (e.g., lack of empathy, making tactless comments) are more burdensome for caregivers than cognitive symptoms (e.g., problems with memory or attention). This work begs the question of the relative contribution of other kinds of PWD symptoms (e.g., executive function, motor function, sleep disturbances, functional health and dependency, visual and spatial deficits, speech, and language) to caregiver burden, health, and well-being.
Impact on the PWD-caregiver relationship
Although much of the research on the impact of dementia on others has understandably focused on the health and well-being of caregivers, dementia also profoundly affects the relationship between the PWD and caregiver. Because many informal caregivers are spouses/partners, children, or friends of the PWD, a pre-dementia relationship typically exists that is rich in shared history, traditions, memories, rituals, divisions of labor, joys, and conflicts. Dementia can dramatically alter these as shared history and memories dim, traditional ways of interacting and sharing responsibilities change, and old joys and conflicts diminish while new ones arise. For these reasons, relationship dynamics and satisfaction can change in important ways.
In terms of relationship dynamics, AD couples have been found to be less interactive, with caregiving wives engaged in more strategies to facilitate communication on behalf of their husbands 22 compared to non-caregiving couples. In a study examining word usage during unrehearsed conversations, 23 both AD and FTD couples used more negative emotional words (e.g., words indicating anger and sadness) than non-caregiving couples, with FTD couples using more of these negative words than AD couples. In a related vein, spouses of individuals with primary progressive aphasia (PPA) have described the loss of communication with their partner as a primary theme in their caregiving experience. 24
In terms of relationship satisfaction, caregivers for PWD with FTD reported lower relationship satisfaction compared to AD caregivers and healthy control couples. 23 Loss of empathy by PWDs across all the dementias has been found to be highly predictive of marital dissolution. 25 In a review of 15 studies examining relationship quality between PWDs and their caregivers, several studies highlighted the association between behavioral symptoms and lower relationship satisfaction. 26
This relationship-focused research, combined with the previously reviewed research on caregiver health and well-being, makes a strong case for studying the impact of particular PWD symptoms on both the caregiver and the PWD-caregiver relationship.
Measuring PWD functioning
Examining the existing literature, most studies of PWD symptomatology have drawn from a small set of instruments to quantify different aspects of PWD functioning. 17 Thus, the Mini-Mental State Exam 27 and the Mattis Dementia Rating Scale 28 are often used to assess PWD cognitive functioning while the Neuropsychiatric Inventory 29 is used to assess PWDs’ problematic behaviors. One way to expand the scope of these assessments is to supplement them with other existing measures. For example, functional health and dependency could be measured using instruments such as the Lawton-Brody Instrumental Activities of Daily Living Scale 30 and the Disability Assessment Scale for Dementia. 31 Evaluations may also include tests specific to certain domains, such as speech, language, visuospatial attention and perception, or executive functioning. Although there are certainly advantages to continuing to build more comprehensive assessments of PWD functioning in this manner, it engenders problems with comparing scores across measures (e.g., dealing with differences in reference time periods, ratings of frequency versus intensity, etc.). In addition, the time demands placed on respondents when asked to complete so many different instruments can quickly become problematic.
An alternative approach that we adopted for the current study was to construct a single instrument asking caregivers to indicate the presence or absence of a list of PWD symptoms in a broad sampling of domains (i.e., memory, executive functioning, speech/language, visual and spatial, motor, changes in behavior, sleep, medical/sensory, and activities of daily living) over a common time period (i.e., currently). This approach has the advantage of encompassing a broad sampling of symptoms seen in many different types of dementia, facilitating comparisons across different symptom domains, and making the assessment less onerous for caregivers.
The present study
We compared the relative impact of multiple domains of PWD symptoms on both the caregiver and the PWD-caregiver relationship in a community sample of caregivers who were living with and serving as the primary care provider for a person who had received a diagnosis of dementia from a medical professional. We utilized existing data obtained from a randomized controlled trial evaluating a new system of in-home assistive technology for caregivers of PWDs. 32 Caregivers completed questionnaires regarding their own health and well-being, the quality of their relationship with the PWD, and the symptoms currently exhibited by the PWD for whom they were caring. Because of the critical role that disrupted communication can play in increasing caregiver burden and changing the nature of the PWD-caregiver relationship, we hypothesized that PWD speech and language symptoms would have strong associations with caregiver health and well-being as well as with the quality of the PWD-caregiver relationship.
Methods
Participants
Data used in this study came from participants recruited for a nine-month randomized controlled trial evaluating a newly developed in-home assistive technology system for dementia caregivers. 32 63 PWDs and their primary caregivers were recruited from two sources: (a) the Memory and Aging Center at the University of California, San Francisco (N = 11); and (b) a professional recruitment firm (Recruitment Partners) that specializes in populating clinical trials for AD and related dementias (N = 52). PWDs from the Memory and Aging Center were being seen as outpatients and expressed interest in participating in research projects. PWDs and their primary caregivers recruited by Recruitment Partners came from dementia care and caregiver support groups located in West Coast communities and PWDs were typically under the care of local neurologists and/or general practice physicians.
All research procedures were approved by the institutional review boards at the University of California, Berkeley and the University of California, San Francisco.
Measures
All participating caregivers completed a questionnaire battery prior to having the assistive technology installed in their home and being assigned to an experimental condition (described in greater detail below). The questionnaires assessed PWD and caregiver demographics as well as: (a) measures of caregiver health and well-being that are often used in the dementia caregiver literature, (b) commonly used measures of relationship quality and satisfaction, (c) caregiver ratings of the presence or absence of PWD symptoms.
Measures of caregiver health and well-being included:
Measures of the PWD-caregiver relationship included:
Caregivers also completed the PWD Symptom Inventory (Supplemental Material), a 54-item self-report scale assessing the presence of symptoms commonly seen in different kinds of dementia. We developed this inventory based on a review of symptoms included in the clinical interview used by the Memory and Aging Center as well as other commonly used dementia rating scales including the Quick Dementia Rating System 40 and the Clinical Dementia Rating scale. 41 Respondents rated each symptom as 0 (“Absent”) or 1 (“Present”) both for “now” and “when symptoms first began.” Only data from the “now” ratings were used for the present study.
Symptoms were chosen to represent nine areas of functioning: (a) memory (5 items, e.g., “Forgetful of names and faces of friends and family”); (b) executive functions (4 items, e.g., “Difficulties with planning and organization”; (c) speech/language (5 items, e.g., “Difficulty coming up with words in conversation”); (d) visual and spatial (5 items, e.g., “Difficulty reading a map, driving or parking, or seeing faces properly”); (e) motor (8 items, e.g., “Difficulty with walking or balance”); (f) changes in behavior (8 items, e.g., “Becoming more withdrawn”); (g) sleep (3 items, e.g., “Difficulty falling asleep”); (h) medical/sensory (8 items, e.g., “Bowel or bladder incontinence”); and (i) activities of daily living (8 items, e.g., “Difficulty dressing on their own”).
Procedures
An initial screening of potential participants was conducted to determine whether the following eligibility criteria were met: (a) the caregiver was the primary unpaid (“informal”) spousal or other adult familial caregiver living with a PWD and (b) the PWD had received a diagnosis of dementia from a medical professional. To be able to install the assistive technology later in the original study, homes had to have Wi-Fi and internet service and the caregiver had to have an iPhone and associated cellular service. Caregivers who met these criteria were asked to complete the baseline questionnaire assessment online. These baseline questionnaires were completed before the assistive technology system was installed and prior to the random assignment of participants to one of two experimental conditions (i.e., fully functional system or limited function system).
The clinical trial lasted for a total of nine months with the questionnaire package administered again at three, six, and nine months. Because these additional questionnaire administrations occurred after the installation of the systems and assignment to experimental conditions, participants in the two conditions were no longer being treated in the same way. Thus, for the present paper we only used data from the initial baseline questionnaire data.
Participants were paid $175 for their participation in the nine-month study (prorated if all questionnaires were not completed) and were provided with the assistive technology system without charge.
Data analysis
To deal with possible missing data and with different numbers of items in the PWD Symptom Inventory subscales, we computed average item scores (sum of answered items/total number of items answered) for all measures and used these average item scores in all subsequent analyses.
To control for Type I error due to having seven outcome measures, we conducted an exploratory factor analysis with SPSS (version 29) using principal axis factoring. The KMO measure of sampling adequacy was 0.76 and Bartlett's test of sphericity was significant, χ2(21) = 153.66, p < 0.001, confirming the appropriateness of factor analysis. Examining the scree plot, there were two factors with eigenvalues greater than 1 (eigenvalues = 3.46 and 1.18, respectively). This two-factor solution accounted for 66.3% of the total variance.
An Oblimin rotation yielded the following factor loadings (in parentheses) for two factors that we termed: (a) “General Distress” consisting of Depression (0.822), Anxiety (0.821), General Health (−0.723), Loneliness (0.660), and Burden (0.652); and (b) “Relationship Quality” consisting of Relationship Satisfaction (0.836), and Interpersonal Closeness (0.198). Using the regression method, two factor scores were calculated for each participant representing the degree to which they exhibited the latent constructs of General Distress (larger scores indicate greater distress) and Relationship Quality (larger scores indicate greater quality). The factors were significantly correlated, r(52) = −0.39, p = 0.004.
We then conducted two linear regression analyses with the two factor scores serving as dependent measures and the average symptom scores for the nine areas of functioning (memory, executive functions, speech/language, visual and spatial, motor, change in behavior, sleep, medical/sensory, activities of daily living) on the PWD Symptom Inventory as predictors (all entered together on the same step). Using the Beta coefficients and associated t-tests, we identified PWD symptoms that significantly predicted each of the factor scores.
We also conducted two additional exploratory analyses. First, to ensure that our regression analyses fairly reflected the underlying pattern of associations between PWD symptoms and caregiver outcomes, we computed zero-order correlations between the nine PWD symptom scores and the scores on each of the seven caregiver outcomes. Second, for PWD symptom scores that emerged as significant predictors in our regression analyses, we conducted additional regression analyses examining the contributions of the individual symptoms that were averaged to derive the symptom scores.
Results
Of the 63 participants who participated in the study, 54 had data for all nine PWD symptom scores and all seven caregiver outcome measures. Thus, subsequent analyses were conducted using only these participants.
Preliminary analyses
Demographic data indicated that the sample of caregivers used in the analyses was primarily older (mean age = 65.7), female (72.2% female), well-educated (59.3% completed at least four years of year college), above median income (50% had a household income over $75,000), and white/European American (68.5% non-Hispanic White or European American). Caregivers were primarily spouses or partners of PWDs (70.4%) or their adult children (22.2%). Additional details concerning sample demographics are presented in Table 1.
Caregiver demographics.
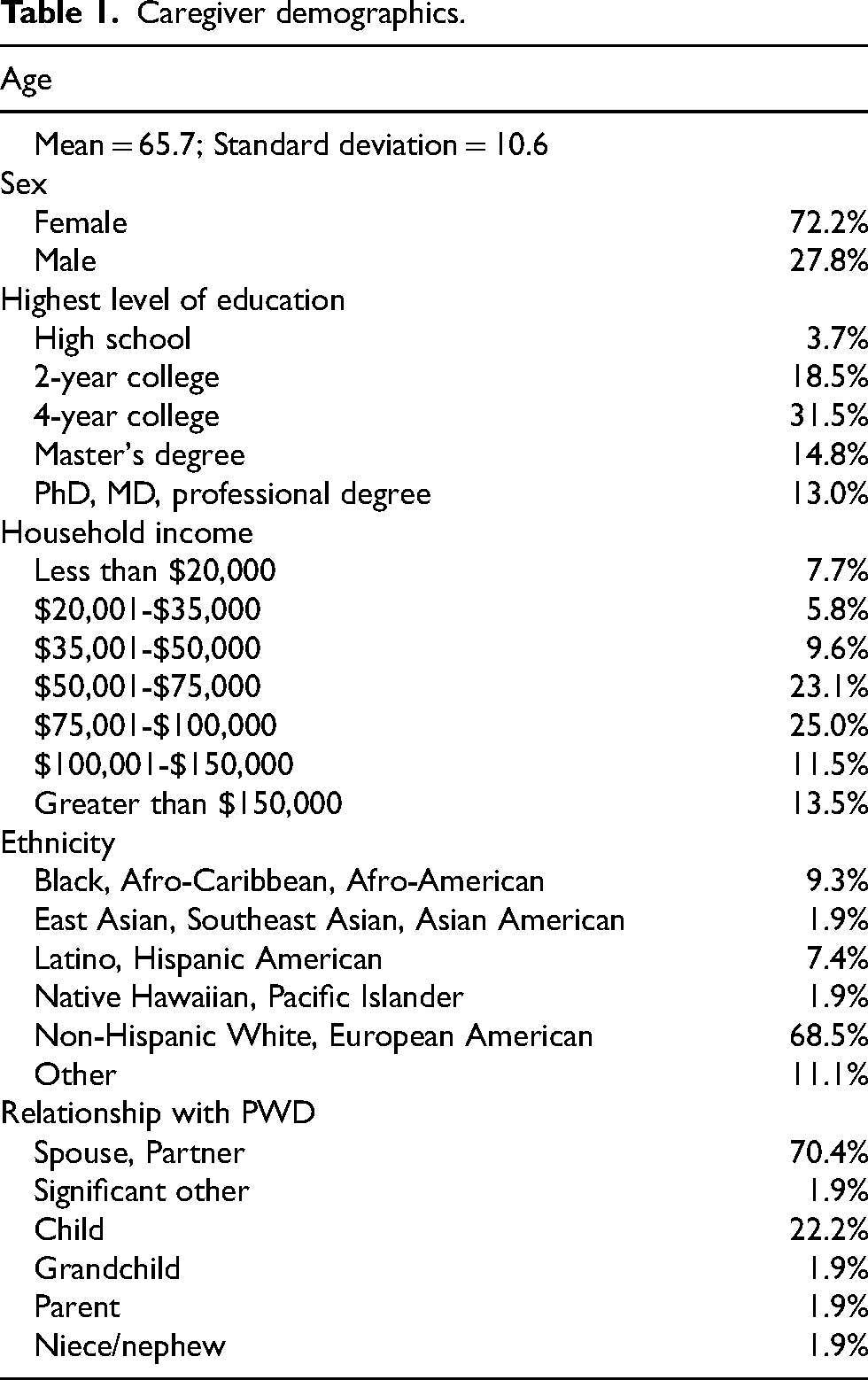
PWD diagnoses were obtained from caregivers based on information they reported receiving from a medical professional. All participants received a diagnosis of dementia. Major diagnostic categories were AD (61.1%), FTD (14.9%), Dementia with Lewy bodies (9.3%), and Parkinson's disease (7.4%).
Summary statistics for the PWD Symptom Inventory and caregiver outcome measures are presented in Table 2.
PWD Symptom Inventory and caregiver outcome measures.

PWD symptoms and caregiver outcomes
For the caregiver General Distress factor, the association with the full set of nine PWD symptom categories was significant, R2 change F(9,44) = 2.82, p = 0.011, R2 = 0.37, adjusted R2 = 0.24. Examining the individual symptom category scores (Table 3), greater General Distress was associated with more PWD speech/language symptoms, Beta = 0.54, t = 3.54, p < 0.001, and more PWD sleep symptoms, Beta = 0.34, t = 2.50, p = 0.016.
PWD symptoms Beta coefficients in regression analyses for caregiver General Distress and Relationship Quality factor scores.
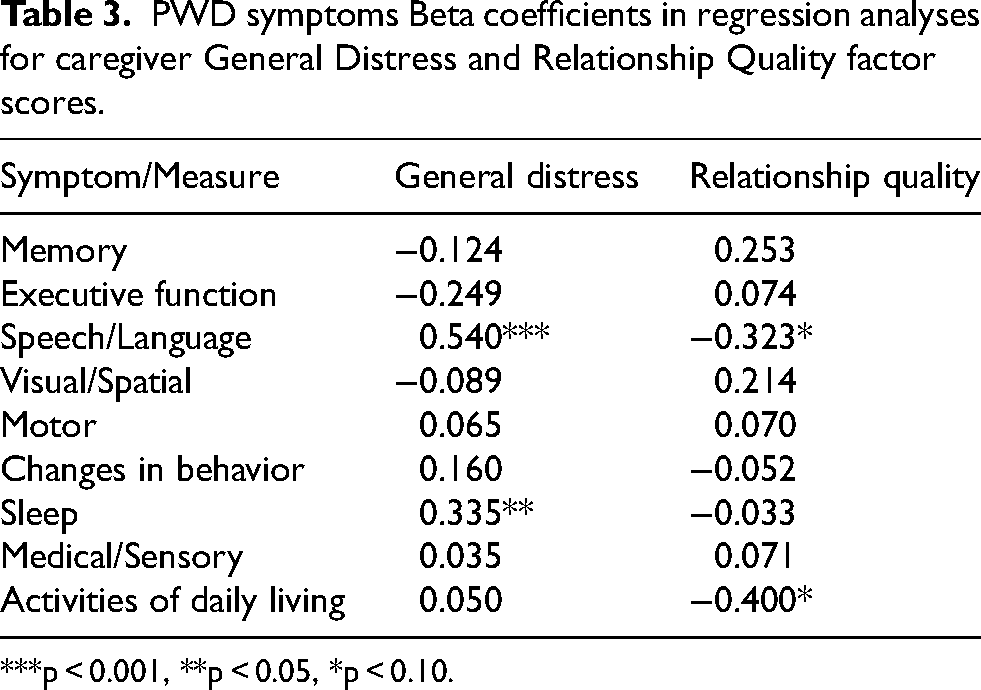
***p < 0.001, **p < 0.05, *p < 0.10.
For the caregiver Relationship Quality factor, the association with the full set of nine PWD symptom categories was not significant, R2 change F(9,44) = 1.53, ns, R2 = 0.24, adjusted R2 = 0.08. Examining the individual symptom category scores (Table 3), there were trend-level (p < 0.10) associations between greater Relationship Quality and fewer PWD speech/language symptoms, Beta = −0.32, t = −1.93, p = 0.060, and fewer PWD problems with activities of daily living, Beta = −0.40, t = −1.78, p = 0.081.
Additional analyses
Zero-order correlations. Predictors of outcomes that are significant in univariate analyses can become non-significant when entered in regression analyses along with more powerful predictors with which they share variance. To determine whether our regression approach distorted the pattern of associations between the PWD symptom categories and caregiver outcome measures, we examined the zero-order correlations between the nine PWD symptom categories and the seven caregiver outcome questionnaires (Table 4).
Zero-order correlations between PWD symptom categories and caregiver outcome measures.
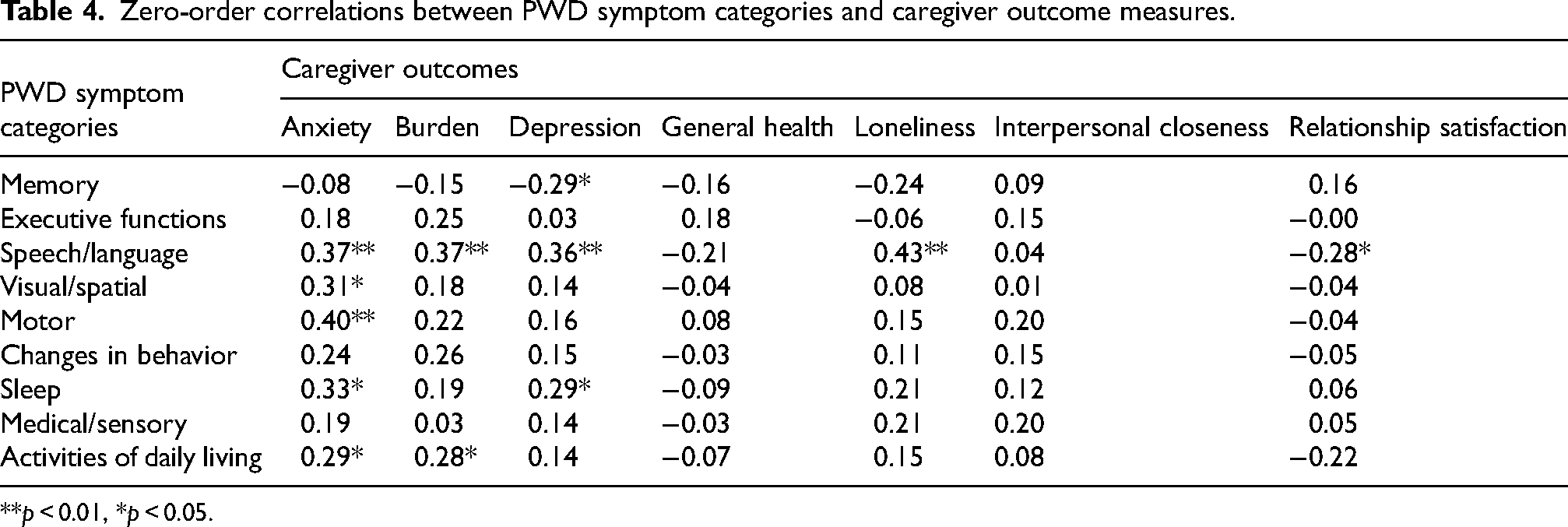
**p < 0.01, *p < 0.05.
Speech/language symptoms emerged as the most frequent predictor of caregiver outcomes, significantly predicting five of the seven caregiver outcomes (predicting anxiety, depression, loneliness, burden, and relationship satisfaction). This was followed (in descending number of significant associations) by sleep symptoms (predicted anxiety, depression), activities of daily living symptoms (predicted anxiety, burden), memory symptoms (predicted depression), visual and spatial symptoms (predicted anxiety), and motor symptoms (predicted anxiety).
Examining these data in terms of caregiver outcomes most frequently associated with PWD symptoms, anxiety (five significant associations) was most likely to be associated with PWD symptoms. This was followed (in descending number of significant associations) by depression (three significant associations), burden (two significant associations), and loneliness and relationship satisfaction (one significant association each).
Individual speech/language and sleep symptoms. As described earlier, we conducted separate regression analyses with the individual symptoms where the symptom category was a significant predictor of caregiver General Distress (predicted by PWD speech/language and sleep symptoms).
For caregiver General Distress factor, the association with the set of five speech/language symptoms entered together was significant, R2 change F(5,47) = 3.93, p = 0.005, R2 = 0.30, adjusted R2 = 0.22. Examining individual speech/language symptoms, greater caregiver general distress was associated with greater difficulty reading, writing, or spelling, Beta = 0.32, t = 2.21, p = 0.032, and greater slurred speech, Beta = 0.27, t = 2.10, p = 0.041. In this regression model, associations were not significant for difficulty coming up with words in conversation, Beta = 0.23, t = 1.60, ns, halting or stuttering in speech, Beta = −0.09, t = −0.65, ns, or difficulty understanding words or concepts in a conversation, Beta = −0.02, t = −0.17, ns.
For the caregiver general distress factor, the association with the set of three sleep symptoms entered together was also significant, R2 change F(3,49) = 3.52, p = 0.022, R2 = 0.18, adjusted R2 = 0.13. Examining individual sleep symptoms, greater caregiver general distress was associated with greater re-enacting dreams during sleep (e.g., arm and leg movement), Beta = 0.40, t = 3.01, p = 0.004. In this regression model, associations were not significant for difficulty staying asleep, Beta = 0.19, t = 1.31, ns, or difficulty falling asleep, Beta = −0.03, t = −0.19, ns.
Discussion
We examined the associations between nine categories of PWD symptomatology (memory, executive functions, speech/language, visual/spatial, motor, behavior, sleep, medical/sensory, activities of daily living) and seven caregiver outcomes (anxiety, burden, depression, general health, loneliness, interpersonal closeness, relationship satisfaction). Primary analyses were conducted using factor scores representing two latent constructs derived from exploratory factor analysis (caregiver General Distress and Relationship Quality) with follow-up analyses conducted using the individual caregiver outcome measures. The present study differed from most existing studies linking PWD symptoms with caregiver outcomes in the breadth of PWD symptoms and caregiver outcomes considered. Previous research has typically focused on one or two kinds of PWD symptoms (e.g., memory and behavior) and a measure of caregiver burden.17,21 Our evaluation of a more diverse set of PWD symptoms and caregiver outcomes enabled a more differentiated view of the relative impact of particular PWD symptoms.
Our hypothesis that PWD speech/language symptoms would be associated with the health and well-being of caregivers was strongly supported. There was also evidence, although not as strong, supporting the hypothesis that PWD speech/language symptoms would be associated with the quality of the PWD-caregiver relationship. Moreover, several strands of evidence indicated that PWD speech/language symptoms were the most robust predictor of adverse caregiver outcomes in this study. In the analyses of the General Distress and Relationship latent construct factor scores, speech/language symptoms were the most powerful of the two significant predictors of Caregiver Distress (Betas: speech/language = 0.54; sleep = 0.34) and, along with activities of daily living, were the only symptom categories that predicted Relationship Quality (albeit at trend levels). A similar pattern emerged in the zero-order correlations between PWD symptoms and individual caregiver and PWD-caregiver relationship measures. In these analyses, PWD speech/language symptoms were significantly associated with five of the seven caregiver outcome measures (associated with anxiety, burden, depression, loneliness, and relationship satisfaction). In comparison, among the other symptom categories, PWD sleep symptoms and activities of daily living symptoms were each associated with two outcome measures (i.e., sleep was associated with anxiety and depression; activities of daily living were associated with anxiety and burden), visual and spatial symptoms and motor symptoms were each associated with one outcome measure (anxiety), and changes in behavior, medical/sensory, and executive functioning symptoms were not significantly associated with any outcome measures. Importantly, these zero-order correlations revealed that PWD language symptoms were related both to adverse caregiver outcomes (e.g., greater anxiety, depression, and burden) and adverse PWD-caregiver relationship outcomes (lower relationship satisfaction).
Examining the individual speech/language symptoms revealed that “difficulty reading, writing, or spelling” and “slurred speech” were associated with greater caregiver General Distress. Notably, these symptoms can occur in several types of dementia and are overt signs of communication deficits, making them likely to be both evident and concerning to caregivers. Difficulty in finding or understanding words in conversation are other symptoms commonly found in language disorders. However, individuals can often mask these problems by finding acceptable substitutions or simply pretending to understand, which may help explain why these symptoms were not associated with caregiver General Distress.
The impact of speech and language deficits on caregivers
Speech and language problems are found in many kinds of dementia and are often the catalyst for seeking medical advice. For example, word finding problems are often among the earliest-appearing symptoms in AD.42,43 In the logopenic form of PPA, typically associated with AD pathology, pauses during speech and naming deficits emerge as early symptoms and problems such as difficulty repeating longer phrases and sentences emerge later. 44 Similarly, in FTD, speech and language problems are prominent features of both the non-fluent/agrammatic and semantic variants of PPA. Typically, effortful/halting speech and simplified grammar emerge early in non-fluent/agrammatic PPA whereas word-retrieval difficulties emerge early in the semantic variant; over time, other aspects of speech and language are also affected. 45 PWDs diagnosed with dementia with Lewy bodies or those with Parkinson's disease often exhibit dysarthric speech, with errors in articulation 46 that can affect intelligibility.
PWD speech and language problems have been found in numerous studies to impact caregiver health and well-being profoundly as well as affecting the quality of the PWD-caregiver relationship. In a study of 50 families, 47 communication difficulties were observed in 68%. In a synthesis of 16 studies that interviewed spousal caregivers of a PWD, 24 a recurring theme was “loss of partner,” including a decline in usual conversations that affected the quality of the relationship. In a review of a different set of nine studies, 48 the authors found a similar theme of loss experienced by family members in how they typically communicated with the PWD. Importantly, breakdowns in communication can also lead to problem behaviors such as frustration and anger when PWDs can no longer express themselves, resulting in additional caregiver burden. 49
Families deal with language decline in dementia in different ways. This can include changes in identity around the assumption of family responsibilities, loss of complexity and connection in the relationship, and developing new strategies for communication.48,50 Caregivers, who spend the most time with the PWD often find themselves in the position of interpreter not only in their own interactions with the PWD, but also for friends, family, and care providers. Spouses of persons with PPA may report experiencing a profound disconnection in the relationship and readjusting their sense of self while “getting on with living”. 24
The importance of speech and language symptoms
Although we had hypothesized that speech/language symptoms in PWD would be associated with caregiver health and well-being and with the quality of the PWD-caregiver relationship, we did not predict that these symptoms would emerge as the most robust predictors. In retrospect, this finding is not completely surprising.
In terms of effects on caregivers, subtle language changes in PWD can be associated with lower caregiver well-being (e.g., less use of “we” pronouns and greater use of “I” pronouns 51 ). Research on people with aphasia due to stroke underscores the profound impact that speech and language deficits in the patient can have on caregivers. In these studies, caregivers were found to suffer from depression, anxiety, fatigue, strained marital relationships, feelings of burden or grief, and/or changes in their own health.52–54 Although some of these adverse effects on caregivers likely reflect the more general challenges of caring for someone who has physical, cognitive or behavioral problems after a stroke, language deficits themselves are often implicated. For example, in a study comparing caregivers for people who were aphasic versus non-aphasic following stroke, 55 caregivers for those with aphasia reported difficulty with communication, understanding, the need to speak on the person with aphasia's behalf and losses in their own social network as caregiving responsibilities consumed more of their time and attention. Importantly, language symptoms induced by stroke may ultimately plateau and/or improve over time. In contrast language symptoms caused by dementia are likely to continue to worsen, thus adding to the burden of caregivers over even longer periods of time.
In terms of effects on the PWD-caregiver relationship, most researchers and clinicians would agree that language is a crucial aspect of interpersonal connection. Language supports emotional intimacy; the sharing of thoughts; verbalizing feelings, needs, and expectations; revealing preferences; and many other aspects of relational discourse. When neurological disease impacts the language abilities of one member of a dyad, it fractures a vital connection, inevitably altering the dynamics of the relationship.23,24,50,56 Conversations become more one-sided, with the burden of communication shifting to the caregiver. Thoughts and ideas cannot be shared as they once were, leaving a void where information was once easily exchanged. The pace of communication can slow as listeners interrupt with questions and requests for clarification. All of this can erode the quality of the relationship for the caregiver, with attendant decreases in relationship satisfaction.
Finally, we should note that our findings did not support previous findings that underscored the importance of behavioral symptoms for caregiver health and well-being (e.g., Chiao, Wu, & Hsiao 17 ; Ornstein & Gaugler 21 ). We expect that this may have resulted from prior studies including a larger and more diverse set of symptoms in their behavioral category. In our study, some of these symptoms were instead included in other symptom categories.
Utility of the PWD symptom inventory
Our findings indicate that having caregivers rate the presence of a broad sampling of PWD symptoms can be useful in research examining the relative impact of different kinds of PWD symptoms on caregiver health, well-being, and relationship quality. These caregiver ratings could also prove useful in other kinds of dementia research. After all, caregivers arguably spend more time with PWD and observe them across a wider range of settings than anyone else. Although there are certainly reasonable concerns to be raised with the objectivity and accuracy of caregiver ratings given personal involvement, fatigue, enmeshment, depression, anxiety, and other factors, we have generally found caregiver ratings to be very useful. For example, we have found that caregiver ratings of PWDs’ emotional functioning (e.g., ability to generate emotional responses and recognize emotions in others) are strongly related to both self-report and more objective measures of caregiver health. 57
Findings from the present study clearly indicate that PWD speech/language symptoms should be adequately represented when assessing PWD functioning in relation to caregiver well-being and relationship satisfaction. Although comprehensive evaluations of communicative functioning should be part of any assessment battery for PWD with speech or language symptoms, there is a need for fast and efficient screening instruments by caregivers that can provide early insights into the speech/language decline. The Quick Dementia Rating Scale, 40 which is often used to rate functional abilities in PWDs, does include a language domain. However, it focuses on the impact of word-finding (which is common in Alzheimer's disease) but doesn’t include other speech/language symptoms that might be found in other forms of dementia (e.g., in language variants of frontotemporal dementia). Our PWD Symptom Inventory obviously cannot substitute for a comprehensive clinical evaluation, but it does include a broader array of speech and language symptoms in addition to word-finding problems (i.e., halting or stuttering in speech, slurred speech, word comprehension, and difficulty reading, writing, or spelling). In this way, it may provide a quick initial assessment of communication deficits seen in a wide range of dementias, which can be augmented, when possible, by a full assessment conducted by a speech-language pathologist.
Implications for interventions
Our findings may help inform the development of interventions designed to improve PWD-caregiver communication and preserve the quality of the PWD-caregiver relationship. Based on our findings that PWD speech/language symptoms are significant contributors to both adverse caregiver and PWD-caregiver relationship outcomes, interventions targeting dyadic communication may help reduce these adverse outcomes. Several interventions have been developed that target communication deficits in PWD58,59 caregivers in their roles as communication partners,60,61 the quality of conversation and communications in dyads,62–64 and psychoeducation to increase understanding of progressive language disorders.61,65 Given the present findings, it would be very useful to assess the impact of these interventions on caregiver health and well-being as well as on the PWD-caregiver relationship.
Strengths and limitations
The present study had several strengths including: (a) sampling a broader range of PWD symptoms and caregiver and PWD-caregiver relationship outcomes than in most previous research; (b) including analyses that compared types of PWD symptoms to determine their relative associations with caregiver and relationship outcomes; and (c) having a participant sample with reasonable diversity in dementia diagnoses, caregiver gender, caregiver relationships (spousal/partner, child), recruitment sources (university-based dementia center, community-based caregiver groups), and ethnicity (31.5% were not white/European American).
The research had limitations as well. While our sample generally reflects current caregiving demographics in the United States 1 in terms of gender (72.2% female in our sample versus 67% overall) and ethnicity (68.5% White in our sample versus 66% overall), several characteristics of the sample could raise concerns about generalizability. Our sample was geographically limited to California and other west coast states and was skewed toward higher SES status in terms of income and education. In addition, because of our recruitment strategy, caregivers in our sample were more likely to be spouses and partners of PWDs (70.4% spousal/partner in our sample versus 60% overall). Importantly, our participants were all enrolled in a randomized controlled trial 32 evaluating a new system of in-home technology designed to provide caregivers with warnings about worrisome events (e.g., PWD falls and wandering). Although the data used for the present study were all collected at the initial baseline, before the assistive technology systems were installed and before participants were randomly assigned to the active or control arms of the intervention, the sample might have differed from a truly random sample of caregivers in areas such as openness to technology and concerns with monitoring PWD safety. In this regard, it is interesting to note that our zero-order correlational analyses of individual caregiver outcome measures revealed that anxiety had the largest number of significant associations with PWD symptoms. Another issue was the possible restriction of variance resulting from using binary (present/absent) ratings for the various symptoms in the PWD Symptom Inventory. In subsequent research, we have modified the inventory to have caregivers rate the extent to which each symptom is present using a 5-point Likert scale ranging from 1 (“never”) to 5 (“always”). Another area of concern was that our measure of Interpersonal Closeness did not have a very high loading (i.e., 0.20) on our Relationship Quality factor. In future work, alternative measures should be sought that improve measurement of this important construct. Finally, although our sample size was reasonable for examining the association between PWD symptoms and our caregiver and PWD-caregiver relationship outcome measures, a larger sample could: (a) provide greater confidence in the robustness of the factor analysis we conducted to reduce the number of variables in our primary analyses; (b) elucidate additional and more nuanced relationships among our measures; and (c) examine effects of important moderators (e.g., diagnosis, gender, spousal versus adult child caregivers), which may reveal subgroups with stronger and weaker relationships between PWD symptoms and caregiver outcomes.
Summary
In a sample of individuals providing primary care for a PWD, results indicated that PWD speech/language symptoms were particularly important predictors of caregiver health and well-being and the quality of the PWD-caregiver relationship. Language, both spoken and written, is a fundamental way that couples share important information about their relationship, such as their daily activities, finances, raising their children, or planning for the future. Attention to the impact of speech and language deficits is critical to inform the development of targeted and effective interventions to promote caregiver health and well-being and to protect the health of the PWD-caregiver relationship.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251340578 - Supplemental material for Associations between dementia symptoms and caregiver and relationship health: A prominent role for speech and language
Supplemental material, sj-docx-1-alz-10.1177_13872877251340578 for Associations between dementia symptoms and caregiver and relationship health: A prominent role for speech and language by Robert W Levenson, Jennifer Merrilees, Maya L Henry and Nina F Dronkers in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors thank the caregivers who participated in this study and our laboratory members who helped with the data collection.
Ethical considerations
All research procedures were approved by the institutional review boards at the University of California, Berkeley and the University of California, San Francisco.
Consent to participate
All participants provided written consent for participating in the research.
Consent for publication
All participants provided written consent for using their data in publications.
Author contributions
Robert Wayne Levenson (Conceptualization; Formal analysis; Investigation; Methodology; Writing – original draft; Writing – review & editing); Jennifer Merrilees (Conceptualization; Investigation; Methodology; Project administration; Writing – review & editing); Maya L Henry (Conceptualization; Investigation; Methodology; Writing – review & editing); Nina F Dronkers (Conceptualization; Methodology; Writing – review & editing).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by NIA grants R01AG041762 and SB1AG059458 to Robert W. Levenson, NIA grant R01AG062639 to Jennifer Merrilees, NIDCD grants R01DC016291 and R56DC016291 to Maya Henry, and NIDCD grant R21DC021042 to Nina Dronkers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.