
Abstract
Background
Non-Hispanic Black and African American men are more likely to have Alzheimer's disease (AD) than non-Hispanic White peers. Despite this, little is known about how Black and African American men perceive dementia risk, which is foundational to prevention.
Objective
Acknowledging that personal vantage point influences behavior, our study examined Black and African American male perceptions about their anticipated risk for AD.
Methods
We conducted a secondary analysis of Black and African American adult male responses to the Recruitment Innovations for Diversity Enhancement electronic survey study. We examined associations between perceived risk of AD and age, education, employment status, household income adequacy, marital status, living status, prior experience with AD, and subjective memory performance using generalized linear models.
Results
Respondents (n = 112) were age 18 to 79 years (M = 51.05, SD = 13.44), and 35% reported prior experience with AD through a friend or family member. Respondents’ perceived risk of developing AD ranged from 0 to 100% (M = 33.46, SD = 28.29). Spearman rho correlations revealed modest but significant correlations between perceived risk and age (r = 21, p = 0.03) and marital status (r = -0.22 p = 0.02). The best fitting generalized linear model revealed low perceived risk for AD was associated with younger age, income adequacy and being married or living as married (χ 2 = 8.76, p = 0.03).
Conclusion
Selected social determinants of health were associated with perceived risk. Future studies should examine additional social determinants of health (e.g., social and physical environment) and measures of cognitive and physical health to further explore relationships with perceived risk of AD in Black and African American males.
Keywords
Introduction
For decades society has assigned stereotypes and gendered roles to Black and African American men leaving these men to feel “invisible”. 1 The overall health of the Black and African American adult male, the invisible man, has been consistently ranked the lowest across racial and ethnic groups in the United States.1,2 With regard to cognitive health, there is a paucity of scientific research involving the Black and African American male adult population, specifically as it relates to Alzheimer's disease. The preservation of brain health for Black and African American men is contingent upon examining and mitigating cognitive health disparities experienced by this community.
Alzheimer's disease has one of the highest incidence rates among persons who identify as Black or African American, twice that of non-Hispanic White peers.3,4 Furthermore, Alzheimer's disease is diagnosed in later stages with greater severity among members of minority racial and ethnic communities, specifically the Black and African American community, compared to non-Hispanic White communities. 5 Multiple overlapping factors contribute to this health disparity, including the lack of Alzheimer's disease and related dementia awareness, absence of preventive screenings and early detection in historically minoritized communities, as well as contributions from the social determinants of health.6–9 The contributions from the social determinants of health include socioeconomic (e.g., income, education) and psychosocial factors (e.g., marital status, living status) which have been well documented to influence both physical and mental health. Further, estimates of the incidence and prevalence of Alzheimer's disease among Black and African American men are likely to be confounded by methodological issues with cognitive screening that have resulted from female gender bias and sociocultural bias in screening tool development research.10,11
At a fundamental level, even less is known about the subjective perspectives of Black and African American men with respect to Alzheimer's disease. Understanding perceived risk for dementia among Black and African American men is a crucial first step in planning potential health promotion programs. Mounting evidence illustrates the relationship between perception of risk, social determinants of health and health behaviors as well as the difference in perception between racial and ethnic groups.12,13 Analyses from the Health and Retirement Study (2012–2022) found a link between perceived risk of developing Alzheimer's disease and performance on assessments of cognitive function. 14 Perceived risk for a condition has also often been associated with actions taken to mitigate or manage the health condition; thus, underscoring the importance of examining the perceived risk of Alzheimer's disease from the unique perspective of Black and African American men. 15
Many researchers have called for an examination of the relationships between perceived risk for Alzheimer's disease and intersecting variables such as Alzheimer's disease and related dementias with education, preventive screening and early detection or Alzheimer's disease and contributions from the social determinants of health (e.g., economic stability, neighborhood and physical environment, education, food, community and social context, health care system) but few studies have answered the call.16,17 This analysis examined Black and African American men's perceived risk of developing Alzheimer's disease in the next 10 years, as well as potential relationships between perceived risk and selected social characteristics, prior experience witnessing Alzheimer's disease in a friend or family member, and subjective memory performance. This analysis is a first step toward future studies examining associations among social characteristics, the social determinants of health, and perceived risk of Alzheimer's disease for Black and African American men. This line of inquiry has the potential to advance science by creating culturally inclusive and responsive educational materials, increasing engagement in cognitive assessments among Black and African American adult men and earlier diagnosis of Alzheimer's disease and related dementias.
Methods
Design
We conducted a secondary analysis of baseline data collected for the Recruitment Innovations for Diversity Enhancement (RIDE) study. 18 The parent study, RIDE, was a web-based study of factors associated with an interest in Alzheimer's disease research among Black or African American adults.18,19 Survey data were collected from October 16, 2020 to September 3, 2021. For the secondary analysis in the current study, we examined baseline values of selected variables collected in the RIDE study to focus on whether social characteristics, prior exposure to Alzheimer's disease through a friend or family member, or subjective memory impairment were associated with perceived risk of acquiring Alzheimer's disease. All variables examined in this analysis were collected at baseline in the RIDE study, prior to exposure to any materials designed to influence interest in research participation. This study received ethical approval from the University of Pittsburgh Institutional Review Board (approval #STUDY20030044) on August 19, 2020.
Participants
The RIDE study recruited 500 community-based male (n = 114) and female (n = 386) participants who responded to a web-based advertising campaign, email communications to community partners, direct mailings, and a university-based research registry. Participants in the secondary analysis (n = 114) were limited to persons who self-identified as a) Black or African American, b) male, c) residents of one of the seven counties of a city located in the southwestern Pennsylvania region, c) age 18 years and older and e) able to read English.
Measures
Participants were asked to self-administer a battery of assessments before watching a two-minute video sharing the details of a research participant's experiences who self-identified as Black or African American.
Social characteristics were self-reported and included age, education level, marital status, living status, employment status, household income adequacy, and prior experience with Alzheimer's disease through a friend or family member. Age was reported in years. Education, marital status, living status, employment status, household income, and prior experience with Alzheimer's disease were reported by selecting from categories on the survey. For the purposes of these analyses, each of these independent variables were dichotomized (education level: high school or less, more than high school; marital status: not married or living as married, married or living as married; living status: living alone, not living alone; employment status: less than full-time, full-time employment; household income adequacy: inadequate, adequate; prior experience: no, yes). The examination of listed variables aligns with previous studies that established a baseline of the public's perceptions about cognitive health and Alzheimer's disease.20,21 Similarly, exploring the relationships between these variables’ perception and the social determinants of health can advance the science by discerning if previous findings are generalizable to a population of racial and ethnic minorities (Black and African American adult men) located in the Southwestern Pennsylvania region.17,22,23
Subjective memory performance was an additional independent variable that was assessed through nine items modified from the 33-item Frequency of Forgetting Scale. 24 The nine items were summed to generate a total score, with higher scores indicating better subjective memory performance.
Perceived risk of developing Alzheimer's disease in the next 10 years was assessed using a single-item approach which was previously employed by Chung et al. (2009) when used to assess perceived risk of developing Alzheimer's disease with participants (n = 778). 25 Participants were asked to report a whole number on a scale of 0 (no chance) to 100 (absolutely certain). This score was used as the dependent variable in the analysis. This score was used as the dependent variable in the analysis. 25
Analysis
Only participants who provided a perceived risk score were included in the analyses. Descriptive analyses (plots, frequencies) were generated using IBM SPSS Statistics version 27 to assess distributions of all variables and normality of the continuous variables (perceived risk, age, and frequency of forgetfulness). 26 The dependent variable, perceived risk for Alzheimer's disease, was not normally distributed. Thus, bivariate relationships among the dependent variable and independent variables (age, education, marital status, living status, employment, income adequacy, prior experience with Alzheimer's disease, and subjective memory performance were assessed using Spearman's Rho correlations. We then assessed multivariate associations among independent variables and the dependent variable with generalized linear models using a negative binominal distribution. We decided a priori to run two models: Model 1 assessed the associations with all predictors (age, education, living status, marital status, employment, income adequacy, prior experience with Alzheimer's disease, frequency of forgetfulness score). Model 2 assessed associations with significant predictors from Model 1. Alpha was set at p < .10 given the exploratory nature of the analysis. We selected the best fitting model based on the lowest values for the Akaike information criteria and Bayesian information criteria.
Results
Of the 114 participants in the sample, 112 participants completed all questions in the electronic survey (Table 1). More than 90% reported having at least some college education or more. Participants ranged in age from 18 to 79 years of age with a mean age of 51.05 (SD = 13.44). Only 49% of the participants reported being married and 35% reported living with someone. Less than half of the participants (47%) reported having full-time employment while most participants (90%) reported that their income met their basic needs. More than one-third (35%) of participants reported prior experience with Alzheimer's disease through a friend or family member. Participants reported a moderate amount of subjective memory impairment (M = 52.57, SD = 10.48). The mean perceived Alzheimer's disease risk in the next 10 years was 33 on a 100 point scale (SD = 28.29).
Participant characteristics (n = 112).*
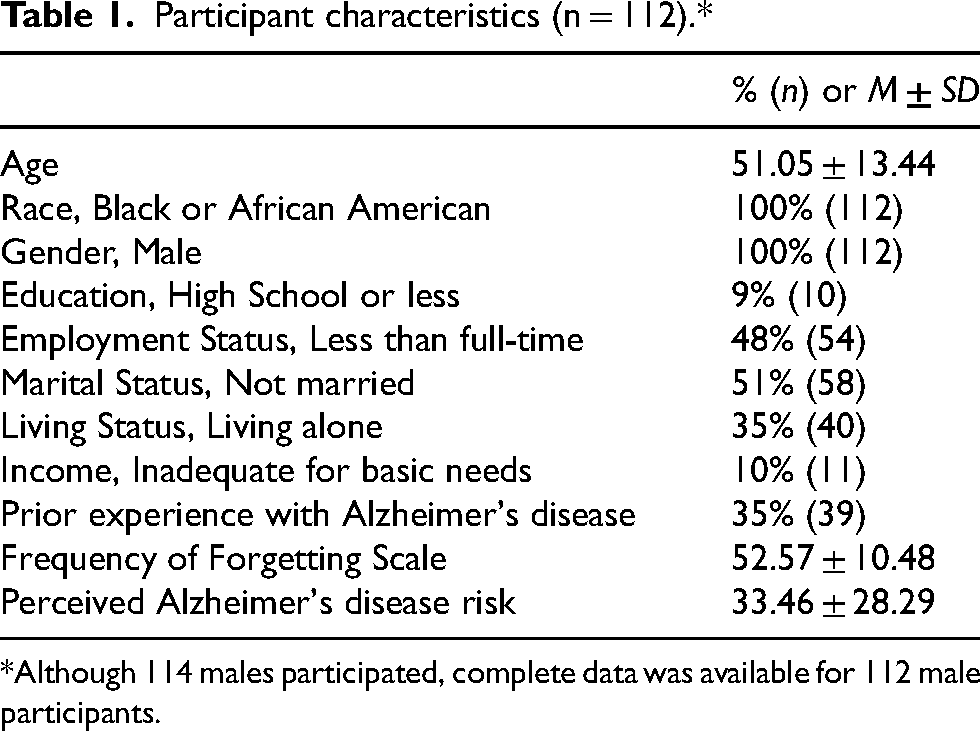
*Although 114 males participated, complete data was available for 112 male participants.
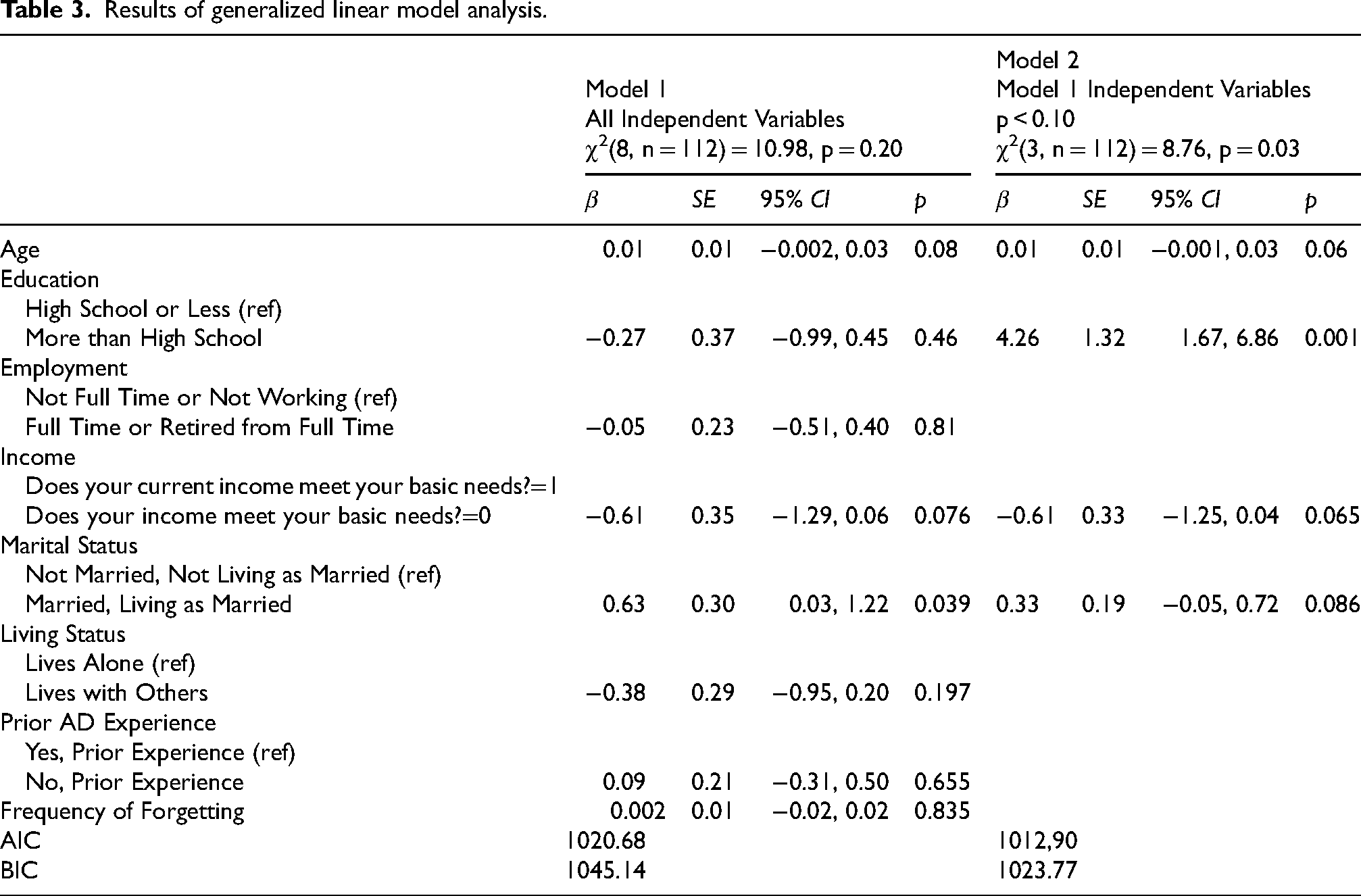
Spearman correlations indicated that age and marital status were significantly but modestly correlated with perceived risk for Alzheimer's disease (Table 2). All other bivariate relationships were negligible. Multivariate analyses with all variables in Model 1 revealed that younger age, income adequacy and being married or living as married were associated with low perceived risk of developing Alzheimer's disease within 10 years. In Model 2, these same variables were associated with low perceived risk. Model 2 was the best fitting model based on Akaike and Bayesian information criteria (Table 3).
Correlations between potential predictors and perceived risk for Alzheimer's disease.
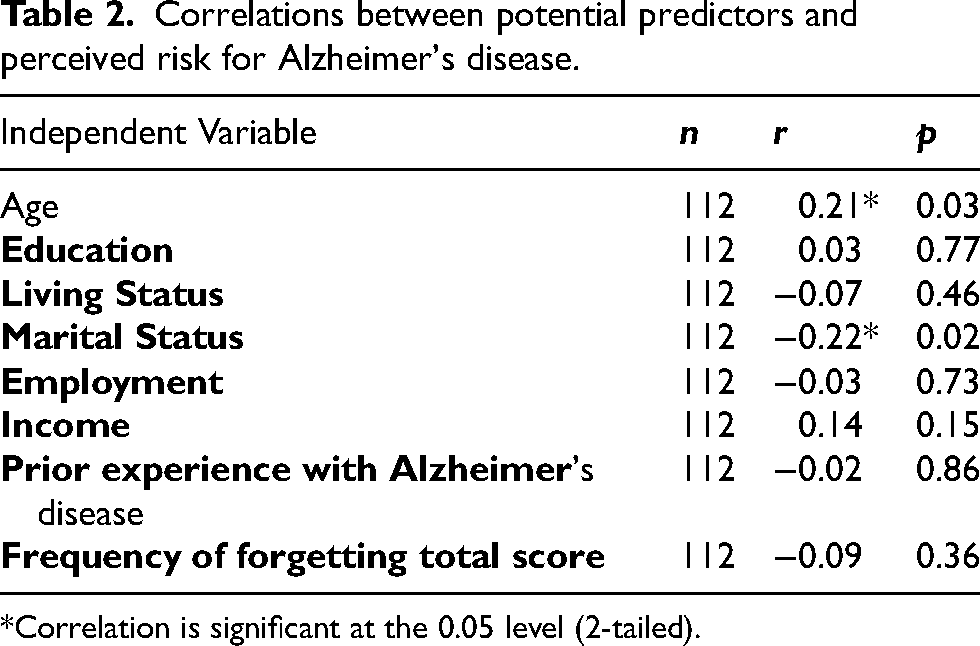
*Correlation is significant at the 0.05 level (2-tailed).
Results of generalized linear model analysis.
Discussion
Many studies have examined associations among social characteristics and the incidence of Alzheimer's disease, but little is known about perceived risk of developing Alzheimer's disease, particularly among Black and African American men. It is important to acknowledge the unique vantage point of Black and African American male adults from the intersection of their social characteristics (race, age, gender), their social determinants of health (social integration, stress, support systems) and disability/chronic illness (Alzheimer's disease) and commit to examining the perceived risk of Alzheimer's disease at this junction for persons from minoritized communities. Our study is grounded in the principles of community-based participatory research and sought to ask the subject matter experts, Black and African American men, about their perceived risk of developing Alzheimer's disease. Such an approach is essential to acquiring a deeper understanding of Black and African American men's perspectives and meeting them where they are to address their specific needs as members of an underrepresented and minoritized community.
In our analysis, younger age, income adequacy, and being married or living as married were significantly associated with a low perceived risk of developing Alzheimer's disease in the next 10 years. The corollary of this statement is that Black and African American men who are older, have inadequate household income, and are unmarried reported a high perceived risk of developing AD in the next 10 years. Those who reported low perceived risk share social characteristics with those with low incidence of Alzheimer's disease. Studies have found that age is a risk factor for Alzheimer's disease and that incidence doubles every five years from the age of 65 to 90.27,28 Multiple studies endorse a correlation between income and incidence of Alzheimer's disease, citing that inadequate income limits opportunities to lead a healthy lifestyle.29–31 Several variables in our analysis are associated with incidence of Alzheimer's disease but were not associated with perceived risk of developing Alzheimer's disease. For example, evidence indicates that high levels of educational attainment can minimize the risk of developing Alzheimer's disease, but a significant association was not observed between education and perceived risk in this sample. 32 Employment status, prior experience with Alzheimer's disease, and frequency of forgetting were not significantly associated with the perceived risk of developing Alzheimer's disease in the next 10 years. There may be more than one explanation for these differences. For example, the participants were not asked to provide specific details relating to non-medical factors such as the social determinants of health which may have influenced their behavior. Data capturing participant's support related to economic stability, health coverage or insurance, acceptability of preventative cognitive screenings, and the impact of stigmas/stereotypes when accessing care could potentially provide additional insight into the relationships between the perceived risk of developing Alzheimer's disease and the variables noted to not have significant relationships.
Findings suggest that variables other than those that were measured may be associated with an elevated perceived risk of developing Alzheimer's disease in the next 10 years for Black and African American men.25,33 The social determinants of health framework may provide additional domains that are worth examining. The six domains of the social determinants of health framework include economic stability, neighborhood and physical environment, education, food, community and social context, and health care system. 34 Our study examined a few variables from two of the six domains (e.g., economic stability, education) at a high level. The domain of economic stability examined income adequacy and level of education was examined from the education domain. In addition, several domains were not addressed in our study (e.g., neighborhood and physical environment, food, community and social context, health care system). 34 Within these domains are variables of interest (e.g., access to healthy food and wellness resources, stress, provider linguistic and cultural competency) that were not addressed in our analysis. Mounting evidence suggests that the type of employment (e.g., manual labor), food insecurity, escalated levels of stress, and repeated exposure to racial discrimination are listed as factors associated with a high risk of developing Alzheimer's disease. 35 An examination including factors from all six domains representing the social determinants of health would provide greater insight into which variables are associated with an increased perceived risk of developing Alzheimer's disease among community-dwelling Black and African American male adults. A deeper look at our findings point to future directions in research seeking to understand and proactively address Black and African American perspectives on Alzheimer's disease.
Limitations
Although our findings from this analysis added new insights, several limitations should be acknowledged. Participants were recruited during the COVID 19 pandemic. For many living during the pandemic there was a shift of priorities from future health risk to immediate health risk. This could have influenced the participants’ responses. In addition, the COVID 19 pandemic imposed a financial burden on many households which could have prevented interested men from participating due to a lack of internet access. Furthermore, the methods used for recruitment may have contributed to variances in the sample that may limit generalizability. There was a large representation of participants with higher levels of education in the sample. The social demographics of study participants in this analysis is supported by the findings of the Pittsburgh's Inequality Across Gender and Race report. This report highlights the unique composition of residents residing in the Pittsburgh area which includes a “high proportion of Black men with graduate degrees than most cities”. 36 Similarly, the sample of participants were limited to one geographical location (southwestern Pennsylvania region).
In addition to sampling limitations, our secondary analysis was limited to the data collected as part of the parent study. There was a single-item assessment of participants’ perceptions of AD risk. Although epidemiological studies have used a single-item measure of overall perceived health, there is a lack of psychometric evidence to support the use of a single-item measure of perceived AD risk. Due to the secondary nature of our analysis, we were unable to capture reliability and validity evidence.37–39 The dataset did not include other measures linked to AD risk such as individual health details (e.g., BMI, hypertension, diabetes, chronic kidney disease, sickle cell disease), personal habits (e.g., ethanol consumption, nicotine use, recreational drug use), objective memory performance or measurement of subjective memory performance over time.
Future research
Future prospective studies can extend this novel work by gathering data at the intersection of social characteristics, the social determinants of health and disability. For example, employing a framework that examines lived experiences from a multidimensional perspective and multidirectional influence would be advantageous. The National Institute on Minority Health and Health Disparities framework (e.g., domains of influence and level of influence) and the socioecological framework (e.g., individual, interpersonal, organizational, community, societal factors) are examples of frameworks.36,40–42 These frameworks can guide the examination of lived experiences of persons from minoritized communities while acknowledging the whole person and simultaneously acknowledging the influence of each social characteristic. Black and African American male adults are experiencing life while navigating multiple social characteristics, varying social determinants of health, disability and in some instances the perceived risk of disability. 43
Mounting scientific evidence suggests that eating a healthy nutritionally balanced diet, engaging in regular exercise, effective stress management, regular social interaction, receiving restorative sleep daily, and minimizing the use of alcohol, nicotine products, and recreational drugs all promote good brain health. 44 Future prospective studies would also benefit from collecting data to characterize the frequency and distribution of the variables (e.g., diet, exercise, stress management) related to the promotion of good brain health.
Future work should examine the reliability and validity of the single-item measure of perceived AD risk. To our knowledge, there is no multi-item assessment tool to measure perceived risk of Alzheimer's Disease. Future instrument development could focus on the creation of a psychometrically-sound perceived AD risk tool with input from community research partners. 37
In conclusion, age, income, and marital status were strongly associated with the perceived risk of developing Alzheimer's disease in the next 10 years for male adults who self-identified as Black or African American. Prior experience with Alzheimer's disease was moderately associated with the perceived risk of developing Alzheimer's disease in the next 10 years for this participant sample. Our secondary analysis did not detect any statistical significance between the perceived risk of Alzheimer's disease, social characteristics (i.e., education, employment, living status, marital status) and subjective memory performance. Additional research exploring the associations among perceived risk of Alzheimer's disease, social characteristics, and the social determinants of health is essential to meeting the needs of the Black and African American male adults to improve physical health and mental well-being.
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Author contributions
Lilcelia A Williams (Conceptualization; Methodology; Writing – original draft; Writing – review & editing); Lauren Terhorst (Formal analysis; Validation; Writing – review & editing); Ishan Williams (Methodology; Writing – review & editing); Elizabeth Skidmore (Formal analysis; Methodology; Writing – review & editing); Jennifer Lingler (Methodology; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Institute on Aging NIA/NINR R01AG054518; NIH/NIA T32 AG021885; Pepper Grant P30 AG024827; P30 AG066468.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Lingler has provided paid consultation to Biogen and Genentech.
The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.