
Abstract
How do we account for the ability or otherwise of regional organisations in the global South to enable equitable and inclusive responses to the COVID-19 pandemic? We answer this question with a focus on Africa and in relation to the rights of women and girls. Drawing on theoretical insights from Feminist Global Health Security and from data on the African Union, other regional organisations in Africa and from non-governmental organisations, local activists and medical centres, we show that regional organisations acted quickly to identify the gendered socio-economic and health needs of women and girls and alerted member states to their responsibility to consider gender rights in their policy responses. But weak gender norms led to a disconnect between this early recognition of the importance of policies to protect women and girls and the behaviour of regional organisations, which could not lead a gender sensitive response or engineer one in member state governments.
Introduction
In addition to killing almost seven million people (at the time of writing), the COVID-19 pandemic exposed the devastating consequences of inequality, between the global North and South and within countries (Sow, 2022; Wang and Huang, 2021). These inequalities are profoundly gendered (Al-Ali, 2020; Grugel et al., 2022). How did regional organisations respond to the pandemic and how do we account for their ability or otherwise to protect the rights of women and girls? There were expectations that regionalism could play a progressive role (Byron et al., 2021; Oloruntoba, 2021; Riggirozzi, 2020), reflecting the view that regional organisations have the power to promote the adoption of and adherence to gender equality norms on the part of their member states. We contribute to the debate about the normative capacity of regional organisations and gender by analysing their responses to COVID-19, with a focus on Africa.
A significant body of constructivist research has highlighted the capacity of regionalism to shape member states’ behaviour through the spread of norms, whether through socialisation or rhetorical entrapment (Börzel and Risse, 2003; Risse, 2010; Schimmelfennig, 2001). Meanwhile a separate literature with a more substantive focus on the global South explores the expansion of regionalism to include social and health policy cooperation over the last 15 years (Bianculli and Hoffmman, 2016; Grugel, 2006; Riggirozzi, 2017; Riggirozzi and Yeates, 2015) – the so-called ‘social dimension’ of global South regionalism (Sanahuja, 2010). Yet, both the constructivist literature and work on the social dimension of regionalism lack an exploration of how governance through regional norms impacts individuals and groups living within those regions, or the ways in which these effects are shaped by gender and other societal inequalities. This article draws on recent research from Feminist Global Health Security, which not only speaks directly to pandemic policy making but also provides conceptual tools that enable us to make links between the existence of hierarchies of attention and priority in regional governance and the impact of regional policies on women and girls on the ‘receiving end’ of policies. Deploying these concepts in the context of regional governance for the first time, we show how the gender biases embedded in regional governance are reflected in the everyday experiences of women and girls. Furthermore, we suggest that hierarchies of priority and attention persist at the regional level despite the articulation of progressive norms in relation to gender equality, suggesting that a deeper analysis of regional governance structures and their impacts is required before placing faith in regional organisations to deliver gender-equitable development through norm-based governance.
We first set out our conceptual approach by reviewing existing understandings of the normative power of regions before turning to Feminist Global Health Security to develop a critical framework for understanding the role and impact of gendered hierarchies in regional governance. We then present our methods and case selection and discuss some of the challenges of conducting research on the normative power of regions. Finally, we demonstrate how gendered hierarchies played out in the regional governance of the COVID-19 pandemic in Africa, with a focus on the impact of these hierarchies on the lives of women and girls. We show that regional organisations signposted the gendered needs of women and girls at the onset of COVID-19, but that these needs were not addressed in policy responses to the pandemic. Indeed, their importance dropped down the agenda as the pandemic progressed, becoming, at best, a second-order priority. Crucially, we show that this failure reflected not only a lack of implementation of gender-responsive regional policies on the part of member states, but a process through which the needs of women and girls slipped down the agenda in regional governance hierarchies too. We suggest that this was a function of perceptions of the issues and people who mattered which informed the regional governance of the crisis, which were in turn shaped by the ways in which African regions are inserted into both African inter-state politics and a wider global architecture of health and development governance. Furthermore, we show that outcomes of these hierarchies of attention and priority on the ground were acutely gendered. Our findings, as such, point to the need to temper enthusiasm about the willingness with which regional organisations have apparently embraced gender equality norms with a more holistic analysis of the ways in which the implementation of those norms is shaped by gendered hierarchies of attention and priority, especially in moments of crisis.
Gender Norms and Hierarchies in Regional Governance
We identify the COVID-19 response in Africa as a case of apparent failure to translate progressive norms that support gender-responsive regional governance into delivery on the ground for women and girls. There is an extensive literature dealing with the role of norms in regional governance through a constructivist lens, the majority of which focuses on the European Union (see, for example, Christiansen et al., 2001; Risse, 2010; Rosamond, 2002; Schimmelfennig, 2001; Schmidt, 2006). This work has tended to understand the role of norms in processes of integration and regional governance through a ‘logic of appropriateness’ (March and Olsen, 2011). That is, while constructivist approaches stress the mutually constitutive nature of agents and (normative) structures, in practice they have often focused on the power of regional norms to shape the behaviour of states and other agents from the top down, whether through processes of learning and socialisation (Börzel and Risse, 2003; Risse, 2010) or rhetorical entrapment (Schimmelfennig, 2001). Not only has there been relatively little engagement with gender by these constructivist theories (see Lombardo and Kantola, 2021); there has also been limited attention paid to understanding the extent to which regional norms impact the everyday lives of individuals.
Although somewhat implicitly, scholarship on the social turn in global South regionalism builds on some of these claims about the diffusion of norms through regional governance. This literature espouses the view that from the turn of the millennium, regionalism in the global South had moved away from an exclusive focus on market opening and should be understood as a space for generating shared social policy norms (Riggirozzi, 2014; Riggirozzi and Tussie, 2012). Building on Acharya’s (2013) work on the global consequences of end of US hegemony, Riggirozzi and Tussie (2012, 2021) argued that regions in the global South would, or at least could, become a space for transboundary, ‘post-hegemonic’ social projects, characterised by commitment to socially inclusive policies and the promotion of equity (see Briceño-Ruiz and Ribeiro Hoffmann, 2015; Da et al., 2007; Sanahuja, 2012). In Africa, Yeates and Surender (2020) pointed to the consistent inclusion of social policy in African regionalism. This focus on the significance of shared approaches to welfare, education and health made some headway in addressing the gender gap in regionalism scholarship (Van der Vleuten, 2016). There was also greater space to move beyond the elite politics of regionalism by considering regional spaces as ‘sites for collective action’ from below (Riggirozzi, 2015). However, the detail of how regional organisations go beyond a rhetorical embrace of the need for more inclusive social policies is not always clear. Mirroring the constructivist work discussed at the beginning of this section, Riggirozzi (2017) argued that regional organisations exert influence by acting as norms brokers and can socialise member states into endorsing progressive social policies, even in circumstances when they do not have the institutional capacity to impose them. As with other work on the power of regional norms, what has not been fully explored is the extent of their impact on the lives of regional citizens.
In contrast to the social turn literature’s emphasis on the potential of regions as spaces for normative change and socialisation, the dominant scholarly reading of African regionalism has taken a more pessimistic view of the ability of regional norms to shape the policies and behaviour of their member states. In fact, the principal purpose of African regional organisations has often been understood as boosting member states’ sovereignty and the legitimacy of ruling elites through the ‘performance’ of regional cooperation (Gibb, 2009; Söderbaum, 2004, 2013). As a result, the reach of regional organisations ‘downwards’ in ways that might shape the lives of people within member states has typically been regarded as limited, especially in areas related to citizenship, wellbeing and sustainable development (Hartmann, 2022; Motsamai and Qobo, 2012). Other scholars have stressed that African regions are constrained not only by the reluctance of their member states to cede authority to supranational bodies but by their dependence on external donors for budgetary support and organisational capacity (Buzdugan, 2013). More recently, however, this account of the limited agency and capacity of regional organisations in Africa has been challenged. O’Reilly and Heron (2022: 6) argue that there is a need to delve into the institutional structures and functioning of African regional organisations in order to understand their specific dynamics and limitations, rather than dismissing their apparent dysfunction as the inevitable product of postcolonial statehood and external dependence. As in the wider regionalism literature, however, there remain few attempts to connect this sort of institutional analysis to the experience of citizens on the ground, nor to link it with gendered structures of inequality.
It is here we turn to feminist scholarship to provide conceptual tools that allow us to make a direct link between regional governance and the lived experiences of women and girls. Feminist institutionalist approaches to regionalism, developed principally in relation to the European Union (Haastrup and Kenny, 2015; MacRae and Weiner, 2017), provide a useful starting point by highlighting the way in which formal and informal regional rules, norms and practices are inherently gendered. These insights have been applied directly to the African Union (AU) and the genesis and implementation of the Maputo Plan of Action elsewhere in our work (Saka, 2023). However, here we seek to move beyond the regionalism literature and to develop and apply insights from feminist scholarship conducted in other sub-disciplines of International Relations (IR). In particular, we draw on emerging Feminist Global Health Security (FGHS) literature to make explicit the link between governance practices in the regional sphere and the everyday experiences of women and girls.
According to Wenham (2021: 32), FGHS starts from the question that has been fundamental to so much feminist scholarship: where are the women? With this question in mind, Wenham follows feminist IR theory in offering a critique of state-centrism in both the practice and scholarship of global politics. This state-centrism, Wenham (2021: 47) argues, is responsible for IR’s failure ‘to acknowledge differences in [policy] impact and implementation at the individual, social group or community level’. The corollary of this critique is that feminist approaches to global health security, and to global politics more broadly, should eschew state-centrism in favour of foregrounding individual human subjects in their analysis, and in particular the embodied and gendered realities of people’s lives (O’Manique and Fourie, 2018: 1; Shepherd, 2009). Furthermore, the rationale for this focus on the gendered realities of everyday lives comes from the central insight that social structures are inherently gendered and that both health emergencies and policies designed to address them have differential implications for women and girls (Wenham, 2021: 34).
FGHS goes beyond simply calling for greater attention to be paid to the impact of health governance on the everyday lives of women and girls by providing conceptual tools that enable us to connect this concern to the global (or in our case regional) politics of health. Here, the concept of gendered hierarchies in global/regional governance is key. Drawing on theories of securitisation from the critical security studies literature, FGHS highlights the ways in which understandings of security and insecurity – and what constitutes a health emergency – are shaped by those working in global health organisations as well as those who transfer and implement health security policies at the national level (Wenham, 2021: 45). Importantly, these policy spaces are understood as being characterised by hierarchies that omit or deprioritise the experiences of women and girls – especially where there are intersections with other social inequalities (Harman, 2021; Smith et al., 2021). What is more, the critical literature on the securitisation of global health highlights the ways in which security has often been framed in terms of protection of Western states from health threats that originate in the global South, and responses focus on preventing the transmission of such threats as opposed to mitigating their impacts on the daily lives of citizens in the global South (Harman, 2021; Wenham, 2021). As Harman puts it, [T]he problem is not just that health emergencies interact with societal inequalities to exacerbate gender inequality, but that that the framing and structures of global health security reproduce gender inequality in the privileging of some issues at the expense of others . . . Gender is not just excluded from health emergency planning and response because of a lack of inclusion of knowledge or experts; it is excluded by the structures of global health security, which create hierarchies of issues and of the people who matter. (Harman, 2021: 609)
FGHS suggests that the impact of these hierarchies is particularly acute in the context of perceived health emergencies where the ‘tyranny of the urgent’ means that structural inequalities are set aside in favour of addressing immediate biomedical needs (Davies and Bennett, 2016; Smith, 2019). We know from existing research that, just like the global institutions referenced by FGHS scholars, regional institutions exhibit gendered hierarchies and biases too (Guerrina et al., 2018; Jenson, 2008; Saka, 2023; Thomson, 2018).
FGHS scholars also highlight a paradox in which increased visibility of gender in international organisations does not necessarily indicate that these hierarchies are being transcended. Smith (2022: 202) describes this gender paradox as ‘an inverted triangle within global health where there are numerous standards related to women’s health, but little incorporation of these into organisational practices or national implementation, and even less evidence of improved health outcomes for women’. Harman (2021: 621), meanwhile, notes that COVID-19 marked a clear change towards the greater visibility of gender in health emergencies but that this did not lead to substantive policies to address the gendered dimensions of the pandemic. Instead, this increased visibility existed in a context that continued to be pervaded by gendered hierarchies (Harman, 2021).
At this point, we return to the puzzle posed in the introduction and at the beginning of this section – how do we account for African regions’ apparent failure to translate norms and policy pronouncements in favour of gender-responsive health policy into positive outcomes for women and girls in the context of the region’s COVID-19 response? While the focus of the FGHS literature revolves around specific questions about the securitisation of global health, we argue here that it provides a number of conceptual insights that can help us to address the puzzle raised in this article and to better understand broader limitations to regional governance through normative power. First, it suggests a critical orientation towards state-centric approaches to regional politics, in which the central focus is on the ability (or inability) of regional normative governance to shape the behaviour and preferences of member states with little attention given to the implications of this for the gendered realities of everyday lives. Second, it directs our attention to the ways in which regional governance and regional social policies incorporate hierarchies that prioritise certain people and certain problems over others, and to the ways in which gender and other societal inequalities shape these hierarchies. While FGHS highlights the acute effects of these hierarchies in the context of perceived health emergencies such as the case examined here, this may also extend to other contexts in which regional governance operates under conditions of resource constraint as is commonly the case in the global South. Third, it is important to consider the ways in which gendered hierarchies exist across national, regional and global levels of governance, and the interactions between these levels. For our purposes, it is also important to consider how both the inter-state politics of African regions and their insertion into the wider global development governance architecture shapes the people and issues that are given the highest priority. Taking this together, we suggest that the translation of progressive social norms at the regional level into results that are felt in the everyday lives of regional citizens is far from a straightforward process in which member states are socialised or rhetorically entrapped. Instead, the process through which progressive norms articulated at the regional level are translated into regional policy initiatives and reach downwards to shape the lives of citizens within member states is mediated by deeply embedded and acutely gendered hierarchies that determine who and what matters in policy making.
Methods, approach and case
We ask questions in this article about the ability of regional organisations to improve the lives of women and girls through their normative power. In doing so, we contribute to broader literatures on the role of norms in regional governance and engage with the social turn in global South Regionalism by introducing the concept of gendered hierarchies in regional governance from Feminist Global Health Security. Our African case study extends the geographical focus of work on the social turn in global South regionalism – which to date has principally dealt with Latin America – while elaborating the constraints that regions face in realising normative visions for social governance. Furthermore, although African regions exhibit a range of features that are distinctive – such as their acute budget constraints, reliance on donor support and a strong reluctance by member states to cede sovereignty to supranational bodies – we contend that our more general observations about the impact of gendered hierarchies on regional governance are likely applicable across other regional contexts. Specifically, we seek to understand the apparent limitations to the capacity of regional organisations in Africa to support a gender-equitable response to COVID-19, taking particular note of the employment, education, living standards and gendered health needs of women and girls. The regional organisations are set out in Box 1. As ‘the premier regional integration arrangement for Africa’ (Kasaija, 2016:143), we pay particular attention to the African Union. 1
Regional organisations and regional economic communities.
Represents all African countries.
Asking questions about whether regional institutions choose, or are able, to promote gender-equitable policy inevitably requires some consideration of their institutional and financial capacity, alongside the policies they deliver. There are always economic limits to what regional institutions, especially in the global South, can achieve because these institutions are nested within a global political economy that sets clear fiscal boundaries on budgets at national and regional levels. We, therefore, pay some attention to the fiscal capacity of African regional organisations. Within this constrained context, however, what we are really interested in is the choices that African regional organisations make about how to prioritise their limited resources.
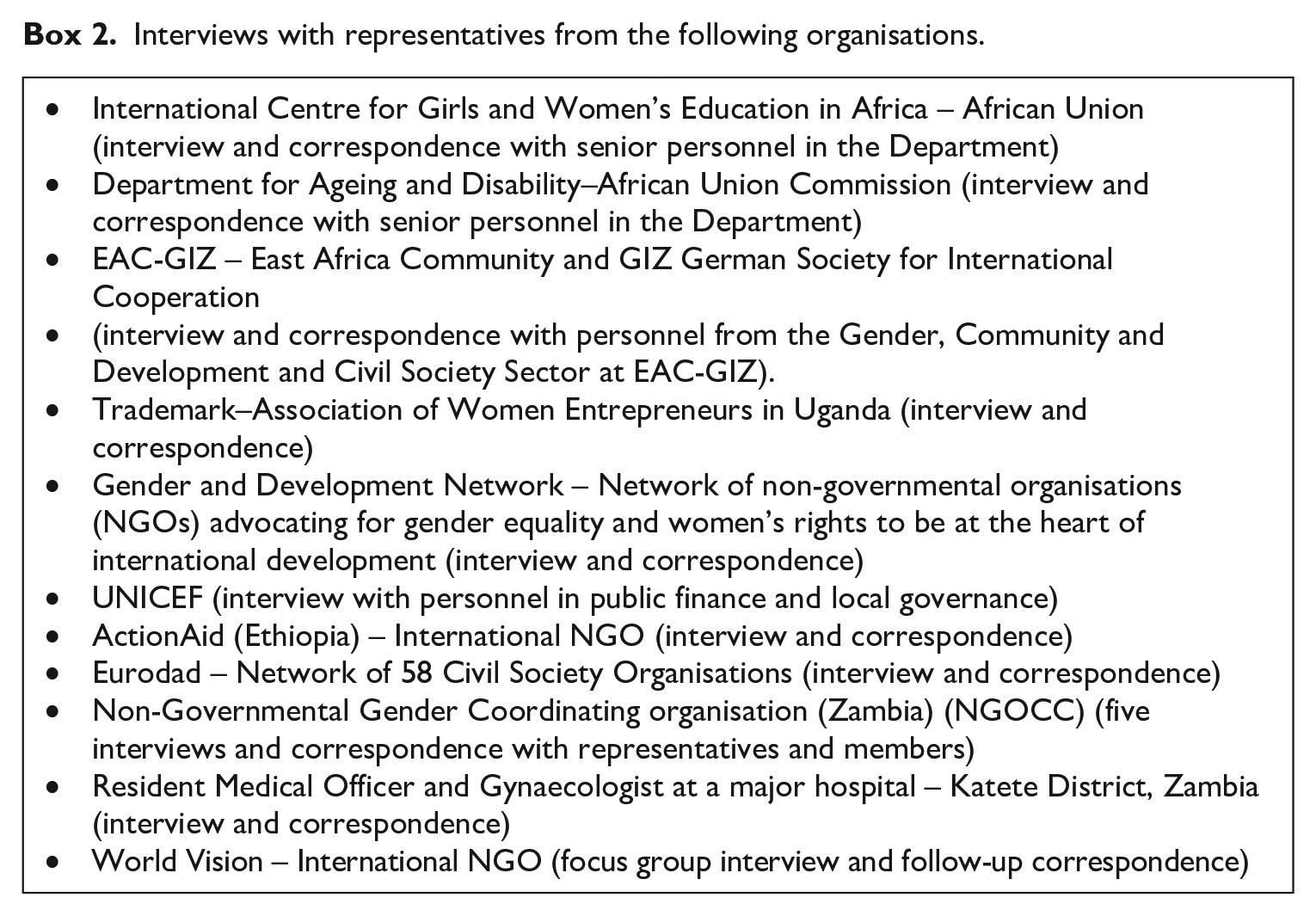
As we have already set out, there is ample evidence from the existing literature to suggest that regional institutions – including those that are the focus of this research – are gendered. However, the gender norms that structure these institutions and the hierarchies of attention and priority that they produce may be difficult to trace empirically because they are generally unspoken or taken for granted (Chappell and Waylen, 2013). In the case of regional organisations in Africa, gathering data on institutions is also particularly challenging, as Hartmann (2016) noted, because data on decisions, decision-making and policies are not always easy to obtain and policy-makers tend to grant limited access to researchers. In our research, we additionally had to contend with the consequences of COVID-19 which meant that ethnographic fieldwork within regional organisations could not be attempted. Consequently, we have relied on an exhaustive analysis of the detail of the policy responses of regional organisations during COVID-19 through a combination of documentary data and data drawn from a series of qualitative interviews with representatives of regional organisations, civil society actors, think tanks, medical facilities and non-governmental organisations (NGOs) in Africa over a period of 18 months (July 2020–December 2021) which we carried out on Zoom. We conducted 14 semi-structured interviews in total and one focus group. These interviews were sometimes followed up with email exchanges. The details of these interviews are set out in Box 2 and the guiding questions we used are in Box 3. Each interviewee was provided with information about research before giving consent to participate in the study. We have anonymised the interview data in agreement with the interviewees.
Interviews with representatives from the following organisations.
Question guidelines for semi-structured interviews.
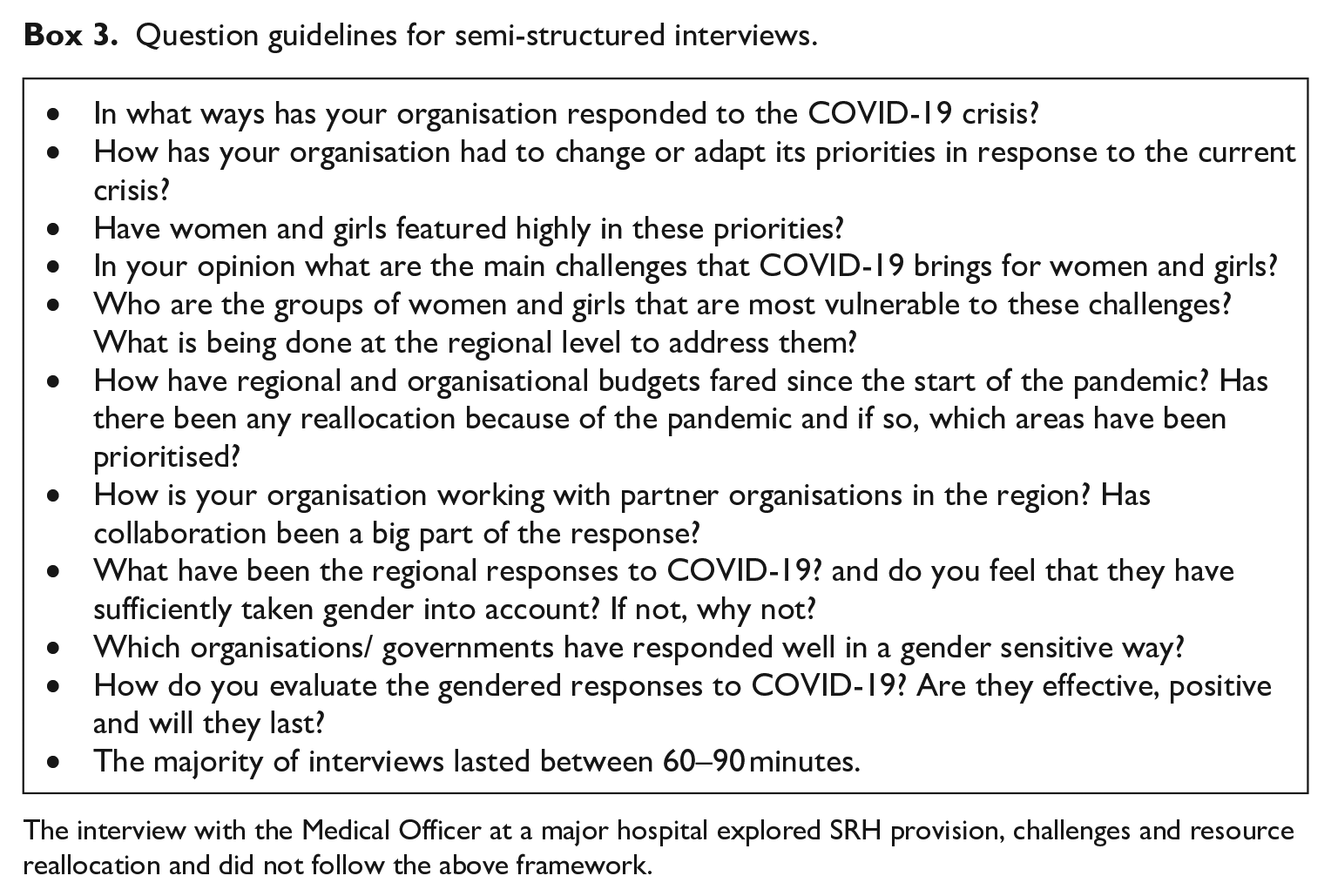
The interview with the Medical Officer at a major hospital explored SRH provision, challenges and resource reallocation and did not follow the above framework.
This interview data provided some direct evidence of the ways in which gendered hierarchies shaped the pandemic response in African regions – that is, respondents commented explicitly on the ways in which issues and groups were prioritised as part of the pandemic response. The data also give us indications of the origins of these hierarchies, for example, by pointing to the importance of both member state and donor preferences as drivers of the regional response to the pandemic. We scaffold this evidence by interpreting it in the context of the conceptual literature set out above as well as existing empirical evidence on the gendered character of regional institutions. Beyond this, we are just as interested in tracing the effects of the COVID-19 pandemic and pandemic responses on women and girls on the ground in Africa, from which we argue that the presence of gendered hierarchies can also be inferred. Taking this together, the article provides a rich and detailed empirical demonstration of how gendered hierarchies played out in the regional governance of the COVID-19 pandemic in Africa, with a core focus on the women and girls on the receiving end. This research was conducted as part of two GCRF/GCRF-MRC funded projects: Thanzi la Onse and Gender and Health Systems in Low- and Middle-Income Countries after COVID-19: the Promotion of Women’s Health and Emerging International Policy Advice. Ethical approval for both projects was received from the University of York, UK and for Thanzi la Onse, approval was also received from the Medical Council, Malawi.
COVID-19 in Africa: exacerbating the gendered crisis of development
The Gender Inequality Index produced by the United Nations shows that, prior to the pandemic, women experienced worse social and development outcomes than their male counterparts, measured through a range of policy areas from reproductive health to empowerment and economic status (Ortiz-Ospina and Roser, 2018). For women and girls in Africa, the arrival of COVID-19 exacerbated these deeply rooted existing gendered inequalities, including the widespread prevalence of gender-based violence, child marriage, poor access to sexual reproductive healthcare, patchy delivery of education for girls and a highly unequal burden of care responsibilities. In the 12 months preceding the pandemic (2019–2020), according to UN Women (2020), 37% of girls in sub-Saharan Africa had married before they were 18 years old, and 12% had done so before they reached the age of 15. Prior to the pandemic, adolescent pregnancies were significantly higher than in any other region of the world, with 28% of all women under 24 having given birth before they were 18. For the poorest women, this figure rose to 42%. In 2019, 21.5% of ever-partnered women and girls had been subjected to intimate partner physical or sexual violence, and one in three girls aged between 15 and 19 had been subjected to genital mutilation. Less than 49% of women were able to securely access family planning and contraception healthcare needs (Melesse et al., 2020). Education for girls was uneven, with 31 million girls without access to secondary education and 49 million girls unable to access both primary and secondary education (Human Rights Watch, 2017). With regard to the labour market, the International Labour Organization (ILO, 2017) estimated that in 2017 more than 90% of workers in the informal sector in Africa were women, contributing to the fact that 81% of women workers were extremely, moderately or close to being poor in 2019 (Aoyagi, 2021). Protecting women and girls from further harm occasioned by the onset of COVID-19 was, in short, urgent.
The first wave of government responses in Africa was modelled on responses in Europe and North America. Borders were closed, informal markets and workplaces were shut down and stay-at-home measures introduced (Haider et al., 2020). These initiatives were presented as government ‘preparedness’ and ‘determination’ to tackle the spread of COVID-19 (Markantonatou, 2021), but they had wide-ranging impacts beyond their intended remit to limit the spread of the virus. As Alaran et al. (2022) argue, one of the first consequences of these measures was to dramatically limit access to health services for women and girls, severely impacting their access to, and the quality of, maternity and sexual and reproductive services. Many antenatal consultations switched to online platforms, in-person appointment times were spaced out and in-person visit numbers were reduced, leaving pregnant women at risk of harm, sometimes denying them crucial information and care and exposing them to the risk of medical neglect and abuse (Reingold et al., 2020). In addition, in many countries of the region, health resources were redirected away from the provision of maternity and sexual and reproductive health services to other areas of healthcare provision under COVID-19; this included the redeployment of experienced midwives to other areas of nursing (Homer et al., 2021). The outcome of these changes was severe, according to Chmielewska et al. (2021) and contributed to an increase in stillbirths, preterm labours and the ‘worsening of pregnancy outcomes . . . during the pandemic’. What is striking here was the absence of learning from previous health crises that closing services to women and girls has a catastrophic impact on their sexual and reproductive health. During the Ebola outbreak in West Africa in 2014–2016, women’s access to healthcare was drastically reduced in order to redeploy resources to other areas of primary healthcare. It is estimated that this decision led to more new mothers and children dying during childbirth than the number of people who succumbed to the virus (Davies and Bennett, 2016). In Sierra Leone, 3593 people died of Ebola virus while up to 4936 additional new-born babies and mothers died during childbirth in what the Gates Foundation (2020) called a ‘silent death toll’. These reductions in healthcare provision came alongside a stark increase in physical or sexual violence by current or former partners, which Bello et al. (2023) estimate to have risen from 33% of women and girls aged 15–49 in 2018 to 52% during the pandemic.
Meanwhile, school closures were implemented widely across the region and had particularly negative effects for girls. For many, it meant an abrupt end to their education for good. UNESCO (2022) has estimated that up to 11 million girls will not return to school, leaving them vulnerable to early marriage. For many girls from poor families, not attending school meant that they lost their one substantial meal a day and threw their nutritional needs back on severely constrained family income. For those for whom school served as a place of safety, the threat of domestic or sexual violence increased; many also faced an increased burden of domestic work. The Ebola outbreak in 2014 had led to significant increases in the number of teenage pregnancies (Davies and Bennett, 2016; Korkoyah and Wreh, 2015), with as many as 14,000 teenage girls in Sierra Leone becoming pregnant during the outbreak, 11,000 of whom had been in school before the pandemic struck (UNFPA Sierra Leone, 2018). Despite this recent evidence, little action was taken by governments to ensure that this would not be repeated under COVID-19. As a result, teenage pregnancies rose dramatically across Africa during the pandemic, with data from Ghana suggesting a nine-fold rise in some communities in the first 3 months of lockdown (UNESCO, 2020). Data from Kenya suggest that school closures tripled the likelihood of girls dropping out of school permanently and doubled the risk of girls becoming pregnant (Zulaika et al., 2022).
The prevalence of women working in poorly paid and informal jobs, meanwhile, meant that working women and their families also paid a high price during lockdowns. For women working in informal markets, border closures reduced their access to products and markets (Aoyagi, 2021). In the formal sector, the World Bank (2020) reported that, in Ethiopia, Malawi, Nigeria and Uganda, up to 15% more women lost their jobs than men.
The limits of regionalism: Responding to COVID-19
According to Grugel et al. (2022: 79), all regional organisations in the global South, in making their response to the pandemic, aspired to advocate for the protection of the most vulnerable and provide logistical expertise and knowledge sharing to member states. African regional organisations have made strong commitments to region-level policies and norms that align with this goal, and in particular with the aim of promoting the rights and welfare of women and girls. Perhaps most importantly, the AU’s Maputo Protocol, which came into force in 2005, commits the region to combating all forms of discrimination against women through the drafting and implementation of legislative, institutional and policy measures to ensure that the rights of women are promoted, realised and protected for the realisation of their human rights (Viljoen, 2009). The Protocol’s commitments on sexual and reproductive health and rights, in particular, were developed into a comprehensive policy framework for the continent – the Maputo Plan of Action (MPoA), 2006-2015 (later extended to 2016–2030) (see Saka, 2023). In the economic sphere, the AU has committed to reducing informal work across the region and increasing labour and social protections for informal workers – the majority of whom are women. Supported by the ILO (2019), the AU adopted the Decent Work and the Transformation of the Informal Economy programme in 2019, which charges the AU and the Regional Economic Communities (RECs) with reducing ‘decent work deficits in the informal economy . . . through progressive transition to formality’.
It is well documented that African regions face significant resource constraints that hamper the realisation of these aims, even outside of a crisis period such as the COVID-19 pandemic. Funding streams for African regional initiatives, especially in relation to social and gender policies, are unreliable and fragmented (Stapel and Söderbaum, 2019). Regional organisations aim to be financially autonomous, but rely heavily in fact on donor funding. While they draw contributions from member states, based either on a funding formula determined by a council of ministers (Southern African Development Community (SADC) and Common Market for Eastern and Southern Africa (COMESA)), a percentage of nominal gross domestic product (GDP) (East Africa Community (EAC)) or a community levy (Economic Community of West African States (ECOWAS)) or a combination of these measures (AU), in reality, this funding is generally insufficient. It is not unusual for regional programmes to be started and then scaled back or even abandoned, or for donors to have to step in and take on even more of the heavy lifting. To illustrate, in 2017, almost 3 years before the COVID-19 crisis, less than 27% of the AU’s expenditure was actually being covered by member states contributions (AU, n.d.). Stapel and Söderbaum (2019) highlight that with 30 of the 55 members regularly underpaying or paying no contributions at all, it frequently fell to donors such as the EU and European states to make up the difference. In a bid to reduce dependence on donor funding, additional measures were agreed at that time, including a 0.2% levy on imports to reduce the budgetary gap. But, by 2021, only 17 AU member states had adopted the levy and contributions to the AU had dropped further to around 25% (Institute for Security Studies Africa, 2022). The AU is not an isolated case either. The EAC’s fiscal year budget 2021/2022 was $91.7m with member states budgeted to provide 59% through contributions with the remaining 41% drawn from development cooperation partners. However, even at the time the budget was set, member states were already in contribution arrears by $50m, leaving donor funders to bridge the shortfall and increasing regional organisations’ reliance on aid (The Citizen, 2022). Meanwhile, most of the RECs – with the exceptions of SADC and to a lesser extent ECOWAS and EAC – receive relatively little donor support, which is instead concentrated on the AU (Stapel et al., 2023).
Regional organisations in Africa came under enormous financial and capacity stress during COVID-19. As we have already suggested, however, we are most interested not in the origins of these constraints, but in how the resources available were used and how this reflects hierarchies in the people and issues that are considered to be the most important and urgent. In the sections that follow, we show that regional institutions in Africa were alerted by their own research, as well as that of international organisations, to the fact that the pandemic would impact particularly harshly on the region’s women and girls but that they failed to translate this into policies to protect women and girls. On the one hand, the AU and the RECs – with of course some differences at the sub-regional level – clearly flagged up the gendered implications of government responses to COVID-19 and of the deep economic recession caused by COVID-19. They also identified the needs of the many women who work in the informal sector and who were without social security protection, the increases in the care burden that would fall to women, the risks of gender-based violence, reduced access to sexual reproductive health services and the barriers that were being put in the way of girls’ education. They did so alongside, and sometimes under pressure from, region-based civil society organisations. On the other hand, however, tackling these issues quickly became deprioritised as regional responses turned to focus on addressing immediate biomedical needs generated by the pandemic. This was not simply a case of the non-implementation of regional norms by member states. Instead, women and girls were not sufficiently highly placed within gendered regional governance hierarchies to receive priority treatment as the impact of the pandemic bit. Furthermore, the deprioritisation of women and girls was exacerbated by the agendas of both member states and donors, both of which failed to endorse or lead on the critical need to gender COVID-19 responses, with important implications for policy and budgets at the regional level. These failures had immediate impacts in terms of girls’ access to education, social and income protection for informal women workers, gender-based violence and women’s and girls’ access to sexual and reproductive health services and raised questions about the capacity of regional organisations to lead gendered social governance, particularly when they are placed under strain.
Grave concerns identified but an early warning system compromised
Regional organisations in Africa were remarkably quick to issue warnings that COVID-19 represented a major regional development crisis and that this crisis would be profoundly gendered. They acted as an early warning system that actions needed to be taken to protect the rights and wellbeing of women and girls. While East Central and Southern African Health Community (ECSA-HC, 2020) offered a disease-focused response, calling in February 2020 for transboundary cooperation to ‘strengthen surveillance systems for prevention, early detection and appropriate response to threats of disease outbreak including COVID-19’, the AU went much further, in line with its remit to try and coordinate social, health and gender policies (AU, 2019). The AU (2020a, 2020b) quickly set out the heightened risks to the region’s women and girls posed by COVID-19. It called for member states to take action to address the challenges lockdowns and restrictions on public and social contact would pose to women (Plomien et al., 2022) and to ensure that the COVID-19 pandemic does not ultimately aggravate other areas of vulnerability for women and girls, including women’s reproductive health, child marriages and domestic violence. (Africa Child Policy Forum (ACPF), 2020)
Such was the apparent sense of urgency that gender should be fully integrated into the regional response that, in June 2020, the AU issued Guidelines on Gender-Responsive Responses to COVID-19 to ‘assist Member States in addressing, managing, responding and recovering from COVID-19, with Gender Equality and Women’s Empowerment (GEWE) priorities guiding said efforts’ (AU, 2020a). Recommendations included ensuring that member states ‘regain and retain socio-economic stability for women and girls’ with approaches highlighting ‘gender mainstreaming and integration, sex disaggregated data’ and crucially, ‘gender-budgeting’ (AU, 2020a). Similarly, the AU flagged up the central importance of maintaining education services for the region’s girls. The AU made clear that closing schools, even temporarily, would effectively end many girls’ access permanently. In July 2020, 3 months after the arrival of the pandemic in Africa, Education Ministers met at the AU to discuss the provision of education across member states. Since schooling had switched to online, the meeting was dominated by the impact of limited computer hardware for children and weak and partial Internet coverage in many rural areas, but it was also acknowledged in the meeting that closing schools posed particular challenges for girls. AU representatives noted in interviews with us that, from early on, the closure of schools was closely correlated with increases in gender-based violence and genital mutilation (interview, 2020). They went on: the COVID-19 pandemic and its prevention measures have posed a major threat to existing member state gains in ending child marriage and exacerbated already existing vulnerabilities to women and girls, such that there is an anticipated rise of up to 10 million more child marriage cases by the year 2063. (AU, 2022)
Regional organisations also reminded governments of the need to address the costs of lockdowns and border closures on women in the informal sector. Research by the World Bank in Liberia, Guinea and Sierra Leone following the 2014 Ebola outbreak showed clearly that women paid a higher price from unemployment and for a much longer time than men (World Bank, 2017). This was recognised across the AU and the RECs and COMESA, SADC, ECOWAS and the EAC all undertook public campaigns to raise public awareness on the experiences of women and their role in the pandemic and post-pandemic economy (COMESA, 2020; SADC, 2021). COMESA (2021a, 2021b) developed toolkits and policies and offered training on gender, work and COVID-19 to member states, while ECOWAS produced policy recommendations through its Action Plan on Gender-Sensitive Response to the Coronavirus Disease and to strengthen gendered responses sought to redefine the terms of reference for the ‘establishment of Member States’ stakeholders’ networks against sexual and gender-based violence’ (ECOWAS, 2020). The SADC and EAC each provided recommendations to member states on actions that they could adopt in order to support women and girls through the pandemic (EAC, 2020; SADC, 2020).
But, quite quickly, this focus on ensuring that protecting women and girls from further costs would be an integral part of the regional response slipped down the agenda. Attention to incorporating the gendered needs of women and girls into the policy response gave way to a focus on exclusively biomedical needs. So, for example, when the AU sought international funding from donors to support the continental response to COVID-19, the need for gender-responsive policies dissipated in favour of the need to strengthen regional diagnostic capacity and invest in frontline health care (AU and Africa CDC, 2020; Omukuti et al., 2021). Developing an effective medicalised response, while ignoring the gendered impacts of COVID-19, gradually became the ‘COVID-19 response’ within the AU, driven by the preferences of member states and donors to fund frontline services, as the FGHS literature and existing research on African regional responses to health crises might have predicted. As Abdulmelik (2017: 216) argued, drawing on the AU and ECOWAS responses to the Ebola crisis, African responses to health crises are ‘embedded in, and mediated by, the international political economy of the Western-designed architecture of humanitarian responses to “crisis” in Africa’, which tend not to see gender as integral to policy. Meanwhile, the emphasis on the part of donors on containing the spread of disease can be seen as a reflection of the ways in which this global architecture has prioritised the security of Western states ahead of the lives and livelihoods of those in the global South (Harman, 2021; Wenham, 2021).
This shift in priorities had two immediate effects: first, it meant that additional funds were not raised for the protection of women and girls and, second, it led to cuts to existing gender programmes in the AU as gender was effectively downgraded in the regional hierarchy of attention and priority. AU departments, including those concerned with women’s health, education and wellbeing, were told in early 2020 to make cuts: Since April 2020, all AU entities have been asked which part of their budgets they can send to the COVID response . . . the real question for each organisation is how do we come up with a list of priorities? (Interview, 2020)
So, rather than increasing funding to address the gendered costs of the pandemic, the AU found itself spending less on programmes for women and girls than in normal times, in order to free up limited resources to meet the general medical needs associated with COVID-19. One interviewee in the AU made direct reference to how the hierarchical and gendered structure of regional organisations shaped regional priorities: Everybody at the AU knows there will be losses to a variety of programmes but there are priorities . . . the top priorities are health, personal protective equipment and ventilators. (Interview, 2020)
Budgets to promote gender equality were dramatically cut. In 2021, the AU Commission inaugurated an internal committee on the Fund for African Women but simultaneously cut its funding by half from 1% of its operating budget to 0.5%.
2
Moreover, the disbursements the fund did receive were delayed, ‘hindering any envisaged progress’, as the AU Commission (2022: 31) itself acknowledged: The COVID-19 pandemic has the potential to reverse most of the gains made over the years in promoting GEWE. Diversion of resources to COVID-19 may delay implementation of gender commitments that are not seen as urgent. (AUC, 2022)
Again, this reflects a common theme within the FGHS literature, in which policies to address wider structural inequalities become subject to the ‘tyranny of the urgent’ and are deprioritised in favour of immediate medicalised responses to health emergencies (Davies and Bennett, 2016; Smith, 2019). This was accentuated as member states sought to cut back on their fiscal commitments in the wake of COVID-19. As one interviewee told us, Budgets are already being reallocated within the African Union Commission. [Our] 2021 budgets have all been cut. It is an austerity budget . . . the Commission is funded by member states and partners have their own issues in their own countries so will reduce funding to the Commission. (Interview, 2020)
Adding to the AU’s woes – and in line with expectations about the priorities of Western states – was the fact that donors, in an effort to get funding to the medical COVID-19 frontline, had already begun to redirect budget lines initially allocated to the AU to member states (interview, 2020). Taken together, while these cuts, from member states and donors alike, left the AU weakened and its leverage reduced, they also reflect a broader set of gendered hierarchies in both member states and donors, which in turn impinged on the priority setting of regional organisations. The result was that, despite being able to act as an early warning system of the gendered costs COVID-19 would present in Africa, the AU did not ultimately prioritise the protection of women or the need to embed gender in COVID-19 policy responses. Its capacity for normative leadership, in so far as gender was concerned, was severely constrained by the gendered hierarchies within regional organisations as well as those that existed within the wider governance landscape in which these regions are situated.
In turn, this shaped the activities of the civil society actors that had tended to support programmes for women and girls at the regional level. Many of the key public services women and girls routinely used, such as reproductive health services, were provided by the non-governmental sector dependent on the AU for funding were cut or abandoned during the pandemic. One interviewee with a major NGO told us: It has been a learning curve . . . [we had] to think of reorganising priorities whilst still delivering an impact. Without proper funds, we cannot have significant impact. (Interview, 2020)
In fact, it seems that NGOs were brought under pressure to use existing grants that provided the services for women and girl for frontline medical responses to COVID-19, using ‘crisis modifier’ clauses that allow donors to intervene to ask for the spending to be redirected away from its original purpose (interview, 2020). One NGO informant recounted how they were asked to redirect funding to support young pregnant girls in accessing education to primary COVID-19 care, despite the fact that teenage pregnancies were rapidly increasing as a direct result of the conditions women and girls were forced to endure during lockdown (interview, 2020). This last example illustrates the far-reaching effects of the gendered hierarchies shaping regional governance of the pandemic.
De-prioritising women’s rights: Effects on the ground
Because regional organisations had been so prominent in articulating gender equality norms in Africa, the impact of the decision to deprioritise women and girls during the COVID-19 crisis had immediate and deep effects on the ground. We show these effects now in two key illustrative domains: sexual and reproductive health services and employment.
In relation to sexual and reproductive services, the effects were little short of catastrophic. With provision of sexual and reproductive health often excluded from member states’ public health provision, women have often relied on donor and NGO-funded services (Ravindran and Govender, 2020). The AU has played a generally supportive role in advocating for better provision and led the drive to promote and protect women’s access to sexual and reproductive health across the region for almost 20 years since the Maputo Plan of Action. But it failed to play this role during the COVID-19 pandemic. Instead, the pattern was repeated from the 2014–2016 Ebola outbreak: budgets for women’s healthcare were quickly reallocated to meet other healthcare needs that were seen as more urgent (Davies and Bennett, 2016; Gates, 2020). As a representative from the Non-Governmental Gender Coordinating Organisation (NGOCC) in Zambia put it, budgets for sexual and reproductive health are simply not perceived as essential health services: . . . it is a result of the prejudice against the needs of women that cause the health planners to undervalue women’s needs. . . . women’s needs are already under-funded but when there is a crisis, budgets for women’s needs are the first to be redirected because society does not consider women’s needs as essential. (Interview, 2021)
The consequences of this decision have been disastrous. Researchers from across Africa were clear that women would experience unwanted pregnancies, unsafe abortion and the lives of women and babies would be put in danger, unless investments were made in the maintenance of reproductive health services (Govender et al., 2020; Riley et al., 2020). Budget cuts were nonetheless implemented. We spoke to one hospital medic, in the Katete District of Zambia, whose experience was typical. As they recounted, the consequences of budget cuts were felt immediately. Women began to present in the hospital with complications from unsafe abortions as the funds for the procurement and distribution of reproductive health products including contraception, medical abortion drugs, antibiotics and equipment because budgets were reallocated away from this area of healthcare to support pandemic response. . .. At the height of the COVID-19 pandemic, contraception in the whole district became inaccessible because the funds were redirected to the COVID-19 response. (Interview, 2021)
The cuts meant that women faced enormous difficulties in accessing the few reproductive health and contraception programmes that remained open (interviews, 2021). The closure of public sexual and reproductive health clinics accounted directly for around 13.4% of women and girls not being able to access services (African Population and Health Research Centre (APHRC), 2022), while an inability to afford private provision, an absence of time to source now-distant reproductive health care and opposition to women travelling the much greater distances needed to access it prevented around 60.7% of women from accessing services. For women seeking abortions or post-abortion care, the picture was particularly bleak. Women’s groups reported that in Burkina Faso, Kenya, Uganda and Ethiopia abortion services closed, often because staff had been redeployed elsewhere.
In relation to work, income and care, meanwhile, abandoning the early policy of trying to ‘gender’ pandemic responses in Africa was also extremely costly for women. Once again, local researchers flagged that, without income and labour market protections, women would experience job losses and exposure to poverty (Casale and Posel, 2020; Casale and Shepherd, 2021; Parry and Gordon, 2021). The 89.7% of African women who work in the informal economy (AU, 2020c) were exposed to the greatest economic harm and led to what the IMF referred to as a ‘she-cession’ across the region (Fabrizio et al., 2021).
The AU is committed to reducing informal work across the region and increasing labour and social protections for informal workers and the AU and the RECs each undertook public campaigns and adopted toolkits to address the gendered economic impacts of the pandemic. Some African national governments responded to calls to mitigate the gendered socio-economic effects of COVID-19 by introducing or expanding social protection measures for socioeconomically vulnerable households, including cash transfers and food support programmes for informal workers (e.g. Morocco, Namibia, Tunisia, Cabo Verde, and Togo) or for vulnerable women directly (e.g. Egypt, Senegal, and Kenya) which were designed to help female micro-entrepreneurs during the pandemic.
The problem was that these measures did not go nearly far enough, partly because they did not provide support to keep women in employment. The chair of one association of women entrepreneurs (market traders and small-scale farmers) in Uganda, with a membership of 60,000, argued that fiscal resources, rather than information campaigns, was needed, along with supporting traders through investing in better infrastructure. She pointed out that the problem was that the nature of women’s economic needs during the crisis was poorly understood because women were excluded from decision-making: There is an urgent need for infrastructure to respond to the economic crisis through simplifying processes to enable trading during COVID-19, building agribusiness to a level that can sustain local demand. Such responses should have been implemented before COVID-19, but the voice of women and those who advocate for women was missing or not heard. Consequently, there was limited focus on [women] entrepreneurs. Stimulus packages were requested. These would support infrastructure for traders and women. However, donors and governments are not interested in this type of investment. (Interview, 2020)
The consequences were inevitable. UNCTAD (2022) revealed that, in the region’s least developed countries,
3
unemployment almost doubled from 6.97% to 11.55% in 2020 alone, disproportionately affecting women and their dependent family members. The AU was certainly aware that governments’ failure to act and the weakness of regional organisations would have huge consequences for these women, as demonstrated in an interview with an AU representative: the dependence on the informal economy within these countries is making the situation worse because countries that implemented lockdowns, this disrupted the ability of the informal economy to continue being operational. (Interview, 2020)
Another AU representative highlighted the additional risk girls faced as a consequence of their mothers’ unemployment: The lockdown is impacting on informal work, where people work that day to earn money to eat that day. Therefore, parents are marrying off girls younger to relieve the financial burden – they are unable to feed them and getting these girls back into education will be a big challenge. (Interview, 2020)
Conclusion
The focus of this article has been on exploring the apparent failure of regional organisations in Africa to lead a gender-equitable response to COVID-19. It is hard not to conclude that the promises of normative leadership by regional organisations – in particular in relation to gendered social issues – fell considerably short during the pandemic, precisely at a time when it was most needed. We have identified a clear disconnect between early recognition at the regional level of the urgent need for policies to protect women and girls, across multiple areas, in the face of COVID-19 and lockdowns and the failure of regional organisations to lead that response in practice. In the process, there was a generalised failure to protect basic rights for women and girls to education, sexual and reproductive health services, access to employment and protection from poverty and early marriage in Africa. As COVID-19 took hold in the region, attention within regional institutions shifted away from the responsibility to protect the most vulnerable women and girls to engineering and funding a solely biomedical and frontline response, exacerbating the problem of keeping open critical services that women and girls desperately needed, from reproductive health clinics to schools.
What explains this failure? Some responsibility can be attributed to funding issues. Regional organisations in Africa depend on both donor and member state contributions and, with COVID-19 increasing fiscal demand on both revenue streams, funding was either redeployed to other areas of pandemic response or simply cut. But even with limited budgets, regional organisations still faced a choice as to whether they protected budgets already established for or allocated to services for women and girls and, in the cases we could identify they chose not to. Of course, some might say that the pace and intensity of COVID-19 made cuts to services that are essential for women and girls almost unavoidable. We profoundly disagree. We see no reason why women and girls should pay a higher price than men and boys during health crises. In that sense, therefore, we suggest that fiscal constraints on gender-equitable regional social policy, though very real, are only part of the explanation. More importantly, we draw attention to the consequences of the deep-rooted gendered hierarchies that exist in the fabric of African regional organisations, as well as their member states and donors, which became exceptionally evident during the COVID-19 crisis. The policies we document here reflect underlying beliefs and practices that place higher priority on some issues and groups than others, with women and girls often deprioritised. Concretely, this meant that, in the midst of a severe health emergency, even the immediate sexual and reproductive healthcare needs of women were not regarded as priority.
These experiences speak to the seriousness of the crisis of social regionalism in a general sense, but they also reflect the failure within all forms of institutionalised regional cooperation in the global South and within scholarly work on regionalism to take gender sufficiently seriously. It was not that regional organisations in Africa did not know how women would be affected, but rather that they were unable to operationalise their knowledge into policy and lead a response that ensured that a minimum floor of services for women would be protected. As such, there are key lessons for the future. From a scholarly perspective, much more detailed research is needed that explores and explains the failure to ‘gender’ regionalism, including research on the operation of regional norms and on regional social policy. Here, we have pointed to the utility of drawing on feminist approaches from other sub-disciplines of IR, particularly where these seek to move beyond the state-centrism of existing approaches to draw attention to the linkages between the operation of governance in the international sphere and the everyday experiences of women and girls. Second, within regional organisations that are discursively committed to supporting gender equity, such as the AU, there is a critical need to interrogate the continuing presence of gendered hierarchies and to strengthen women’s voices and build intersectional capacity to effectively join up policies that affect women and girls, recognising that these policies cut across the traditionally separate domains of social policy, educational policy, welfare, employment and so on. Doing so will require deepening relationships with women’s civil society organisations in order to protect the programmes that serve the needs of vulnerable women and girls and have them designated core services that must be protected at all costs (Bastagli and Lowe, 2021; Omukuti et al., 2021). Fundamentally, we suggest that it is only by interrogating and breaking down gendered hierarchies within regional organisations, as well as those imposed through their connections to member states and the wider global governance architecture and strengthening existing gender equality regional norms that regions will be able to begin to deliver on their discursive commitments to norms of gender equity for the women and girls at the receiving end.
Footnotes
Author Contributions
All authors have contributed equally to this work and approved it for publication.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknolwedge the funding support of two Global Challenges Research Fund (GCRF) projects: Thanzi la Onse (GCRF-MRC grant number MR/PO28004/1); and Gender and Health Systems in Low- and Middle-Income Countries after COVID-19: the Promotion of Women’s Health and Emerging International Policy Advice (GCRF-University of York).